
Abstract
Data management in transmural care is complex. Without digital innovations like Health Information Exchange (HIE), patient information is often dispersed and inaccessible across health information systems between hospitals. The extent of information loss and consequences remain unclear. We aimed to quantify patient information availability of referred oncological patients and to assess its impact on unnecessary repeat diagnostics by observing all oncological multidisciplinary team meetings (MDTs) in a tertiary hospital. During 84 multidisciplinary team meetings, 165 patients were included. Complete patient information was provided in 17.6% (29/165, CI = 12.3–24.4) of patients. Diagnostic imaging was shared completely in 52.5% (74/141, CI = 43.9–60.9), imaging reports in 77.5% (100/129, CI = 69.2–84.2), laboratory results in 55.2% (91/165, CI = 47.2–62.8), ancillary test reports in 58.0% (29/50, CI = 43.3–71.5), and pathology reports in 60.0% (57/95, CI = 49.4–69.8). A total of 266 tests were performed additionally, with the main motivation not previously performed followed by inconclusive or insufficient quality of previous tests. Diagnostics were repeated unnecessarily in 15.8% (26/165, CI = 10.7–22.4) of patients. In conclusion, patient information was provided incompletely in majority of referrals discussed in oncological multidisciplinary team meetings and led to unnecessary repeat diagnostics in a small number of patients. Additional research is needed to determine the benefit of Health Information Exchange to improve data transfer in oncological care.
Keywords
Introduction
Oncological care management is challenging because of its complexity. 1 Many oncological patients receive multimodality treatment, which requires a multidisciplinary approach. Multidisciplinary oncological care has increasingly been implemented globally to improve quality of care and treatment outcomes.2,3 To further improve outcomes and reduce treatment-related adverse events, complex oncological care has increasingly been centralized in specialized healthcare organizations.4–6 Consequently, patients often undergo initial diagnostic tests, treatment and follow-up in various hospitals.7–9
Data exchange in transmural oncological care is crucial. Since patients are often treated in multiple hospitals, critical patient information such as medical history, diagnostic test results, and medication lists is often dispersed across medical records of different healthcare organizations. Because of the heterogeneity of Electronic Health Record (EHR) systems in hospitals and interoperability between these different systems is often not yet possible, digital exchange or access to patient information in other healthcare facilities could not be achieved. A lack of access to patient information at the point-of-care impedes coordination and potentially introduces flaws and inefficiencies.10,11
Previous literature focused on the impact of patient data exchange during referrals in acute care settings rather than in elective, oncological care settings. In acute care, incomplete transfer of patient information between hospitals led to unnecessary repeat imaging in 23–60% of patients.12–16 Repeat and redundant diagnostic procedures were associated with an increase in resource utilization, costs, and impaired patient safety.13–15,17
In oncological care, the completeness and consequences of current information exchange without digital access to patient information between hospitals has not been determined yet. The study aim was to quantify patient information availability of tertiary oncological referrals, and to assess the impact of incomplete patient information on notification during multidisciplinary team (MDT) meetings and unnecessary repeat diagnostics.
Methods
Setting
This study was conducted in an academic, tertiary healthcare facility in the metropolitan region of Amsterdam, The Netherlands. After diagnostic work-up in general and academic hospitals, medical specialists referred oncological patients to the tertiary care center for additional diagnostics or specialized treatments. Referral took place by sending a referral letter and other corresponding documents in portable document format (PDF) by fax or secured e-mail. Imaging data were sent on a compact disc (cd-rom) by mail or secured weblink. Patient information was digitally inaccessible between hospitals, due to a lack of interoperability between hospitals’ EHR systems in the Netherlands.
Study population
All tertiary referred patients who were newly discussed at oncological MDT meetings were studied. The following patients were excluded from the analysis: (1) referred by general practitioners, national screening programs, or dentists, (2) presented at the emergency department, or (3) referred after in-hospital consultations.
Study design
A prospective cohort study was conducted between November 2018 and February 2019. All twelve oncological MDT meetings in the tertiary care facility were observed by an independent physician for 6 weeks. The observed MDTs were (1) breast cancer, (2) colorectal cancer, (3) oesophageal and gastric cancer, (4) head and neck cancer, (5) haematology, (6) kidney, prostate and bladder cancer, (7) liver cancer, (8) lung cancer, (9) neuroendocrine tumors, (10) neuro-oncology, (11) pancreatic and bile duct cancer, and (12) skin and soft tissue cancer. The newly discussed patients were identified during these meetings.
Data collection
Data were collected at three time points (Figure 1). First, the transferred patient information by the referring hospital was evaluated during the first presentation at the outpatient clinic. Second, an independent physician observed the MDT meetings to determine notifications of missing data. Third, additional performed diagnostic tests were assessed until one month after the first outpatient clinic appointment or start of the treatment. Motivations to perform these tests were obtained from the medical records and reviewed by the chair or a medical specialist of the concerning MDT. Data capture was performed in Castor EDC software (Castor, Amsterdam, The Netherlands). Flowchart of data collection. Abbreviations: MDT, multidisciplinary team.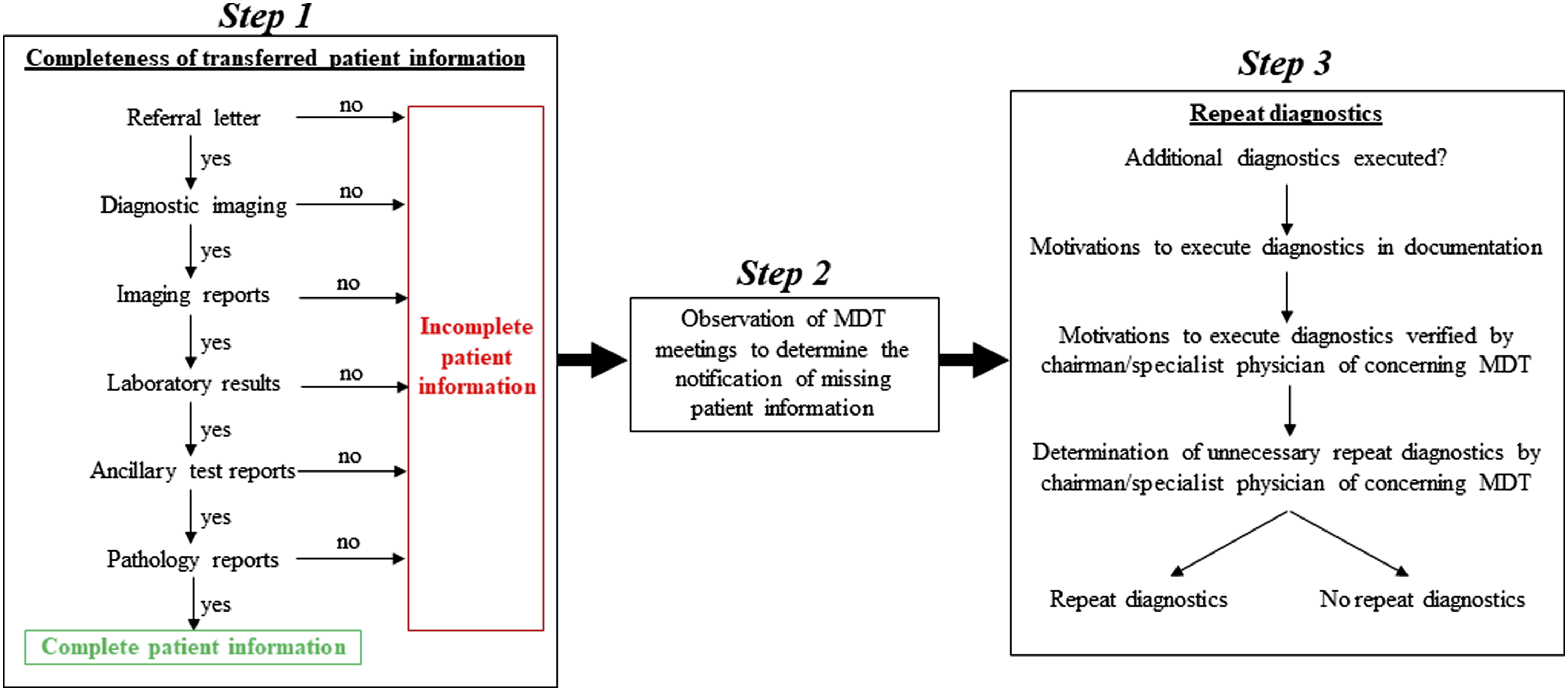
Study outcomes and definitions
The primary outcome measure was completeness of patient information at first outpatient clinic appointment. Overall completeness of patient information was defined as providing the referral letter and complete results of diagnostic tests performed in referring hospitals, delineated in the available correspondence. Diagnostic test results comprised submission of diagnostic imaging, imaging reports, laboratory test results, ancillary test reports, and pathology reports. Diagnostic imaging included all imaging modalities except for ultrasound. Ancillary tests comprised endoscopy, spirometry, and other tests. Secondary outcome measures were notification of incomplete information exchange during MDT meetings and repeat diagnostics. Repeat diagnostics were defined as unnecessary duplication of diagnostic tests as a consequence of incomplete information exchange.
Statistical analysis
Completeness of patient information per component, overall completeness, and repeat diagnostics were shown in absolute numbers and percentages. The confidence interval of the proportion including continuity correction was calculated. Statistical analysis was performed using IBM SPSS Statistics 26.0 software (SPSS Inc., Chicago, IL, USA).
Ethical approval
The study was conducted in the context of the Healthcare Quality, Complaints and Disputes Act with approval of the heads of participating departments. 18 Afterwards, approval was granted by the Medical Ethics Review Committee of Vrije Universiteit Medical Center (METc VUmc 2019.587).
Results
Patient and multidisciplinary team characteristics
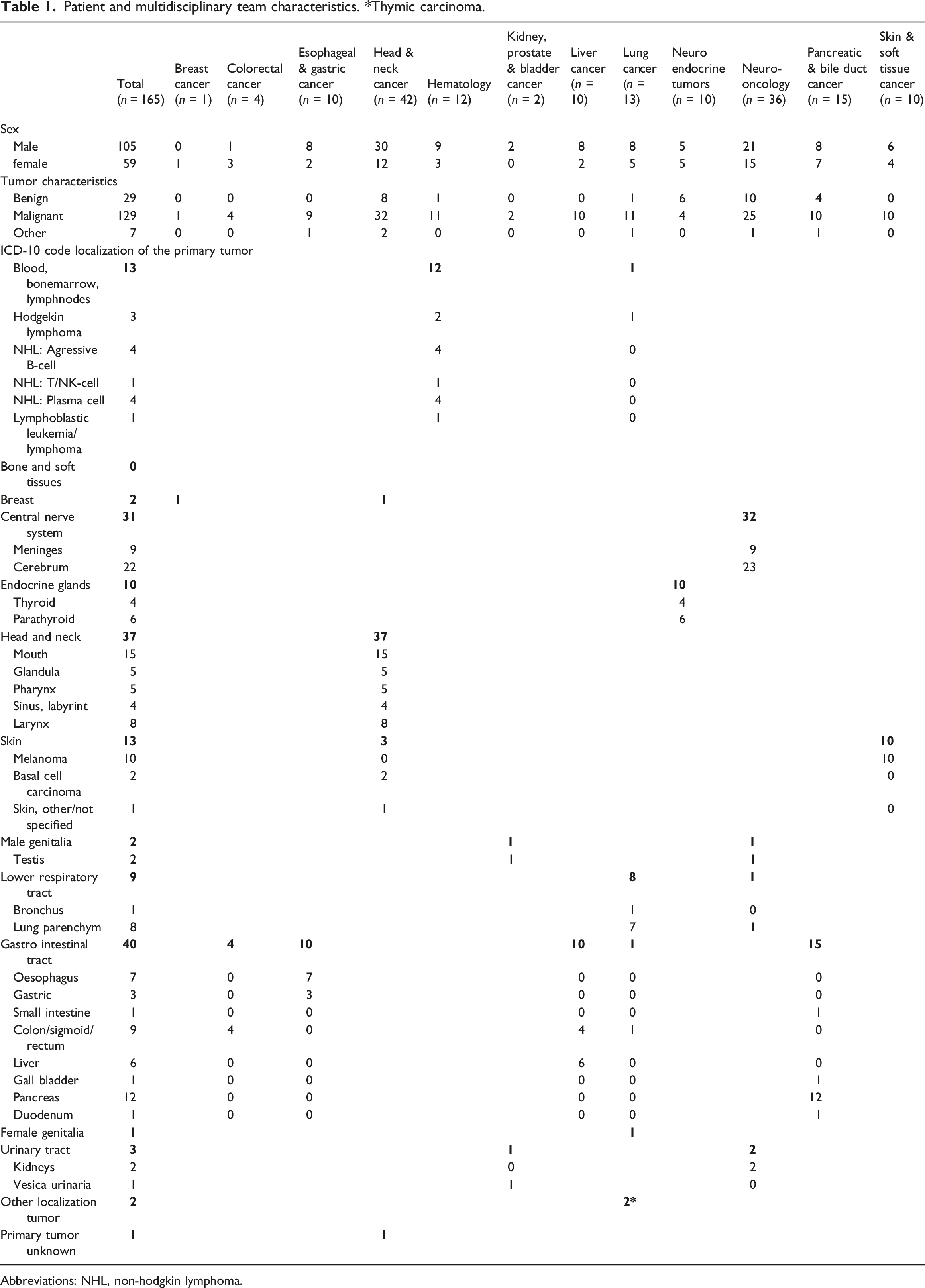
In total, 840 patients were discussed in 84 oncological MDT meetings. Of the 355 newly discussed patients, 165 were referred by medical specialists from 42 hospitals and included for further analysis (Figure 2). In this group, 129 patients had a malignant tumor, 29 a benign tumor, and 7 other pathology. For a complete overview of the origin of tumors and distribution between MDTs, see Table 1. Flowchart of patient selection. Abbreviations: MDT, multidisciplinary team. Patient and multidisciplinary team characteristics. *Thymic carcinoma. Abbreviations: NHL, non-hodgkin lymphoma.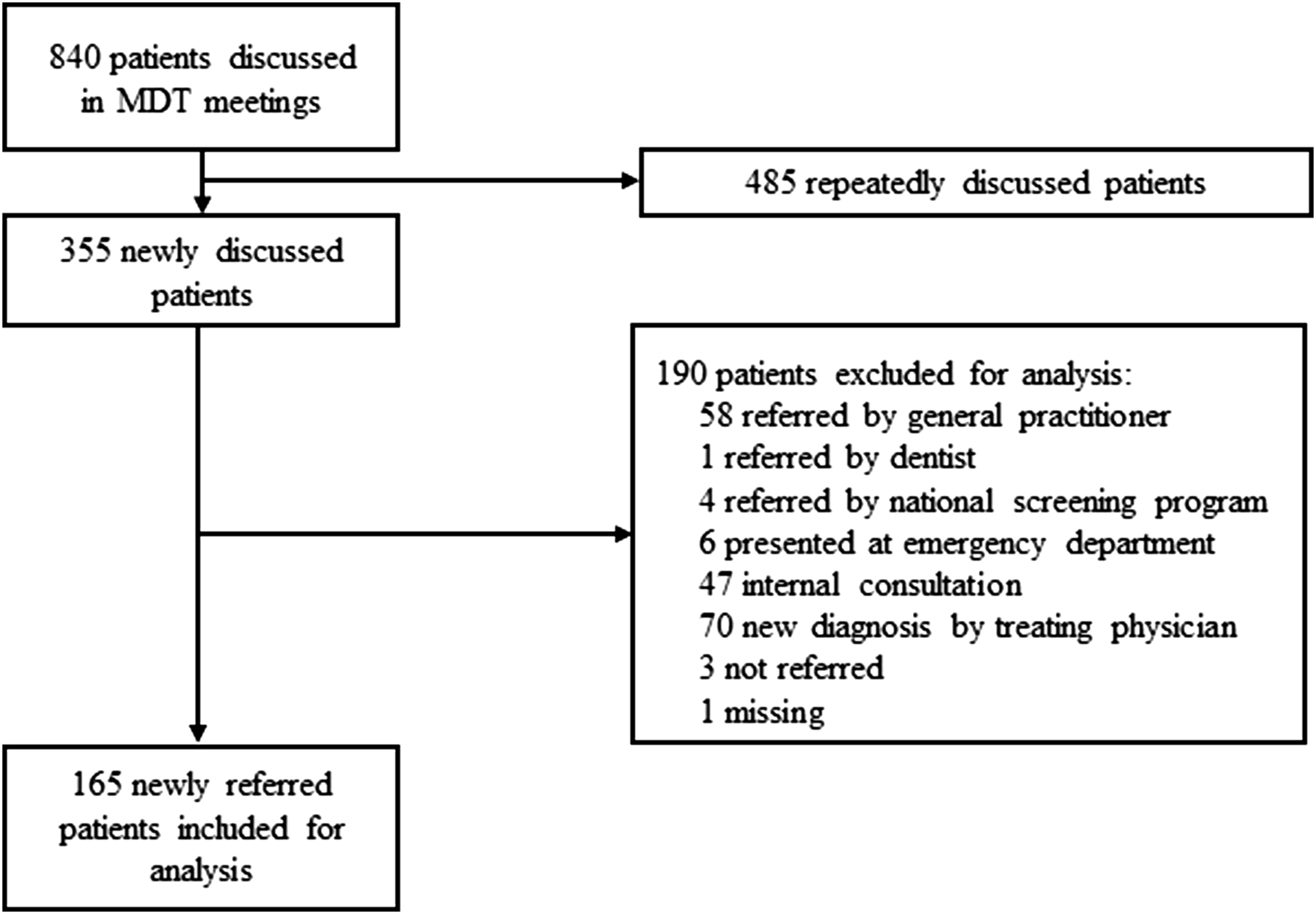
Completeness of patient information
Completeness of patient information and notification during MDT meetings.
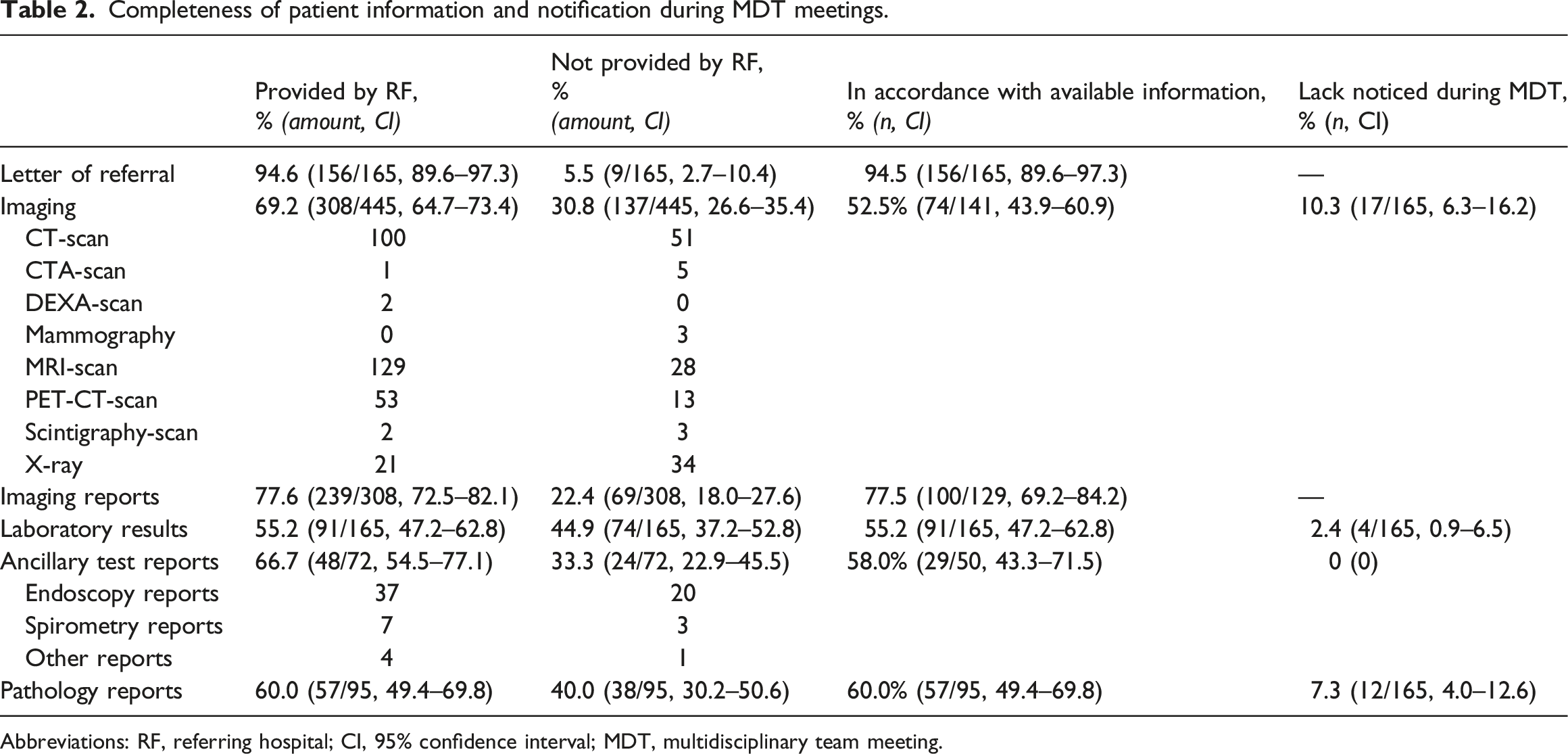
Abbreviations: RF, referring hospital; CI, 95% confidence interval; MDT, multidisciplinary team meeting.
Notification during multidisciplinary team meeting
Missing patient information was noticed in 18.2% (30/165, CI: 12.8–25.1) of patients during oncological MDT meetings (Table 2). Incomplete diagnostic imaging was noted in 17 patients (10.3%, CI: 6.3–16.2). Laboratory test results were missing in 4 patients (2.4%, CI: 0.9–6.5). Lack of ancillary test results was not reported. Missing pathology reports were noticed in 12 patients (7.3%, CI: 4.0–12.6).
Repeat diagnostics
Motivations for additional diagnostic tests.

Discussion
This study shows that patient information was incompletely transferred in over 80% of oncological patients referred to a tertiary care facility. Missing patient information was noticed in 20% of newly discussed patients during oncological MDT meetings and over 15% of patients had to undergo unnecessary repeat diagnostics.
The present study was the first one to prospectively assess the availability of complete patient information provided by referring hospitals and the effects in elective oncological care. Previous research in the field of acute care showed that 7–41% of imaging was not transferred and not available for review at the emergency department.12,13 The variety among studies could be explained by the examined imaging modalities. The presented study investigated all imaging modalities except for ultrasound, whereas Bible et al. investigated computerised tomography (CT) scans and magnetic resonance (MR) scans and Gupta et al. only CT scans.12,13 In addition, data transfer modalities could differ among acute and oncological care. Patients requiring acute care were often transferred to a tertiary referral hospital by ambulance, accompanied by a referral letter and diagnostic imaging on a cd-rom, while diagnostic imaging on cd-rom was sent by mail in elective oncological care. Transportation by mail could take several days and medical information could get lost. Moreover, advanced radiology import systems were available at emergency departments rather than outpatient clinics. Furthermore, it is interesting to note that our results on missing imaging reports (22.4% of patients) were consistent with other reports. Sung et al. described a lack of 16% of imaging reports and Bible et al. showed 8% of missing reports.12,16 Altogether, in acute and oncological care, incomplete availability of patient information at time of consultation was described in literature.
Unavailable patient information could have negative impact on valuable hospital resources, costs, and patient’s safety due to prolonged waiting time to treatment or repeat testing.13–15,17,19 Redundant testing could unnecessarily harm patients and repeat imaging could lead to radiation-related complications such as contrast nephropathy and increased long term cancer risk.20,21 The current study shows that 68.5% of the patients underwent additional diagnostics, of which 15.8% was preventable. Laboratory tests followed by imaging were most frequently repeated unnecessarily. The assessment of several diagnostic tests, including diagnostic imaging, laboratory tests, ancillary tests, and pathology, is a strength of this study since most studies have focussed solely on imaging. The hepato-pancreatic-biliary cancer cohort of Hallet et al. showed that 43% of patients underwent repeat imaging with the same modality and protocol, but the indication for repetition was not taken into account. 19 In acute care, repeat imaging was demonstrated in 23–60% of patients that presented at the emergency department.12,13,15,16 Hence, without access to patient information and test results between hospitals, a considerable number of referred patients undergo unnecessary repeat diagnostics, which might affect patients safety.
Motivations for repeating diagnostics are essential to determine preventability. In the current study, these motivations were established by order requests in the medical records and were revised by the chair of the concerning MDTs. The main motivation was to gain additional disease-specific information. Gupta et al. showed that the predominant motivation for repeating CT scans in a setting of trauma care was progression of symptoms. 13 Moore et al. demonstrated that 36.8% of trauma patients underwent repeat CT scans because of an inadequate data transfer on cd-roms and deterioration of the patient was the second most common reason with 26.3%. 15 So, even though the majority of repeat imaging is mandated by the need for additional information in the work-up of the patient, a substantial amount of repeat imaging could be prevented by complete data transfer and should therefore be called unnecessary.
In order to improve patient data availability across multiple providers and reduce unnecessary repeat diagnostics, the information system Health Information Exchange (HIE) has frequently been cited as a potential solution.21–26 The HIE infrastructure connects EHR systems of multiple hospitals, resulting in electronic access to health-related information such as diagnostic imaging and test results, discharge summaries, and medication lists, at the point-of-care. 27 By improving interoperability of EHR systems between healthcare facilities, HIE networks have the potential to improve the quality of healthcare, reduce costs, and increase patient satisfaction.21–25,28 Two systematic reviews about the usage and effect of HIE in clinical care were published.29,30 These reviews concluded that implementation of HIE may reduce emergency department usage and save costs in particular cases, but the effects on other outcomes are still unknown. In addition, several barriers have been identified to adopt HIE in clinical practice, including concerns about costs/funding, efficiency and workflow, lack of technical support, competition, inability to measure the value of HIE, and privacy and security concerns.31,32 From the patient’s perspective, the majority are willing to share their data in an HIE, but concerns about privacy and security are the main reason for opposing HIE or wanting to retain consent for data sharing.33,34 So, although many barriers to acceptance and sustainability need to be overcome, our results highlight the importance of exploring the potential of HIE for patient data availability in clinical practice since the potential benefits of HIE and patient willingness are recognized.
The HIE infrastructure has been implemented in many countries, although the availability, scaling of HIE infrastructure, and the maturity of HIE processes vary widely, not to mention cross-border interoperability.35,36 One of the leading countries is the United States of America. Since the Health Information Technology for Economic and Clinical Health (HITECH) Act, as part of the American Recovery and Reinvestment Act, has passed in 2009, there has been a rapid growth in adoption of EHRs in clinical and hospital care settings.35,37 Nowadays, electronic transmission of referrals is common within a healthcare organization using the same EHR system. However, when referring physicians use different EHRs or are outside the organization, the estimates of HIE adoption rates were about 50% in 2013, although this percentage is rising. 35 In Austria, Germany, and Switzerland, EHR adoption rates in hospitals were 52%, 50%, and 78%, and HIE adoption rates in hospitals were generally lower with 52%, 17%, and 14% in 2019, respectively. 32 In spite of the implementation of EHRs in the Netherlands, patient information is not yet digitally accessible across healthcare organizations due to privacy restrictions. In April 2011, the Senate of the Dutch Parliament unanimously rejected the Act for a national EHR because of privacy concerns. 38 Subsequently, healthcare facilities individually concluded contracts with various EHR providers. Due to a lack of interoperability between the multiple systems, digital data exchange was hampered. Since 2014, local and national initiatives on digital information exchange have been developed and will be implemented soon.39,40 So, advancements in HIE have been made globally, but the current state of HIE implementation varies widely between countries.
Several limitations of the current study need to be considered. First, it is acknowledged that this study was limited by a potential underestimation of the completeness of patient information since scanned documents in EHRs of the study hospital were analyzed instead of EHRs on providers’ level. For example, 58.1% (43/74) of patients without transferred laboratory results underwent additional laboratory tests in the study hospital. Consequently, we could not establish whether these laboratory tests were performed unnecessarily. Second, a prerequisite for adequate patient information transfer is clarity on the required patient information. Oncological MDTs of tertiary care centers should communicate their needed information as requirements differ per tumor type. This study did not consider these tumor-specific requirements. Third, the question remains whether incomplete patient information transfer has substantial clinical impact. This study aimed to quantify the clinical impact by establishing unnecessary repeat diagnostics and notification of incomplete data during MDT meetings. The timing for measuring the notification was suboptimal as additional patient information could have been requested in the referring hospital prior to the MDT meeting. These efforts could lead to a prolonged time to decision-making in the treatment strategy. 19 In addition, former imaging and test results have additional value in interpreting new test results and disease course over time. Therefore, further research needs to examine the various clinical consequences more closely.
In conclusion, this study shows that incomplete patient information was transferred in the majority of tertiary oncological referrals and over 15% of patients had to undergo unnecessary repeat diagnostics. Further research should be undertaken to determine the role of HIE in transferring complete patient information, reducing unnecessary diagnostics, and ultimately, improving the quality of oncological care.
Footnotes
Declaration of conflicting of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Netherlands Organisation for Health Research and Development (ZonMw) [grant Citrien Fund; grant number 839205001], as part of Moving towards Regional Oncology Networks program.
Ethical approval
The study was conducted in the context of the Healthcare Quality, Complaints and Disputes Act with approval of the heads of participating departments. 18 Afterwards, approval was granted by the Medical Ethics Review Committee of VU University Medical Center (METc VUmc 2019.587).