
Abstract
The Medication Reconciliation (MedRec) process aims to improve patient safety through safe prescription and medication administration. A validated survey was carried out to address aspects related to MedRec process, its obstacles, the role of information technology, and the required functionalities for optimizing the MedRec process. A total of 81% of the survey’s respondents acknowledged the roles of EHR (62% of respondents), PHR (41%), and electronic medication registration list (33%) as necessary technology tools for MedRec. Most respondents emphasized the need to compile multiple medications’ entries of information technology systems into one application (96.4%), allowing the entries from community pharmacies (90.6%). Further, incorporating information technology into the MedRec process presents a challenge in terms of legal responsibility (92 %) and the ability to integrate medications with other hospitals and community medications (78.6%). Findings affirm the need for a well-designed MedRec process aided with information technology solutions. The external data and user preferences should be considered when redesigning the MedRec process. The study also suggests initiating a policy that mandates sharing data necessary for creating a compiled medication list for each patient. MedRec is an indispensable tool for building a fruitful medication management system in a healthcare organization.
Keywords
Introduction
Medical errors are inevitable given the current disparities in healthcare providers, even within a single vendor. The Medication Reconciliation (MedRec) is the process of creating a complete list of medications by reviewing the current and the newly ordered medication to promote safety and reduce the possibility of medication errors. 1 Most medication errors occur during transferring patients (admission, transfer, discharge, or referral) as more than 40% of those errors are attributed to poor or lack of Medication Reconciliation. 2 Studies also show that 46% of errors occurred while admitting or discharging patients. 3 Fourteen percent (14%) of patients who experienced medication discrepancies at discharge were prone to readmission within 30 days than the 6% who did not experience discrepancies. 4
In Saudi Arabia, a tertiary hospital study revealed that 37% of admitted patients had at least one discrepancy in medications ‒ mainly omitting medication ‒ while 35% had dosage errors. 5 The occurrence of this discrepancy often intensifies when patients need multiple care settings and specialties. Furthermore, patient handoffs and care episodes by different providers can even exacerbate the situation. 4 Therefore, MedRec is designed to create the most accurate medication list by recording a patient’s current and required medication, comparing the list to those in the patient’s records and revising orders, and finally counseling patients on their complete medication list. 6
A study concluded that MedRec had reduced the number of medication discrepancies significantly (88%) and the proportion of patients with discrepancies as well. 7 Further, patients who underwent the MedRec process had a 67% reduction in risk for hospital revisit due to adverse events compared with those who had not experienced MedRec. 8 The implementation of electronic tools and other information technology interventions to the MedRec process would further minimize medication errors, in particular the omission-type of errors. 9
The Joint Commission (JC) acknowledged MedRec among the top three patient safety goals in 2015. The JC identified the five best practices for performing MedRec (NPSG.03.06.01) as part of the hospital-wide accreditation program. 10 However, implementing the MedRec process adds a financial burden on hospitals and requires a heavy workload to satisfy the demanding process. 11 Unfortunately, the positive impact of the MedRec process on medication discrepancies and errors cannot be extended to other process outcomes. 9 For example, IT-aided MedRec had no significant impact on the mortality rate in one study. 8 A systematic review concluded that the level of evidence on the impact of RecMed is low and further studies are required to assess the implications of information technology. 11 Therefore, this study aims to assess the MedRec practice in terms of value, rate of adoption, and explore the role of information technology in facilitating the MedRec process.
Method
The descriptive, cross-sectional study uses a survey that examines pharmacists’ opinions on Medication Reconciliation as a process and the role of information technology in process improvement. The survey was developed through reviewing the relevant literature, namely Tamblyn et al., 12 and interviewing the stakeholders. After drafting the main elements, the survey was validated by three expert reviewers, and a pilot study was conducted (13 surveys) wherein the final survey was modified accordingly. The survey comprises 14 questions addressing the following aspects:
I. Demographic data (gender, experience, pharmacy profession level, and type of hospital).
II. Familiarity with Medication Reconciliation (MedRec) including practice in hospitals (whether they practice and document MedRec), its value (impact on medication errors and patient safety), and the responsible profession to carry out MedRec (Pharmacist, Clinic Pharmacist, Nurse, and Physician).
III. The role of information technology in facilitating MedRec through an investigation of preferred technologies, anticipated challenges and required functionalities.
IV. Lastly, an open-ended question set for further comments and notes.
A five-point Likert scale was applied spanning from strongly disagree to strongly agree per question, and the “Agree” and “Strongly Agree” are combined as favoring score. The generated answers with quantitative nature were analyzed using a quantitative approach (using SPSS, V.25) and thematic analysis for the open-ended question. A sample size calculation was conducted considering the total population (8653 based on a recent pharmacy workforce survey in Saudi Arabia, 13 95% confidence level and 5% of margin error, the minimum sample size was 368 subjects. After receiving the ethical approval, six hospitals (three non-profit and three for-profit hospitals) were approached, and subjects were recruited on a convenience basis. Pharmacists and Clinical Pharmacists, who are currently practicing or had previous experience with MedRec, are the only participants in this study.
Results
Three hundred and ninety-three (393) surveys were distributed, and only 319 respondents have practiced or currently practicing MedRec. Forty-three surveys were excluded from further analysis, as it had missing values in 50% of the questions. As a result, the final sample size consisted of 276 participants (54% were male); 35% of the participants have work experience between 1 and 5 years, while 20% have 6–10 years, 16% with 11–15 years of experience, 10% with 16–20 years, and 17% with more than 20 years. Most respondents were pharmacists, 22% had clinical or decentralized roles, whereas the remaining group included clinical pharmacists. Only a small percentage of the participants (12.6%) are currently not practicing MedRec, while 58% had attended workshops on MedRec (see Table 1).
Descriptive analysis.
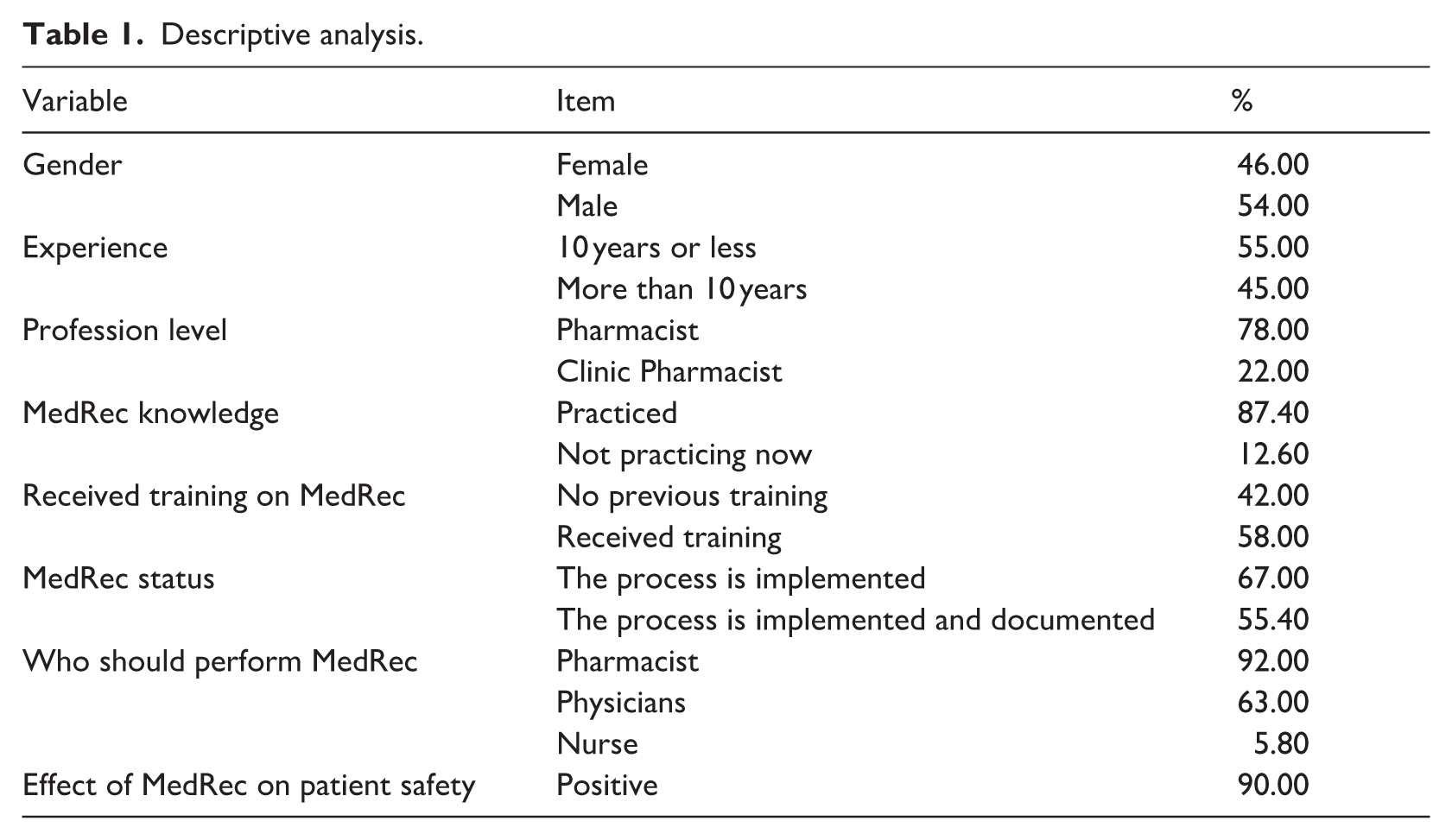
Sixty-seven percent (67%) of the participants responded that MedRec is implemented in their current hospitals, and only 55.4% revealed that it is documented. The majority of the participants considered Pharmacists (94%) as the ones who should be responsible for performing MedRec, followed by Physicians and Nurses (63% and 5.8%, respectively). Overall, 90% of the participants acknowledge the value of using MedRec as it can reduce medication errors and promote patient safety.
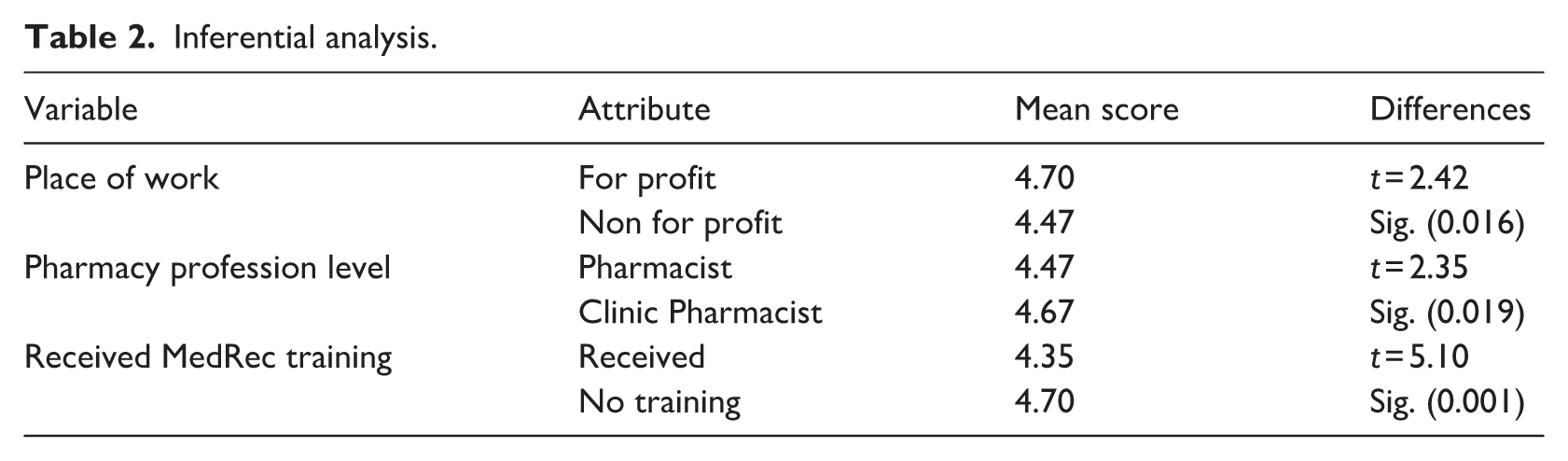
No significant statistical difference was found in the gender-based appreciation of the value of MedRec (t = 2.27, p = 0.45). However, there is a statistically significant difference in the level of appreciation of MedRec based on place of work, as those who work in for-profit hospitals appreciate MedRec more than Pharmacists in non-profit hospitals. Pharmacists who did not attend workshops valued MedRec more than the Pharmacists who did. Clinical Pharmacists appreciate MedRec more than Pharmacists (Table 2). No correlation was found between appreciating MedRec and work experience.
Inferential analysis.
As for the role information technology in facilitating MedRec, the respondents agreed on the three top-tier technologies to improve MedRec: EHR (75.7%), PHR (60%), and electronic medication registration tool (40.2 %). In relation to the required functionalities, most respondents emphasized the importance of compiling the multiple medications’ entries of information technology systems into one application (96.4%), followed by allowing the entries from community pharmacies and combining them with the therapeutics category (90.6%). A total of 81% of the respondents recommended that the designated application must generate a summary of the updated list of all medications and transmit the list to every pharmacy and prescribing physicians identified by the previous dispensing data. Finally, the feature of adjusting, stopping, or continuing community medication will provide a high value according to 53% of the respondents.
In terms of the anticipated challenges of using IT in MedRec, the respondents stated the following items: liability and legal responsibility (92%), ability to integrate medications with other hospitals and community medications (78.6%), willingness to re-prescribe drugs that were instructed by other physicians in the community (64.13%), the shift from commercial-name prescribing to generic product and dose-per-administration prescribing (40.6%), the time allotted to using IT (34.05%), disruption of workflow and clinic environment (15.60%), the running costs (15.57%), and finally, only 13.40% of the respondents mentioned IT knowledge and skills.
In response to the survey’s final question, 22.40% of the participants explicitly emphasized the need to redesign the reconciliation process to align with Information Technology. In addition, 13.70% of the respondents stressed the need for a structured form to standardize data collection and assure proper reconciliation process.
Discussion
The study confirms the value of MedRec as most pharmacists recognize its role in reducing medication errors and enhancing patient safety. The medication reconciliation process has the potential to identify medication discrepancies and minimize adverse drug events.9,14–18 A study indicated that MedRec could significantly reduce unforeseen medication discrepancies by 45% after using electronic Medication Reconciliation. 14
In this study, pharmacists’ positive attitudes toward MedRec is in line with the findings of a study conducted in psychiatric hospitals in Saudi Arabia, which concluded that 70% of pharmacists acknowledged the role of MedRec as a patient safety tool. 19 Unfortunately, only 30% of hospitals have a safety committee to oversee medication safety practices. Also, 37% of hospitals provide patients with medication lists at discharge, and none had pharmacists involved in obtaining medication histories. 15 In the context of MedRec training, workshop attendees tend to adopt a less favorable attitude to MedRec due to a lack of resources and poor training, according to Aljumah, as 40% of pharmacists have raised concerns over the lack of resources to guarantee successful delivery of MedRec. 19 Other major barriers to pharmacists practicing MedRec include its complex nature and time constraints.20,21 These barriers indicate the need for redesigning training and the reconciliation process during patient admission and discharge. Furthermore, establishing a culture that supports patient safety and a system-level intervention should be initiated with high management support and clear goals. 16
Most respondents appointed pharmacists as the professionals who should perform MedRec, unlike Alhasar and her colleagues’ study, which shows a lack of agreement on who should perform MedRec, whether pharmacists or physicians. 18 The disagreement might arise from the fact that their study’s sample is only composed of pharmacists. However, pharmacists’ involvement should be ensured as it enhances patient safety. 18 Further, pharmacist-led MedRec practice demonstrated cost-effectiveness and reduced the cost of preventable medication error by 43% per error per patient, as indicated in one study. 22
The respondents were aware of the promising role of information technology in facilitating the MedRec process and including data from other dispensing pharmacies and community physicians. This finding is supported by a body of literature that envisions the enormous potential of information technology in expediting the MedRec process. 23 The respondents have also emphasized the need to align technology with the MedRec workflow process, and hence users’ preferences should be sought and addressed.
Most respondents selected Electronic Health Record (EHR) as the preferred means to perform MedRec as opposed to Personnel Health Record (PHR) and standalone Medication registration tool, as the process entails making all medication items available during the MedRec. 24 Most respondents have also emphasized the importance of compiling medication entries into a single application, allowing entries from community pharmacies, and integrate them into the therapeutics category. These attempts are in line with Schnipper and his colleagues; their study concluded that using electronic MedRec that aligns the community medication with hospital medications resulted in a significant reduction in unintentional medication discrepancies. 25 Since decision support rules help empower the designated system, it is not functional to operate the system in question as a standalone system. This finding corresponds to the findings of Wright et al. 26 qualitative study on the necessary features for implementing reconciliation assistive technology. Establishing an Electronic Medication Reconciliation can improve patient safety and help minimize adverse drug events and discrepancies, as it can be integrated with hospital prescribing technology (CPOE or ePrescriber) to provide features of adjusting, stopping, or continuing community medication. 27
With the capability of Electronic Medication Administration Record to track medications and through the power of Clinical Decision Support System (CDSS), medication discrepancies will be minimized, and a safe health system could be introduced. Nonetheless, interviewing patients for verification, clarification, and reconciliation of the medications list is still necessary. 23 It is imperative to provide the patient with some educational resources and further investigate the feasibility to incorporate patient-generated data (or even PHR) into hospital medical records. Yet, such incorporation would require physicians or pharmacists to verify the external data, and assess the liability and legal responsibilities for relying on external data sources when making a clinical decision. 23
The willingness of physicians to re-prescribe drugs that were started by other physicians in the community should be studied. There is no consensus on how to overcome the challenges posed by MedRec. One approach was presented in the RightRx project presented by Schnipper and his colleagues’ study to build the system with two options: allowing 7-day medication supply or implanting a business rule of “continue as previous” option. 25
The study revealed that a hospital system must summarize all medications and transmit the updated list to every pharmacy and physician identified by the previous dispensing data. This finding necessitates establishing an operational Health Information Exchange through the National Health Information Center (NHIC). Further, the transition of care summary that conforms to the common interoperability standards and structures, like Health Level 7 (HL7)’s Clinical Document Architecture (CDA) and the American Society for Testing and Materials (ASTM International) Continuity of Care Record (CCR), can be exchanged between different care providers. Then medications can be compiled, and a list of current medications can be generated. 28
The study also recommends a policy-oriented intervention that entails adopting highly interoperable EHR and creating a compiled medication list for newly admitted patients as an important patient safety measure. Findings should be seen within the context of a descriptive-type study and limited to pharmacists’ perspectives.
Conclusion
Medication Reconciliation is an indispensable tool in promoting patient safety by reducing medication discrepancies. A well-designed MedRec process informed by developments in information technology can enhance quality, efficiency and medication processes safety.
Research Data
sj-docx-1-jhi-10.1177_1460458220987276 – for Medication reconciliation process: Assessing value, adoption, and the potential of information technology from pharmacists’ perspective
sj-docx-1-jhi-10.1177_1460458220987276 for Medication reconciliation process: Assessing value, adoption, and the potential of information technology from pharmacists’ perspective by Abdullah Al Anazi in Health Informatics Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.