
Abstract
Objectives:
This study explores the evidence available on Nursing Minimum Data Sets (NMDSs) by summarising: (a) the main methodological and reporting features of the reviews published in this field to date; (b) the recommendations developed and published in such reviews regarding the NMDSs, and (c) the categories and items that should be included in the NMDSs according to the available reviews.
Methods:
An Umbrella Review was performed. A search of secondary studies published up to November 2021 that were focused on NMDSs for adult hospitalised patients was conducted using MEDLINE (via PubMed), CINAHL and Scopus databases. The included studies were critically evaluated by using the Checklist for Systematic Review and Research Syntheses. The full review process was performed according to the Preferred Reporting Items for Systematic reviews and the Meta-Analyses statement.
Results:
From the initial 1311 studies that were retrieved, a total of eight reviews published from 1995 to 2018 were included. Their methodological quality was variable; these reviews offered four types of recommendations, namely at the overall, clinical, research and management levels. Additionally, seven NMDSs emerged with different purposes, elements, target populations and taxonomies. A list of categories and items that should be included in NMDSs have been summarised.
Conclusions:
Nurses are daily involved in the nursing care documentation; however, which elements are recorded is mainly defined at the local levels and relies on paper and pencil. NMDS might provide a point of reference, specifically in the time of health digitalisation. Alongside other priorities as underlined in available recommendations, and the need to improve the quality of the reviews in this field, there is a need to develop a common NMDS by establishing its core elements, deciding on a standardised language and identifying linkages with other datasets.
Keywords
Introduction
Werley & Lang (1988) defined the Nursing Minimum Data Set (NMDS) as ‘a minimum set of elements of information with uniform definitions and categories concerning the specific dimensions of nursing, which meets the information needs of multiple data users in the health care system’. 1 Specifically, a NMDS is both a tool and a strategy that label and theoretically defines each essential data or element that should be used by the majority of nurses across all types of healthcare settings. Due to its non-specific nature, a NMDS can also be used by a number of health care professionals, researchers and systems. 2
The NMDS has been established in the last forty years as a system capable of evaluating costs and the quality of the healthcare services provided, as well as to measure nursing workloads. 3 Specifically, the United States-NMDS (US-NMDS) was established in 1977 4 and was officially introduced in 1985. 5 Today, the US-NMDS and its developments are recognised as a point of reference in this field. 2 NMDS have also been established in hospital and community settings in different countries, such as in Canada, 6 Finland, Sweden, Switzerland, 7 Germany 8 and Austria. 9 Specific NMDSs have also been developed for sub-group of patients, settings or purposes, such as the Perioperative Nursing Data Elements (PNDS) approved in 1999 by the American Nurses Association’s committee on nursing practice, 10 and the Society of Gastroenterology Nurses and Associates-Minimum Data Set (SGNA-MDS). 11 More recently, a NMDS has been developed to support policymakers in preventing, controlling and managing drug poisoning in Iran. 12
According to Goossen et al. (1998), five important steps are required to develop an NMDS: (a) identification of relevant elements; (b) accurate definition of variables/elements or data; (c) determination of different values assumed by each variable; (d) adequate and standardised terminology for data recording; and (e) methods of aggregation and coding in databases created for NMDS purposes. 13 Subsequently, Sermeus and Goossen added that an NMDS must have a nursing focus with a minimal number of items capable of meeting the needs of the most possible users who may access the data and use it in a uniform manner. 14
In those contexts in which an NMDS has been well-established at system levels, it has been documented to allow: (a) a comparison of data collected in multiple settings and heath care institutions, including the international levels; (b) an evaluation of the nursing care offered and its outcomes and also a comparison of different settings; (c) a decision-making support tool aimed at designing further services according to the prevalent needs; and (d) a decision-making processes in both clinical and administrative fields. 1 Moreover, NMDSs can be used in both paper-and-pencil and electronic records, as well as during handovers 15 and to facilitate data collection and analysis, and thus, ultimately the measurement of a nursing service. 16
At the nursing care system level, the use of a NMDS has been documented to provide nurses with the opportunity to increase accuracy in planning and evaluating the nursing care (e.g. a Nursing Homes NMDS including falls and injury 17 ), and to prevent misunderstandings given that the elements collected within it are standardised both qualitatively and quantitatively. Moreover, it has been highlighted that a NMDS allows to analyse easily accessible and comparable data, offering the opportunity to make comparisons among groups of patients as well as across nursing diagnosis, interventions and outcomes (e.g. a Primary Care NMDS, including nutritional data to monitor the nutritional status 18 ). The data collected, may increase the quality of the health care services and, ultimately, the research capacity. 2 Having uniform data can also provide evidence regarding the amount of work performed by nurses and thereby provide support for establishing the resources needed at the bedside to ensure quality and safety in patient care (e.g. a NMDS for electronic nursing handovers 15 ; a NMDS regarding vascular access devices use and outcomes 19 ). Furthermore, given that nowadays there is a growing interest for electronic health records (EHRs), whose goal is to collect consistent and uniform data about patients 20 in efficient manner, the concept of NMDS has increased its importance. EHRs and other technologies are designed to obtain information on defined patients’ exposures and outcomes and to combine many different functionalities comprising the clinical decision support, 21 the health information exchange (HIE), 22 the administrative processes and other purposes. 23 To allow all these functions, the range of EHRs available impacting the nursing care (with some examples provided in Supplementary Table 1) should be based on a consistent NMDS: therefore there is an emergent and well-recognised connection between the EHRs and the NMDS.
Several reviews have been published to date to provide practical and research recommendations and to summarise commonalities and differences across the available NMDSs. However, no summary of these reviews has been provided, and those stakeholders or decision makers responsible to develop EHRs record’s systems at the institutional, regional or the national levels are still unsupported in their attempt to base the electronic nursing records on a reliable and recognised NMDS. Driven by the reason to summarise the evidence from the available research syntheses whose information should be critically assessed, an umbrella review covering a broad spectrum of literature by encompassing different study types (e.g. systematic review, scoping review) and various conditions (e.g. minimum data sets linked to the fundamentals of care) or populations (e.g. across countries) was designed. Having an accessible summary of the reviews available in this field might support: (a) policymakers and experts in designing electronic NMDSs; (b) managers in implementing an NMDS based upon standardised data, thus ensuring comparability and the continuity of care (e.g. from the hospital to community care); and (c) researchers in identifying priorities and in increasing nursing research productivity given that the lack of accuracy in datasets requires additional data collection. Therefore, the intent of this study is to render accessible the knowledge produced to date by providing a summary of the available reviews in this field.
Methods
Study aims
The study aims to summarise the evidence available on NMDSs. Specifically, the following research questions are addressed: (a) What are the methodological and reporting features of the reviews published to date in the field of NMDS? (b) What recommendations have been developed and published in these reviews regarding the NMDSs? and (c) What data, elements or information (hereafter categories and items) should be included in the NMDSs according to the available reviews?
Study design
An umbrella review protocol was designed. As reported by Aromataris & Munn (2015) on behalf of the Joanna Briggs Institute, 24 umbrella reviews are reviews aimed at incorporating all types of syntheses of research evidence, including systematic reviews in their various forms, with the intent to summarise all secondary studies available in a field. 25
Literature review
A search strategy was performed from March to May 2019, then updated in November 2021 (last search date 15th November 2021), by using ‘nursing minimum data set’ as a keyword. MEDLINE (via PubMed) and CINAHL (Cumulative Index to Nursing and Allied Health Literature) were accessed as the most relevant databases in the nursing field. The inclusion criteria were: (a) secondary studies, such as reviews, systematic reviews, narrative reviews and overviews, that had an available abstract; (b) written in Italian or English; (c) without any restriction as to year of publication to achieve a comprehensive outline of the evidence; and which focused on (d) NMDSs for adult patients cared for in hospital settings. All reviews considered appropriate have been included. Moreover, the title of each included article was entered on the Scopus database to find descendant reviews, which were also screened according to the aforementioned inclusion criteria. Their references were then screened in order to identify other relevant reviews to be included. Authors of the present review performed the entire process by working independently and then agreeing on the findings.
The search string produced 1311 eligible articles. After the removal of the duplicates, a total of 980 articles remained; 970 of these were excluded according to the inclusion criteria. Articles were excluded for a variety of reasons, such as main focus not on patient (e.g. datasets to support workforce planning in nursing
26
), non-English full-text articles (e.g. German
27
), publication type not meeting the inclusion criteria (e.g. study protocols
28
) and care not provided in hospital settings (e.g. nursing homes and community settings
29
). One of the remaining nine articles was excluded
18
upon analysis of the full text due to the specificity of the NMDS investigated in the study. Therefore, there were eight reviews included in this study as reported in Figure 1 according to the Preferred Reporting Items for Systematic reviews and a Meta-Analyses (PRISMA) 2020.
30
Flow chart of the search strategy and results according to the PRISMA
30
statement. Legend: PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses; CINAHL = Cumulative Index to Nursing and Allied Health Literature.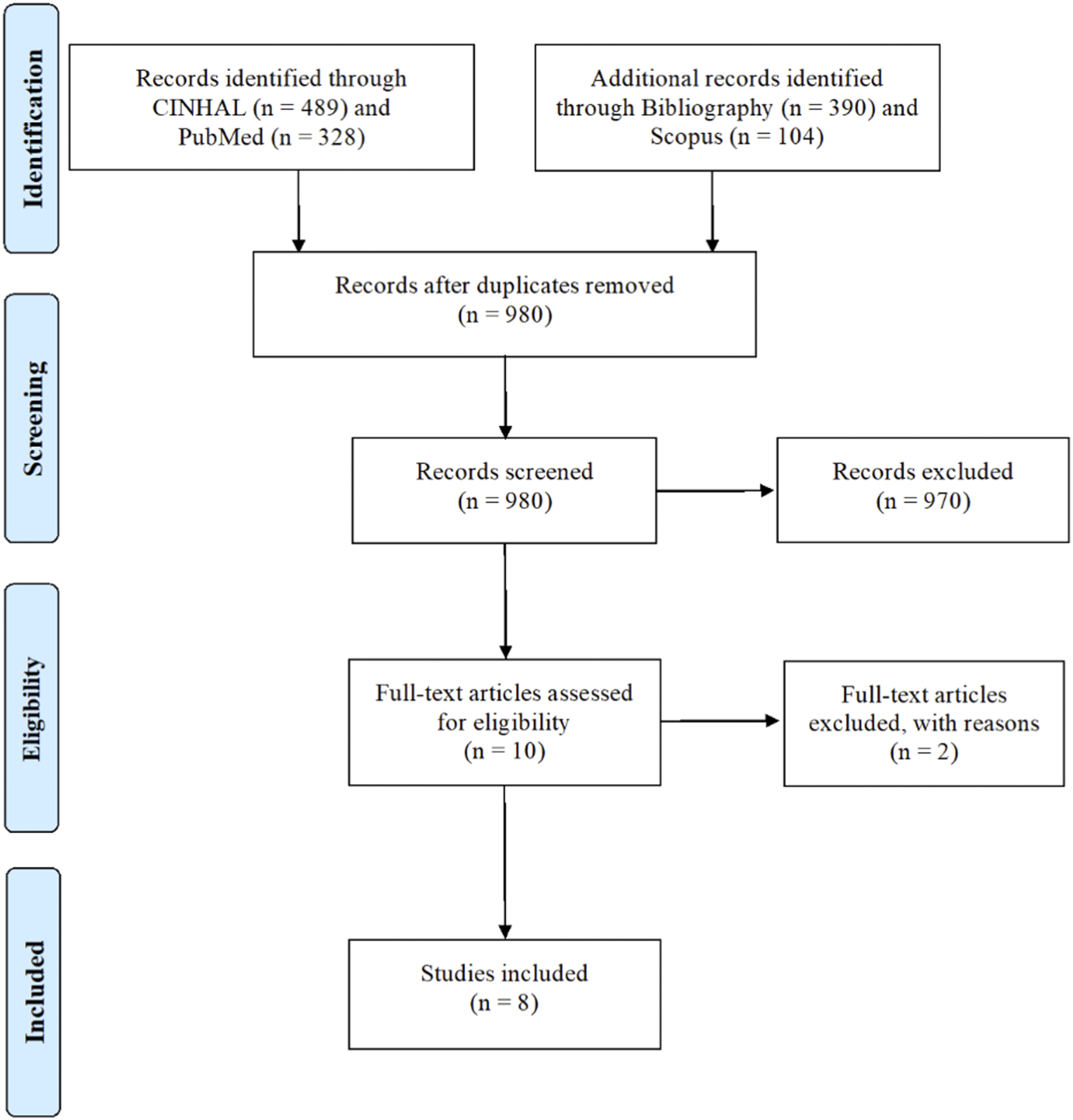
Quality appraisal
The methodological quality of the included reviews was assessed according to the Joanna Briggs Institute’s ‘Checklist for Systematic Review and Research Syntheses’ criteria. 31 The checklist used allows for a quality assessment and the identification of bias in design, conduct and analysis throughout the 11 questions. 25 Specifically, this tool explores the clearness in the explication of research questions as well as bias, the suitability of the search strategy, the evaluation of the included studies and the quality of the obtained results. The answers to each item vary between Yes (Y), No (N) and Unclear (U); the evaluation was performed by two reviewers independently (XX, XX) with disagreements resolved within the research team (no discrepancies emerged.). None of the eligible reviews has been excluded from the umbrella review according to the methodological quality emerged. This decision was based according to the following elements: (a) some reviews emerged to be designed and developed before the establishment of the methodological quality criteria (e.g. Goossen et al., 1998 13 ); (b) some of them, despite the limited quality, are considered seminal works in the field – as also appears from the citation ranked in the Scopus database (e.g. Sermeus and Goossen, 2002 14 ); and (c) the intent of the umbrella review was to emerge all recommendations published to date in this field of research, the categories, and the items that should be included in a NMDS. Therefore, the quality appraisal was performed to evaluate the methodological characteristics of the included reviews 32 and to gain an overview of the methodological quality achieved in this research field.
Data extraction
Data was extracted and summarised in three steps. First, the following data was extracted from each review: (a) author(s); (b) year of publication; (c) country; (d) study design; (e) databases or sources used by researchers while performing the reviews; (f) keywords used to search literature; (g) inclusion and exclusion criteria; and (h) number of studies included. Moreover, (i) the recommendations contained in each included review were extracted and categorised in overall, clinical, managerial and research recommendations. Second, in order to describe the NMDSs identified, there were extracted data regarding (a) the country, (b) the purpose(s) of the review, (c) the terminology used, and (d) the target population (e.g. medical units). Third, in order to identify variables, data, elements (=categories and items) composing the NMDSs as documented by reviews, these were extracted. In this research step, NMDSs not for hospital purposes (e.g. the CNMDSA; Community Nursing Minimum Data Set Australia) 13 and those not regarding nursing and/or health care documentation as well as those derived from multi-method studies (e.g. the NH-MDS; Nursing Handover Minimum Data Set) 15 were not included. All elements extracted were checked by two researchers to ensure rigour and accuracy in data extraction.
Data synthesis
The included reviews were described by their main features (e.g. year and country of publication, design, inclusion and exclusion criteria, population involved); moreover, the recommendations reported were categorised according to their intent as: (1) Overall, concerning general recommendations; (2) Clinical, including suggestions for clinical practice implementation; (3) Research, addressing the future direction of research in the field; and (4) Managerial, regarding the implementation of NMDSs at the micro (units), and macro levels (policy levels).
The NMDSs that emerged were categorised according to Goossen and colleagues, both for single items reported and for macro-classification. 13 Elements that emerged have been read carefully by two researchers (XX, female, clinical nurse; and XX, female, professor in nursing science) who subsequently have analysed their correspondence (not all elements were included in communications); in order to avoid redundancies, multiple elements which were part of the correspondence and related to one of the items reported by Goossen et al. (1998) 13 were also considered one time. For those items without any correspondence, a list was created. Goossen et al.’s (1998) categorisations were taken as a point of reference; however, according to the study purposes, NMDSs not described in their review were also considered, for example, the Thai NMDS (NMDS for Thailand), 33 the NH-MDS (Nursing Handover Minimum Data Set) 15 and the NMDS for fundamentals (Nursing Minimum Data Set for nursing practice around the Fundamentals of Care). 34
Results
Reviews: main characteristics and methodological quality
As summarised in Table 2, a total of eight reviews published from 1995 5 to 201834,35 met the inclusion criteria. Ryan & Delaney’s (1995) review was the first that was published in the field which was aimed at summarising the available research regarding NMDSs and soliciting researchers on the use of NMDSs. 5 Later, Goossen et al. (1998) compared five NMDSs to develop and implement an NMDS system in the Netherlands. 13 Sermeus & Goossen (2002) then summarised definitions, characteristics, content, stages of development, examples and issues related to NMDSs. 14 One year later, Volrathongchai and colleagues (2003) summarised studies regarding the development and the implementation of a Thai NMDS. 33 Next, Mac Neela et al. (2006) published an overview which included a critical analysis on the development, use and validity of available NMDSs. 7 In the last 10 years, Johnson et al. (2012) developed an extensive review with the intent to develop an electronic NMDS to use along with verbal handovers 15 ; moreover, Muntlin Athlin (2018) examined the link between NMDSs and the fundamentals of care in nursing practice and identified gaps to call upon future research on terminology standardisation. 34 More recently, Jeffs et al. (2018) provided an overview of the current state of performance measurement, key trends and a methodological approach to leverage in efforts to generate a standardised data set for fundamental care. 35
While most reviews do not explicitly report the number of studies taken into account, Johnson et al. (2012) included 10 studies published between 2008 and 2009, 15 while Muntlin Athlin (2018) included 20 studies published between 1999 and 2016. 34 Even keywords used to search the literature were not reported in each review. However, Ryan & Delaney (1995) used ‘NMDS’ and a combination of two or more of the nursing care elements of the NMDS (diagnosis, intervention, outcome or intensity) or the phrase ‘nursing care’ 5 ; Goossen et al. (1998) chose ‘nursing minimum data set’, ‘NMDS’ and ‘nmds’ 13 ; Muntlin Athlin (2018) employed the broad keyword ‘all fields’ adding a Boolean operator ‘minimum (AND) data (AND) set (AND) nursing’ and the plain keyword ‘nursing minimum data set’. 34
Quality appraisal of the included reviews using the ‘checklist for systematic reviews and research syntheses’. 31
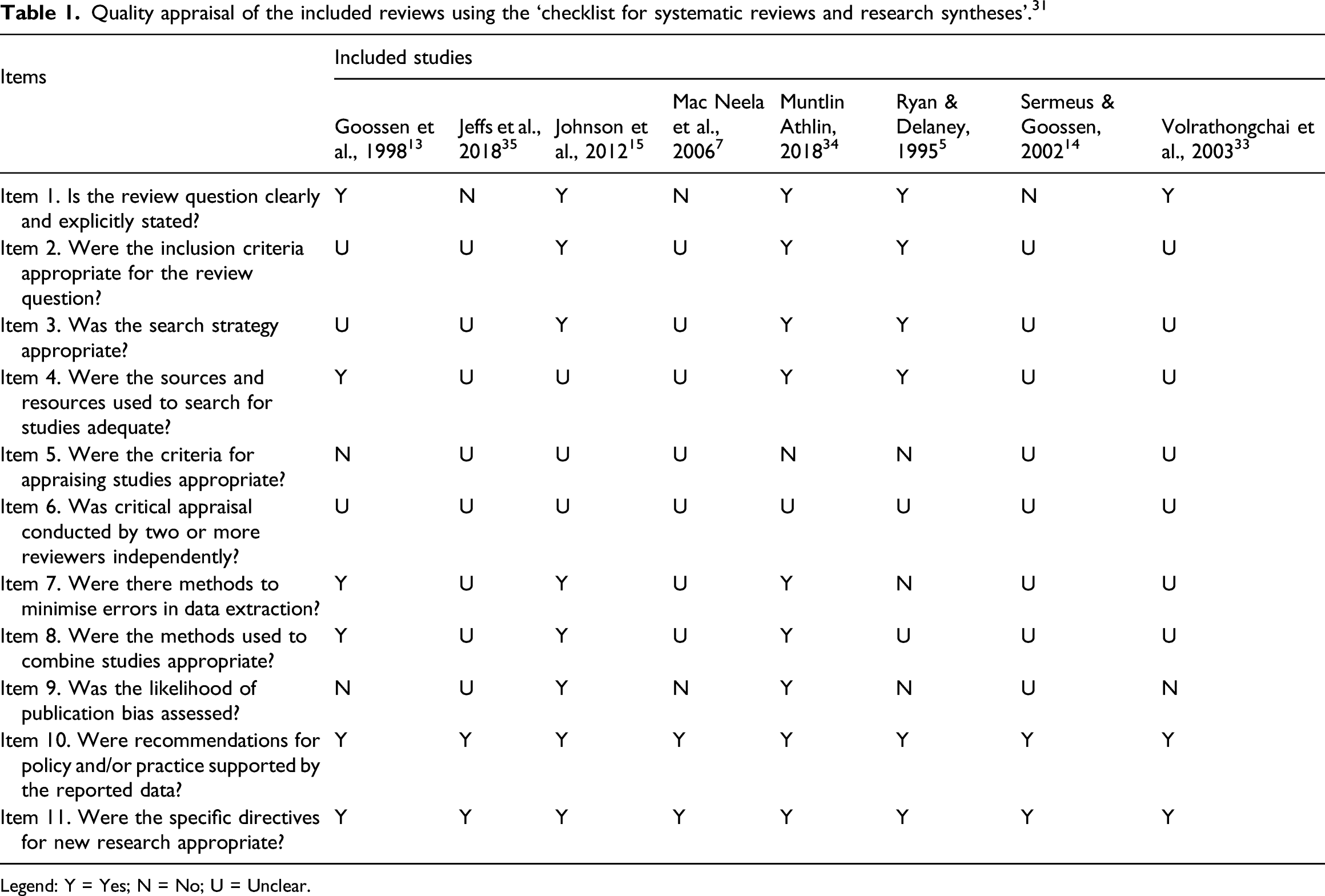
Legend: Y = Yes; N = No; U = Unclear.
Reviews: Recommendations
Summary of included reviews.
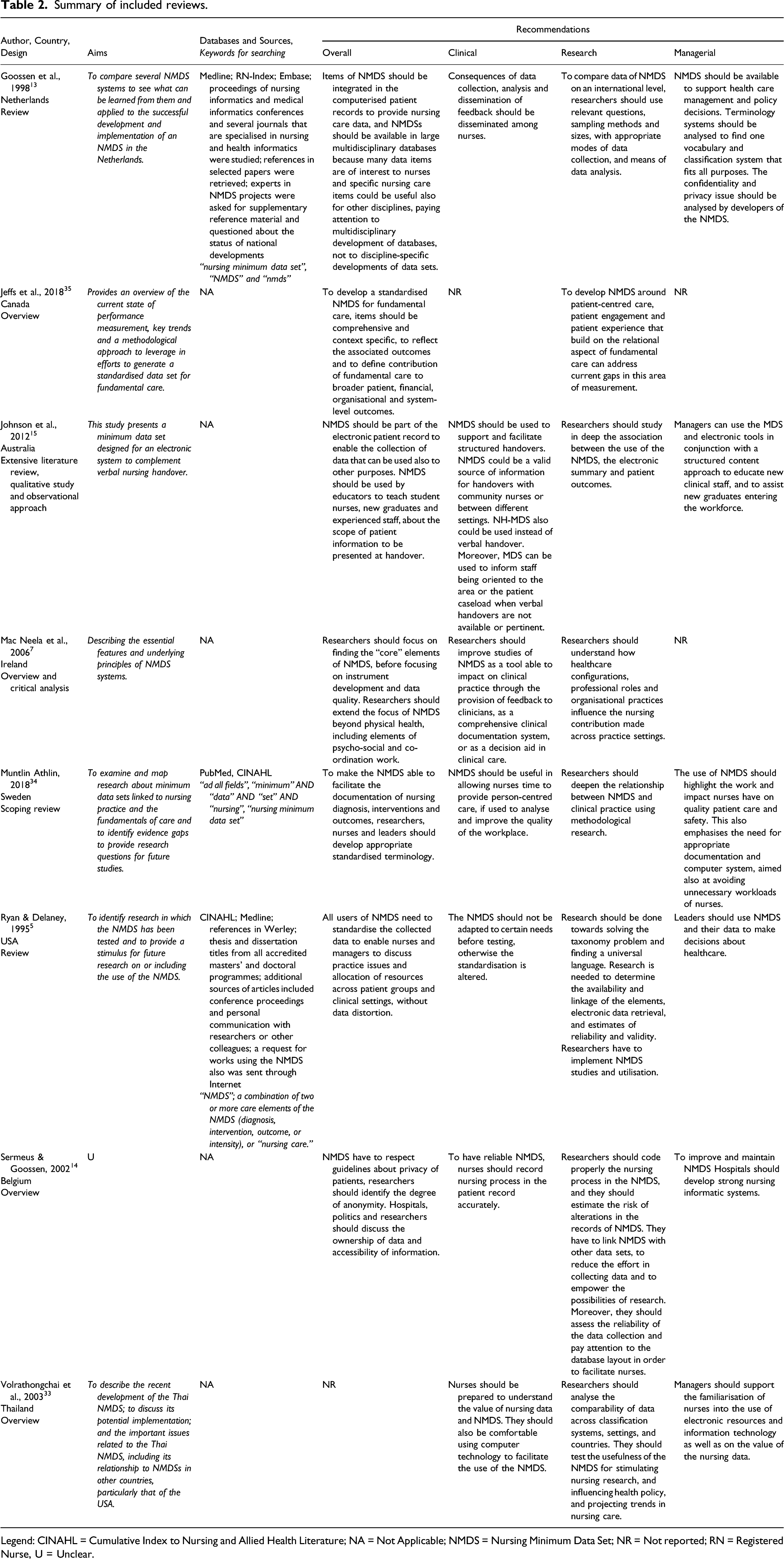
Legend: CINAHL = Cumulative Index to Nursing and Allied Health Literature; NA = Not Applicable; NMDS = Nursing Minimum Data Set; NR = Not reported; RN = Registered Nurse, U = Unclear.
Data collection should be standardised, allowing nurses and managers to discuss clinical practice and resource distribution issues without bias.5,13 In the implementation of an NMDS, easy data availability and quality of the information should be ensured.5,7 NMDSs should also be integrated with the electronic patient records and included in multidisciplinary databases used by multiple professionals.13,15 The suggestion has also been made that the level of data anonymity and privacy regulations should be discussed when implementing NMDSs.13,14 Furthermore, in order to prepare upcoming generations, it has been recommended that students be prepared to use the NMDS. 15
As to Clinical Recommendations, in the review by Volrathongchai et al. (2003), the need for nurses to understand the importance of NMDSs was underlined. 33 Nurses should be not allowed to adapt the tools to their context 5 and they should be prepared to report nursing data accurately. 14 Moreover, it has been recommended that nurses become familiar with information technology to facilitate NMDS implementation. 33 In this light, MacNeela et al. (2006) 7 and Goossen et al. (1998) 13 suggested the provision of electronic feedback or a system supporting the decision-making process: in fact, when used as a tool to improve workplace quality, NMDSs can support nurses in focussing on person-centred care. 34 Moreover, Johnson et al. (2012) 15 recommended that verbal handovers should be based on an NMDS.
The Research Recommendations in the reviews included the development of a link with other databases with the intent to expand research capacities 14 and to analyse the comparability of data across different classification systems, settings and countries. 33 NMDS implementation has been recommended to open a new research era in which it should be easy to explore how the structure of the health system, professional profiles and the practices used can affect the contribution of nursing to patient care. 7 Moreover, implementing research to validate the NMDSs, their effectiveness5,15,33 and their capacity to estimate patient outcomes 15 might expand the visibility of nursing care. Researchers should establish adequate search questions, sampling methods, collection and data analysis methods. 13 Furthermore, it has been recommended that the research be deepened to find the essential elements to be included in order to develop and validate an NMDS capable of capturing the nursing care in various settings and populations.5,7 Special attention should be devoted to those invisible elements of care such as patient engagement and experiences that are not currently measured. 35 Researchers should also direct their efforts towards achieving a universal classification and language to express the nursing care.5,13,34
Among the Managerial Recommendations, the need to use NMDSs to make data-driven decisions influencing health care was highlighted.5,13 Hospitals, administrations and researchers alike should define issues of data ownership and accessibility 14 ; it is also pivotal for hospitals to develop an adequate computer system to support and facilitate the use of NMDSs.5,13,34 Moreover, it has been recommended that managers improve the familiarisation of nurses with the use of electronic resources and information technology as well as with the value of the nursing data, 33 educating clinical staff and all new graduates. 15
NMDSs: Main characteristics
Only four reviews documented the items composing the NMDSs, namely: (1) Goossen et al. (1998) reported the Nursing Minimum Data Set of the United States (US-NMDS), the Minimal Verpleegkundige Gegevens/Résumé Infirmier Minimum for Belgium (MVG/RIM), the Health Information: Nursing for Canada Components (HI:NC) and TELENURSE & International Classification for Nursing Practice as well as TELENURSE & ICNP for Europe;
36
(2) Volrathongchai et al. (2003) reported the Nursing Minimum Data Set for Thailand (Thai NMDS);
33
(3) Johnson et al. (2011) reported the Nursing Handover Minimum Data Set (NH-MDS)
15
; and (4) Muntlin Athlin (2018) reported the Nursing Minimum Data Set for nursing practice concerning the fundamentals of care (NMDS for fundamentals).
34
Characteristics of nursing minimum data set according to the classification by Goossen et al. (1998). 13
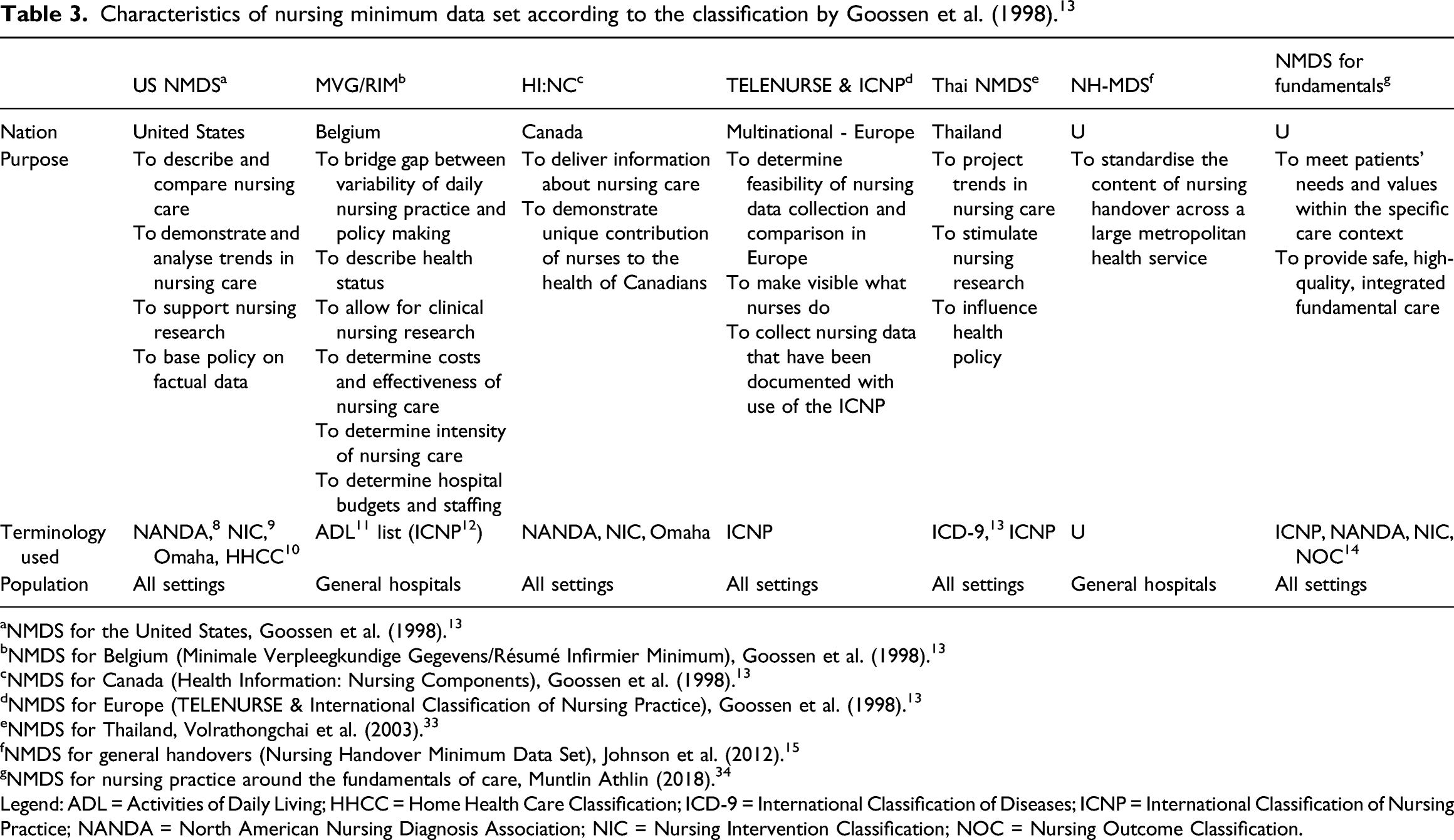
aNMDS for the United States, Goossen et al. (1998). 13
bNMDS for Belgium (Minimale Verpleegkundige Gegevens/Résumé Infirmier Minimum), Goossen et al. (1998). 13
cNMDS for Canada (Health Information: Nursing Components), Goossen et al. (1998). 13
dNMDS for Europe (TELENURSE & International Classification of Nursing Practice), Goossen et al. (1998). 13
eNMDS for Thailand, Volrathongchai et al. (2003). 33
fNMDS for general handovers (Nursing Handover Minimum Data Set), Johnson et al. (2012). 15
gNMDS for nursing practice around the fundamentals of care, Muntlin Athlin (2018). 34
Legend: ADL = Activities of Daily Living; HHCC = Home Health Care Classification; ICD-9 = International Classification of Diseases; ICNP = International Classification of Nursing Practice; NANDA = North American Nursing Diagnosis Association; NIC = Nursing Intervention Classification; NOC = Nursing Outcome Classification.
NMDSs: Categories and items
Classification of items included in the nursing minimum data sets according to Goossen et al. (1998). 13
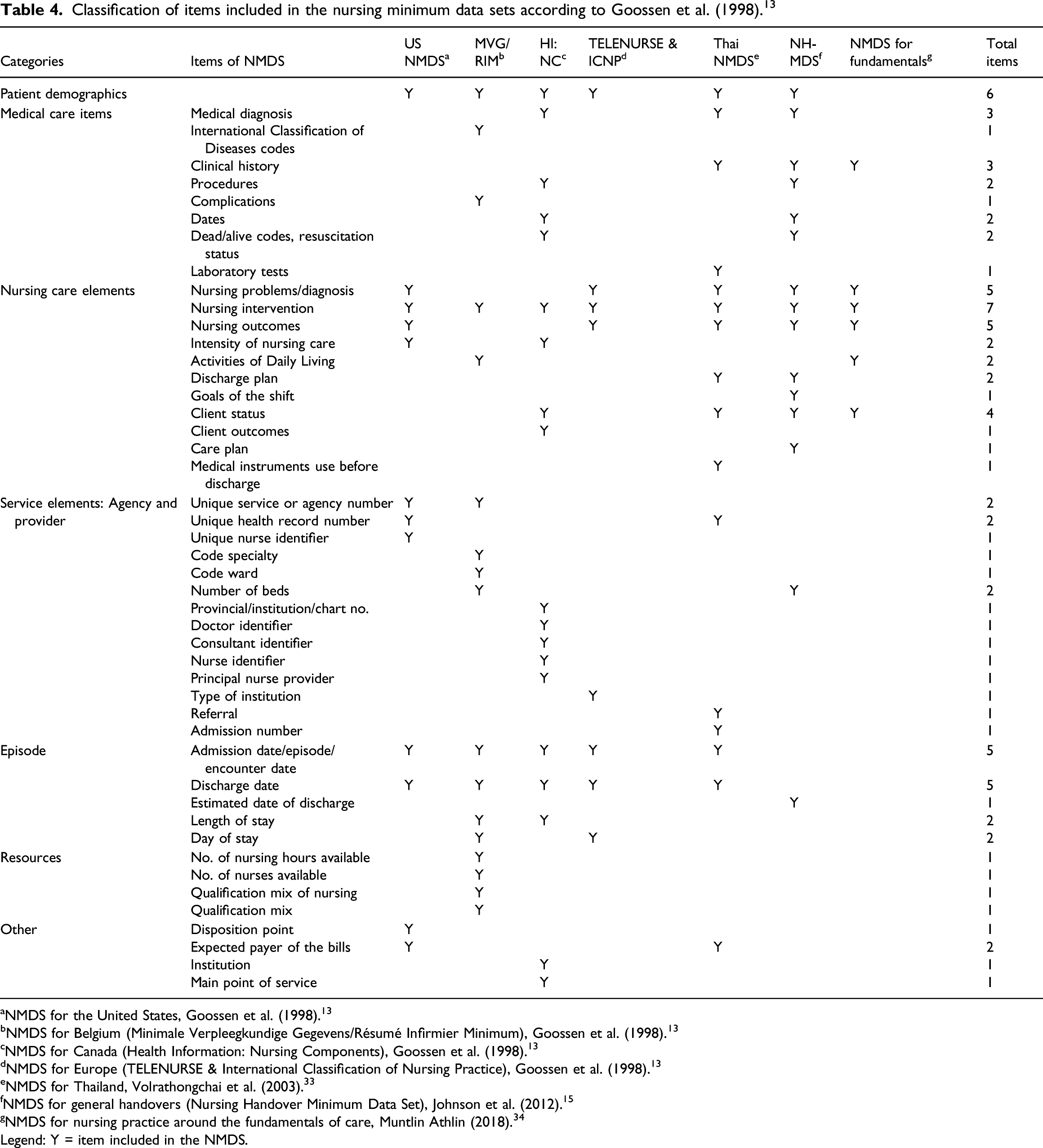
aNMDS for the United States, Goossen et al. (1998). 13
bNMDS for Belgium (Minimale Verpleegkundige Gegevens/Résumé Infirmier Minimum), Goossen et al. (1998). 13
cNMDS for Canada (Health Information: Nursing Components), Goossen et al. (1998). 13
dNMDS for Europe (TELENURSE & International Classification of Nursing Practice), Goossen et al. (1998). 13
eNMDS for Thailand, Volrathongchai et al. (2003). 33
fNMDS for general handovers (Nursing Handover Minimum Data Set), Johnson et al. (2012). 15
gNMDS for nursing practice around the fundamentals of care, Muntlin Athlin (2018). 34
Legend: Y = item included in the NMDS.
The NMDSs that do not report either Nursing problems/diagnosis or Nursing outcomes are the MVG/RIM and the HI:NC. 13 In addition, the MVG/RIM has included another element in the Nursing care elements (the Activities of Daily Living) and it held in great consideration the Resources, considered in terms of personnel. Among the items of the Service elements: Agency and provider category, the HI:NC reports multiple elements to identify the staff members who provide care (Doctor identifier, Consultant identifier, Nurse identifier, Principal nurse provider). In contrast, the Muntlin Athlin’s NMDSs 34 for fundamentals care contains elements mainly pertaining to the categories of Nursing problems/diagnosis, Nursing intervention and Nursing outcomes; the Clinical history is also cited, while other categories are not reported. The NH-MDS 15 is the tool that lists multiple Medical care items and Nursing care elements that can be useful in clinical practice; among items belonging to the other categories, the Estimated date of discharge and Bed number emerged.
With the exception of the NMDS for nursing practice around the fundamentals of care, 34 all of the NMDSs reported elements of Patient demographics. Similarly, the same consideration can be applied to the Episode category, in which one or more elements regarding hospitalisation are reported: the most common found in five NMDSs (US NMDS, MVG/RIM, NI:NC, TELENURSE & ICNP and Thai NMDS) 13 are: Admission date/episode/encounter date and Discharge date. The elements listed in the Other category include those pertinent to the health service provision at the national level.
As reported in Table 4, the US-NMDS 2 is focussed on nursing care, its changes, and the possibilities of comparing nursing data: therefore, its report elements concerning the categories of Patient demographics and Nursing care elements are closely related to the provided care and some service aspects that complete patient care and exclude the Medical care items. The MVG/RIM 4 concentrates on the progression of research but focuses above all on determining the extent of nursing care, reporting more items in Resources to identify aspects concerning timing, financial resources and personnel.
The HI:NC 6 emphasises the nursing contribution to the health system, reporting elements that highlight what nurses do and the consequences that these actions have on patients (specifically Nursing intervention and Client outcomes); it also provides the identification of the caregiver.
The TELENURSE & ICNP’s 36 focus on Nursing problems/diagnosis, Nursing intervention and Nursing outcomes, citing only items that are part of Patient demographics and Episode. It only mentions the Type of institution, thus putting minimal emphasis on the context. The Thai NMDS 33 includes items that are widespread not only among the Nursing care elements but also in all other categories in order to contextualise the care provided and to record those elements that could be useful in making managerial decisions. The NH-MDS 15 is aimed at standardising the nursing handovers within hospital settings and includes aspects of the Medical care items and the Nursing care elements commonly considered in daily care. Finally, the NMDS for fundamentals 34 aims to bring attention to the fundamental elements of care and patient values and has been included in the Nursing care elements.
Discussion
Reviews: Main characteristics and methodological quality
Eight syntheses of research evidence have been published on NMDSs to date. Different aims, study designs and methods have been used, from narrative to scoping reviews. Moreover, reviews have been conducted from 1995 13 to 2018, 34 suggesting that several primary studies have been published over these years. The critical appraisal of the reviews performed with the Checklist for Systematic Review and Research Syntheses 31 returned a variable set of findings with recommendations addressed in all studies. However, no reviews performed a critical appraisal of the primary studies included: reviews were conducted in different timeframes, and this might justify the lack of consideration of some aspects given that review methodology has changed over the years. 31 In terms of consistency, keywords used to retrieve the primary studies varied, suggesting the need to standardise the language in the field, which could be achieved, for example, by establishing a clear taxonomy. 5 However, according to its importance as capable to inform policies at the system (e.g. how to develop nursing electronic records), and at the nursing care levels (e.g. comparing outcomes) this research field require reviews with higher methodology.
Reviews: Recommendations
The eight reviews offered four types of recommendations—overall, clinical, research and management levels—that can be helpful in designing, validating, implementing, and disseminating the minimum data sets. First, all reviews recognised that the NMDS is a core element in the health sector because it provides access to reliable and comparable information about patients by collecting, processing and analysing data in a standard way. To achieve this goal, an NMDS should (a) be comprehensive and setting-specific 5 ; (b) use a uniform terminology 13 ; (c) be supported by proper information systems (e.g. computer) 15 ; and (d) allow a sort of flexibility according to the possible variations across care plans. 13 Second, some reviews recommended that an NMDS should lead to the delivery of person-centred care service7,34,35: in this light, more emphasis should be undertaken to fully integrate the Fundamentals of Care Framework into available data sets, 37 thus allowing nursing care to become more visible and traceable. Third, research progress has been highlighted as a significant factor for a successful NMDS implementation. In our umbrella review, research insights might be summarised along two lines. On the one hand, some reviews suggested exploring the relationship between NMDSs and nursing sensitive outcomes in order to fill the gap specifically with regard to the contribution of nursing care towards patients.15,35 On the other hand, more emphasis should be devoted to assess data comparability across different settings 13 : in other worlds, the availability of an overall NMDS capable of capturing all core elements of nursing care across settings will facilitate the continuity of care, the establishment of a common point of reference and the linkages with other health care datasets. Fourth, all reviews made the recommendation to consider the NMDS as supporting healthcare policy decisions. Moreover, at the managerial levels, strategies to promote nurse’s preparedness in approaching the electronic NMDS were recommended, 33 suggesting that the work environment should be appropriately shaped. In this context, more emphasis on risk management issues should be given in the available NMDS, especially since only one study evaluated its implementation with regards to risk management (e.g. adverse events). 34
NMDSs: Categories and items
Seven NMDSs have emerged, a number that can be considered limited given that the NMDS has been established since 1977. 4 However, we can assume that a large number of NMDSs have been established at hospitals and at the regional or country levels for practical purposes, but their degree of formalisation in primary or secondary studies have been limited. Every day, nurses devote a huge amount of time to documenting the care 38 in ad hoc prepared paper-and-pencil or electronic systems. Exploring these informal NMDSs with the intent to merge their features, as well as their advantages and disadvantages, might be useful. However, continuing to have different NMDSs mainly designed at the hospital levels prevents any form of measurement of the nursing care.27,28
The available NMDSs have been developed for different purposes, although all refer to support for nursing care, to make it visible and to increase the capacity of nurses to measure its impact on patients. 34 Moreover, NMDSs have also been established for internal purposes, such as increasing cultural awareness among nurses.13,34 Therefore, they have been established to date mainly with a practical intent, and only a few of the NMDSs have been developed for research purposes,13,33 such as to evaluate their effectiveness during handovers. 15 Non-standardised terminology is still present across the NMDSs, threatening any form of data comparison, probably because NMDSs have been established for practical purposes. Some NMDSs have been based on the NANDA, NIC and NOC classifications, 13 while others on the ICNP, 33 suggesting that international professional and scientific associations should debate this point.
With regard to the analysis of the correspondence between NMDS items and the categories identified by Goossen et al. (1998), 13 the NI:NC (the NMDS for Canada) 13 highly covered the categories, while the lowest was the NMDS for Fundamentals of Care. 34 On the one hand, the majority of tools neglected some aspects connected with service elements (e.g. number of beds) and resources (e.g. mix of nursing qualifications), mainly because these are not core elements of nursing care. On the other hand, the majority addressed elements of nursing care, such as activity of daily living and the nursing diagnosis. The categories defined by Goossen and colleagues (1998) 13 should be updated to be consistent with the needs of current patients, professionals and health care services. Moreover, some elements not strictly connected with nursing care that are not contained in the available NMDSs might be considered as elements of other linked datasets about nursing care with the aim of providing an efficient system. There is a need to develop a consistent NMDS system to ensure the support needed as main data sources of the available and that emerging EHRs technologies (e.g.39,40).
Limitations
This umbrella review has several limitations. First, we limited the search strategy to the major databases of the nursing discipline and some reviews may have been missed. Secondly, according to the research questions, we mapped the main aspects of the included reviews: the different methods used in conducting the reviews prevented a homogeneous extraction and synthesis of the data. Thirdly, the categorisation of the recommendations that emerged were performed by researchers and their professional background might have affected the process and the findings; moreover, the process of categorisation using the framework established by Goossen et al. (1998) 13 might have also influenced the findings. Furthermore, we have included all reviews without considering their methodological quality: with the advancements in the reporting guidelines and methods, future umbrella review should consider the methodological quality as an inclusion criterion.
Implications for practice
The overall findings of this umbrella review may have multiple implications: • At a nursing care level, the identification of nursing minimum data categories and items as emerged, may provide a guideline on how these can be standardized both nationally and internationally and how this can inform and advance the quality of nursing practice and healthcare in general given the critical role that nursing plays in healthcare. • At a hospital and managerial level, given the impulse to develop electronic records39,40 also to save the extensive time required to fill in paper-and-pencil records, the emerged NMDS categories and items might create the basis to progress in the digitalization of both nursing records and handovers. • At a system level, the overall recommendations that emerged might support and address policies aimed at standardising languages, tools, and methods in the nursing field mainly through electronic resources and information technology. • At a research and evaluation level, findings might help in implementing a minimum data set enabling easy comparison and benchmarking of the data, thus promoting both research and managerial decisions, for example regarding the evaluation of nursing sensitive outcomes and workloads.
Conclusions
Nurses have always recorded the care provided to patients to ensure the continuity of care, to assess the care and its effects on patients and to make their contributions visible. To date, documentation systems developed in each hospital with non-standardised language still prevail. Moreover, these systems are often based upon a paper-and-pencil approach and offer a lack of comparability of documented data, threatening both research and managerial decisions, for example, regarding the evaluation of nursing workloads.
In the context of the digitisation of care, we have critically analysed the available reviews to summarise the recommendations regarding the NMDs established to date and the elements included. Available reviews were produced from 1995 to 2018, thus revealing a continuing intent to summarise the available evidence produced by primary studies. A variability in the core elements of NMDSs as well as in the languages and in their purposes have emerged. NMDSs should be developed to not only improve the practice but also the capacity to undertake effective decisions at a clinical and managerial level. Researchers and professionals are called to establish at the worldwide level the core elements of a dataset in a standardised language. Moreover, there is a need to update the recommendations that emerged by continuing to analyse the reviews produced in the field an also establishing a periodic evaluation of their implementation.
Supplemental Material
Supplemental Material - Nursing minimum data sets: Findings from an umbrella review
Supplemental Material for Nursing minimum data sets: Findings from an umbrella review by Francesca Freguia, Matteo Danielis, Renzo Moreale and Alvisa Palese in Health Informatics Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Due to its nature, this study does not need any ethical approval.
Guarantor
Alvisa Palese
Contributorship
FF and AP conceiving the idea and performed the review. FF, MD, RM and AP wrote the manuscript. All the authors approved the final version of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.