
Abstract
Objective
To carry out a systematic literature review to identify the Value Based Digital Health elements.
Methods
The search for records was carried out for the period 2012 to January 2024, in two main databases, EMBASE and Scopus. Records were limited to studies published since 2012. Studies presented either a conceptual framework on the concept of Value-Based Digital Health (VBDH), or results from an empirical work to generate evidence on the value of digital health, or a combination of both. The characteristics of the study, the type of digital health and measures and/or their value elements included, are synthesized and interpreted. To synthetize information, the patient journey phases are used as themes, where the identified value elements are allocated. This is analyzed by type of agent (of the general healthcare framework).
Results
The search yielded a total of 606 abstracts for screening. In the end, 67 studies were finally included for data extraction. VBDH elements are presented by phases of the patient journey and by agent. Despite the high heterogeneity of patients, theoretical and empirical works converge in elements such as the value of patient-centered care, education (health literacy) in the use of new digital health technologies, mechanisms to increase patient confidence and their participation in the health decision-making processes, or the importance of collecting patients’ reported outcomes and experiences, among other elements. The review also found empty areas among theoretical and empirical studies, where no VBDH elements were identified.
Conclusion
This systematic review identified the theoretical and empirical elements to measure the value of digital health and provides a framework of VBDH elements. Some of the theoretical elements are actually used in practice. Others, however, despite being relevant from a theoretical point of view, do not seem to be measured empirically. This work provides researchers of a source, for consultation, of value based digital health elements. This is helpful for improving the measurement of the value of digital health.
Keywords
Introduction
There are multiple definitions of Digital Health in the literature. Digital Health (DH) primarily focuses on healthcare in the digital world, bridging the evolution of advances in informatics and technology in medicine, health and all aspects of health care with the application of these developments in clinical practice, the patient experience, and their social, political and economic implications. The common element to all definitions of Digital Health is a digital intervention that examines the provision of healthcare and not only the use of the technology itself. 1 When referring to value of health tools, generically, in the literature this has been defined as the outcomes that are important to patients, relative to the costs required to achieve those outcomes. 2 In this study, the value of digital health will be explored, including not only looking for the value-based elements of health technologies, but any digital health resource used for the provision of health services. This is what this work understands by the concept of Value-Based Digital Health (VBDH).
The concept of Value-Based HealthCare (VBHC) was introduced by Michael Porter about fifteen years ago. 3 VBHC is currently being used as a guide for the healthcare practice towards those activities that generate the best possible health results or outcomes for each monetary unit of expenditure. The VBHC approach, thus, emphasizes the overall result of the health care process, that might be carried out on people or patients, considering the partial or complete recovery of the health state and the sustainability of that recovered health in relation to the efforts made. It has been argued, however, that the use of technology only leads to better health outcomes if the related cultural challenges are acknowledged and the new needs of patients are, actually, met. 4
Health systems are currently undergoing a digital transformation process that affects all areas of the health care process. The VBHC paradigm is evolving to a VBDH approach in many leading healthcare systems worldwide. VBHC and VBDH are closely related, both in the search for more effective and value-focused healthcare for patients. Paul Sonnier defined Digital Health as “that discipline where the digital and genomic revolutions converge with health and healthcare.” 5 However, defining the concept of VBDH and its implications is a work still in progress, but necessary, to give strength to this emerging concept, in order to help on this transformation process, by improving its quality, resilience, sustainability and innovative capacity. VBDH is, in the end, understood as the use of digital tools, solutions, strategies, and ecosystems to contribute to the generation of value in health. 6 Investigating the concept of VBDH is, thus, crucial because it optimizes healthcare and improves the efficiency of the healthcare system by focusing on outcomes that matter to patients and maximizing the use of resources.7,8
Some literature reviews have attempted to identify how VBDH is conceptualized in the literature, but these were in very specific settings,9,10 with the focus only on the economic value, and not on the effectiveness of VBDH, 11 or was done for the perspective of health professionals only. 12 No systematic literature review has, yet, approached, the concept of VBDH including all perspectives and all identifiable settings. Efforts have been also made trying to identify the degree of maturity of healthcare professionals on the use of digital health tools and technologies. Specifically, there is evidence of negative experiences due to the fact that the transformation process on this new digital changes the way some health services are provided. 2
The aim of this study is, thus, to carry out a systematic literature review on the identification of the VBDH elements.
The nature and extent of published evidence, that has linked both concepts, theoretically and empirically, is summarized into a conceptual framework of use in research and in the clinical practice.
Methods
Review design
A systematic literature review on the identification of value elements of digital health, VBDH, is the chosen method for gathering and analyze information regarding the concept of VBDH. Systematic literature reviews follow strict protocols. 13 First, the selection of at least two databases for the search was done and agreed by all authors, leading to the choice of EMBASE and Scopus as the two main databases for consultation for this work. The combination of these two databases led to a good number of records. It was considered that additional databases would need to be consulted if the selection of papers would not lead to an enough number of papers for the data extraction. This was not necessary in the end. The review method is qualitative, and targets the identification of value elements of digital health, and their description, in theoretical and empirical studies. To synthetize information, the patient journey phases (prevention, diagnosis, access to health care services, hospital/home care, specialist care, treatment and valuation/measurement of health outcomes) are used as themes, where the identified value elements will be allocated at the data extraction phase. This will, also, be analyzed by type of agent. Two researchers worked on the screening of abstracts and full texts. The data extraction method was also agreed by all authors, but was conducted by one researcher. A second researcher checked 10% of the screened abstracts, until there was agreement with the final selection and distribution among included and excluded records. This second researcher also checked the data extraction and the quality and bias assessment. The review was not registered in PROSPERO given that the initial idea was to conduct a scoping review (although in the end a full systematic review was conducted), which is a type of review that does not require registration in this system.
Search strategy
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 14 The PICO/PECO method was applied to structure. 15 The framework of this systematic review according to PICO was: any place where the process has been studied and/or attempted to measure the value of digital transformation in the provision of health services (population); Digital transformation in health (Intervention); the elements identified in the theoretical literature vs. empirical works (comparison); theoretical elements to explain the value of digital health, and value elements of digital transformation in the provision of health services (outcomes).
The keywords of the search algorithm were combined using Boolean terms. The search strategy was conducted in EMBASE and Scopus:
((digital health OR digital healthcare OR digital health care OR digital health intervention* OR digital health technolog* OR telemedicine OR telehealth OR eHealth OR electronic health OR M-health OR mobile health) AND (value-based healthcare OR value-based health care OR value based healthcare OR value based health care)) NOT (Cost-effectiveness OR cost-utility OR cost-benefit)
Inclusion and exclusion criteria
Records were limited to any academic article or grey literature (e.g., reports from official and reliable institutions such as, for example the WHO) published since 2012 and available in full text format, in English or Spanish language, that provided relevant information about the theoretical model of the value of digital health transformation, as well as empirical works that actually measure the value of the said transformation, either for some specific digital technology, or for the set of digital health technologies in general. Articles that offered only a cost-effectiveness/utility analysis without any additional disruptive or novel measure of the value of new digital health technologies were not of interest, and were, thus, excluded.
Both purely theoretical and empirical descriptive studies, well designed, or with solid econometric analysis, were admitted. For qualitative studies, it was verified that the source of the information was reliable, or that the interviewed population had knowledge at an expert level. It was not filtered by age groups, but information was extracted in relation to age (when such information was presented in the study) in the full text review phase, in order to ensure including the results of the population in working age. No criteria were set in relation to the country of study. Included papers were classified into areas of application (using the categorization of the patient journey phases). All identified exclusion criteria are detailed in PRISMA flow diagram (Figure 1).

PRISMA flow diagram result of the systematic literature review.
Data extraction
The identified references were imported into Zotero, the bibliographic software used for the selection and screening of studies. The screening of studies included the exploration of titles and abstracts in a first stage, and full-texts in a second stage. The search and final selection of references were carried out in January 2024 by two researchers, who did the work in parallel and independently. Any doubts or disagreements between the two researchers regarding the selection and exclusion criteria were discussed with a third researcher. The methodology followed for data extraction was reviewed and approved by all authors.
The following information was extracted for every paper:
Paper general information: authors and year of publication, title, journal, objective and country of study. Information related with the study methods:
Type of study: depending on the methods used, such as qualitative study (for studies conducting focus groups, for example), Randomized Controlled Trials, Observational studies… Area of study: depending on the type of patients or population involved in the study (e.g., chronicity, ophthalmology, infectious diseases…). Target population description. Randomization methods description (when applicable). Data information: time horizon analyzed, number of participants, % female, age information, digital health technology analyzed and its description (and same for the comparator, if there is one). Application or phase of the patient journey: Access to health care services, prevention, diagnosis, Hospital/clinical/home care, specialist care, Treatment, Valuing and measuring outcomes, behavioral health, and reimbursement decisions. Primary outcomes: here the focus was on any outcomes related with the value of digital health technologies or interventions, including (but not just) Patient Reported Outcome Measures and Patient Reported Experience Measures (PROMs and PREMs). Also, when PROMs and PREMs were evaluated, such as instruments for the measurement of Health-Related Quality of Life or satisfaction instruments, an indicator of the instrument validity was also provided. Methods for analysis: to make sure of the methods being appropriate for the results obtained, and make sure to keep only papers which methods are strong and analysis of enough (moderate or high) quality. Information regarding the study results, discussion and conclusions:
Main results of the paper, with the focus on value elements of digital health technologies or interventions. Discussion of the paper: relevant aspects of the discussion, explaining the contribution of the paper. Paper strengths and limitations, as a complementary measure of the paper quality. Conclusion: summary of the main results, as a complementary field that will help to make the interpretation of what are the main or the most important findings, and, sometimes, what is suggested for further research.
A supplementary file with the data extraction is available as supplementary material.
Analysis
Papers were classified and analyzed in three categories:
Theoretical or conceptual frameworks: papers presenting a theoretical framework, discussion or commentary papers. Empirical works: for papers making some kind of evaluation of a novel Digital Health Technology. Theoretical and Empirical works: papers mixing theoretical and empirical methods. Facilitators: elements that have demonstrated positive value. Barriers: elements that have demonstrated negative effect / value. Neutral or uncertain: elements for which value is neutral or still uncertain, but that literature suggests exploring due to its relevance.
Having extracted the information described above, the results regarding the value elements identified in the paper were classified, again, in three categories:
The analysis conducted in this study identifies, for each type of study (theoretical papers: papers that offer pure theoretical analysis, empirical studies: studies involving qualitative or quantitative data analysis, or mixed methods: for studies combining theoretical and empirical analysis), the elements for VBDH for each phase of the patient journey (access to health care services, prevention, etc.), by type of digital health technology or intervention, and by agent involved. All agents were considered, as a societal perspective was used, and this includes: health centers, stakeholders, providers, patients, health care systems, researchers and society.
Quality and risk of bias assessment
The scale to assess quality of the studies and their risk of bias was specifically elaborated for this study, similar to previous studies (such as Parmar et al.
16
) given that there are too many observational studies and none of the existing tools looked suitable formulating the precise questions to evaluate the quality of the different type of studies. This quality and bias assessment tool was developed based on various quality assessment tools for studies of different designs. The creation of adapted tools for quality and bias assessment is considered a valuable resource for evaluating study quality in systematic literature reviews.
17
The adapted tool used here, assesses internal validity (risk of bias), external validity (applicability/variability), and reporting quality based on a set of questions/statements:
Selection bias: The sample is not representative of the population intended to be analyzed Ecological fallacy: Logical fallacy inherent in making causal inferences from group data to individual behaviors Confounding bias: The analysis does not account for those confounders that are expected to have an effect on the outcome and that have not been accounted for by the inclusion of other. Reporting bias: Inappropriate or inaccurate reporting of aspects of the study Time bias: Bias introduced owing to the timeframe considered Measurement error in exposure variable: Errors related to the exposure variable. Measurement error in health outcome: Errors related to the health outcome measurement.
For randomized control trials, selection bias was assessed by analyzing the appropriateness of sampling methods (power, sample size, blind design, and randomization). Those studies that provided information on the value of digital transformation in the most current context of study were considered to be of stronger quality and -at least- lesser temporal bias. The greater the distance (in years) between the time period analyzed and the time of publication, the greater was considered the risk of time bias. A greater measurement risk in our exposure variables (digital health and the value of transformation) was considered for those articles offering theoretical models not tested by empirical work, or for empirical works where the sample is too small (less than 100 for quantitative studies or less than 20 for focus groups and qualitative interviews).
For each publication, each domain of the adapted Parmar et al. scale was studied and given a score of 1 for a low risk of bias, 2 for a moderate risk and 3 for a high risk. The overall rating was calculated as follows: 1 (strong) is given if none of your domains are classified as weak, 2 (moderate) if up to two domains are classified as weak, or 3 (weak) if three or more domains are classified as weak. Records with an overall rating of 3 were finally excluded, leaving only records rated of strong and moderate quality for the final analysis.
Results
The search strategy (across titles and abstracts) identified 614 potential studies from EMBASE (452), Scopus (162). After removing duplicates 606 abstracts remained for review. Four hundred and ninety-four abstracts were excluded as a result of the titles and abstract screening phase and 112 were selected for full text screening. Documents were excluded in the data extraction phase, some because they did not offer results, others because the full text was not available, and others because they were not of enough quality or highly biased. Finally, 67 studies were included from which the detailed information was finally extracted.
A PRIMSA flowchart representing the process of selecting eligible sources for this study is presented in Figure 1. The reasons for exclusion in the screening and eligibility phases are detailed in the PRISMA. Reference lists of primary research reports and previously published systematic reviews with a focus on digital health and/or VBDH were also reviewed in an attempt to identify additional studies. Data extraction and final risk of bias and study quality assessment and scores are available as supplementary material.
Among the 67 studies fully extracted, there were 14 theoretical studies, 40 empirical studies and 13 studies combining theoretical and empirical methods. By agent type, and for each of the phases of the patient journey, the elements of VBDH were identified, and are now summarized. Each paper was allocated to one phase of the patient journey, depending, mainly, on the type of study, on main objective of the paper, and on the study setting. The areas of application identified in the analysis are now done, for each type of agent and by literature category.
Areas of VBDH identified for health care organizations
Only one paper of the theoretical literature identified VBDH elements of access to health care services for health organizations, analyzing the value of Health Information Technologies (HIT). 18
Areas of VBDH identified for stakeholders
One theoretical study found relevant VBDH elements, related to access to health care services, for stakeholders, analyzing the value of eHealth. 19
Two studies, within the mixed methods studies identified, found VBDH elements related to patients’ treatment for stakeholders, analyzing the value of Electronic Medication Adherence products and a disruptive Digital Health Technology.20,21
Areas of VBDH identified for providers
Related with access to health care services, theoretical works found the following VBDH elements. Six studies found specific value elements for providers, related with access to health services, six of them finding elements of positive value. Different technologies were analyzed, including HIT, Emerging digital health care practices, smart nursing, AI and big data, and High Definition Video-to-Video services,18,22–26 one of them finding an element of negative value, related with the burden of health care professionals. 18 Two mixed methods papers found VBDH elements, analyzing digital health communication technologies and Electronic Medical Records.27,28 Related with prevention, one empirical study identified VBDH elements for providers, of analyzing a Quitline-like phone counseling and Telemedicine integrated into Primary Care. 29 Related with diagnosis: One theoretical study analyzing imaging analysis technologies 30 and two empirical studies, on CT, imaging were identified.31,32 Related with hospital/clinical/home care, two theoretical studies identified VBDH elements for providers, analyzing mobile health and smart home devices and the Internet of Medical Things (IoMT).33,34 In addition, one empirical study, studied the value of EHR. 35 Related with specialist care, three empirical studies identified VBDH elements of telemedicine, a theory driven digital intervention, and Digital Health Monitoring Platforms for specialists.36–38 Related with treatment, one empirical study analyzed digital health technologies in general, 39 and one mixed method's paper analyzed the value of Electronic Medication Adherence products. 20 Related with the valuation and measurement of outcomes, twelve studies were found identifying VBDH elements for providers, analyzing very different digital health technologies including a Virtual Reality App, Digital Monitoring Adherence systems, Social media-based health education, AI kit, mobile apps, online telehealth, Imaging related machine learning, teleconsultation, text messaging, Machine learning techniques applied to PROMs and Digital Communication Technologies.40–51 In addition, one study, among the mixed methods included studies, identified negative VBDH elements of Electronic Health Records for this area. 44
Areas of VBDH identified for patients
Related with access to health care services: nine theoretical studies were identified, discussing VBDH elements for different types of DH technologies, including HIT, Emerging Digital health care practices, Smart nursing, AI, High Definition Video-to-Video services and eHealth.18,19,22–26 Among the empirical studies identified within this area of access to health care services, two studies were found, both analyzing VBDH elements of mHealth.52,53
Among the mixed methods studies, three studies were identified: One study, analyzing wearables, 54 a second study, analyzing a cloud-based referral platform 55 and the third study, analyzing an Integrated Digital Patient Education system. 56
Related with prevention, two empirical works identified VBDH elements for patients: one study, analyzing teleophthalmology for screening. 57 The second one, analyzing a Quitline-like phone counselling and Telemedicine integrated into Primary Care. 29
Related with diagnosis, one theoretical work was identified on the VBDH for patients of imaging analysis. 30 Empirically, one study, analyzed Breast Imaging technologies. 58
Related with treatment, three empirical papers were identified. One studied integrated care with telemedicine support. 59 The second paper, studying Digital Health Technologies. 39 The third paper, analyzing an interactive telephone intervention. 60
Related with the valuation and measurement of outcomes, thirteen empirical papers were found, identifying value elements, analyzing: a VR App, 40 telerehabilitation, 61 telehealth education, 62 a digital intervention for online help seekers, 63 a care coordination digital intervention, 64 a Digital Monitoring Adherence system, 41 a mobile phone text messaging self-managing support system,65,66 an evidence-based SDM aid, 67 a computerized intervention, 68 teleconsultation, 48 an open medication system via iPad, 69 and a Digital Communication Technology. 51 One paper among the mixed methods papers, analyzed a eHealth intervention of integrating self-report in Electronic Patient Records (eRAPID). 70
Related with behavioral health, one study, analyzing the use of wearables. 71
Areas of VBDH identified for health care systems
Related with access to health care services, seven theoretical papers identified VBDH elements for health care systems, analyzing: smart nursing, 23 Artificial Intelligence (AI), 26 High Definition Video-to-Video Services,25,72 eHealth in primary care in high and low-resource settings, 19 an electronic mindfulness-based intervention (eMBI). 73 Among mixed methods papers, one paper analyzed a cloud-based referral platform. 55
Related with diagnosis, one study among the mixed methods included studies, analyzed the value of telehealth services. 74
Related with the valuation and measurement of outcomes, one empirical paper was found, analyzing a Digital Communication Technology. 51 In addition, two papers among the mixed methods papers, were found. One, analyzing an eHealth intervention of integrating self-report in Electronic Patient Records (eRAPID), 70 and the second paper, also on Electronic Health Records. 44
Areas of VBDH identified for researchers
Theoretical works identified some positive values in the area of access to health care services for researchers: One study, discussing smart nursing, 23 the second paper, on smart home devices and the Internet of Medical Things, 33 and the third paper, discussing an electronic mindfulness-based intervention (eMBI). 73
Related with treatment, one empirical work studied the value of Digital health Technologies. 39
Areas of VBDH identified for society
Theoretical works identified elements of VBDH for the society related with access to health care services. Technologies analyzed include learning health systems, 75 emerging Digital health care practices, 22 telehealth services 72 and eHealth. 19
Related with the valuation and measurement of outcomes, three empirical papers were found, analyzing a telemedicine outreach system, 76 an mHealth ROADMAP platform, 77 an HPV Cancer Free App. 78
Related with reimbursement decisions, one theoretical analyzed telehealth and the value of digital connectivity. 79
Areas of VBDH identified for patients and providers
Theoretical works found some VBDH elements for both, patients and providers.
For the application area of access to health care services one study was found analyzing emerging digital health. 22 Another study, on Artificial Intelligence. 26 The third paper identified, discussed high definition Video-to-Video services. 25 Finally, the fourth and last identified paper, discussed eHealth. 19
Among empirical studies, some studies were found identifying VBDH elements for patient and providers in the application area of specialist care. These studies include the analysis of telemedicine (virtual visits), 36 a theory driven digital intervention, 37 or Digital Health Monitoring Platforms. 38
One study among the mixed methods studies captured VBDH elements for patients and providers, in the application area of valuation and measurement of outcomes. The study analyzed EHR. 44
Areas of VBDH identified for patients and health care systems
Theoretical works found VBDH elements for patients and health care systems, in the application area of access to health care services. One of the studies analyzed eHealth. 19 Another study, discussed health sensors, smart home devices and the Internet of Medical Things. 33
Related with valuation and measurement of outcomes, theoretical works finding VBDH elements for both, patients and Health Care Systems, were also identified: One discussing an electronic mindfulness-based intervention (eMBI), 73 a second one, analyzing a care coordination intervention, 64 and a third study, analyzing a computerized intervention. 68
Among the mixed methods studies, one paper also found VBDH elements of personal Digital Health Profile (DHP), for patients and health care systems, for the area of prevention. 80 In the area of treatment, a study found VBDH elements for health care systems and researchers analyzing a digital self-management intervention. 81
Elements of VBDH identified by the literature and conceptual framework by literature category
The detailed results and analysis for theoretical studies, empirical studies and mixed methods studies are detailed in Table s1–3, respectively.
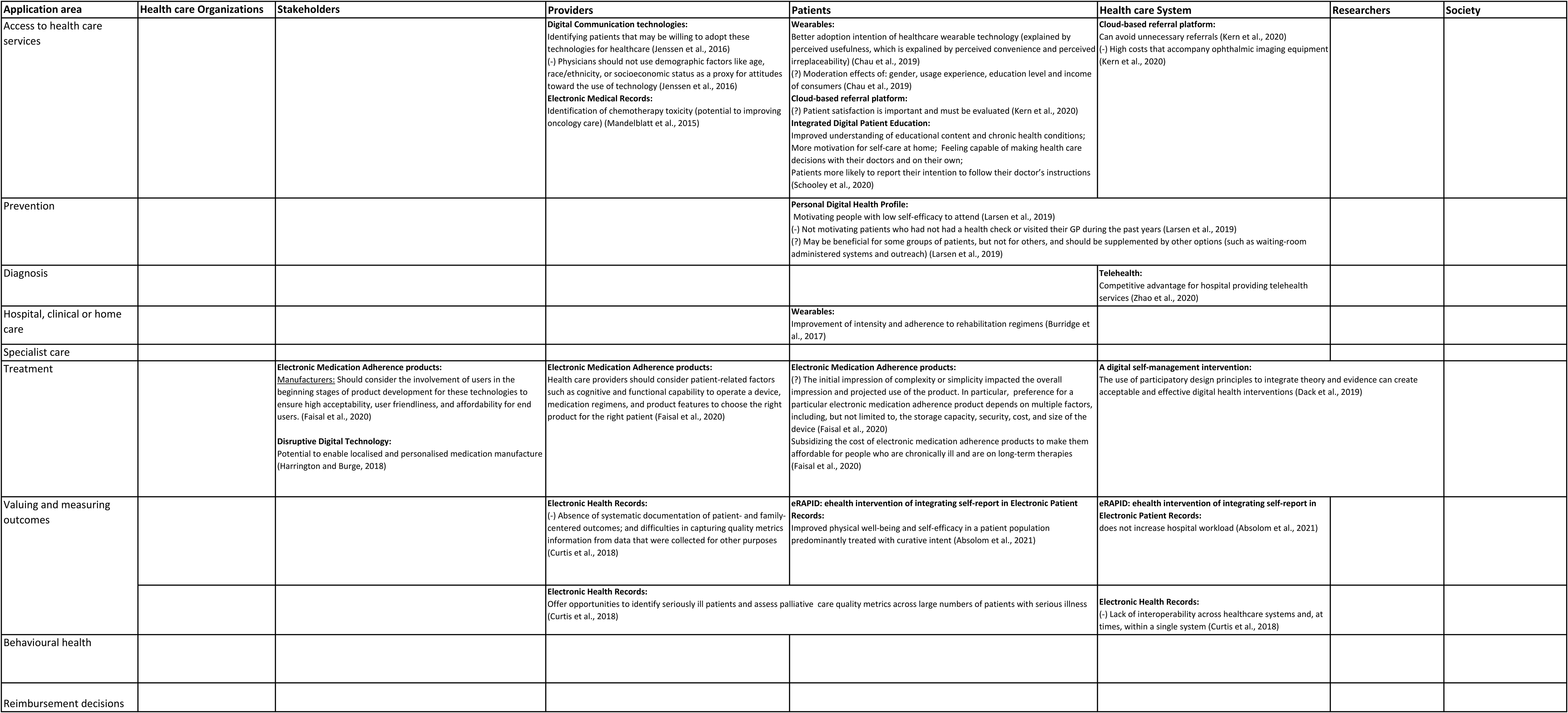
Tables 1–3 have also been of value for generating a conceptual framework, represented by Figures 2–4. The framework provides a list of VBDH elements, by type of agent and application area (phases of the patient journey) according to theoretical literature, empirical and, mixed methods literature, respectively.

Framework of value elements by agent type and application area of the patient journey according to theoretical literature.

Framework of value elements by agent type and application area of the patient journey according to empirical literature.
Value elements by agent type and application area of the patient journey according to mixed methods literature.
Summary of theoretical included papers included: content and main results.

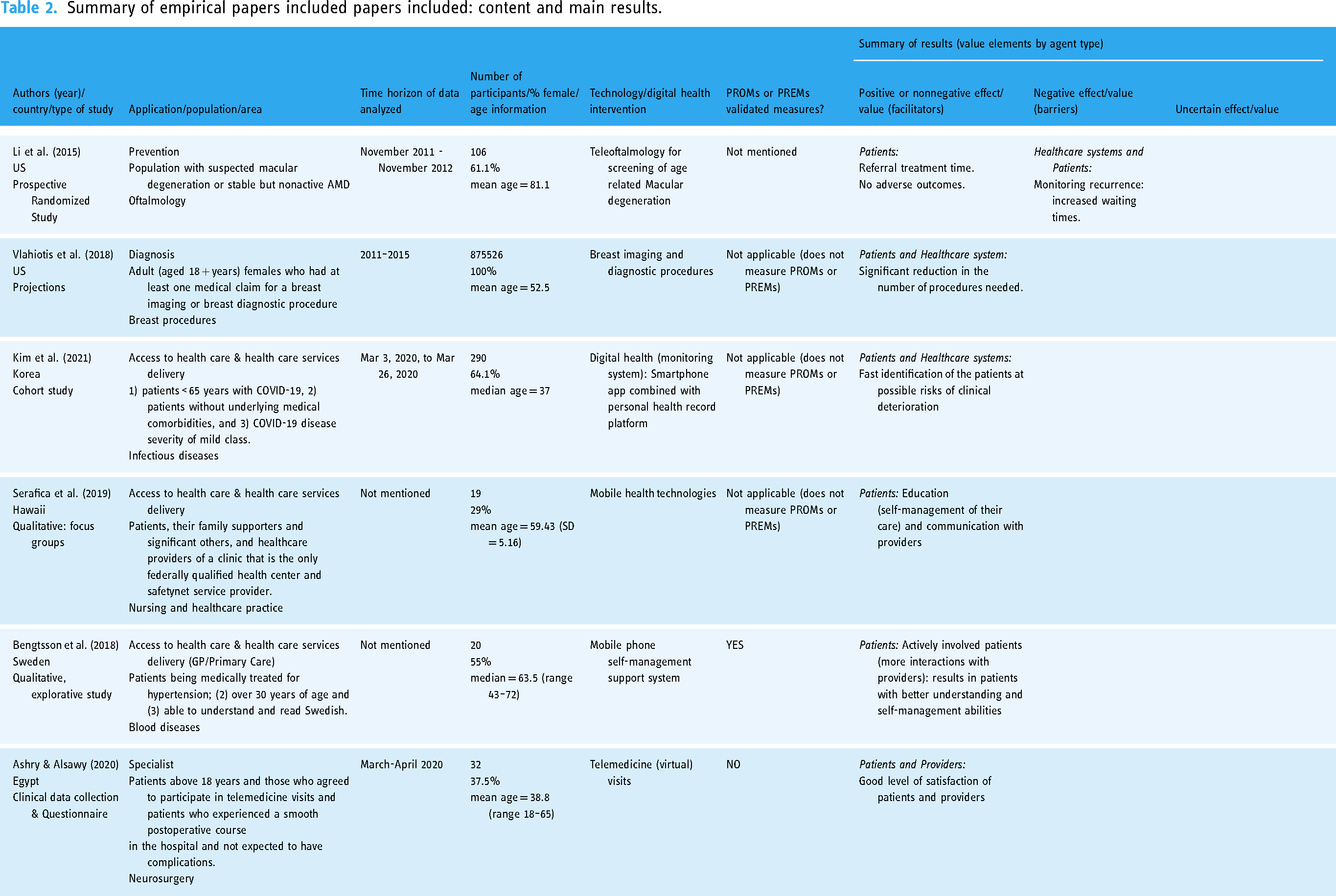
Summary of empirical papers included papers included: content and main results.
Summary of papers mixing theoretical and empirical methods included: content and main results.

Discussion
This systematic literature review helped identifying, from the most relevant sources published in recent years, those elements that, according to theory, would be relevant to creating digital health value. Through the extraction of information from the reviewed sources, literature was synthetized in a way that VBDH elements can be identified at different levels (by phases of the patient journey), for different agents (in the society) and by type of digital health technology and intervention.
The review also helped identifying the elements that are actually being used to measure the value of digital health empirically. For example, to generate value in the access phase and provision of health services, theoretical and empirical literature coincide in elements such as research, education, patient-centered care, or trust. While theory proposes as an important element the government's regulatory and acting capacity, the empirical works reviewed do not present any type of measure that correspond to this approach. In relation to the diagnosis phase, for example, only the theoretical literature finds as key elements for this phase of the care process the importance of models by pathologies or pathological subspecialties, and of agile transmission, centered on the patient, 30 something that has not yet been studied empirically. Related with the prevention of diseases, hospital care and treatment phases, this study did not find any elements in the theoretical literature, while empirically the existence of certain elements that serve to demonstrate the value of digital health in these areas is being demonstrated. On the valuation and measurement of health outcomes, theoretical literature suggests the need for restructuring of medical practice, which should tend towards more flexible implementation models, 73 while the empirical literature reviewed does not find anything in this regard. However, coinciding elements in this phase are the importance of research (in this case focused on data collection, especially PROMs and PREMs), the importance of feasibility and confidence in new technologies, and the importance of information systems that allow identifying barriers to optimize the effectiveness of interventions based on new health technologies.
There were some common elements found between several of the different phases of the care cycle, such as the importance of patient-centered care. However, no theoretical article focused on the prevention and treatment phases has been identified, suggesting further research could focus on identifying such VBDH elements. Future research should study this context, as these phases of the patient's care cycle should be given the same importance than any other phase.
The main contribution of this study is to offer the VBDH elements identified in the literature (separately by theoretical and empirical works), by type of agent and for the different phases of a patient journey. Previous publication exists, providing a framework for defining Value-Based Health Care. A paper published recently, offers a strategic framework for VBHC implementation to achieve better patient outcomes. 82 An umbrella review was done for the value of mobile health applications used in patients with mental health problems. 83 However, no framework has been proposed yet to identify specific elements of VBHC in the context of Digital Health. Another paper reviewed how digital transformation can help achieve VBHC, 84 supporting the fact that Determining “value” may require a system-level model and framework to understand better the distributed components that are interrelated by complex processes within a healthcare system. Something that has already been a concern by researchers in the field. 85 Therefore, this systematic review is a novel and useful piece of information for researchers who may want to develop, for example, new instruments of patient reported outcomes or experiences regarding the use of different digital health technologies. The framework proposed, result of the synthesis of information extracted, offered by this review, despite its complexity due to the multiple levels of analysis considered, identifies areas where no VBDH elements are identified, and therefore could also be useful for researchers who may be wondering what areas of application are still in need for further research in this sense. Finally, the data extraction could also be used as a data lake (easy to update) of VBDH interventions, for example, helping in the design of research projects in different areas of application.
This study has limitations. The main limitation is on the subjectivity of the interpretation of results offered by the literature, for example, when allocating the value of a digital technology to a specific phase of the patient journey or for a particular type of agent. However, the interpretation of the results was reviewed by all authors, and the final version has the agreement of all authors of this study. Any other limitations are natural of the methods for conducting any systematic literature review. It may be the case that relevant papers have been excluded in the screening phases of the review, and also it is possible that evaluating the quality and risk of bias of the selected studies, some papers qualified as weak (and thus, excluded) could be relevant papers for the purposes of this study.
Conclusion
This systematic literature review provides a framework composed of the main elements, for each phase of a patient's care cycle, that generate value for digital health technologies and interventions. Furthermore, contrasting the elements identified in theory and empirical work in the context of VBDH, the review shows a list of elements that coincide between both types of literature, as well as some existing gaps in the literature. This work, therefore, offers elements that build up a strategic framework, with empirically observed elements for VBDH, as well as suggests future lines of research that should be priorities for progress in VBDH. It provides researchers of a source, for consultation and development of future research projects, that might be useful for academic researchers as well as a tool to be used by clinicians in the clinical practice or by policy makers in decision making processes in the context of digital health. Conditioned to the existence of instruments to measure the value of these elements, this is a first step for improving the measurement of the value of digital health.
Supplemental Material
sj-xlsx-1-dhj-10.1177_20552076241277438 - Supplemental material for Value-based digital health: A systematic literature review of the value elements of digital health care
Supplemental material, sj-xlsx-1-dhj-10.1177_20552076241277438 for Value-based digital health: A systematic literature review of the value elements of digital health care by Marisa Merino, Jaime del Barrio, Roberto Nuño and María Errea in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241277438 - Supplemental material for Value-based digital health: A systematic literature review of the value elements of digital health care
Supplemental material, sj-docx-2-dhj-10.1177_20552076241277438 for Value-based digital health: A systematic literature review of the value elements of digital health care by Marisa Merino, Jaime del Barrio, Roberto Nuño and María Errea in DIGITAL HEALTH
Footnotes
Conflicting interests
ME has received consulting fees for her working time. Marisa Merino and Jaime del Barrio belong to ASD but their authorship has not biased the results obtained in any way.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Asociación Salud Digital.
Authors’ Contributions
MM and JdB conceived the study idea. The research question was refined by ME. All authors agreed on the research objectives and study protocol. ME searched the databases for literature and MM and ME screened the abstracts. ME reviewed full texts, supervised by MM and RN. ME wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Guarantor
MM
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.