
Abstract
To evaluate perceptions of a laryngeal cancer fact sheet amongst people with direct experience of the disease and its treatment. A mixed methods study (questionnaire and interview) evaluating the information resource was conducted across two institutions. In total 20 participants responded to the questionnaire. Overall participants reported the information resource was detailed and understandable. Insufficient information was provided on: impact on family in eight participants (40%); impact on work in six (33%); and, second opinions and long-term side effects in five (25%). The majority (67%) wanted a large amount of information with the preferred source being one-on-one meetings with their doctor. The thematic analysis identified three main themes: preferences for information, self-management; and, information sources. People with direct experience of laryngeal cancer and its treatments reported the information resource was comprehensive and clear. There were some gaps in the information provided, particularly related to survivorship issues.
Introduction
Communication of health information is a deceptively challenging task. There are several variables that affect communication such as an individual’s information needs, their information preferences and health literacy, the quality of health care professional (HCP) communication, and the quality and complexity of information. Commonly insufficient attention is paid to these factors, resulting in failure to provide information suitable for patients and ultimately to the detriment of patient understanding, preparation, and subsequent health outcomes. 1
In taking advantage of the world-wide web, individuals, healthcare professionals, groups, and organisations have generated myriad healthcare related information pages, some of dubious quality. 2 While patients and families are increasingly searching for health information on the internet. 3 The quality of head and neck cancer information has been assessed and been found wanting in many instances, particularly the readability and health literacy levels targeted. 4 Concerns have been identified regarding the quality of content, including: explanation of treatment and risks and benefits of treatment options. 5 The quality of written information can impact patient perceptions of treating doctors’ professionalism and attitudes to their care. 6 With these concerns about the available information sources for people diagnosed with head and neck cancer, a new online information resource directed toward this population was developed by an expert panel called Beyond Five (www.beyondfive.org.au).7,8 This novel laryngeal cancer fact sheet was selected for assessment due a previous study on patient experience on unmet information needs which produced a tailored fact sheet to patients. 8
The web-based resource incorporates material delivered online or downloadable in the form of fact sheets. In this study, we aimed to evaluate perceptions of the laryngeal cancer fact sheet amongst people with direct experience of the disease and its treatment.
Methods
Study design
A mixed methods approach was used to address the aims of this study. It incorporated a cross-sectional survey to assess patient perceptions of the laryngeal cancer fact sheet and semi-structured interviews with participants to explore their perceptions in greater depth. The laryngeal cancer fact sheet description is described in the Appendix A. The design and reporting of this study was consistent with the consolidated criteria for reporting qualitative research (COREQ). 9 Ethical approval was obtained from the Sydney Local Health District Research Ethics Committee – RPAH zone (Protocol No X16-0486 & HREC/16/RPAH/696).
Participants
People were eligible to take part if they: (i) were aged 18 years or older; (ii) had a confirmed diagnosis of laryngeal cancer; (iii) spoke English sufficiently well to complete the interview without an interpreter; and, (iv) had no cognitive impairment precluding the ability to provide informed consent. Participants were recruited during standard of care visits at the Chris O’Brien Lifehouse and Westmead Hospital, Sydney, Australia. At all sites a member of the treatment team would inform potential participants about the study, provide them with brief written information about the study, and obtain their consent for the researchers to contact them.
Procedure
Recruitment and data collection took place between April 2018 and April 2019. Participants read the information statement which described the study and completed a written consent which was either returned to a member of their treatment team or via reply paid postal mail to the research team. Once written consent was received the participants received the laryngeal information sheet either from a member of the treatment team or via postal mail.
The 16-item questionnaire was completed by participants and returned by postal mail. A subgroup of participants were invited to participate in a qualitative substudy. These participants confirmed verbal consent to participate at the state of the semi-structured interview ( Appendix C ), which then explored participants’ perception of the fact sheet and its relevance to their cancer experience. The semi-structured interviews were completed via telephone after the questionnaire had been submitted at a time convenient to the participant. Interviews were audio-recorded and transcribed verbatim, with the median duration of interview being 11 min (range 4–22 min)
Questionnaire
The 16-item, self-report questionnaire consisted of items covering: treatment received, health literacy level, aspects of the fact sheet (adequacy, readability, and delivery of information), information preferences, and feedback. The full questionnaire is provided in appendix B. Health literacy screening questions investigated: (i) self-rated ability to read information from the hospital; and, (ii) confidence filling out medical forms. 10 Preferences regarding the adequacy of information were rated on a 3-point scale: ‘not enough’, ‘the right amount’, or ‘too much’. The understandability of information was rated on a 3-point scale: ‘easily understood’, ‘understood’, or ‘could not understand’. Regarding information preference, patients selected from one of the following options: ‘I want only the information needed to care for myself properly’, ‘I want additional information only if it is good news’, or ‘I want as much information as possible, good and bad’. The format of information provision was assessed by asking ‘where did you get most of your cancer information?’ with six response options to select from. The last question allowed for open-ended responses about potential improvements to the factsheet.
Data analysis
Descriptive statistics were used to summarise survey responses using Microsoft Excel for Office 365 MSO (Redmond, Washington, United States). Qualitative data were subjected to thematic analysis using a framework approach, involving:
(i) Familiarisation with data: completed by three authors (JJ, HD, HS) who read the transcripts multiple times as interviews were completed.
(ii) Developing a coding framework: the three authors developed a framework of codes grouping them under thematic headings independently and then collaboratively.
(iii) Indexing: Themes were reviewed and revised, and any inconsistencies discussed and resolved.
(iv) Charting: Transcripts were coded using the framework and a thematic matrix chart was created using Microsoft Excel, with each participant being assigned a row and each subtheme a column.
(v) Mapping: Participants’ experiences were discussed, contrasting the similarities and differences in responses.
Thematic saturation was reached after 12 participants as no new themes were identified in three consecutive interviews, however as a further four interviews had been arranged these were completed as planned, and used to member check the themes identified and demonstrated complete thematic saturation. 11
Results
Sociodemographic and treatment characteristics
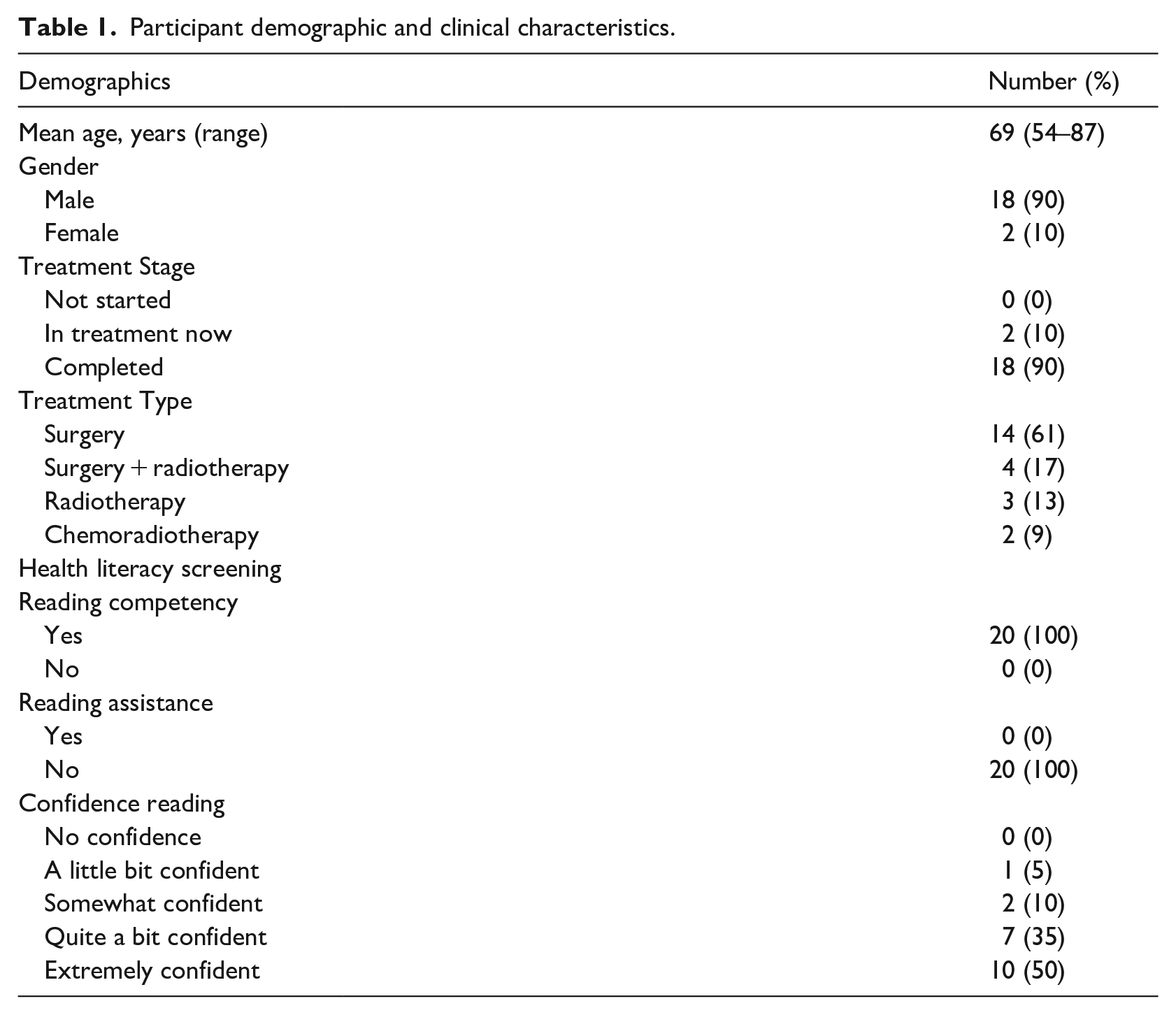
Clinicians invited 56 people previously diagnosed with and treated for laryngeal cancer to take part in the study and a total of 20 people were recruited (response rate 36%). Of these, 16 subsequently agreed to take part in an interview. Participants’ median age was 64 years (range 54–87), with the majority being male (18 vs 2). The sociodemographic and clinical characteristics of the participants are summarised in Table 1. Most participants had been treated with surgery alone (14 patients; 61%), surgery + radiotherapy (4; 17%), radiotherapy (3; 13%), or chemoradiotherapy (2; 9%).
Participant demographic and clinical characteristics.
Health literacy levels
The sample demonstrated higher levels of health literacy, with 17 people (75%) indicating ‘quite a bit’ to ‘extreme confidence’ reading information from the hospital. While all 20 participants (100%) reported not needing help reading the fact sheet.
Quantity of information in the fact sheet
Participants reported the ‘right amount’ of information was contained in the fact sheet regarding: cancer care team and treatment options 19 (95%), diagnosis, investigations and signs/symptoms 18 (90%), staging, side effects and supports available 17 (85%), and causes of laryngeal cancer and impact on mental health 16 (80%). Participants reported ‘Not enough’ information on impact on family eight participants (40%), impact on your job or work 6 (33%), getting a second opinion 5 (25%) and long-term side effects 5 (25%). The results are summarised in Figure 1.
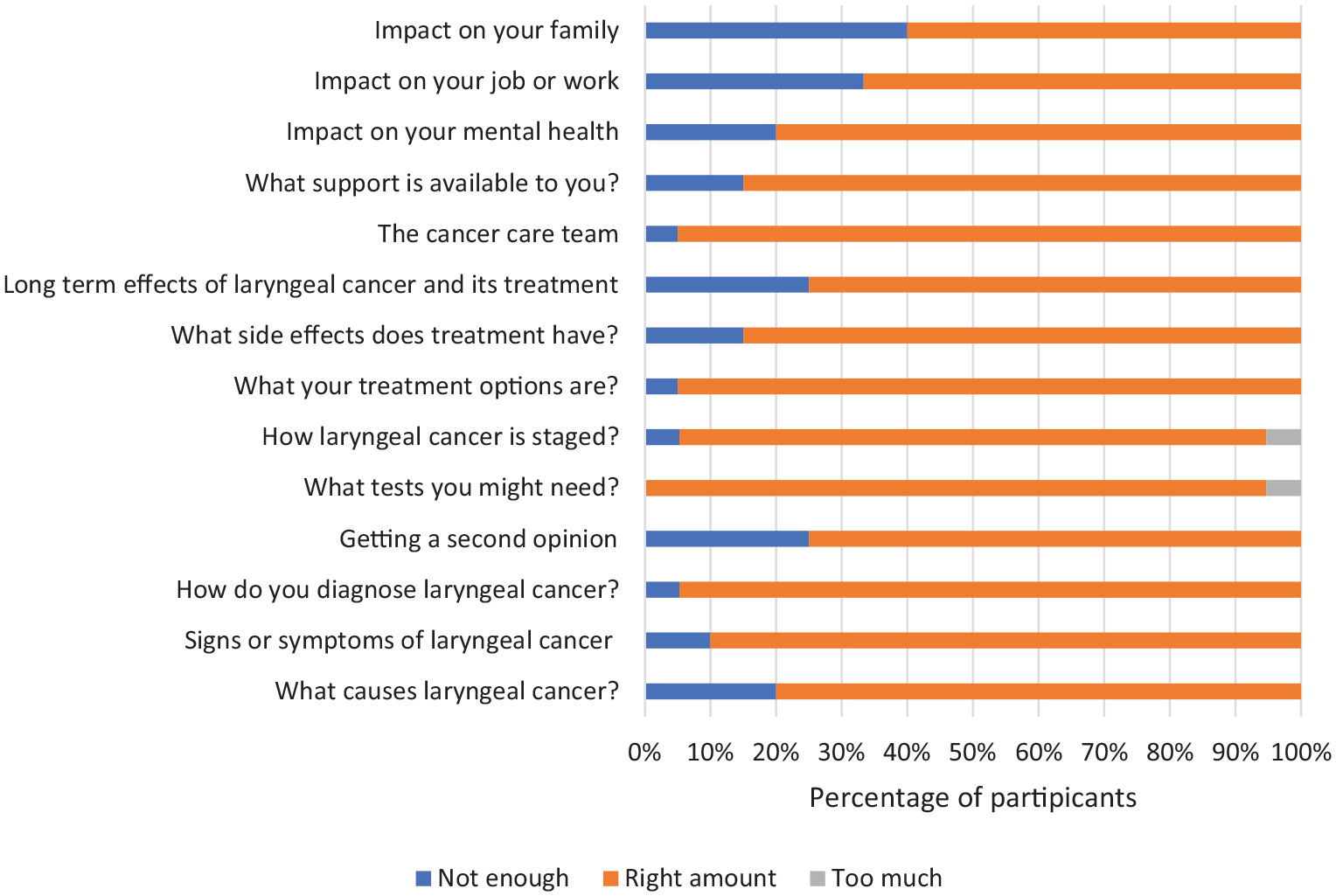
Adequacy of laryngeal cancer fact sheet information.
How understandable was the information?
The information was reported to be easily understood in all the topics listed above by 95% of participants. One participant reported difficulty understanding the long-term side effects of treatment (Figure 2).
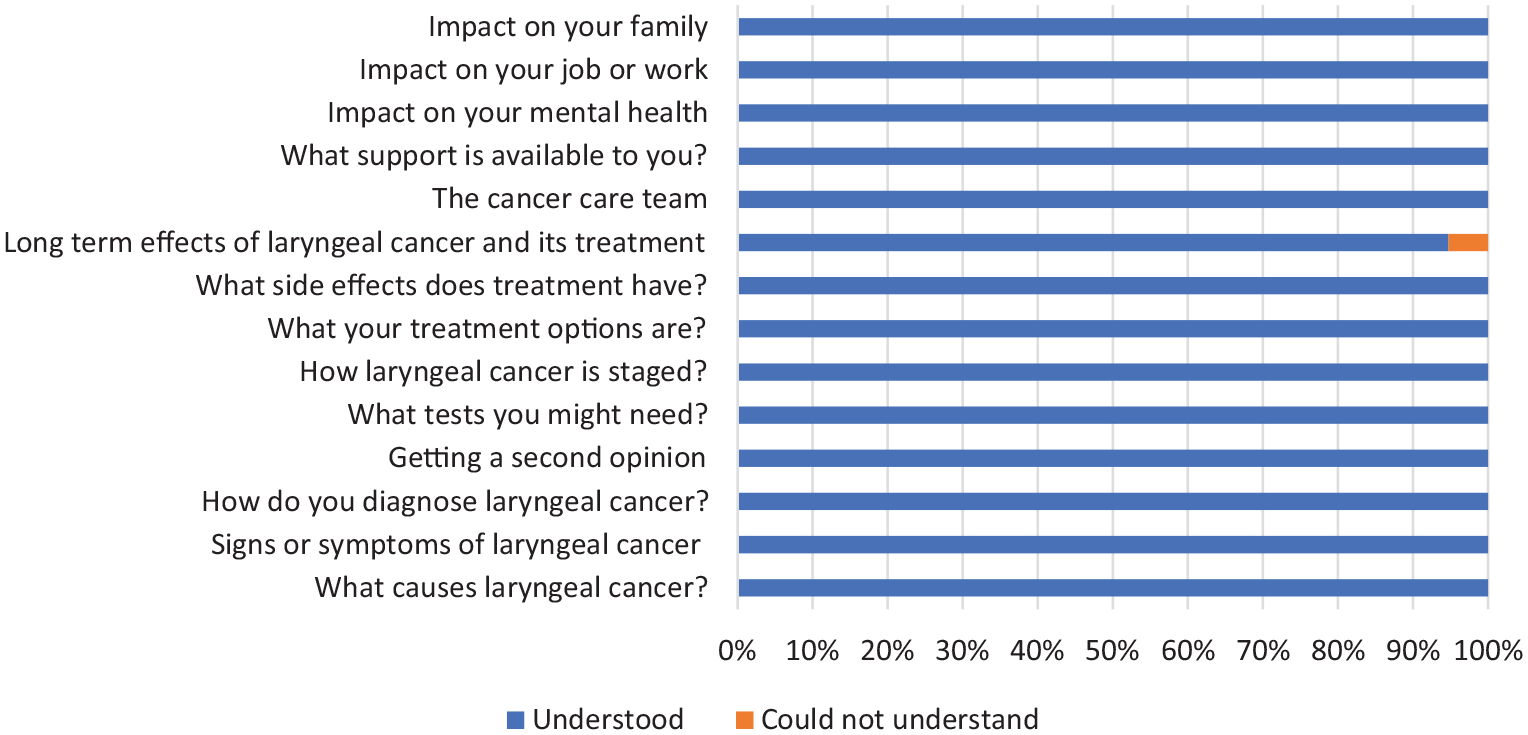
Understandability of laryngeal cancer fact sheet information.
Content and resourcefulness
Most participants (16, 80%) reported the information resource covered everything they wanted to know (Figure 3). Topics participants found helpful were: information on causes of HNC; diagnosis; cancer staging; treatment; and, acute side-effects. Participants stated the fact sheet was written in plain language and avoided medical jargon. Four participants (20%) reported deficiencies in the information resource, including: impact on work and family; obtaining a second opinion; and, long-term effects of cancer and treatment (speech, lymphoedema, swallow, removal thyroid, parathyroid and lymph nodes).
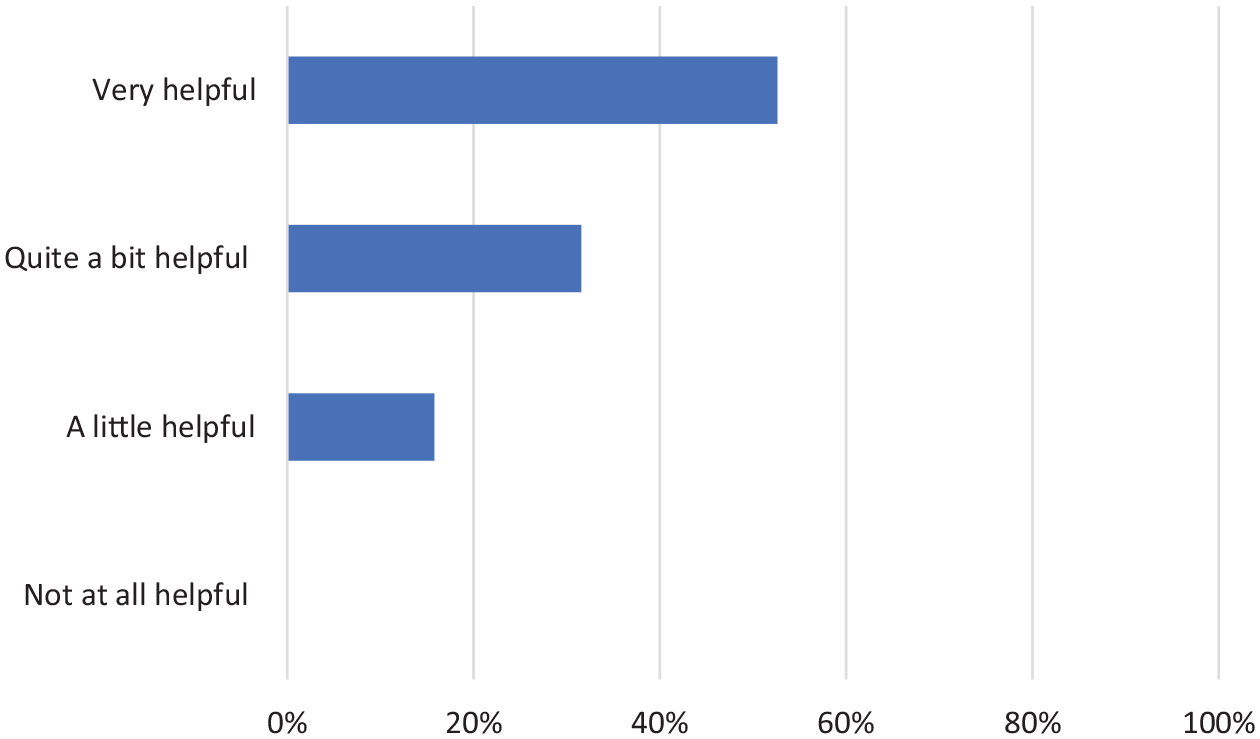
The usefulness of laryngeal cancer factsheet.
Design and layout
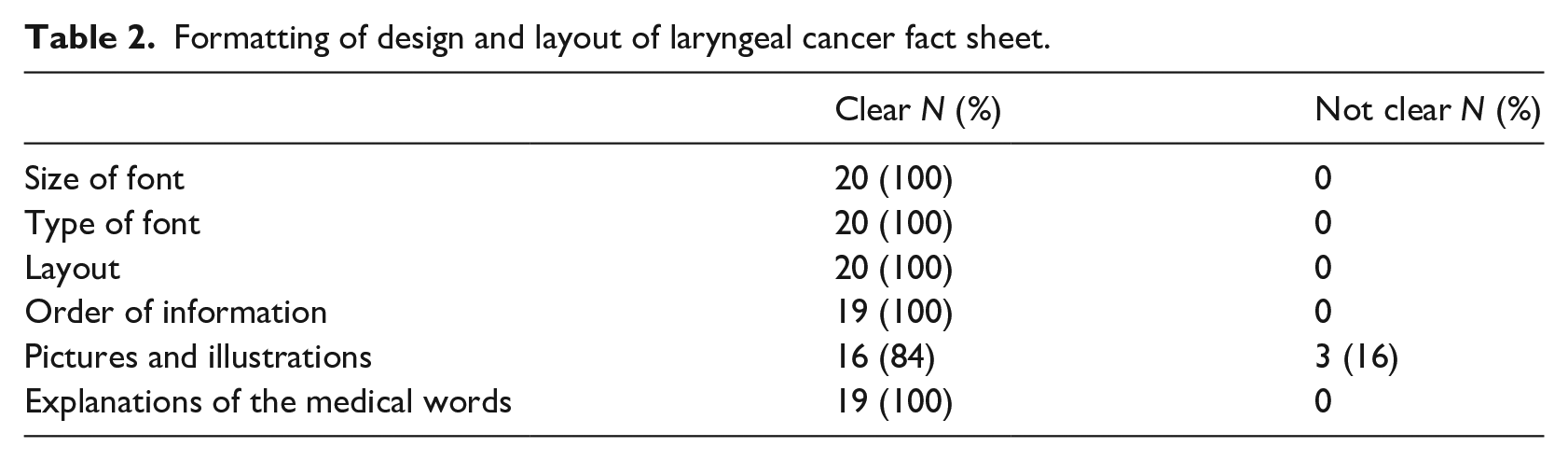
The fact sheet was reported as clear to all participants in three of the four areas assessed: size of text; font; layout; and, definition of medical terminology (Table 2). However, three (16%) reported the picture/illustration (Figure 4) unclear. Suggestions to increase clarity of the resource included increasing the font size.
Formatting of design and layout of laryngeal cancer fact sheet.
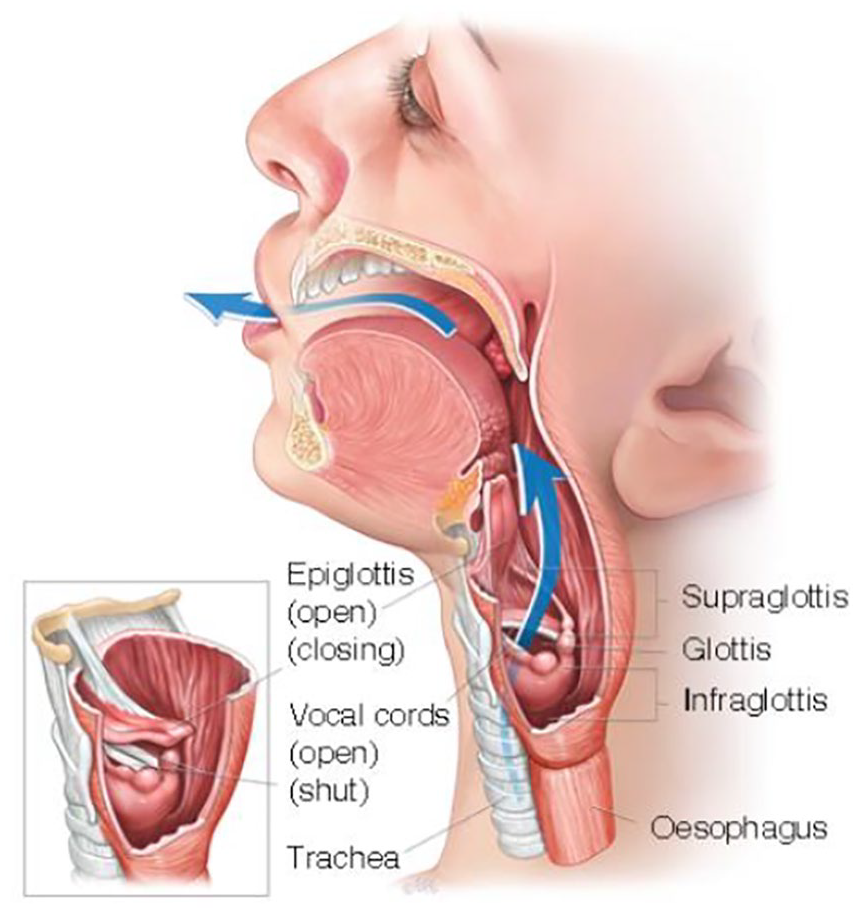
Beyond Five laryngeal cancer fact sheet anatomical illustration.
Mode of information presentation and impact on participants
The most favoured modality of information presentation was written (10 participants, 50%) followed by written plus internet-based material (9, 45%), and finally internet alone (1, 5%). After reading the information resource, most participants (15, 88 %) felt prepared for their cancer and treatment, one (6%) felt anxious and one (6%) depressed. Participants indicated they would be more prepared for treatment and post-treatment by talking to their doctor in conjunction with the fact sheet, having a close relationship with their HCP, and receiving an explanation of the risks of treatment and non-treatment.
Preference and source of information
Most participants (18, 90%) indicated a preference for as much information as possible, whether good or bad. The remaining two (10%) only wanted information needed to care for themselves properly. Multiple modalities were used to obtain information: one-on-one meeting with doctor (16), followed by fact sheet – paper or online (3), followed by other written information (2), other internet information (2) and internet-based videos (one patient).
General feedback
A small number of participants responded to the open-ended questions indicating the information resource was informative. Interestingly, one participant recognised it was a ‘condensed variant of the website [electronic laryngeal cancer factsheet accessible on Beyond Five website]’. Further information was wanted on laryngeal laser treatment in the fact sheet.
Thematic analysis of interviews
A total of 16 participants completed interviews and their characteristics are detailed in Table 3. Thematic analysis of the semi-structured interview transcriptions identified three main themes: information preferences; self-management; and, information sources.
Characteristics of participants completing interviews.
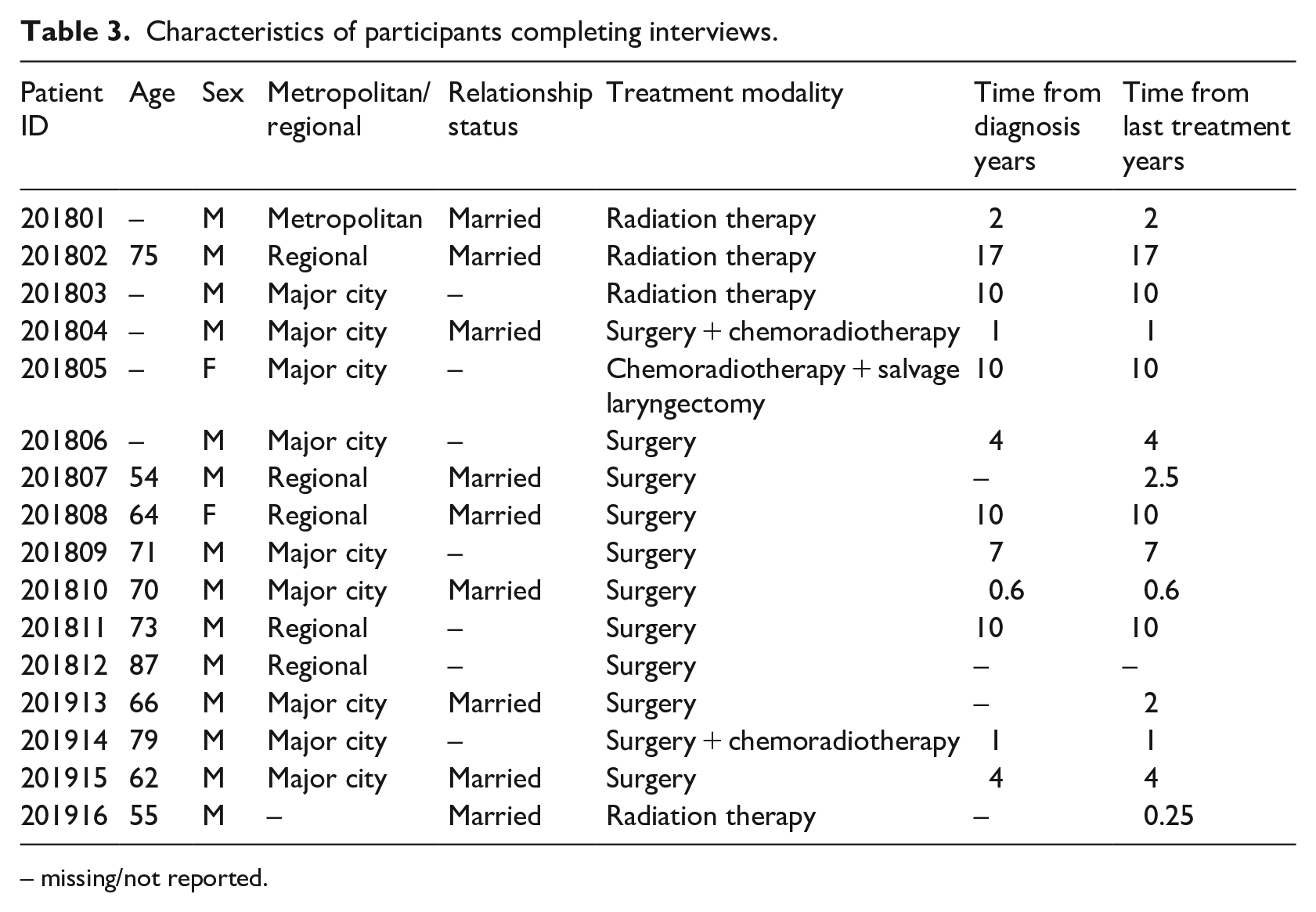
– missing/not reported.
Information preferences
Participants largely concurred that the information provided was thorough, covering the breadth of topics relevant to laryngeal cancer:
“The information factsheet is extensive and covers the majority of laryngeal cancer topics” Participant Identifier (PID) 201804
In contrast, some felt there was too much information, wanting a more succinct resource:
“You are better off making it shorter and snappier than to have them get a third of the way through it and I have still have this much to read” PID 201809
The accessibility of information was a subtheme identified, with participants generally feeling that making information available via the internet was a good thing. Doing so increased accessibility, making information available to more people.
“Look now I am not computer literate. The majority of the population it would be better to be available on their smartphones or their laptops or other media they have” PID 201809
However, they did note the limitations of this information, particularly in the lack of human connection.
“But I say if you want to know more about the possibility of what you have then nothing beats face-to-face. You need the warmth and connection I suppose when you’re looking into their eyes” PID 201915
The issue of usability of the information resource was identified as important to participants. Overall the information resource was read in isolation from other information, with participants indicating it was easy to follow and a useful reference tool. Although, some felt it required effort to process the information.
“The verbal information provided by the medical team was clear and the online resources and factsheet could be used as a reference to go back to between consultations and aspects of treatment” PID 201804
“The document is one of those things. You need to sit down in quiet space and digest” PID 201810
The contents of the information resource gave patients a hope their disease can be cured.
“And when you read all these things, it gives you a lot of hope it can be cured and you can come back to normal again.” PID 201916
The timing of information was noted as important, with most participants expressing a preference for receiving the resource at the time of diagnosis.
“Oh, I would have liked this at the very beginning when I was first diagnosed” PID 201805
However, there was some variability in participant views with others suggesting diagnosis was not the optimal time to receive detailed information.
“Ah, I would have read it much differently and gained much more from it day two of treatment than before” PID 201802
Self-management
The participants indicated information could be used to support self-management during treatment and beyond cancer.
“It gave me the idea of what to maybe expect and side effects and things like that.” PID 201801
“All the information about the swallowing function and what to expect after the surgery was very helpful.” PID 201804
“. . .it was great to read that and find out exactly what the process was, what happens from the treatment, the problem that is causes, and, you know, people go through it.” PID 201808
Information sources
There were four subthemes on sources of information: videos being useful: resources outside of the laryngeal cancer factsheet; risk of resources; and, people as resources.
The videos included on the Beyond Five website were important in helping participants process information and seemed to be more effective at doing so than the static diagram in the printed resource.
“The diagrams within the resource are not as beneficial as the online videos which portray patients and their experiences with laryngeal cancer” PID 201804
“Particularly the diagrams, were some of those were animated? I think they were. I found that very helpful in terms of understanding that anatomy.” PID 201810
Going beyond the information and videos provided, there were examples of videos of their procedures that they found useful in understanding the surgery and its potential impacts.
“My doctor at the time made a video of my vocal cords and gave it to me to take home to watch” PID 201806
Participants reported using any resources available to them, which included: internet-based information and online forums, family members, and other written information.
“My sister is an anaesthetist. So I have access to medical information as well” PID 201915
“ah, I picked up another one Living well after cancer. The other stuff (impact on job or work, impact on family) from the booklets that was published by the Cancer Council” PID 201916
Patients were concerned about the misinformation online outside of the laryngeal cancer factsheet.
“I don’t go online to get information, if there is something medically or you know there is something wrong with me. You know I think there is too [much] misinformation” PID 201805
“When do you stop? And then you go to Dr. Google, finding out a whole lot of bad or not necessarily accurate information” PID 201915
Participants recognised sometimes the best information resource was a person with direct experience of the disease and surgery they were to have.
“Yes, being able to have the opportunity to speak with a patient who has gone through a laryngectomy was useful” PID 201804
While, additionally, family members could be effective information resources, capable of assisting participants process information.
“She [partner] helped me understand it and just being there” PID 201807
HCPs were recognised as sources of verbal information, with important roles in clarifying information, and guiding participants to useful information sources.
“The verbal information provided by the medical team was clear and the online resources and factsheet could be used as a reference to go back to between consultations and aspects of treatment” PID 201804
“If you were needing more information, that information would need to come from the doctors or nurses or speech pathologists or dietitian or whatever” PID 201805
Discussion
The laryngeal cancer fact sheet was assessed for relevance and usefulness to 20 participants with direct experience of the disease and its treatment. Overall the fact sheet was understandable, covered most topics, and was clear. The participants had a high health literacy level and preferred to read the information resource alone. There were valuable suggestions from participants to improve the laryngeal cancer resource. The use of information resources is hampered by a lack of access to them at point of care, proving an important barrier in information provision.
The laryngeal cancer fact sheet provided the right quantity of information about the medical diagnosis, investigation, and treatment. The content categories are consistent with cancer patient preferences identified in other cross-sectional surveys.8,12 There were information gaps highlighted: impact on job or work, regional travel assistance, second opinions, and long term sides effects. This is consistent with the unmet information domains reported in the literature: physical, activities of daily living, psychological, social support, communication, and financial. 13 There were contrasting views about the information resource in our study, in particular, the side-effects of radiation therapy may need improvement or may not be sufficiently detailed to depict the experience of some people. 14 There was a need for all risk factors to be mentioned to assist with informed decision-making. These results are in line with results of studies completed with people with advanced cancer who were making decisions about treatment using a decision aid who wanted information on risks and prognosis. 15 Transoral laser excision for early laryngeal cancer was a topic patients wanted more information about. Laser excision of laryngeal cancer is widely used in practice, cost-effective and an alternative to traditional external beam radiotherapy. 16
Supportive care needs of patients treated for laryngeal cancer were not covered sufficiently in the resource. Information is needed on the practical domains including finances, transport and housing for both patients and carers. Burdens associated with geographical relocation to a tertiary centre are significant factors patients consider in regards to treatment decisions which also effects their families. 17 Having a patient education resource which is understandable and helpful will contribute new knowledge and may have a positive impact on patient behaviour. 18
Understandability of information is not limited to written material, other formats such as video, visual aids, graphs or pictures are used to assist people with lower health literacy. 19 The diagram within the laryngeal cancer factsheet was not clear and too small meaning participants found it difficult to use. Participants’ preferred the HNC-specific website (beyondfive.org.au) as it offered multi-media resources to explain the anatomy and personal stories of others having undergone treatment. A systematic review of video-assisted patient education classified information formats into three categories: (1) providing objective information verbally or graphically (‘didactic presentation’); (2) real people engaged in a specific practice (‘practice presentation’); and, (3) real people enacting scenes (‘narrative presentation’). The review reported the most powerful education tool to modify patient behaviour was the narrative presentation. 20 Having multi-media resources allows more able and interested users to move from simple to detailed information.21,22
Well-prepared patients are better able to manage their health and other medical issues that arise. Understanding information provided on what to expect with treatment allows patients to experience better health outcomes, enhances patient satisfaction and treatment compliance. 23 A descriptive study reported providing more information on the cancer treatment allowed patients to be more involved in their cancer treatment choices and engage in more discussion with the health care team. 24 Providing information that fulfils the needs of cancer patients is vital to ensure patient satisfaction, better health-related quality of life (HRQoL), and reduced anxiety and depression, a recommendation consistent with our findings. 25 Preparation for treatment needs to include all alternatives including the risks and benefits of non-treatment compared to treatment options, focusing on comfort. 26
Timing of education needs to be right, although there is no consensus on when exactly is the right time. 27 Timing of education needs to be considered in the context of the potential for emotions to affect information processing, a concern particularly pertinent to a cancer diagnosis. HNC treatments and laryngeal cancer treatments can have a spectrum of morbidity from dysphagia to inability to speak with a laryngectomy. Patients in our study were not prepared for short and long term side effects as information was provided in insufficient detail or too late in the treatment trajectory.28–30 Thus it’s important to use multiple information formats over multiple sessions to ensure information provision is timely and effective. 31
Psychological distress amongst cancer patients exists on a spectrum from adjustment, failure to adjustment and clinical levels of anxiety and depression. In our study, low levels of psychological distress were reported after reading the fact sheet. Psychological distress is associated much more strongly with survivorship concerns than the cancer diagnosis itself. 32 Psychosocial care of patients with cancer consists of both education and supportive care. Education encompassing ‘cure’ and ‘hope’ was found within our laryngeal cancer information resource and valued by participants. Although they reported a need for information on support for family members including psychological support, spiritual support and educating the carer with information. 33
High quality patient and family education consists of verbal communication involving a multidisciplinary approach, considering the range of learning styles, literacy levels, and cultures. 27 Unfortunately, few HCPs are trained to provide effective one-on-one communications with patients. Participants wanted the HCP to guide them through the laryngeal cancer resource to allow them to clarify any misunderstanding or unmet needs at diagnosis. 34 Information available in multiple formats caters for the variety in learning styles and health literacy levels.
Providing the laryngeal cancer information resource on the Internet (beyondfive.org.au) ensures it can be easily updated and maintained, and can connect patients with HCP and other patients through various media platforms. Contemporary American Cancer Society guidelines emphasise the provision or referral of HNC survivors to appropriate resources able to cater to their needs. Web-based resources can be accessible in multiple formats by patients in their own time and at their own pace.35,36 People unfamiliar with computers can have the written information resource printed by their HCP. Thus, HCP are important in bridging the gap between information needs and delivery of these web-based resources.
There are several limitations to consider when interpreting these results. The majority of our participants were post-treatment and had information about their laryngeal cancer and treatment before assessing our resource, likely influencing their responses on both the survey and in the interviews. Our population had relatively high health literacy levels at screening, thus our capacity to comment on the experience of people with low health literacy levels is limited. Given the requirement to read the participant information statement and complete a written questionnaire, there were major barriers to the recruitment of people with lower health literacy skills. Despite a proportion of people diagnosed with HNC in Australia being from culturally and linguistically diverse backgrounds, our information resource, questionnaire and interview were available only in English. Finally, the response rate of 36% makes it difficult to generalise the results, though this is a common problem with questionnaires. 37
Conclusion
The laryngeal cancer information resource is a detailed, clear, and accessible patient education material. It is acceptable to patients and best provided at the time of diagnosis. Further development of the information resource is required to incorporate information about survivorship concerns, impact on work, impact on family, and long-term side effects. Participants expressed a preference for information provided by their HCP and internet-based multi-media resources accessible outside their consultations.
Supplemental Material
sj-docx-1-jhi-10.1177_1460458221989403 – Supplemental material for Assessment of an evidence-based laryngeal cancer fact sheet: A mixed methods study
Supplemental material, sj-docx-1-jhi-10.1177_1460458221989403 for Assessment of an evidence-based laryngeal cancer fact sheet: A mixed methods study by Joe Jabbour, Heather L Shepherd, Thomas Beddow, Puma Sundaresan, Chris Milross, Carsten E Palme, Jonathan R Clark and Haryana M Dhillon in Health Informatics Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.