
Abstract
This study aimed to evaluate the effect of a novel progressive web application (PWA) on the patient’s oral and denture knowledge and hygiene. Fifty-two removable partial denture wearers were randomised to receive education using the PWA, or verbal instructions accompanied by demonstration of hygienic procedures. Changes in the participants’ knowledge score, plaque index, gingival index and denture plaque was evaluated during a follow-up period of 3 months. The participants’ acceptance of PWA was explored through usage logs and a feedback form. Both groups showed significant improvement in knowledge scores, oral and denture hygiene indices (p < 0.001) after education. The PWA group demonstrated significantly lower gingival index score than control (p = 0.008) at the third month review. In conclusion, there is potential of using mobile application in educating elderly patients and the PWA is a viable option for providing post-denture delivery instructions.
Introduction
Within the past decade, the Internet usage among the population showed an upward trend worldwide. Similarly, in Malaysia, the percentage of Internet users have increased from 55.9% to 84.2%. 1 One of the advantage of utilising the Internet in healthcare is reachability, as seen in its significantly positive impact on health outcomes of rural adults. 2 The use of information and communication technology for health (eHealth) 3 had been vastly reported in the medical field. Patient empowerment towards healthcare was achieved through education and improvement in health literacy. This widespread approach of health promotion was made possible with rapid advances in mobile technologies and applications, popularly known as mHealth. As patients can easily access useful information at their convenience, these technologies aid in self-management of healthcare.4,5 Health care professionals and patients are rapidly accepting telemedicine due to disruption of physical delivery of health care services during the coronavirus disease pandemic. In the near future, eHealth and mHealth is anticipated to be completely integrated into health care delivery platform. 6
Conventionally, mobile applications used for healthcare may be native, web or hybrid applications. 7 A new approach to mobile application development was introduced in 2015, known as the progressive web application (PWA). 8 Its user-interface design and navigation are similar to those of native application, but it is more affordable to develop and maintain. Thus, PWA is gaining popularity for mobile application construction, 9 even in the healthcare sector. 10
In dentistry, current mobile applications for oral health promotion significantly reduced gingivitis and improved oral hygiene. These applications have shown excellent results as a tool to educate and motivate good oral hygiene.11–13 However, the majority of these studies were conducted on Orthodontic patients which consist of adolescents. 14 Considering the success of these applications, a similar oral health application could be potentially used for dental chairside education and as a reference material for older patients. The present study aimed to evaluate the effect of a newly developed educational PWA on removable partial denture (RPD) wearers’ oral and denture knowledge and hygiene compared with that on the control group who received verbal instructions with demonstrations. Furthermore, their acceptance of this new educational approach was evaluated.
Materials and methods
Study design
A prospective, parallel randomised controlled trial was conducted on 52 cobalt–chromium RPD participants at the Faculty of Dentistry, Universiti Kebangsaan Malaysia (UKM), from August 2019 to November 2019. Ethical approval was obtained from the UKM Ethics Committee [UKM PPI/111/8/JEP-2018-583] before the commencement of the study.
The sample size was calculated based on the primary outcome measure, which is the change in the knowledge test score. A minimal sample size of 36 subjects was required on the basis of an effect size of 0.4 derived from a previous study, 12 with significance levels of 5% and 80%. A total of 52 subjects were recruited to allow for potential dropout rates of 40%.
A random number generator (https://stattrek.com/statistics/random-number-generator.aspx) was used to assign unique identification numbers to the participants, who were then allocated equally into the PWA and control groups via a random sequence generator software (https://www.graphpad.com/quickcalcs/randomize1/). The participants’ allocation group was concealed in sealed brown envelopes labelled with their identification numbers by a research assistant who was not involved in the data collection nor analysis. The study was single-blind, whereby the participant’s allocation was kept anonymous from the outcome assessor.
Eligibility criteria
The inclusion criteria included patients wearing cobalt–chromium RPD made at the dental laboratory in the dental faculty and delivered by undergraduate students from June 2017 to June 2019, patients who own a smartphone with Internet access and have been using it within the last 6 months, patients aged 25–75 years and patients who are literate in English or Malay language.
The exclusion criteria included patients who do not wear their RPDs or only wear them occasionally; patients with a history of denture repair or reline and those using denture adhesive; patients with physical or mental disabilities that impede their ability to perform oral hygiene activities; patients involved in other oral-health education or oral hygiene maintenance programme; active smokers and patients with medical conditions that may affect their gingival health, such as drug-induced gingival hypertrophy or xerostomia.
Intervention
The participants were educated by two trained research assistants using the PWA or the conventional method practised by the undergraduates at the dental faculty. Only participants in the PWA group were provided with the Uniform Resource Locator (URL) and Quick-Response code (QR code) to instal the PWA on their phones’ home screen (Figure 1). In the PWA group, the research assistant explained the PWA contents to the participants after installation. In the control group, the participants were educated verbally, accompanied by a practical demonstration of hygienic procedures on dental models. A checklist was provided to both research assistants to ensure consistency when employing the conventional method.
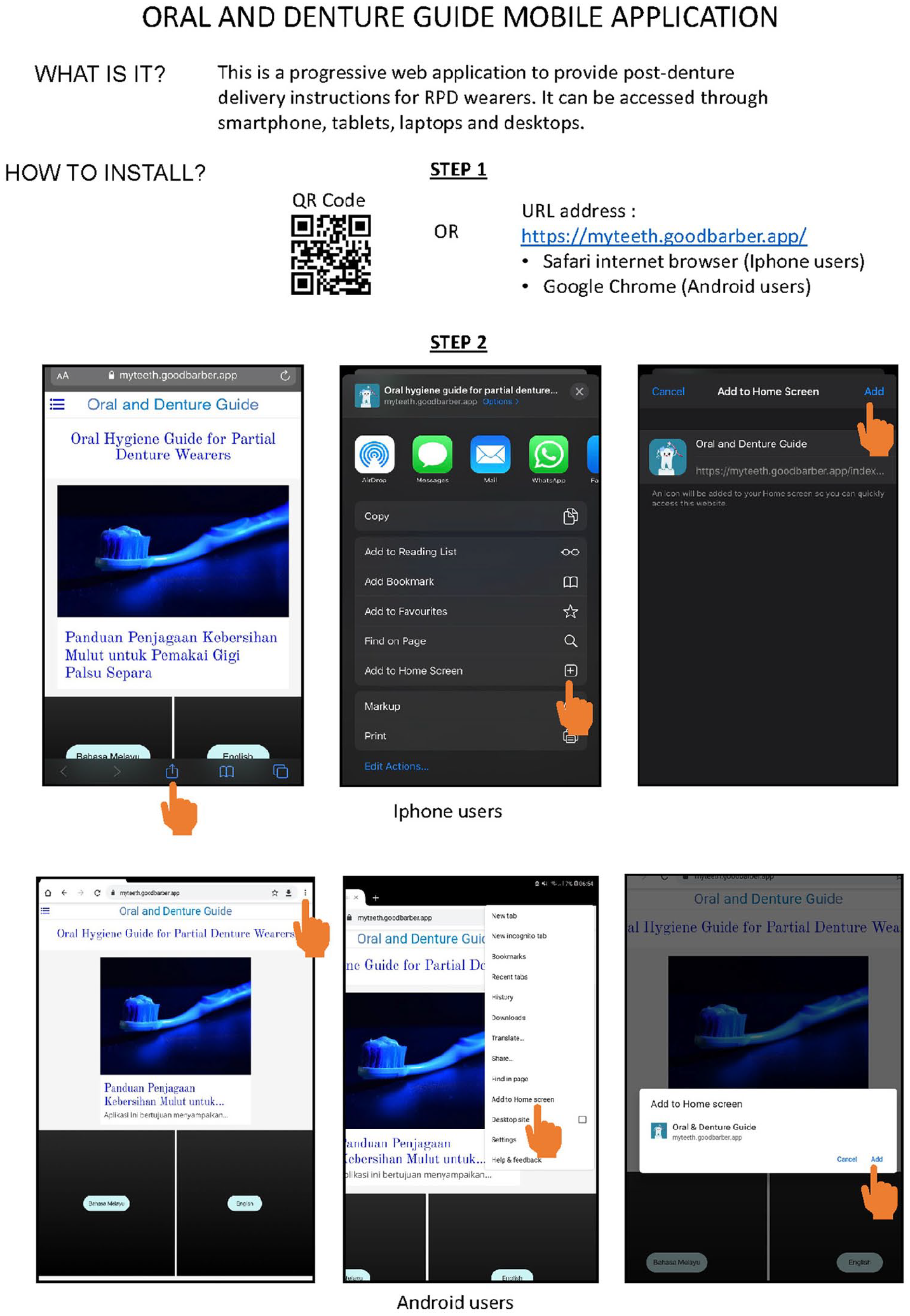
Installation instructions for ‘Oral and Denture Guide’ PWA.
The PWA evaluated in this study was named ‘Oral and Denture Guide’. It was created on Angular JavaScript 4.0 using GoodBarber, which is an application builder. 15 The development of this PWA was based on user-centred design principles. 16 It was validated using a mixed-method approach consisting of expert assessment of content and design and user involvement. 17 The final layout of the PWA after refinement (Figure 2) was pilot tested before the study.
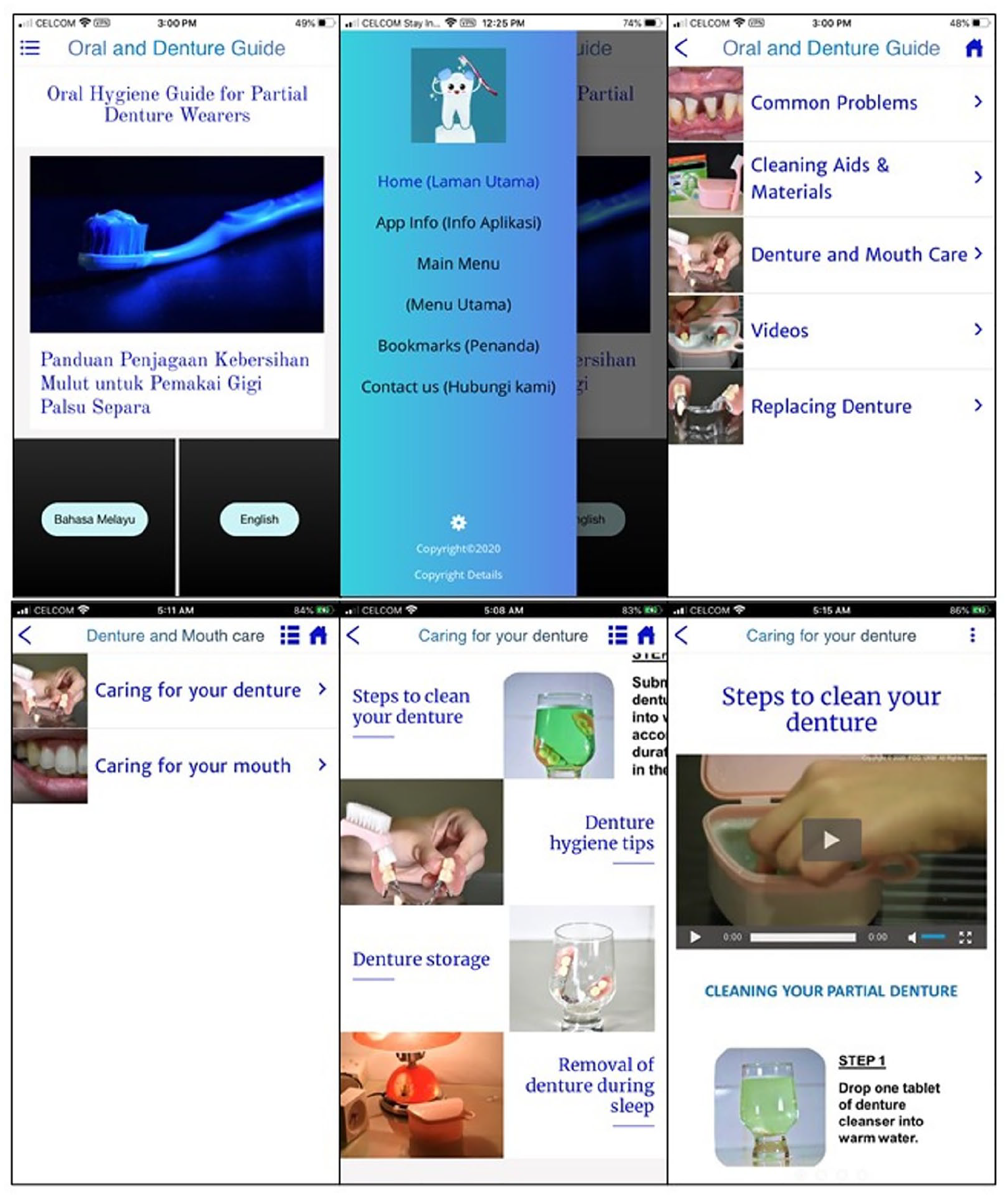
Final layout of ‘Oral and Denture Guide’ PWA. Clockwise from top-left: screenshot of homepage, navigation menu, main menu, sub-menu, section displaying a list of topics and article containing illustrations and video.
The ‘Oral and Denture Guide’ PWA has a bilingual content consisting of recommended essential post-denture delivery information 18 and videos on oral and denture hygiene procedures. The evidence-based written details were accompanied by pictures to improve understanding. All the pictures and videos in the PWA were produced by the authors. Given that the end-users included the elderly, the authors paid attention to font selection and user interface design to enhance the usability of this application. 19
Outcome assessment
The participants’ knowledge was measured using a self-administered questionnaire before education (T0), after education during the same visit (T1) and 3 months after the first visit (T2). The developed and validated questionnaire was used to collect the participants’ demographic data and test their knowledge of denture care and hygiene. Pilot test was conducted to gauge the suitability of the questions and the average knowledge score. One mark was given for every correct answer, whilst zero was given for every wrong answer and ‘Not sure’.
Silness and Loe’s plaque index (PI) and gingival index (GI) 20 were used to evaluate the participants’ oral hygiene. A single examiner calibrated the indices before the study, with intra-examiner kappa values of 0.814 for PI and 0.826 for GI. The same operator examined all the participants at baseline (D0), 1 month after education (D30) and 3 months after education (D90). The plaque and gingivitis levels on the buccal, lingual, mesial and distal tooth surfaces of all teeth were recorded to obtain the overall mean value. When in doubt between two scores, the higher score was chosen.
Denture plaque (DP) scores were measured to assess the denture hygiene amongst participants. The fitting surface of the RPDs were stained using GC Tri Plaque ID Gel plaque disclosing agent (GC Corporation, Japan) following the methods described by Jeganathan et al. 21 The research assistant then placed each RPD in a photo lightbox and took coloured photographs by using a digital single-lens reflex camera (Nikon D5600, Japan) mounted on a camera stand. The RPDs were subsequently cleaned in an ultrasonic cleaner using Biosonic Enzymatic Ultrasonic Cleaner (Coltene, Japan) and returned to the participants. The blinded single examiner superimposed gridlines measuring 0.5 cm × 0.5 cm on the photographs of the RPD and examined them in the computer screen under a magnification of 200%. The scoring criteria were as follows: 0 = no plaque, 1 = light plaque (25% of the fitting surface was covered), 2 = moderate plaque (26%–50% of the fitting surface was covered), 3 = heavy plaque (51%–75% of the fitting surface was covered) and 4 = very heavy plaque (76%–100% of the fitting surface was covered). 21 For patients wearing maxillary and mandibular RPDs, the higher score between the two was recorded. The intra-examiner reliability test performed to 10% of the participants at D0, D30 and D90 had kappa values of 0.688, 0.722 and 0.706, respectively, indicating good agreement.
Acceptance of the ‘Oral and Denture Guide’ PWA
The actual usage of the PWA was investigated using objective and subjective measures to assess the patient’s acceptance. 22 The objective measure included the usage logs generated by the software in the form of PWA traffic, whilst the subjective measure consisted of the feedback form administered to the participants in the PWA group during the third visit. The study procedure and data collection are displayed in Figure 3.
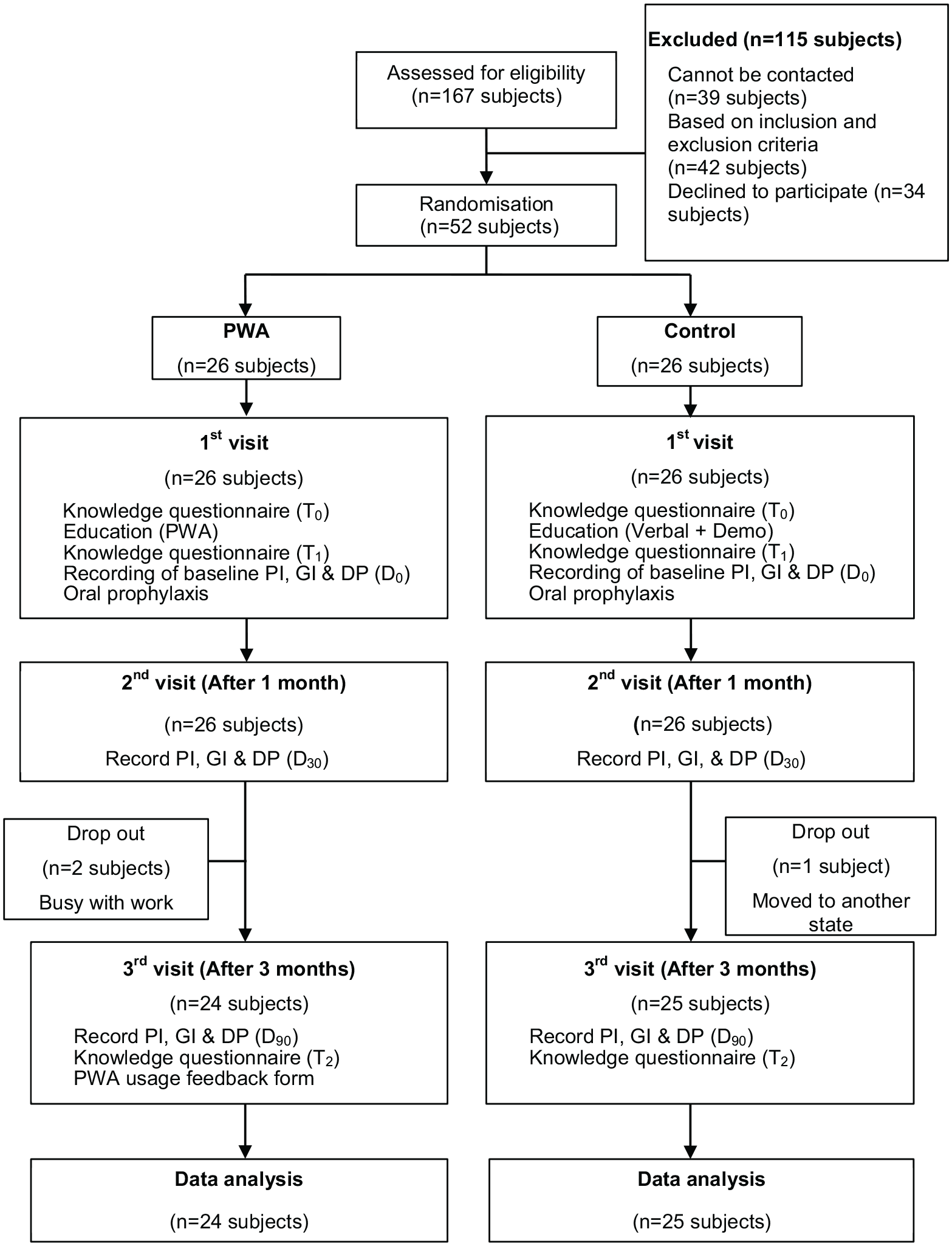
Workflow diagram depicting the study procedure and data collection.
Statistical analyses
The data collected were explored and analysed on SPSS (version 26, IBM). The participants’ demographic characteristics were summarised using descriptive statistics. The effect of PWA on the knowledge scores compared with that of the conventional method of education was analysed using two-way mixed ANOVA. For ordinal data, differences in the PI, GI and DP scores between the PWA group and the control group at all three visits were determined using the Mann–Whitney U test. Friedman test was conducted to analyse the changes in baseline PI, GI, and DP scores within each group after exposure to education. The level of significance was set at p < 0.05.
Results
The 52 participants allocated to the PWA and control groups did not show any significant difference in terms of demographic factors (Table 1). Three participants failed to return for the third-month review, and 50% of the remaining 24 participants in the PWA group were aged 60 years and above.
Patients’ demographic data at baseline.
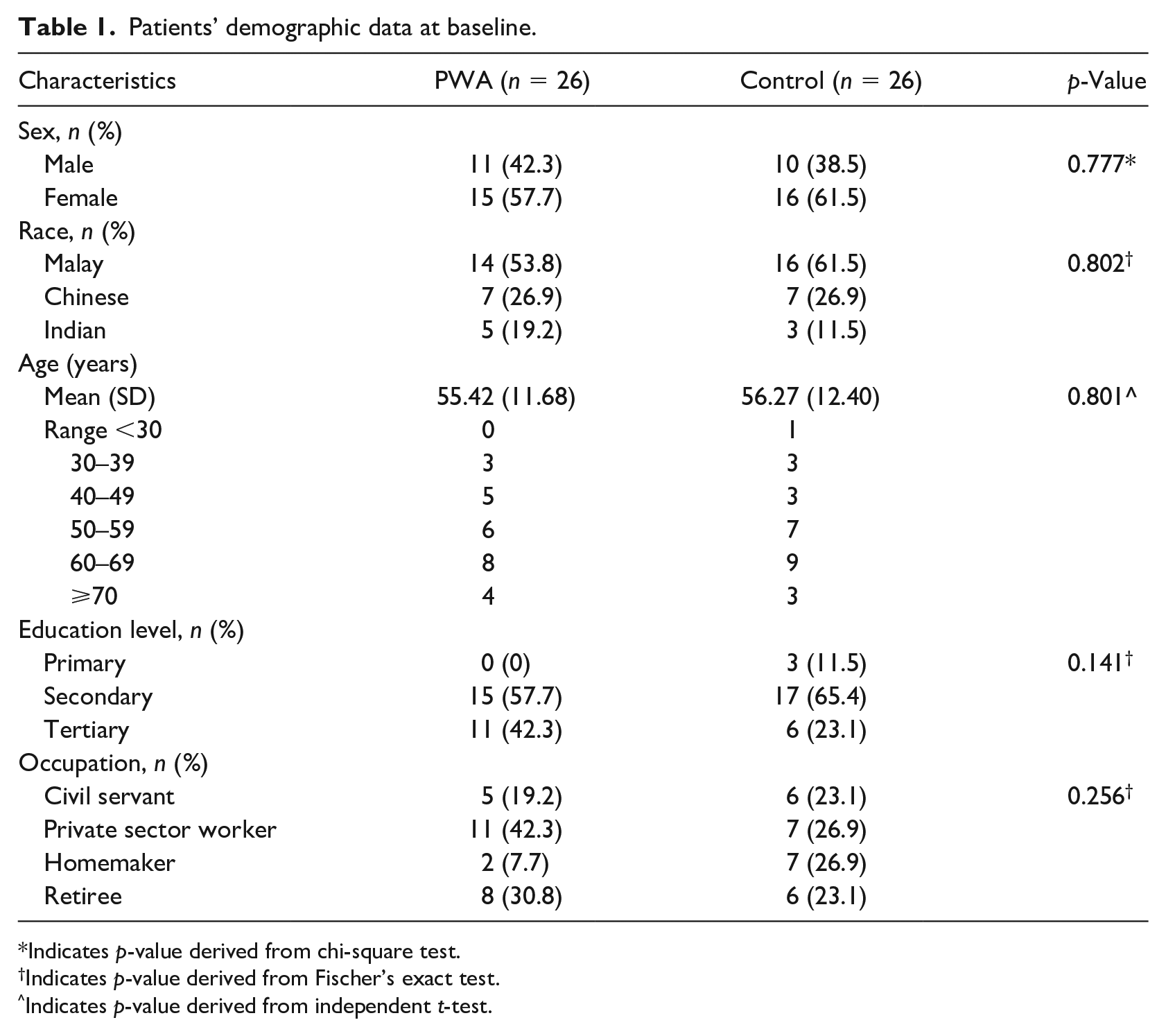
Indicates p-value derived from chi-square test.
Indicates p-value derived from Fischer’s exact test.
Indicates p-value derived from independent t-test.
Knowledge scores
The results of the two-way mixed ANOVA showed no significant difference in mean knowledge scores (F = 0.007, p = 0.934) between the PWA group and the control group at T0, T1 and T2. However, the knowledge scores changed significantly after exposure to education in both groups (F = 195.062, p < 0.001). Post hoc analysis reveals significant difference for T1 > T0, T2 < T1 and T2 > T0 with a significance level of p < 0.001 respectively, as displayed in the graph in Figure 4.
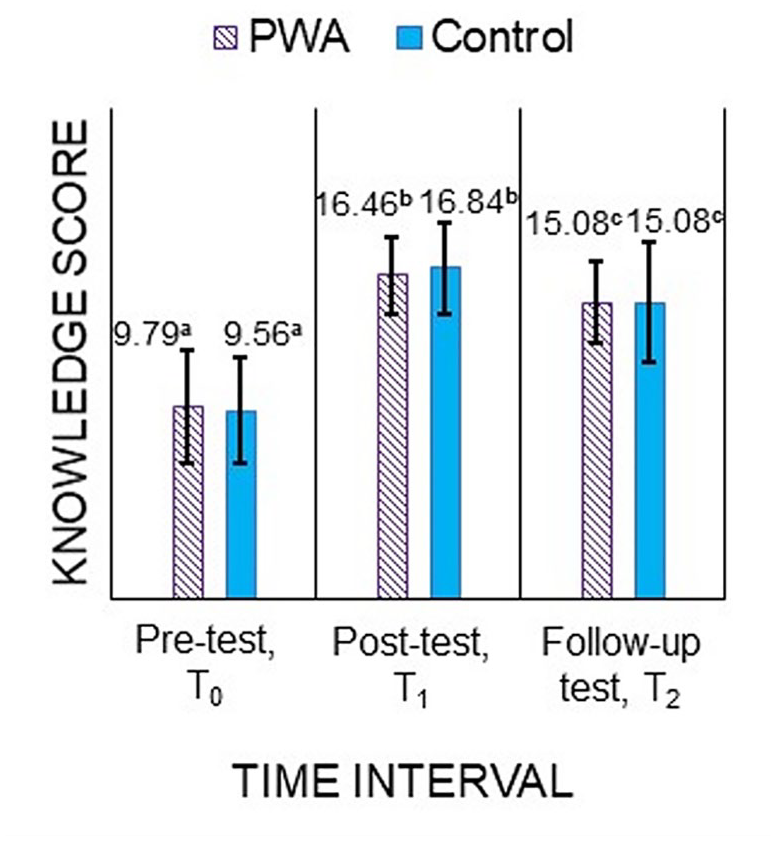
Participants’ mean knowledge scores in the PWA and control groups at different time intervals. Means followed by different letters indicate statistically significant differences.
Given that 50% of the participants in the PWA group were seniors, further investigation was conducted to compare the knowledge scores between the PWA participants below 60 years of age (<60 years) and those aged 60 years and above (⩾60 years). Mann–Whitney U test was used for intergroup comparison because the data were not normally distributed. No significant difference was observed in the mean rank knowledge score between the two age groups at T0 (p = 0.319), T1 (p = 0.319) and T2 (p = 0.590). By contrast, intragroup comparison using Friedman test showed significant changes in the mean rank knowledge score in both age groups after they were educated (p < 0.001). Pairwise comparison with Bonferroni correction shows significant difference at T1 > T0 (p < 0.001) and T2 > T0 (p = 0.005) for <60 years and T1 > T0 (p < 0.001) and T2 > T0 (p = 0.007) for ⩾60 years.
PI, GI and DP scores
Table 2 displays the statistical analysis of the intergroup and intragroup comparisons of PI, GI and DP scores.
Intergroup and intragroup comparisons of PI, GI and DP scores.
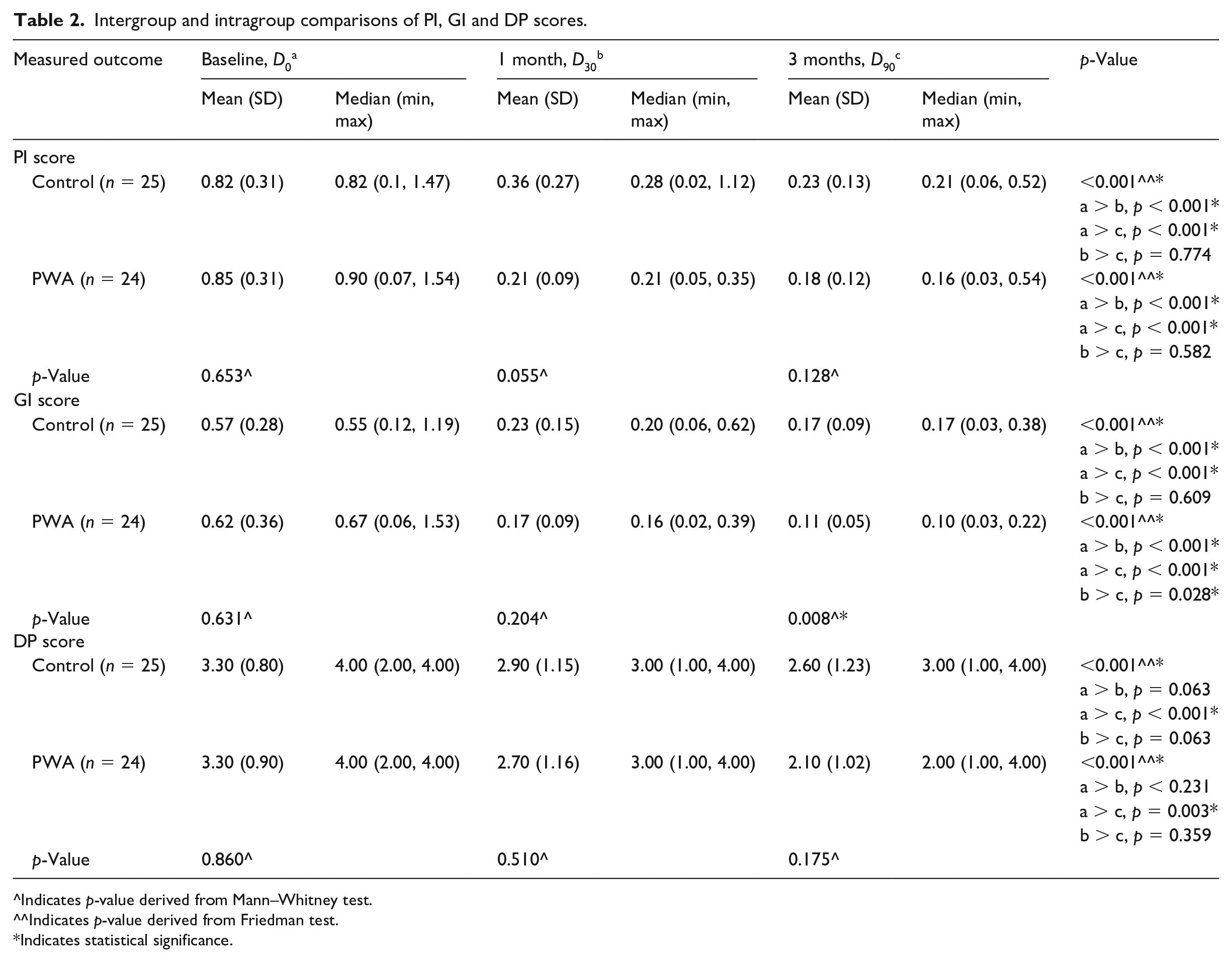
^Indicates p-value derived from Mann–Whitney test.
^^Indicates p-value derived from Friedman test.
Indicates statistical significance.
Both groups revealed a statistically significant reduction (p < 0.001) in the PI and GI scores from D0 to D30 and from D0 to D90. The GI scores at D90 was significantly lower in the PWA group than in the control group (p = 0.008). No significant difference was found in the median DP scores between the two groups after they were educated (p = 0.175).
‘Oral and Denture Guide’ PWA actual usage
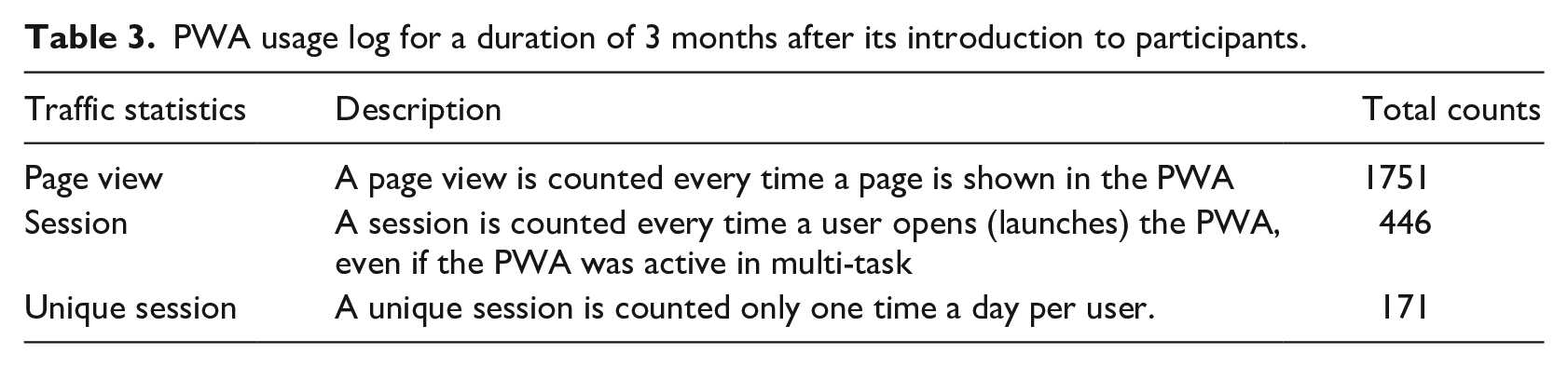
Table 3 displays the usage log for a duration of 3 months generated in the PWA software, starting from the day after its introduction to the participants. From this usage log, the frequency of usage was gauged by analysing the average number of users and the number of times it was accessed per user in 3 months. The number of pages viewed in the PWA each time it was used reflected the usage intensity.
PWA usage log for a duration of 3 months after its introduction to participants.
The calculation method are as follows:



The data analysed showed that in 3 months, an average of two persons used the PWA per day. Each user utilised it around three times. When the patients accessed the PWA, an average of four pages were visited each time.
The feedback forms administered to the 24 participants in the PWA group revealed that 92% used the PWA at least one time (Figure 5). Two participants did not use it because they felt that the information obtained during the dental chairside education was sufficient. For the participants who accessed the PWA, the most common reason was to seek additional information, followed by to refer to details that they have forgotten and to share the content with someone they know or to watch videos in the PWA. The majority of the participants responded that the section on denture care was the most useful, and 75% of the participants mentioned that they recommended the PWA to someone they know.
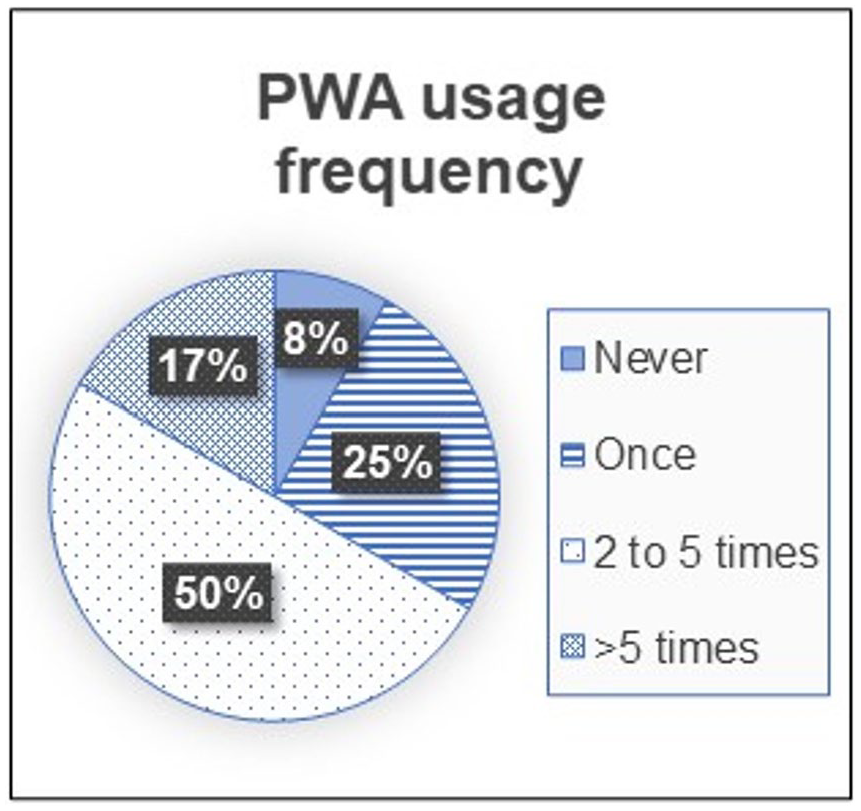
Frequency of PWA usage by the participants. The pie chart shows the percentage of participants using PWA in accordance with the number of times it was used within 3 months.
Discussion
This study was conducted strictly on patients who received cobalt–chromium RPD dentures processed at the dental faculty, and delivered by undergraduate students under the supervision of specialists within a 2-year duration. These criteria ensure standardisation in the material and design principles of the RPD, which influences gingival health. 23 A maximum duration of 2 years was selected as older RPDs without adequate postplacement care may have integrity defects. 24 Participants above 75 years were excluded due to possible changes in cognitive function 25 and manual dexterity, 26 which may both affect the study outcome.
Most published studies on dental-related mobile applications were native applications. PWA was chosen in the present study because of its multi-platform advantage. PWA can be installed and distributed without application marketplaces, work without Internet connectivity, receive push notifications and look like regular mobile applications. It can be installed by different phone operating systems users directly from the Uniform Resource Locator (URL) or by scanning the Quick-Response code (QR code). Phone operating systems and application stores do not restrict its usage, hence the cost-effective development and distribution. 10 PWA also requires less installation space than native application, thereby addressing user’s memory space concern. 27 Although PWA is inferior to native application in terms of its ability to access user contacts or calendar, this extra feature was not necessary in the ‘Oral and Denture Guide’ PWA.
The scale in the index by Jeganathan et al. is widely used to assess the DP in RPDs18,28,29 and presents high values of agreement with reliability test. 21 Consistently measuring the distribution of plaque on dentures is difficult to perform by visual inspection alone. 30 Thus, in the present study, dentures images were superimposed with gridlines to aid in scoring, as described in the methodology section earlier. Scoring was conducted by a single examiner to reduce measurement error. 30
To the authors’ knowledge, this is the first clinical study to develop and evaluate the efficacy of a mobile application for post-denture delivery education of patients with RPD. The results revealed no significant difference in knowledge gain between the participants in the PWA and control groups. Comparison with previous studies18,31 on the influence of the method of education on RPD wearers’ knowledge was not possible because these studies measured oral hygiene instead of knowledge score as an outcome.
Considering the participants who installed the PWA had the advantage of having a take-home reference material, their performance was expected to improve during the follow-up test at T2. However, the results showed a decline in their knowledge scores compared with that at T1, which was a similar trend to that in the control group. This outcome differed from the findings of Marchetti et al., who revealed knowledge gain and retention in participants exposed to mobile application. These positive results were attributed to the repetition of educational content through messages sent by the mobile application developed in their study. 12
On the contrary, active reminders were not sent to the PWA participants in the current study, because the authors were interested in knowing the actual usage on the basis of the participant’s own initiative. Similarly, hygiene instructions were not reinforced during the 1-month review for the control group to avoid bias between the two groups. These results further emphasised the importance of periodic reinforcement of oral health education. Moreover, the study by Marchetti et al. was conducted on adolescents, whereas half of the participants in the present study were seniors. The storage capacity of working memory differs between older (aged 60–79 years) and younger (aged 18–25 years) individuals. 32 Furthermore, some processing deficits of the working memory possibly exist in older adults, 32 leading to loss of information acquired over time.
Despite the drop in the knowledge scores during T2, the significant increase in the scores compared with those during T0 showed that the PWA was indeed as effective as the control in delivering valuable information to the participants. In this controlled study, accurate and consistent information was delivered through the conventional method of verbal instructions. However, in practice, different levels of knowledge about denture hygiene maintenance amongst dental practitioners led to conflicting instructions about denture cleansing methods, resulting in the ineffective conveyance of post-denture delivery instructions. Some of them have an unfavourable attitude in educating patients, especially the elderly. 33 Studies reported that a high percentage of patients did not receive denture hygiene instructions post-denture delivery.34,35 Unsurprisingly, the knowledge and levels of denture hygiene amongst patients are generally unsatisfactory.36,37 Using the PWA for dental chairside education can overcome the shortcomings of the conventional method which were subjected to human error and time constraints. Moreover, patients were more likely to recall and practise the guidelines for denture care when provided with written educational materials that contain illustrations.18,31 Instead of a traditional information leaflet which may be misplaced or lost, the PWA can be a good alternative as a reference material as it is more cost-effective and engaging. Comparison of knowledge gain between the participants below 60 years of age and those aged 60 years and above revealed no significant difference, indicating that the elderly benefitted from the PWA as much as the younger age group. This finding is encouraging, because it may address the problem of elderly patients receiving insufficient denture care information.33,38
The participants’ oral hygiene was significantly improved by the ‘Oral and Denture Guide’ PWA compared with that of the control group. This finding was in agreement with the findings from the studies on oral-hygiene focussed applications.11,13 Although no significant difference was found in the PI score between the PWA and control groups, gingival status may be a more reliable measurement of improvement in oral hygiene. 39 The plaque levels assessed may be misleading, because some participants could be more meticulous with their oral hygiene on the day of measurement, resulting in less plaque.
For denture hygiene, no significant difference was found in the DP scores between the PWA group and the control group. This result differed from that of Ribeiro et al., who reported better denture hygiene in the group provided with written illustrated educational material than in the control group. 18 However, this significant difference only started to become evident at the 6- and 12-month reviews, whereas the participants in the present research were only followed up for 3 months. Moreover, denture hygiene instructions were repeated when necessary during the review sessions. Thus, Ribeiro et al.’s positive results may be attributed to the periodic reinforcement.
Acceptance is an attitude towards a technology that could influence technology adoption. In the present study, the participants’ acceptance of this educational approach was assessed by exploring the actual usage 22 and their response to PWA. The usage frequency (Figure 4) was lower than that obtained by Underwood et al., who reported that 44.8% of participants used the oral health application of interest two times daily. However, most of them used it for less than a week. 40 Although the reported frequency of use was high, the majority of their participants were aged 7–12 years. Moreover, the data reported were based on self-reported usage, which is a subjective measure, whereas the values reported in the present study includes data from the usage log statistics. 22 Besides, the participants in the present study reported that they mainly used the PWA as a source of reference and found the section on denture care to be most useful, thereby substantiating the role of PWA in conveying post-denture delivery instructions. Considering that elderly people take time to adopt new technologies but do so if they find these technologies beneficial, 41 the participants’ overall response towards PWA was reasonably good.
This study had some limitations. Some differences may exist amongst the RPDs that possibly influenced the GI scores between the PWA group and the control group. Given that the participants received their RPDs within a 2-year duration, increased surface roughness in old dentures 42 could affect cleanliness. Denture design factors, such as the lingual plate major connector, may affect not only the quantity but also the quality of plaque intraorally; thus, these factors may have considerable effects on gingival health. 28
Besides, the participants were only followed up for 3 months without periodic reinforcement during reviews. Retention of the knowledge gained and improvement in behavioural habits over an extended period were not certain. Moreover, participants may not change their old practises on denture care despite acquiring new knowledge. 31 Thus, the effect of the knowledge gain on their denture hygiene routine is uncertain. The PWA usage by the participants measured through the usage log is an estimate value because the individual user cannot be specifically identified as no log in details were required when accessing the PWA. The results obtained could not be extrapolated to the general population because the PWA may only be useful to a specific group in the society due to limitations, such as language, literacy and the need for a mobile device with Internet access.
Future studies may incorporate behaviour modification techniques when developing mobile applications and exploring their effect on denture hygiene utilisation and habits. Mobile applications could also be improvised, such as adding a read-out loud function or using comprehensive videos to overcome issues of language and literacy. Mobile applications are expected to be widely used amongst all ages in the society as smartphones gradually replace conventional mobile phones. The results of this study suggested that the elderly are receptive to this new educational approach; thus, mobile application developers should consider them as target users and incorporate design features that are user-friendly for elderly people.
Conclusion
The ‘Oral and Denture Guide’ PWA developed in this study was as effective as the conventional method of conveying post denture delivery instructions, even amongst elderly patients, as reflected by the participants’ improvement in their oral and denture knowledge and hygiene. This PWA could address the problems discussed in the literature, including the inadequate information received by patients during denture delivery, which is dependent on the knowledge, attitude and practise of their dentist. Nevertheless, active reminders should be incorporated in this PWA to periodically reinforce oral health education for retention of essential knowledge on oral and denture hygiene.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr. Haslina Rani, a Dental Public Health Specialist at the Faculty of Dentistry, UKM, for her input in the validation process of the PWA content. A special thanks to Miss Zaihosnita Hood, a Human–Computer Interaction Expert in UKM, for her contribution in the design evaluation of the PWA’s user interface.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Young Researcher Incentive Grant by University Kebangsaan Malaysia. The grant number is GGPM-2017-108.