
Abstract
While there are an increasing number of mobile health applications to facilitate self-management in patients with chronic disease, little is known about which application features are responsible for impact. The objective was to uncover application features associated with increased usability or improved patient outcomes. A rapid review was conducted in MEDLINE for recent studies on smartphone applications. Eligible studies examined applications for adult chronic disease populations, with self-management content, and assessed specific features. The features studied and their impacts on usability and patient outcomes were extracted. From 3661 records, 19 studies were eligible. Numerous application features related to interface (e.g. reduced number of screens, limited manual data entry) and content (e.g. simplicity, self-tracking features) were linked to improved usability. Only three studies examined patient outcomes. Specific features were shown to have a higher impact. Implementing them can improve chronic disease management and reduce app development efforts.
Introduction
Chronic diseases, including cardiovascular and respiratory diseases, cancer, and diabetes, are a significant cause of morbidity and mortality worldwide. 1 Despite the existence of many therapies for these diseases, adherence and self-management are often suboptimal, resulting in a large annual financial burden to health systems. 2 With the advancement of digital technology, individuals and companies have made an effort to address chronic disease management. 3 One example is the use of mobile health applications (app(s))—computer programs on smartphones—to improve patient self-management. 4
Current literature supports the use of mobile app interventions for chronic disease management.5,6 Many studies show statistically significant improvements in clinically relevant indicators of chronic disease management with mobile app interventions; for example, one meta-analysis clearly indicated these interventions can reduce HbA1c% levels in diabetics, a common indicator of appropriate diabetic management. 5 Moreover, research also provides evidence of app “usability,” defined by the International Standardization Organization as the “extent to which a product can be used by specified users to achieve specified goals with effectiveness, efficiency, and satisfaction, in a specified context of use.” 6 For example, patient populations rate most hypertension apps as “usable.” 7
However, a vast amount of mobile health interventions have been reported to fail during clinical implementation.8,9 Given the large number of apps available, the frequency at which apps are developed, and the cost of development, it is important to identify the specific features that are more promising. 10 Little is known about the specific app features that are responsible for improvements in chronic disease management.5,7,11 Typically, investigators hypothesize about desirable features. For instance, Lee Jungh et al., 12 analyzed several mobile interventions to determine whether they improved disease outcomes or usability and then discussed several app features shared by successful interventions in common.
To our knowledge, no review has focused on specifically studying the app features of smartphone interventions targeting chronic disease management. We found one meta-analysis on text messaging interventions that showed that personalized messages, scheduled less than daily, were most effective at improving chronic disease management. 13 However, as the mobile world has advanced beyond text messaging, a deeper understanding of new mobile features is due. Given app diversity, it is important to know what makes a given mobile app intervention effective at improving chronic disease management. This information could help end users, such as development teams, design interventions with the most favorable app features.
Objective
The goal of this review was to determine the impact of specific mobile app features on chronic disease management or usability.
Methods
Design
We conducted a convergent mixed study rapid review, where qualitative, quantitative, and mixed method studies were integrated to better understand the complex and new phenomenon of mobile app use in health management. 14 Rapid reviews are essentially less comprehensive than systematic reviews and aim to uncover results quicker and with less divergent accompanying findings. 15 They are particularly appropriate for the study of mobile apps, given the rapid evolution of technology. 16
Information source and search strategy
A literature search was conducted on 13 May 2018 in a single major database (MEDLINE) for relevant original studies on app features. The intentionally broad preliminary search terms were: “Mobile Applications (Mesh)” Or “Smartphones” Or “Mobile Apps” Or “Cell Phones Or iPhones.” Search terms beyond the MeSH term were required, given the frequent delay in assigning MeSH categories to new studies. To further narrow the search, additional filters for English papers, human subjects, adult populations (18–44 years), and publication year (past 5 years) were applied. The search strategy was discussed with a health science librarian. We opted not to limit the search with terms for specific chronic diseases such as diabetes or human immunodeficiency virus (HIV) infection. This resulted in more records to screen but prevented us from missing potential studies.
Study selection
One reviewer (A.G.) conducted study selection as per rapid review norms. 17 Selection was completed in two rounds. First, records were screened by title and abstract and second, by full text. A second reviewer resolved any uncertainties (I.V.). The following eligibility criteria were applied:
Population
We included original studies conducted with adults who were clinically diagnosed with a chronic disease, such as diabetes, HIV infection, heart failure, or depression.
Intervention
To be included, studies needed to investigate interventions based on smartphone mobile apps to help patients self-manage their conditions. Self-management was defined as the “active participation by a patient in his or her own health care decisions and interventions. 18 ” Interventions strictly based on text messaging have been studied extensively and were excluded. Interventions utilizing computers, tablets, and other wearable devices were also excluded to focus on widely available portable devices, that is, smartphones. Interventions that only provided information to clinicians were excluded, as our interest was in what helps patients themselves manage their disease(s).
Outcomes
Eligible studies examined the impacts of specific app features on disease management or usability. Studies that measured outcomes of an app without narrowing in on specific app features were excluded.
There were no additional exclusion criteria for the number of apps studied or the number of participants in each study as we wanted to be comprehensive and extract the maximum amount of both quantitative and qualitative information.
Data extraction
Each study’s authors, date, country, population examined, design, duration, and number of participants were extracted to provide context for how each app feature was studied. The reviewer then extracted (1) a description of each app feature considered and (2) the study’s quantitative or qualitative findings on the reported impact of each feature on chronic disease management or usability.
Synthesis
The raw results include, per study, each app feature studied and the impact described on chronic disease management or usability. These data were then synthetized using qualitative synthesis methods. More precisely, we used grouping and clustering to divide features into meaningful categories for interpretation. 19 During the synthesis process, we used several steps to regroup studies inductively. The first distinction was made between app features relating to content and those concerned with interface. Content refers to what is delivered by the intervention, while interface concerns how the content is accessed. Content features were further broken down into information presentation features, personal data tracking and tailoring features, communication with health worker features, and social support features. Interface features were divided into screen features, data entry features, and security features.
Results
Study selection process
From 3661 initial search records, 19 original studies were included in the review (see flowchart in Figure 1). The most common reason for article exclusion during the title and abstract screen was because the app being studied was not designed for chronic disease management. During the full-text review, studies were mostly excluded for failure to study a specific mobile app feature. This exclusion criterion was applied with caution, since some studies provided relevant data on specific mobile app features as secondary outcomes and were eligible.
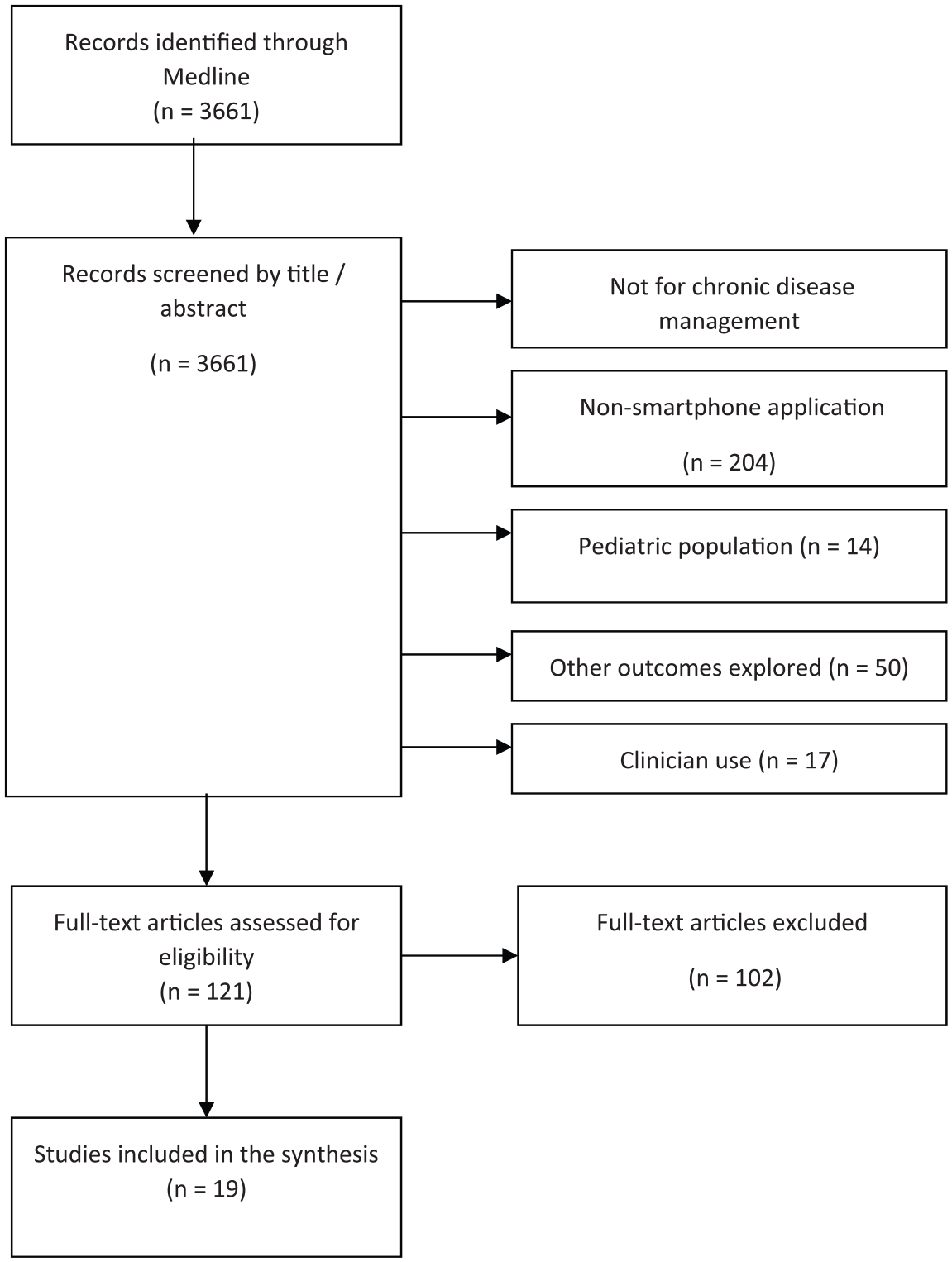
PRISMA flow diagram of the record inclusion process.
Characteristics of included studies
Specific chronic diseases represented by the retained studies were diabetes (n = 4 studies), HIV infection (n = 4), mental illness (n = 2), hypertension (n = 2), chronic pain (n = 1), thalassemia (n = 1), chronic obstructive pulmonary disease (n = 1), and rheumatoid arthritis (n = 1). Three additional studies concerned patient populations with multiple chronic diseases. Study designs varied. Approximately half (n = 11) were quantitative studies, whereas seven were qualitative and one was mixed. Prevalent among the quantitative studies were surveys on specific features (n = 6), quasi-experimental cohort studies where several features were implemented and outcomes such as depression scores or viral loads were measured (n = 3), and quasi-experimental cohort studies where several features were implemented and usability outcomes were measured (n = 2). Prevalent among the qualitative studies were interviews (n = 5) and focus groups (n = 2) that inquired with open-ended questions, about patient preferences for proposed features or for suggestions on what features to include. The characteristics of each included study can be found in Table 1.
Characteristics of included studies.
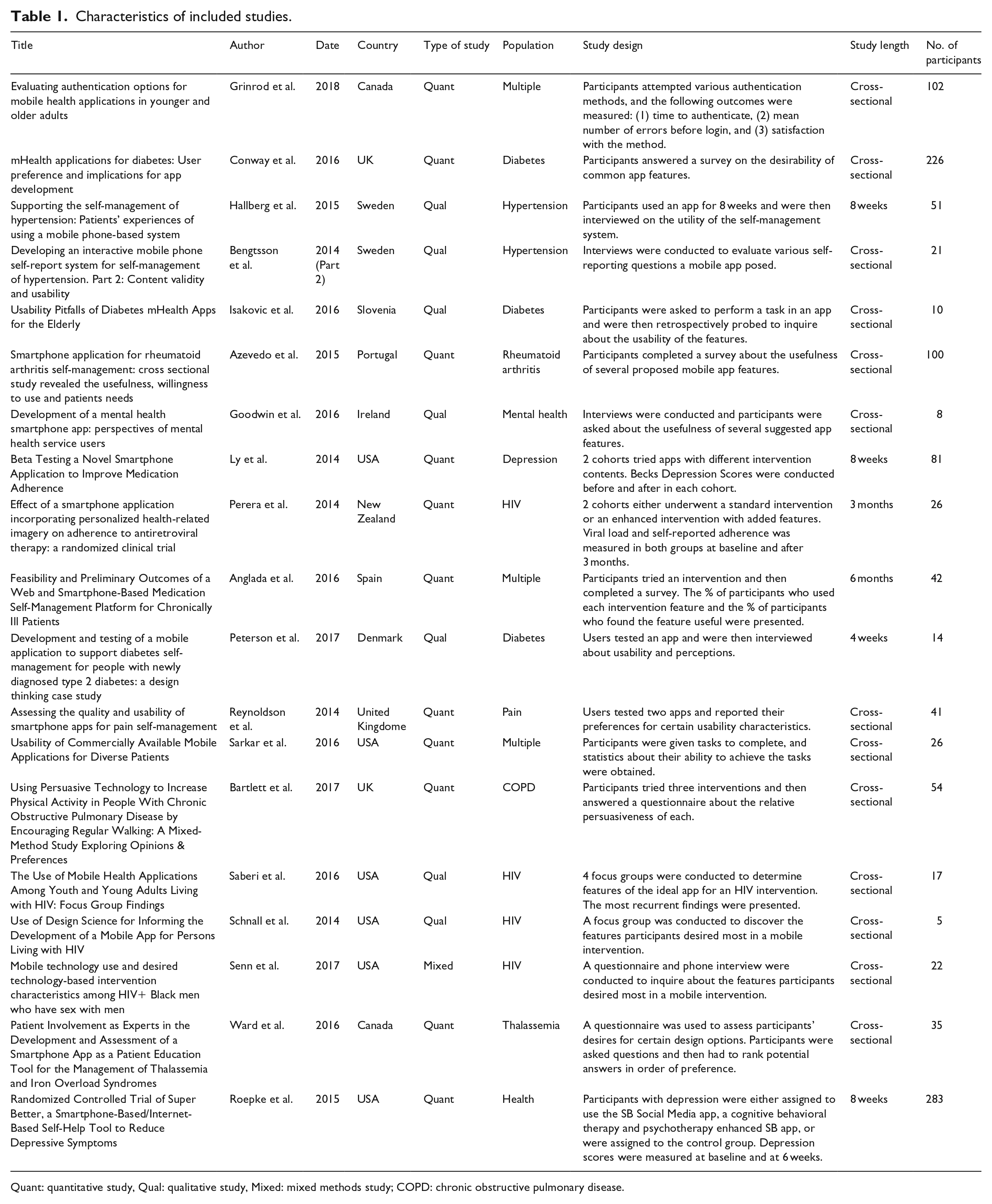
Quant: quantitative study, Qual: qualitative study, Mixed: mixed methods study; COPD: chronic obstructive pulmonary disease.
Results of included studies
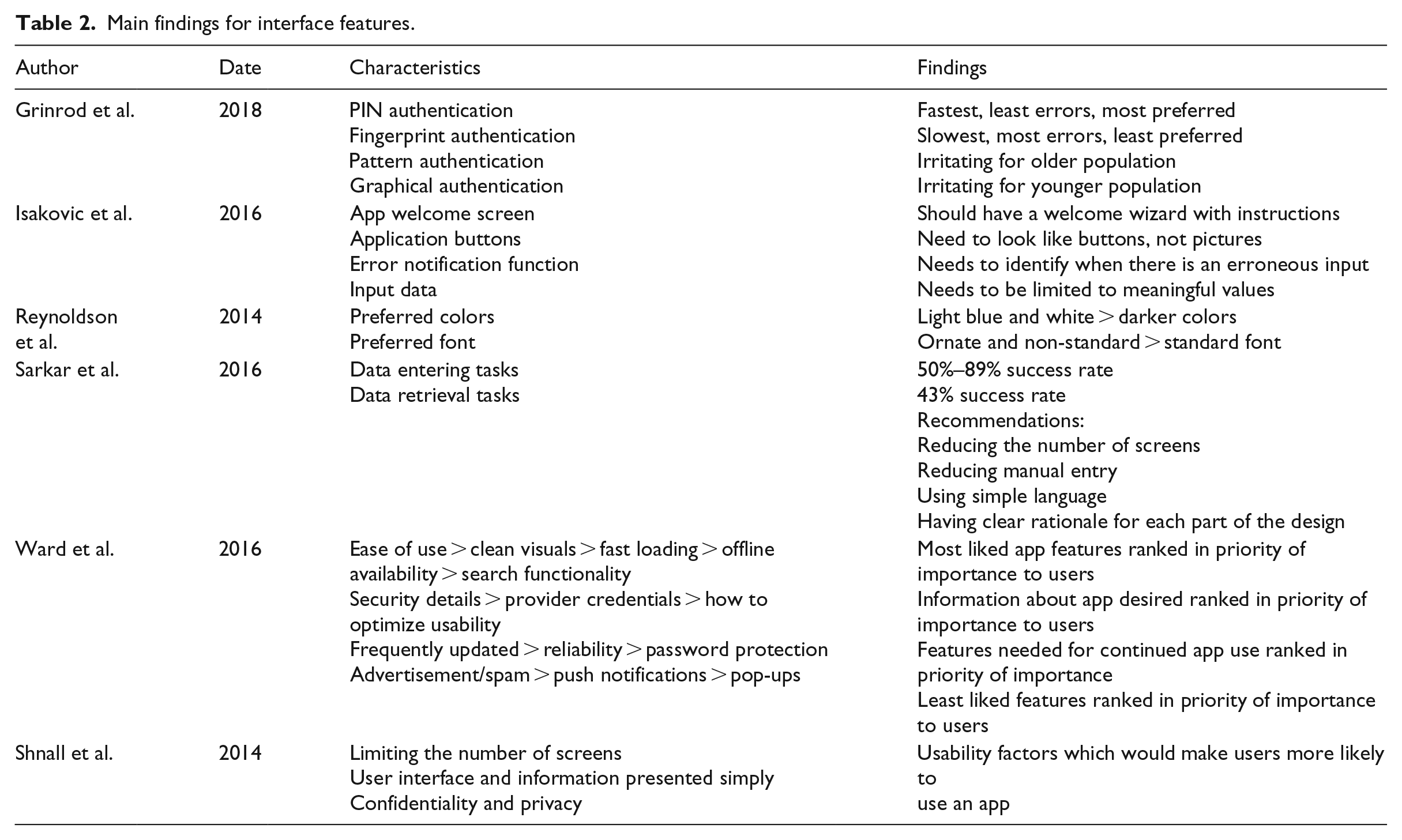
As per our eligibility criteria, each retained study examined several app features and resulted in findings for each feature. The raw features and findings, per study, are presented in Table 2 (Main findings for interface features) and Table 3 (Main findings for content features).
Main findings for interface features.
Main findings for content features.
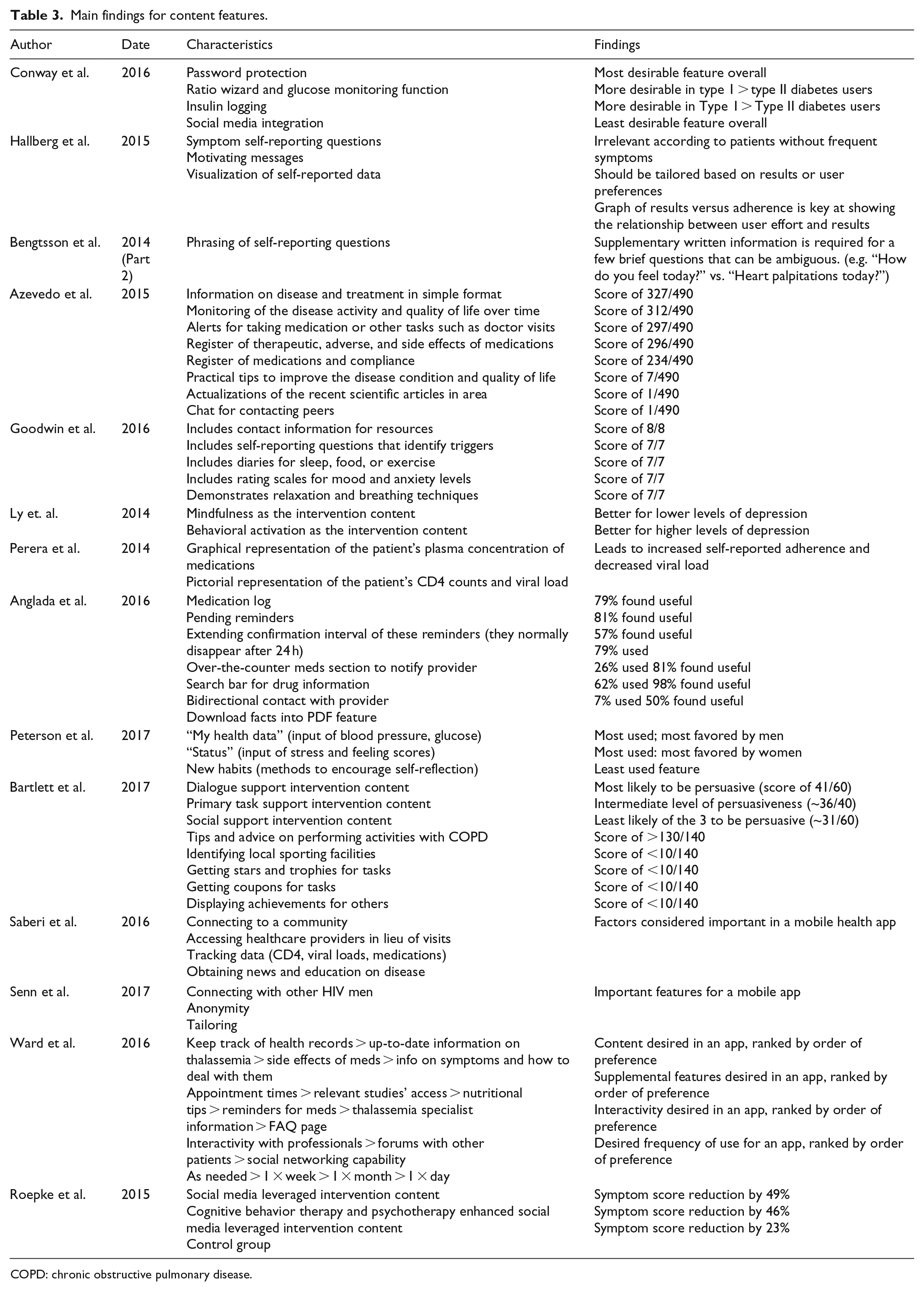
COPD: chronic obstructive pulmonary disease.
Interface-related app features
Interface features (i.e. screen features, data entry features, and security features) were examined in approximately one-third of the studies (n = 6, 32%).
Regarding screen features, two studies identified the need to minimize the number of screens one must encounter per task.20,21 Two studies identified the need for clean visuals22,23 and one identified the benefit of a “welcome wizard” with instructions, the first time an app is used. 23 An additional study showed that light colors and ornate fonts were most beneficial. 24
As to data entry features, one study identified the need to limit the use of manual data entry. 20 One study showed that input data should be limited to meaningful values (i.e. within the possible range of values). 23 Moreover, this study highlights the benefit of an error notification function that signals erroneous inputs. 23
For security features, one study examined authentication methods and found that password protection is essential and that PIN entry is preferred to other methods. 25 Another study similarly showed the value users place on security. 21 A final study suggested limiting advertisements, notifications, and pop-ups. 22
Content-related app features
Content features (i.e. information presentation features, self-tracking features, communication with health worker features, social support features) were examined in three quarters of the studies (n = 14, 74%).
Regarding information presentation features, two studies demonstrated the need to present information on disease and treatment in a simple format.21,26 Another showed that a dialogue support approach was the content most likely to be persuasive over the primary task support approach and the social support approach. 27
Considering self-tracking features, five studies showed that tracking personal data and information was beneficial.21,28–31 Four additional studies demonstrated that tailoring content to each user based on their profile and past data is beneficial.19,24,32,33 For example, symptom self-report questionnaires should be automatically tailored to the patients’ frequency of symptoms to avoid burdening respondents. 32 In addition, one study showed that graphical presentations and visuals increased medication adherence and improved outcomes. 34
As to communication with healthcare worker features, a method to communicate with healthcare providers, in lieu of a clinic visit, was deemed helpful in three studies.21,24,31
Regarding social support features, there were contrasting findings on their desirability, depending on the disease. For people living with HIV (PLHIV), connection to other users was suggested as an important feature, if anonymity was respected.31,33 However, users with diabetes or rheumatoid arthritis did not deem these features helpful.26,28 In addition, the ability to obtain media news and education in a distilled manner was suggested for PLHIV. 31 However, this was not deemed helpful for rheumatoid arthritis patients. 26
Discussion
Many commercial apps have been found to be effective and useful in patient populations, without any determination of which app features were responsible.5,7,11 To our knowledge, this review contributes the first summary of the benefits of specific smartphone app features for use in the self-management of chronic diseases. It is, thus, unique and complimentary to past research on mobile apps. It is also one of the first reviews to draw on the newer capabilities offered by smartphones beyond text messaging.
Results of our review showed that numerous app features related to interface (e.g. reduced number of screens, limited manual data entry, simple authentication methods) and content (e.g. simplicity, self-tracking features, communication with healthcare workers) were linked to improved usability. With regard to social support features, results were mixed. Figure 2 summarizes the most frequently valued features.
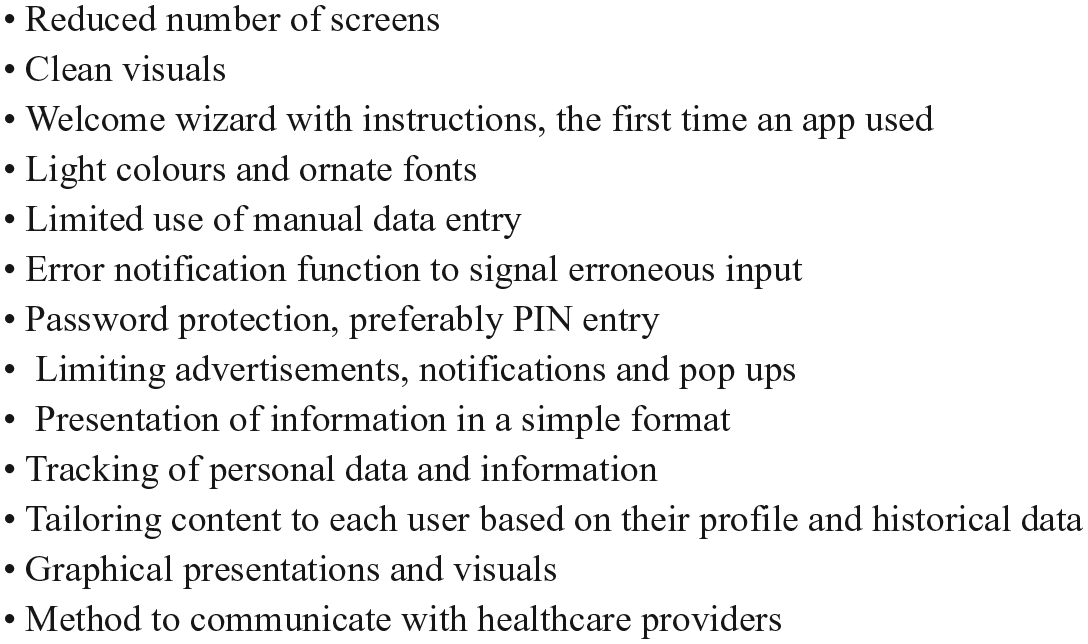
Summary of frequently valued features.
Given the significant global burden of prevalent chronic diseases, achieving improved chronic disease management is of paramount importance. 1 These study results could help optimize app design and increase app usability. In an expanding market of apps for chronic disease management, 10 it is important to identify promising features and prevent implementation failure, a common challenge.8,9
While this review was conducted in accordance with predefined and recognized review methods, there are some limitations. 15 The validity of the results may be limited by an adherence bias. Patients who agreed to participate in the included studies may be more likely to self-manage their health conditions. Should this be the case, the perspective of poor self-managers may be underrepresented. Future research should ensure users from all spectrums of compliance are included. In addition, this study is a rapid review, not a systematic review, and focuses on records from a sole database. Once additional studies accumulate on this topic, it may be worthwhile to efficiently conduct a systematic review.
Regarding next steps, there is a need to continue researching specific app features, given the many apps and features that are continuously developed. Particular effort should be devoted to investigating newly emerging trends in mobile health such as gaming. 2 It should also be noted that most studies (n = 16) assessed usability and not improvements in markers of chronic disease management. Although the assumption is that usability leads to improved chronic disease management, future intervention studies should include patient outcomes directly such as depression scores or viral loads.
Conclusion
In summary, this study overviews the current status of research assessing the effectiveness of specific app features in smartphone intervention for chronic disease self-management. Several specific features are important to include in app interventions. Doing so can reduce wasted app development efforts, maximize intervention efficacy, and lead to overall better chronic disease management for patients. Further research is needed in this domain, as there are numerous apps and features in development. Moreover, studies assessing patient outcomes directly are needed.
Footnotes
Acknowledgements
We would also like to thank the MSD Avenir Foundation for their support.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BL and KE and in the process of developing a smartphone application for routine use in the patient and clinician management of barriers to antiretroviral therapy adherence in people living with HIV.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: AG and KE are funded, in part, by a Strategy for Patient-Oriented Research (SPOR) Mentorship Chair in Innovative Clinical Trials awarded by the Canadian Institutes of Health Research (CIHR) (![]() ) to BL (grant number 383427).
) to BL (grant number 383427).