
Abstract
Background
HIV/AIDS is a major public health issue in Cameroon. Traditional paper-based monitoring systems often fail to provide timely and accurate data, essential for effective program management. The increasing availability of mobile phones and internet services presents an opportunity for mHealth technologies to improve data collection and monitoring. However, the successful integration of mHealth into existing systems requires an understanding of the attitudes and challenges faced by end-users. This study explores the attitudes of mHealth end-users and the challenges they face in integrating mobile technology into HIV program monitoring in Cameroon.
Methods
A mixed-methods approach was employed, involving both qualitative and quantitative data collection. The study included 251 respondents from 4 regions (East, Adamawa, Centre, and Littoral) and 4 FGDs. Data were collected using questionnaires and focus group discussion guides. The quantitative data were analyzed using SPSS, while qualitative data were transcribed and analyzed using Nvivo9 with an inductive thematic approach.
Results
The quantitative analysis revealed that 78% of respondents had a good attitude toward mHealth, with a mean score of 4.48 ± 0.956. A significant difference was found in the mean attitude scores between those categorized as having good (M = 4.94, SD = 0.244) and poor attitudes (M = 2.71, SD = 0.540; t = -42.50, df = 237, p < 0.001). Qualitative findings supported these results, with most FGD participants expressing a preference for mobile applications over traditional methods due to ease of use and efficiency. Factors such as region of work (F = 5.259, p = 0.002) and educational level (F = 13.45, p < 0.001) significantly influenced attitudes toward mHealth, while age and work experience did not show significant associations. Key challenges identified include the need for better training and support for mHealth technologies, issues with the reliability of mobile devices, and the need for integration with existing systems.
Conclusion
There is strong support for the use of mobile technology in improving data collection and patient care. There is a generally positive attitude toward mHealth among end-users in Cameroon, with significant support for its continued integration into HIV program monitoring. However, challenges such as device usability and internet access need to be addressed to enhance the effectiveness of mHealth interventions. Future initiatives should consider these factors to improve data collection and program monitoring in Cameroon.
Introduction and background
HIV/AIDS is one of the major public health concerns in Cameroon. Despite significant progress in combating the virus, challenges remain, particularly in maintaining accurate and up-to-date information on HIV cases, treatment adherence, and program effectiveness. Traditional paper-based monitoring systems often struggle to provide real-time data and comprehensive insights required for informed decision making in a dynamic landscape of HIV care.1,2 As access to mobile phones and internet services continues to increase in the region, mHealth-related services will also increase. 3 However, the introduction of mobile technology for health programs monitoring and evaluation (M&E) doesn’t connote abandoning the pre-existing systems of data collection, management, and storage. In a report of the 71st World Health Assembly held in March 2018, the WHO adds that, “The spread of digital technologies and global interconnectedness has a significant potential to accelerate Member States’ progress towards achieving Universal Health Coverage (UHC), including ensuring access to quality health services.” 4
The use of mobile technology for M&E of health programs and surveillance by mainly International nongovernmental organizations (INGOs) is a relatively new but promising phenomenon in the African context. The success or failure of mHealth initiatives heavily relies on the attitudes and perceptions of end-users. Slater et al. 5 highlight the importance of consideration of user perspectives and attitudes in the adoption of mHealth technologies. To effectively implement mHealth, in HIV program monitoring it is essential to have a contextualized understanding of these attitudes and challenges. Therefore, this study aims to fill this knowledge gap by investigating the attitudes and challenges encountered by mHealth end-users in the context of HIV program monitoring in Cameroon. Studies have demonstrated the relationship between several sociodemographic characteristics (including age, academic qualification, and years of work experience) and attitudes.6,7 Although mHealth technologies have supported a broad scope of service delivery, our study focused on its use in monitoring, given the current drive by stakeholders to use this innovation to improve the timeliness and quality of data. Findings will provide recommendations on adopting end-user tailored approaches to implementing mHealth interventions for data services in resource-limited settings.
Context
In Cameroon, through technical support of the United States Government (USG) funded projects to the Ministry of Public Health, mHealth have supported the HIV/AIDS program through; SMS-based appointment and medication reminders that improve retention and adherence; smartphone and tablet applications for real-time adherence tracking and counseling; mobile data reporting tools for routine surveillance of HIV indicators; and community health worker data collection platform to collect Prevention of Mother-To-Child Transmission/Early Infant Diagnosis (PMTCT/EID) data and guide referrals. Since health data collection and reporting at the facility level is currently paper-based, some implementing partners of the USG-funded projects adopted the use of mHealth technology to enhance data collection and reporting in HIV service delivery in the regions of the country where they operate.
Selected facilities and NGOs working at the community level in four regions have been supported to implement mHealth technologies. The front line of service delivery in hospitals, health facilities, and community-based organizations that used mHealth technologies to collect and report data were Psychosocial workers, Community Health Workers, and Nurses; all of these Health cadres are herein referred to as “end-user.” These tools did not replace the traditional paper-based registers, as they have not yet been approved by the Ministry of Public Health.
It is important to note that the Ministry of Public Health officially mandates the use of standardized paper-based registers for data collection and reporting at hospital and health facility levels. These registers remain the primary source of national health information and are the official tools for aggregating and transmitting data through the health information system.
Methodology
Research design
We employed a mixed methods design to collect qualitative data through focus group discussions (FGDs), while quantitative data were collected through an online questionnaire from 251 respondents from different work organizations.
Selection of the study site
The study was conducted within four selected regions across the national territory: East, Adamawa, Center, and the Littoral region. These regions were selected for the study because mHealth projects that focus on HIV have been implemented in these areas for 5 to 8 years. These regions also represent a diverse cross-section of the country, encompassing different geographical and socio-economic contexts, rural, urban, and semi-urban settings.
Target population
This study involved all mHealth end-users in the selected regions working either in a hospital-based setting or in NGOs providing HIV services at the community level.
Sample size calculation
Sample size calculation was done using Yamane's formula. This formula is a simplified method to calculate sample sizes for finite populations, particularly useful when dealing with large populations and limited resources for data collection. The formula is expressed as:
N = the population size
E = the margin of error (which is ± 5%)
n = Minimum Sample size
N = 774
e = acceptance margin of error = 0.05 (5%)
Thus, n = 774
1 + 774 (0.05)2 = 288 participants
In this study, given an estimated population of 774 and a 5% margin of error, the calculated minimum sample size was 288. This helped ensure that the views of mHealth end-users were captured with sufficient statistical validity.
Sampling technique
All health facilities and NGOs in the four targeted regions were targeted. Health facilities and NGOs that have implemented mHealth interventions for at least 5 years were selected. The 5-year cut-off was chosen to ensure inclusion of health facilities and NGOs that are at various levels of adoption (routine use of mHealth in M&E). Within the study regions, the selection targeted individuals who were actively involved in the use of mHealth technologies within HIV program monitoring in Cameroon. This included psychosocial agents, case managers, and HIV testing agents, who had direct experience with integrating mobile technology into their work. Respondents were stratified by cadre, that is, Case managers, HIV testing agents (who were community health workers), and psychosocial agents. Respondents were randomly selected proportionate to size to reach the required sample size.
Data collection
Qualitative data
Participants were chosen based on their roles, level of experience, and involvement with mHealth tools, ensuring that the discussions would capture a broad range of perspectives and insights. A FGD guide was used to collect qualitative data to explore the attitudes and challenges mHealth end-users face in integrating mobile technology into HIV program monitoring in Cameroon. The FGD guide was pretested with case managers in a district hospital, which was not in the selected region, and refined accordingly. Participants for the FGDs were purposively selected to ensure gender balance and representation of all cadres engaging in the use of mHealth technologies. In each Region, one FGD was conducted, comprising 7 to 10 participants, with a total of 4 FGDs conducted. FGDs on average lasted 1 hour. True saturation was achieved after the third focus group session, as no new themes emerged. To confirm this, an additional focus group discussion was conducted, which also yielded no new insights.
Quantitative data were collected using a semistructured guide that was piloted with 10 university students and refined accordingly. The questionnaire was organized into three sections: participant demographics, attitudes of mHealth end-users, and the challenges encountered in integrating mHealth technology for HIV program follow up. The questionnaire was distributed via Google Forms. Data were collected between January 2022 and February 2023.
Written informed consent was obtained from all participants prior to their enrollment in the study; end-users who did not provide consent were excluded.
Ethical approval for the study was obtained from the Faculty of Health Sciences Institutional Review Board (FHS IRB) of the University of Buea, Cameroon (Approval No: 2020/1241–06/UB/SG/IRB/FHS).
Data management
Questionnaire entries from participants were properly checked for completion. Daily, questionnaire links were sent to respondents through WhatsApp and email. Responses were stored in an Excel sheet with a copy saved on Google Cloud to ensure security and privacy. The data were exported into Statistical Package for the Social Sciences (SPSS) Version 26 (SPSS Inc., Chicago, USA) for analysis. Consistency and validation checks were done to check for invalid codes and missing data. All missing data were coded as 999 in SPSS.
For qualitative data, extensive notes were taken by one of the researchers during the sessions in addition to audio recordings. Informed consent was sought from the FGD participants prior to the sessions and were informed that they would be recorded (for data analyses purposes) had the right to withdraw from the session anytime. They were assured of anonymity in reporting.
Data analysis
Quantitative data were analyzed using SPSS Statistics version 26. Descriptive statistics were used to summarize the data, with continuous variables presented as means and standard deviations, and categorical variables displayed in frequency tables, bar charts, and pie charts. The attitude of mHealth end-users was assessed by scoring their responses and categorizing them into “good” or “poor” attitude, 8 groups based on a threshold of 65% answers (which is an average of the Likert scale responses) considered to demonstrate “good” attitude.
n other to assess the attitude of mHealth end-users, end-users would be considered to either have good or poor attitudes toward mHealth based on their responses. The questions were measured on a two-point Likert scale (Yes and No) and each positive (Yes) response to a question was scored 1 point, otherwise 0. 8 In total, the maximum obtainable score was 6 points corresponding to the 6 questions that were asked. The 6 questions showed good internal consistency in our data (α = 0.92). End-users with scores ≥ 5 were categorized as having a good attitude toward mHealth; otherwise, they were categorized as having a poor attitude.
An F test and chi-square test were employed to examine associations. Logistic regression was then utilized to identify the factors influencing mHealth end-users’ attitudes toward integrating mobile technology in HIV program follow up.
For the qualitative data, audio recordings from the FGDs were transcribed verbatim and processed using NVivo9 software. An inductive content thematic approach was employed to identify and categorize recurring themes. In the first stage, two researchers read the transcribed interviews carefully to identify repeated patterns that were coded and grouped into subcategories and main categories Related issues were them grouped into themes. Where discrepancies arose, these were resolved through discussion and inclusion of two other researchers to reach an agreement. Main messages were identified as quotes to support identified themes.
Results
Level of intervention in the HIV/AIDS program implementation
Because responsibilities overlap, a respondent can be involved at more than one level of intervention in service delivery within the HIV program. According to feedback from participants, majority (73%) indicated they intervene as psychosocial agents where they are responsible for counseling clients, followed by 67% of respondents who indicated they intervene at the level of screening clients (screening here refers to the determination of eligibility for testing) and 61% of respondents intervened at the level of care and treatment. An almost equal percentage of participants intervene in Sensitization and Prevention (55% and 53%, respectively). While 20% of the participants indicated that they facilitate supply chain activities, 4% would intervene in data collection and analysis (Figure 1).
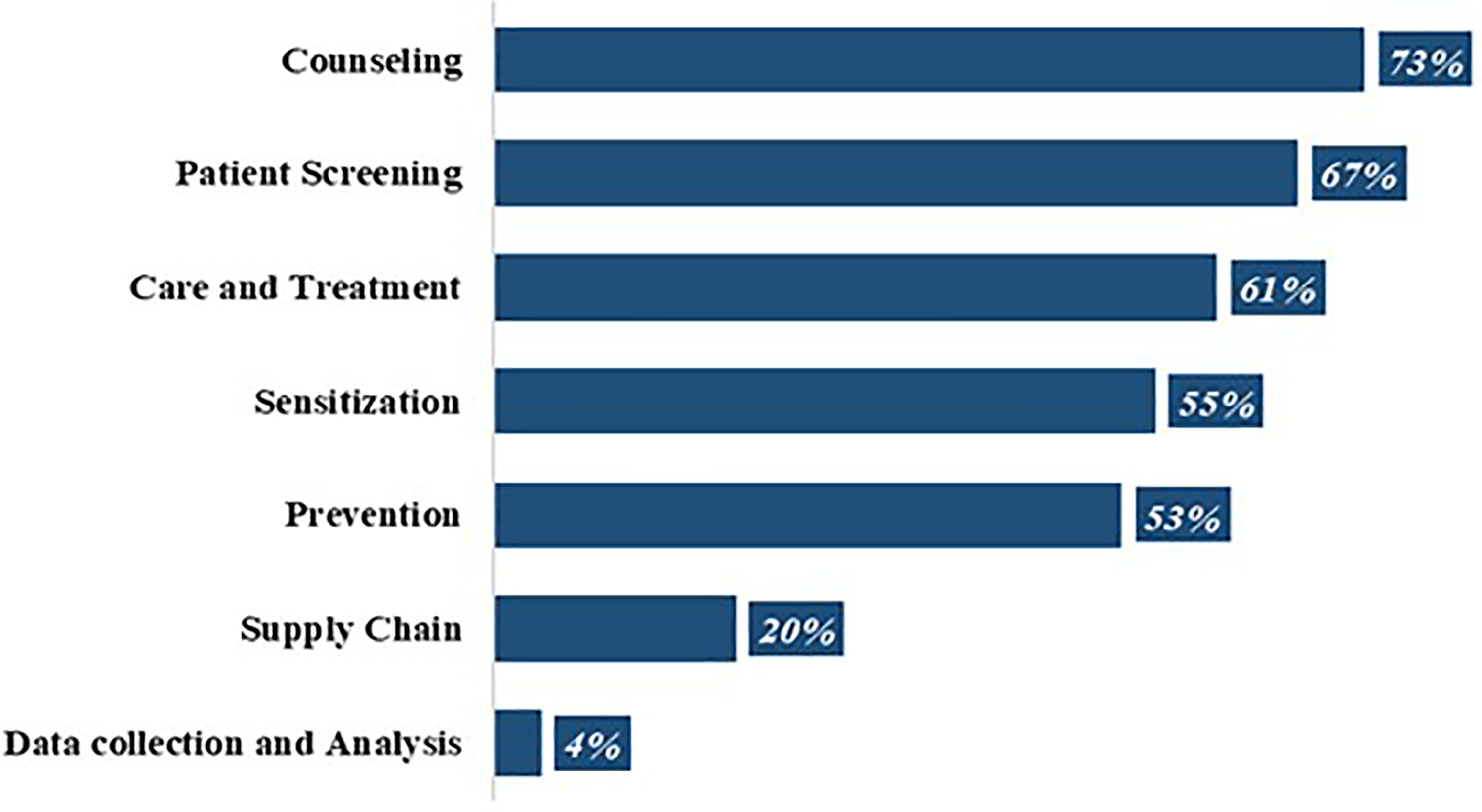
Level of intervention in the HIV AIDS program.
A follow up to get details on the key activities of the respondents revealed the following activities; counseling clients on prevention and treatment, recording testing and initiation, recording and tracking distribution of prevention materials, reminding clients about their appointments, reminding clients to take medication, creating awareness, and record client activities (Figure 1).
Attitude of mHealth end-users
Seventy-eight percent of end-users have a good attitude toward mHealth, while 22.9% of the respondents had a poor attitude toward mHealth. The overall mean score was 4.48 ± 0.956 with a minimum score of 1pt and a maximum score of 6pts.
Five vital questions were asked to assess participants’ attitudes toward mHealth. More than three-quarters (89%) of the participants affirmed that they use the mobile application for data collection.
This result was supported by feedback from FGDs where almost all participants expressed their preference for mobile applications in terms of data collection compared to using traditional papers or registers. Comparing tablets with smartphones, participants cited numerous reasons for choosing tablets, the most common reason being the larger screen size, making it easier to view work-related materials. Additionally, tablets were deemed to be more conducive to enhanced productivity and a richer media experience. The touchscreen interface was also mentioned as a factor in the preference for tablets/smartphones. “We're digital, so we're moving forward. We can't go backward and forward at the same time, as we all know, the tablets are a very indispensable tool because we're in WhatsApp groups, we're in forums and these forums allow us to share information concerning work. The information enables us to communicate better with each other. At the moment, if we're chatting, it's because we have these gadgets. So in my opinion, the tablet is way more preferable at the job site as compared to the button phones”. (FGD Male participant)
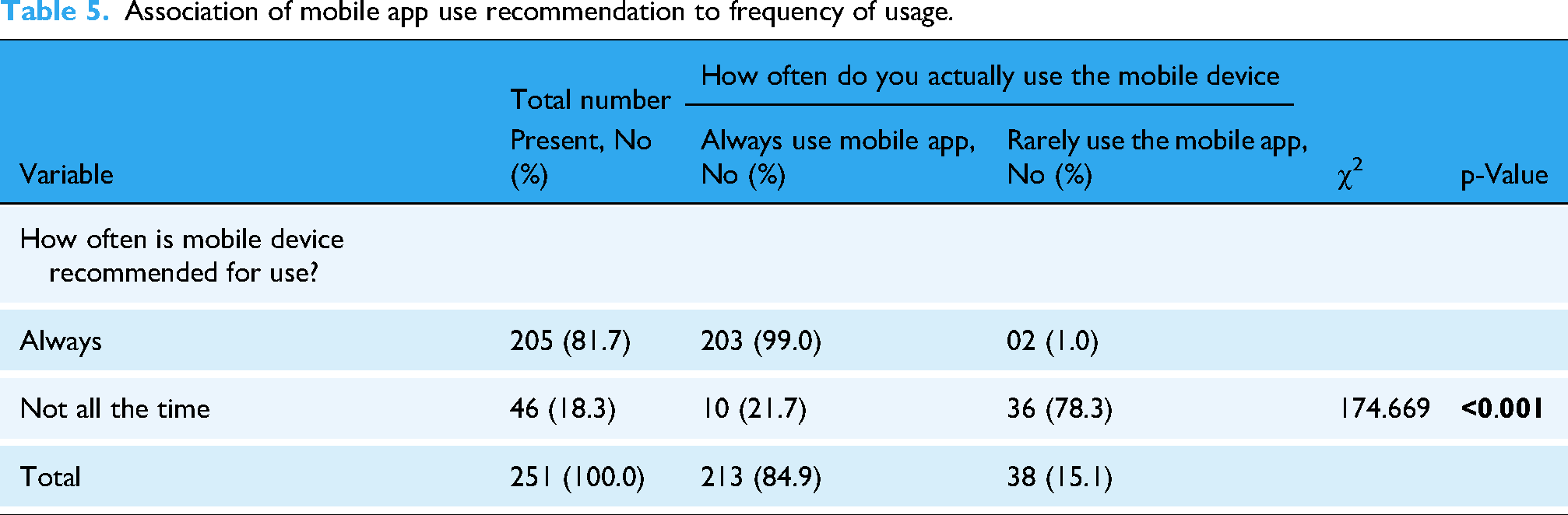
When asked how often they use mobile applications to collect data, the majority of the participants, equivalent to 85% noted they use it always. This indicates that the few who have not accepted the technology are those not adequately using the platform as recommended. More than three-quarters of the participants, equivalent to 82% of the participants, indicated that the use of mobile applications to deliver their work is “always recommended” to them at their job site.
FGD respondents supported these results, with participants citing how these gadgets help them deliver at work.
One participant, in particular, explained: “I use my phone to send monthly and activity reports. Without it, it would be difficult for me to do my job effectively”. (FGD Male participant)
All participants agreed with this sentiment, emphasizing that mobile phones are not just convenient but an essential tool for their daily work operations.
Whether or not mobile technology facilitated their work, almost all of the respondents (97%) agreed that mobile devices are of great help to them at their site of work.
FGD respondents supported these statistics as they highlighted various advantages of mobile devices facilitating their work, including easy accessibility and manipulation of data, and seamless triangulation of data using digital platforms. One of the participants specifically mentioned “that the main advantage of using digital platforms is that it provides them with quick and easy access to patient information, no matter where they are.” They can access all the relevant information about a patient from anywhere, without the need to visit a specific site. This is in contrast to paper-based systems, where they would have to physically visit the site to access the information. The participant further added that in facilitating their work, digital platforms eliminate the need for intermediaries to get access to patient information and enable them to make informed decisions quickly and efficiently. “The digital platform is best in facilitating my work because there, it's easier to manipulate and store data. And of course, from time to time, we can access our data at any time, even if we're at home, if, for example, we've left a document in the office and the management calls us at home saying that he needs a piece of data from that document. If we have the tablet with us, we can easily share the data with our superiors who ask for it, rather than thinking of how we will go to the office to get data from the document. So I think the digital platform is much better”. (FGD Female Participant)
Similarly, a majority of the respondents knew the name of the application/tool they used for work (Table 1).
Attitude of mHealth end-users.

For respondents who knew the name of the mobile application, a follow up on the name of platforms being used noted that Commcare and Scorecard were the most used platforms (Figure 2).
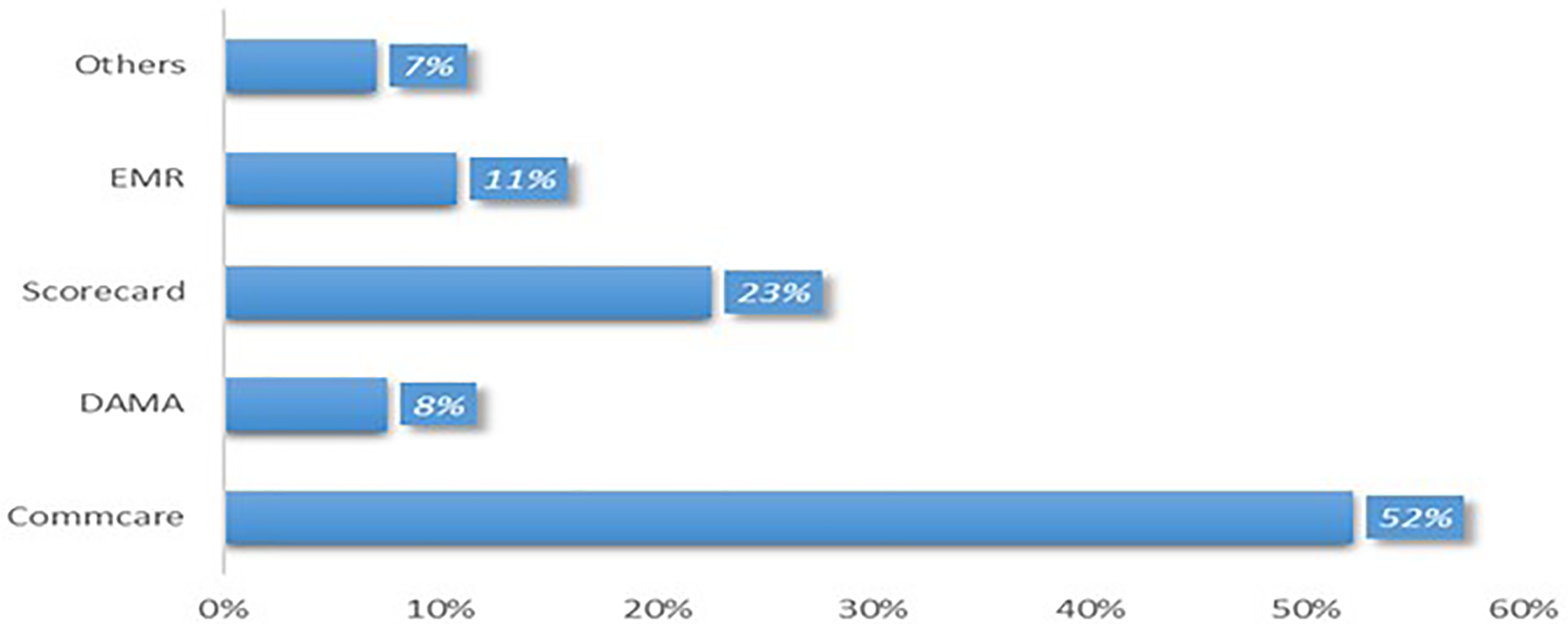
Platforms used for data collection.
Association of mHealth end-user attitude with sociodemographic factors
The quantitative study involved 251 participants from 4 regions: East (39.4%), Centre (24.3%), Adamawa (21.1%), and Littoral (15.1%). Twelve end-users declined to participate, and 25 end-users who had initially agreed to participate did not submit their questionnaires, taking the total number of participants down to 251. Participants were mostly aged 30 to 39 years (49%), with 40% aged 20 to 29 years. The majority had a university education (54%), while 71% had 1 to 5 years of work experience. End-users predominantly used smartphones for data collection and reporting (66.1%) (Table 2).
Sociodemographic characteristics of the study population (n = 251).

Age groups exhibited comparable mean attitude scores (F = 1.026, p = 0.382), suggesting age might not strongly influence mHealth attitudes. However, regional disparities were evident (F = 5.259, p = 0.002), with the Adamawa and Littoral regions showing higher mean attitude scores compared to the East and Centre regions.
Educational attainment significantly impacted attitudes (F = 13.45, p < 0.001). Participants with secondary, upper secondary level (General Certificate of Education, GCE advanced level), and university education levels displayed higher mean attitude scores compared to those with primary education. Conversely, work experience showed no significant association with attitudes (F = 1.648, p = 0.194), implying its limited impact (Table 3).
Association of mHealth end-user attitude (scale) with sociodemographic factors.

F: F-statistics; M: mean; SD: standard deviation.
The attitude scale variable was categorized into two categories (Good Attitude and Poor Attitude). The chi-square association test was used to test these categories for association with the demographic factors. End-users who work in the Littoral region were significantly more associated with a good attitude toward mHealth (p = 0.004) compared with those in the remaining 3 regions, whose attitude did not show any statistical significance. mHealth end-users with secondary academic qualifications were significantly more associated with a good attitude toward mHealth (p < 0.001) compared with end-users with other educational qualifications (Table 4).
Attitude of mHealth end-users by sociodemographic factors.

To determine if constant reminders to use mobile devices would encourage their actual use, the results showed that the more frequently their organization recommended the app be used, the more often the mobile applications were utilized, and this association was found to be significant (Table 5).
Association of mobile app use recommendation to frequency of usage.
A significant association was found between educational level and the preferred data capture method (χ2 = 20.349, p = 0.002). Participants with primary and secondary education levels tended to prefer paper-based documentation (forms and registers), while those with university education levels showed a stronger preference for mobile devices. Academic qualification emerged as a strong predictor of attitudes toward mHealth. There was a strong association between higher academic qualifications, ranging from Secondary to University level, and positive attitudes toward mHealth. Participants with Upper secondary educational backgrounds exhibited significantly greater propensities toward embracing mHealth compared to those with only primary education. This association persisted even after controlling for other variables, underscoring the independent influence of academic qualification on attitudes toward mHealth (Table 6).
Preferred methods of data capture by sociodemographic factors.
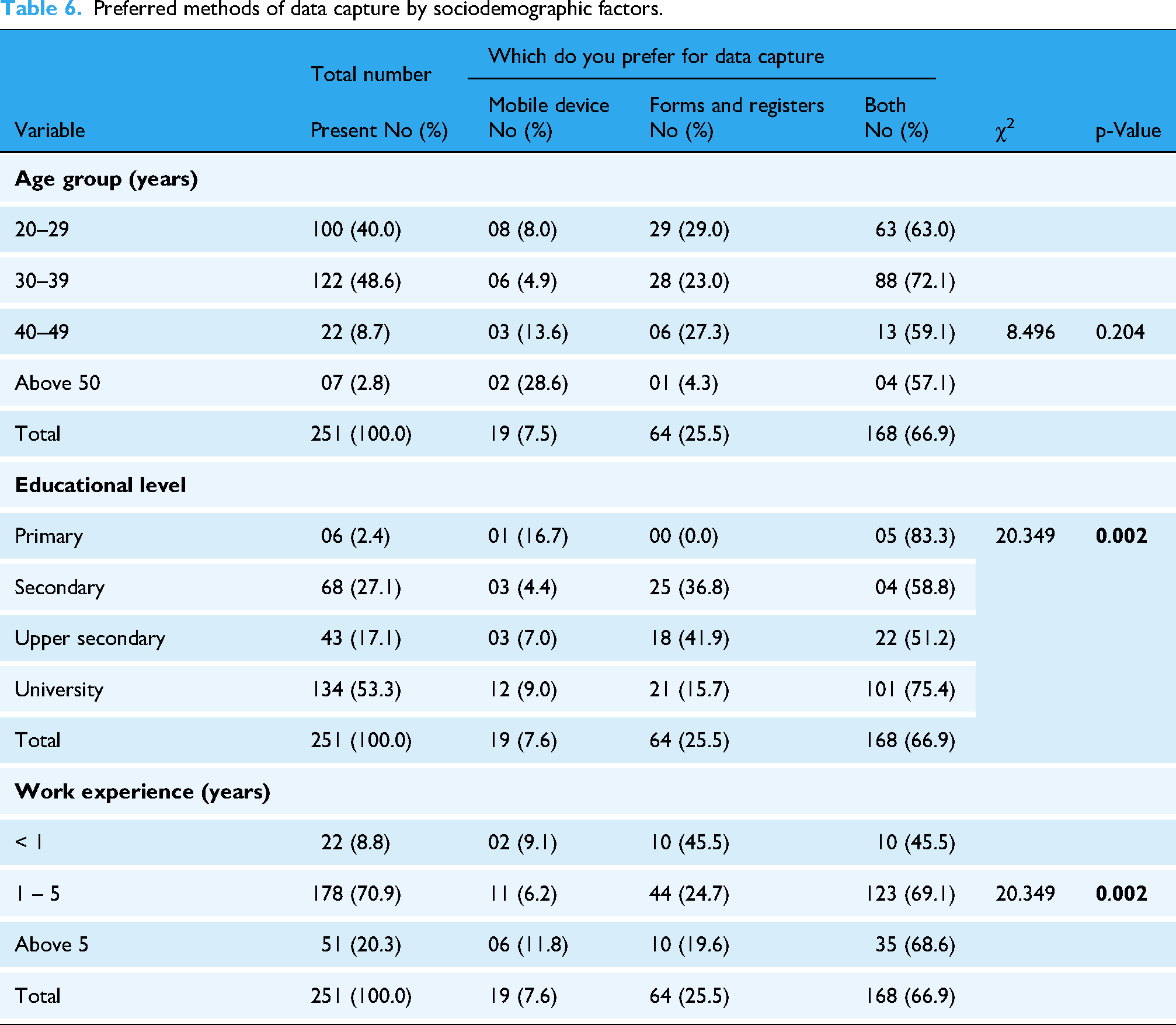
Additionally, there was a significant association between work experience and the preferred method of data capture (χ2 = 20.349, p = 0.002). Individuals with less than 1 year or above 5 years of work experience tended to favor paper-based documentation (forms and registers) while those with 1 to 5 years of work experience showed a higher preference for mobile devices (Table 6).
Participants from the Adamawa and Littoral regions had a significantly higher likelihood of possessing positive attitudes toward mHealth compared to their counterparts in the East region. Even after accounting for other variables, such as academic qualification and work experience, these regional differences remained significant, indicating that the region of work independently influenced attitudes toward mHealth (Table 7).
Determinants of end-users’ attitude towards mHealth.

AOR: adjusted odds ratio; COR: crude odds ratio.
Factors favoring mHealth use for M&E in Cameroon
Regarding mentorship, more than three-quarters (84.5%) of the respondents affirmed they get mentored on how to perform their respective tasks using a mobile device. A majority of FGD participants responded affirmed to this, with almost all of them stating that they do receive mentorship and assistance from experts within their organization. Participants cited specific individuals who offered them mentorship assistance, such as M&E officers, data managers, and project managers.
One participant in the FGD shared a personal experience, stating that: “The M&E officers and project managers attend to us when we face challenges and, on top of that, they're always reassured that the gadget is working normally and that it's giving us the information we need.” (FGD Female Participant)
Some participants also mentioned that distance is not a barrier when it comes to receiving mentorship. They stated that they can always contact their mentors through phone calls for directives when they get stuck in the course of using the device.
Overall, it was evident from the discussion that the respondents receive adequate mentorship and assistance from experts within their organization when it comes to using digital devices for their activities.
More so, over two-thirds (88%) of participants said they have standard operating procedures (SOPs) at their disposal to help them in their work. Region of work also played a crucial role; workers in the Centre region were less likely to have access to SOPs and formal training compared to those in the East, Ngaoundere, and Littoral regions (χ2 = 58.127, p < 0.001) (Table 8). Feedback from FGDs noted only a few participants who confirmed that they had received SOPs from experts in their organization on how to use digital devices. “As far as procedures posted somewhere are concerned, no, there aren't any SOPs. What we do is make use of the user manuals that come out of the equipment boxes, that's all”. (FGD Female participant)
Challenges faced by mHealth end-users.

When asked whether or not they face difficulties using their mobile device to do their job, 16.3% of respondents indicated they face difficulties. However, some FGD, participants cited challenges they faced while using mobile devices at work. They raised concerns about network issues and the tendency of devices to malfunction easily. While acknowledging these challenges, some participants suggested a mitigation strategy adding that paying keen attention to the quality of the tablets before purchasing them.
Job title significantly impacted the likelihood of facing difficulties, with nurses and psychosocial agents reporting more challenges compared to community health workers and data clerks (χ2 = 12.046, p = 0.017) (Table 8).
Seventy-nine percent of the respondents indicated they received formal training from their employer on how to use mobile devices to capture data. A strong correlation was found between the level of education and the receipt of formal training on using mobile devices, with those holding a university degree more likely to have received training (χ2 = 11.883, p = 0.018) (Table 8).
During FGD, participants highlighted the absence of secure storage space provided by their office for their devices. This lack of secure storage options led to various challenges, including instances where servers were lost due to limited means of equipment preservation. Participants expressed that the provision of secure storage facilities would help alleviate these issues.
Despite the absence of secure storage options, some participants mentioned that their organization has implemented measures to maintain device security, such as requiring individuals to sign documents acknowledging their responsibility for the devices. However, participants noted that these measures may not be sufficient to ensure device safety.
Participants also discussed reasons why their organization has not created secure storage facilities, citing security concerns and the lack of necessary security measures in their department.
Regarding the sustainability of mobile devices for data collection, participants overwhelmingly agreed that it is an efficient and practical approach that organizations should adopt. They emphasized the advantages of using digital platforms, such as preventing duplicate data and facilitating communication and information exchange among colleagues and collaborators. “Yes, and I in particular think that using a mobile device to collect data is a sustainable method that can last for a long time, and to me, this method should be embraced and congratulated because we're in a digital age. We have to keep up with the times. So, everything is digital and if we want to move forward, we have to adapt to technological change. So, I think it's the best thing ever”. (FGD Female participant)
Some participants emphasized the importance of ensuring the durability of mobile devices to improve sustainability. They suggested avoiding downloading certain content that could potentially damage the device, leading to malfunctioning and data loss due to formatting. Overall, there was a consensus among participants that utilizing mobile devices for data collection is a sustainable option for organizations aiming to streamline their data collection processes.
Discussion
Key findings from this study reveal that 78% of end-users had positive attitudes toward mHealth, preferring mobile applications over traditional methods due to ease of use and efficiency. Attitudes were significantly influenced by region of work and educational level, while age and work experience showed no significant associations. Key challenges included the need for better training, device reliability issues, and integration with existing systems.
These findings offer valuable insights into the current state of mobile health technology implementation in Cameroon. The outcomes are consistent with findings from numerous studies within the African region.9,10
Eighty-two percent of participants aged between 30 to 39 and 20 to 29 years displayed a positive attitude toward mHealth, with over 80% of them acknowledging its potential benefits. However, this association was not statistically significant, indicating that the observed differences could have occurred by chance. This finding contradicts the results of a study by Faqih, which found that demographic variables such as age and gender significantly influence the adoption of mobile technologies in healthcare systems in Jordan. 10 Similarly, this result contrasts with the study conducted by Babarinde in Lagos, where the younger 20- to 29-year-old end-user population was significantly associated with the use of mobile health. 11 Faqih's work focused on healthcare professionals and administrators, groups whose digital skills and roles systematically differ by age, while Babarinde's study targeted a younger end-user cohort within a specific program, naturally accentuating age-related adoption differences; by contrast, our study sample is broader and more uniformly trained, and because the mHealth platform has progressed beyond early pilot stages into scaled-up implementation with repeated mentorship and guidance, older participants have “caught up,” smoothing out any generational adoption gap.
Individuals with higher academic qualifications, ranging from secondary to university level, were more likely to have positive attitudes toward mHealth interventions. This association remained significant even after controlling for other variables, suggesting that academic qualification is an important independent predictor of attitudes toward mHealth. This finding aligns with the results of Osei's study in Ashanti, Ghana, where health workers with a secondary level of education were significantly associated with the use of mobile health. 12 Higher academic qualifications likely equip individuals with stronger eHealth literacy, the composite of traditional, health, information, media, scientific, and computer literacies, which in turn enhances both their perceived ease of use and perceived usefulness of mHealth tools. 13 Educated users are more accustomed to learning in technology-mediated environments, more confident in troubleshooting technical challenges.
We observed that end-users in the Littoral and Adamawa regions exhibited significantly higher mean attitude scores toward mHealth than those in the East and Centre regions. This pattern mirrors broader findings that regions with superior digital infrastructure and strong facilitating conditions report more favorable technology acceptance. 14
End-users in the Centre region were less likely to have access to SOPs compared with those in other regions. The Centre Region hosts the political capital city of the country (Yaoundé) and, as a result, hosts several main offices for health development partners. Most mHealth projects have been piloted and implemented in this region by various development partners. This places them in a position to adopt and use mHealth relatively faster, with minimal need for SOPs, compared to the other regions that participated in our study
We observed a high adoption rate of mobile applications for data collection, with 89% of participants confirming their usage. This underscores the acknowledgment and acceptance of the benefits that mobile technology brings to data gathering within the context of HIV programs. Most respondents reported frequent use of mobile devices for data collection, indicating that these devices have become integral to their data collection workflow. This preference for mobile technology is attributed to its convenience and efficiency in capturing and managing data in real-time.15,16 Eighty-two percent of participants indicated that the use of mobile applications for their work is “always recommended” at their job site. This suggests strong endorsement and support for integrating mobile technology into their work processes within HIV program implementation in Cameroon. The recommendation to use mobile applications highlights the recognition of potential advantages such as improved accuracy, timeliness, and ease of data collection and management.
Additionally, an overwhelming majority of respondents (97%) agreed that mobile devices are of great help to them at their work site, indicating the perceived value and usefulness of mobile technology in supporting their daily activities. This underscores that mobile devices significantly contribute to enhancing efficiency and effectiveness in delivering HIV services, aligning with findings from other studies. 17 Most participants highly recommend using mobile applications to perform work-related tasks, consistent with results reported by Rahman and colleagues in 2017. 18 Findings from FGDs further supported these results, with all participants expressing positive sentiments about the benefits of using mobile phones to enhance productivity. They emphasized that mobile phones are not merely convenient tools but essential components of their daily work operations.
There was a significant association between the frequency of organizational reminders for app usage and the actual usage of mobile applications. Specifically, the findings indicate that when organizations actively encouraged and recommended the use of the app, it positively influenced individuals’ behavior, leading to increased usage of the mobile applications. In other words, the level of organizational endorsement and promotion had a positive impact on the adoption and utilization of mobile applications. The significance of this association highlights the importance of organizational support and endorsement in driving the adoption and usage of mobile applications.19,20
Over three-quarters of participants reported that they do not encounter difficulties when using mobile devices to perform their job responsibilities. This suggests that a large portion of the participants feel comfortable and proficient in utilizing mobile devices as tools for their work-related tasks. Ease in using mobile devices implies that they have the necessary skills, knowledge, and confidence to effectively leverage these devices in their job roles. This positive sentiment toward mobile device usage for work suggests a favorable integration of technology into the workplace and highlights the potential benefits and efficiency offered by mobile devices in supporting job performance. This is also backed by the fact that a significant majority of respondents (84.5%) affirmed that they receive mentoring on how to perform their respective tasks using a mobile device. This indicates the recognition of the importance of guidance and support in effectively utilizing mobile technology in their work. The provision of mentorship suggests a commitment to enhancing the participants’ skills and knowledge in leveraging mobile devices for improved job performance within the context of the HIV program. This finding is consistent with Meeks’ research, which identified that supervision (mentorship) interventions had a significant positive effect on the use of mobile health applications. 21 Even though over two-thirds of participants (88%) reported having SOPs at their disposal to assist them in their work, FGDs revealed that the participants had a poor understanding of what they termed SOPs, as these SOPs were mostly absent. Participants, however, received guidance and mentorship on how to use these devices. This contradicts work by Jembai in Malaysia, where more than 90% of respondents acknowledged the availability of SOPs, especially during the COVID-19 era. 22 SOPs are organizational documents that provide standardized guidelines and procedures and help ensure consistency, quality, and efficiency in their tasks.
Although over two-thirds of participants reported having SOPs, FGDs revealed poor understanding and limited actual availability, highlighting a critical disconnect between policy and practice in digital health implementation.
A handful of participants indicated that they encountered challenges. These difficulties encompass a range of issues from technical problems, usability concerns, and connectivity issues, to insufficient training or support. Identifying these challenges is essential for addressing barriers and improving mobile devices’ overall user experience and effectiveness in their work processes.
One noteworthy finding was that psychosocial agents faced a greater array of challenges compared to other respondents. This suggests that the nature of their work, which likely involves providing emotional support and counseling, may present unique obstacles when utilizing mobile devices. Understanding these challenges can help organizations develop targeted strategies to address the specific needs of psychosocial agents. Integrating digital health courses into the training curricula for health professionals can empower them to utilize mobile devices more effectively in data management and communication tasks.
Conclusion
This study reveals a predominantly positive attitude among end-users toward integrating mHealth technologies into HIV program monitoring in Cameroon, consistent with trends observed across sub-Saharan Africa. While age was not a significant factor, academic qualification emerged as a key predictor of mHealth receptiveness, highlighting the need for capacity-building efforts tailored to varying educational backgrounds. The strong organizational support for mHealth, coupled with high uptake for data collection and reporting, highlights institutional readiness and the potential scalability of mobile technologies in program monitoring.
However, persistent challenges, particularly among psychosocial workers, point to gaps in training, infrastructure, and contextual adaptation of digital tools. These findings call for differentiated implementation strategies that consider cadre-specific needs and foster inclusive digital literacy.
At a broader level, the results affirm that successful integration of mHealth into HIV monitoring systems requires more than technological availability; it demands sustained institutional support, equitable workforce capacity development, and secure data management systems. As countries move toward digitizing health information systems, especially in the context of HIV, these insights contribute to shaping scalable, human-centered, and sustainable digital health strategies. Further longitudinal and implementation research is recommended to assess long-term adoption patterns, impact on health outcomes, and system-level integration across diverse contexts.
Study limitations
The findings were not validated by the respondents, which could have potentially enhanced the work. However, the authors possess substantial knowledge of digital health, which supports the credibility of the results.
Nonresponse of over 25 participants. This reduction in sample size could have lowered the statistical power of our analysis.
The study did not disaggregate the quantitative sample by gender, which limits the ability to assess potential gender-related differences in attitudes toward mHealth.
Footnotes
List of abbreviations
Acknowledgments
The authors would like to express their sincere gratitude to all the participants who contributed to this study. Your willingness to share your experiences, insights, and time was invaluable to the success of this research.
ORCID iDs
Ethical approval
This study was obtained from the Institutional Review Board of the Faculty of Health Sciences, University of Buea, Cameroon, Ref: 2020/1241-06/UB/SG/IRB/FHS. All participants provided informed consent before their inclusion in the study. Participation was voluntary, and confidentiality was assured throughout the research process.
Informed consent
Written informed consent was obtained from all participants before their enrollment in the study; end users who did not provide consent were excluded.
Contributorship
FSN, ON, ALN, and PJN were involved in conception and design; FSN, ON, and NT in administrative support; FSN in provision of study materials or patients; and FSN, ON, CSA, and JNO in collection and assembly of data, data analysis and interpretation. All authors contributed to manuscript writing and final approval of manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Gurantor
FSN is guarantor of this work, who has full access to all the data in this study and take responsibility for the integrity and accuracy of the data.
Peer Review
This article was not commissioned and was submitted to the journal as an original research manuscript. It has undergone external peer review by independent experts. All reviewers were selected by the journal, and the authors have addressed the reviewers' comments and revised the manuscript accordingly. The final version has been approved by all authors and is submitted for publication consideration.