
Abstract
An electronic audit and feedback (e-A&F) system was developed to support healthcare providers’ awareness of their own performance, improve delivery of care and ultimately the safety of patients while in hospital. The point-of-care e-A&F system provides healthcare providers, from a 600-bed tertiary hospital in Western Australia, with near real-time feedback via web-based dashboards. The aim of this evaluation is to determine the implications of e-A&F across multiple dimensions and domains of care in a tertiary hospital setting. The study also aims to address the paucity in the literature by validating hypothesised design and implementation mechanisms on its effectiveness. Key datasets to be examined include those related to patient outcomes, staff behaviour and costs. Quantitative methods, such as interrupted time series analysis and multiple logistic regression analysis, amongst other methods, will be employed to achieve these aims.
Introduction
Patients can experience unintentional but potentially avoidable harm in hospital, which, in addition to the impact on the individual patient, can have broad social and economic consequences.1–3 In Australia, which is widely 4 considered to have a well developed healthcare system, one in nine people admitted to hospital will experience an adverse event. 5 A patient who contracts an infection during hospitalisation and requires a longer stay epitomises these all too common occurrences.5,6 If this particular event were to be examined, it is possible that healthcare provider hand contamination could be found to represent a modifiable risk factor for this patient outcome, which another organisation, with greater compliance in professional practice standards, may have been able to avoid. 7
A Cochrane review of 140 randomised control trials investigating the effect of audit and feedback on healthcare professional practice found that the median absolute improvement was 4.3%. 8 Although this pooled estimate is arguably small a wide range of effect estimates was found. This included an upper quartile of 16.0% improvement in compliance, which suggests that audit and feedback can be a useful intervention to improve delivery of care and patient outcomes in some settings.8–12 The range in study findings also supports the widely held view that the individual features of an intervention can substantially influence its effectiveness.13–16
The Clinical Performance Feedback Intervention Theory (CP-FIT), developed to define these specific features, suggests that successful feedback is achieved through a series of sequential processes. 13 The CP-FIT is a comprehensive framework based on a systematic review of qualitative audit and feedback studies and provides specific design recommendations. 13 The theory suggests that the process of successful audit and feedback involves the identification of standards of clinical performance against which care will be measured; the collection and analysis of performance data; communication of the measured performance to healthcare providers; reception, comprehension and acceptance of these data by health professionals; a planned behavioural response and ultimately improvements to patient care. 13
Given the unacceptable proportion of patients who continue to experience unintentional and potentially avoidable harm during hospitalisation, a reduction of this harm should be seen as a collective priority. Accreditation programmes are one approach that national governments have employed to address this unintentional and potentially avoidable harm and help provide quality assurance in hospitals.5,17 Although global accreditation programmes differ in detail, there has been convergence over time towards a broadly similar model.18–24 In Australia, hospitals and day procedure services are accredited against the National Safety and Quality in Health Service Standards (the ‘National Standards’).
Evidence of compliance with the National Standards is required by Australian hospitals to achieve accreditation status (see Table 1 below).25,26 In 2017, a Western Australian tertiary hospital commenced development of a novel electronic audit and feedback (e-A&F) system, Consumer-Engaged National Standards Audits (CENSAs). This system was designed to collect evidence against the National Standards, support staff to learn about their performance, and improve delivery of care.
Summary of Australian National Standards. 25

CENSAs offers healthcare providers with near real-time feedback via web-based dashboards which utilise the business intelligence tool Tableau© (Seattle, WA). Data are entered at the bedside on mobile devices by trained auditors using a web-based data collection tool and stored in the secure health service data warehouse. Data validation processes, governance oversight and auditor training provide quality assurance. The dashboards, which are refreshed daily, provide feedback for each work area in the form of quality indicators aligned to the eight overarching National Standards (see the example Figure 1: CENSAs Dashboard Standard 4 – Medication Safety).
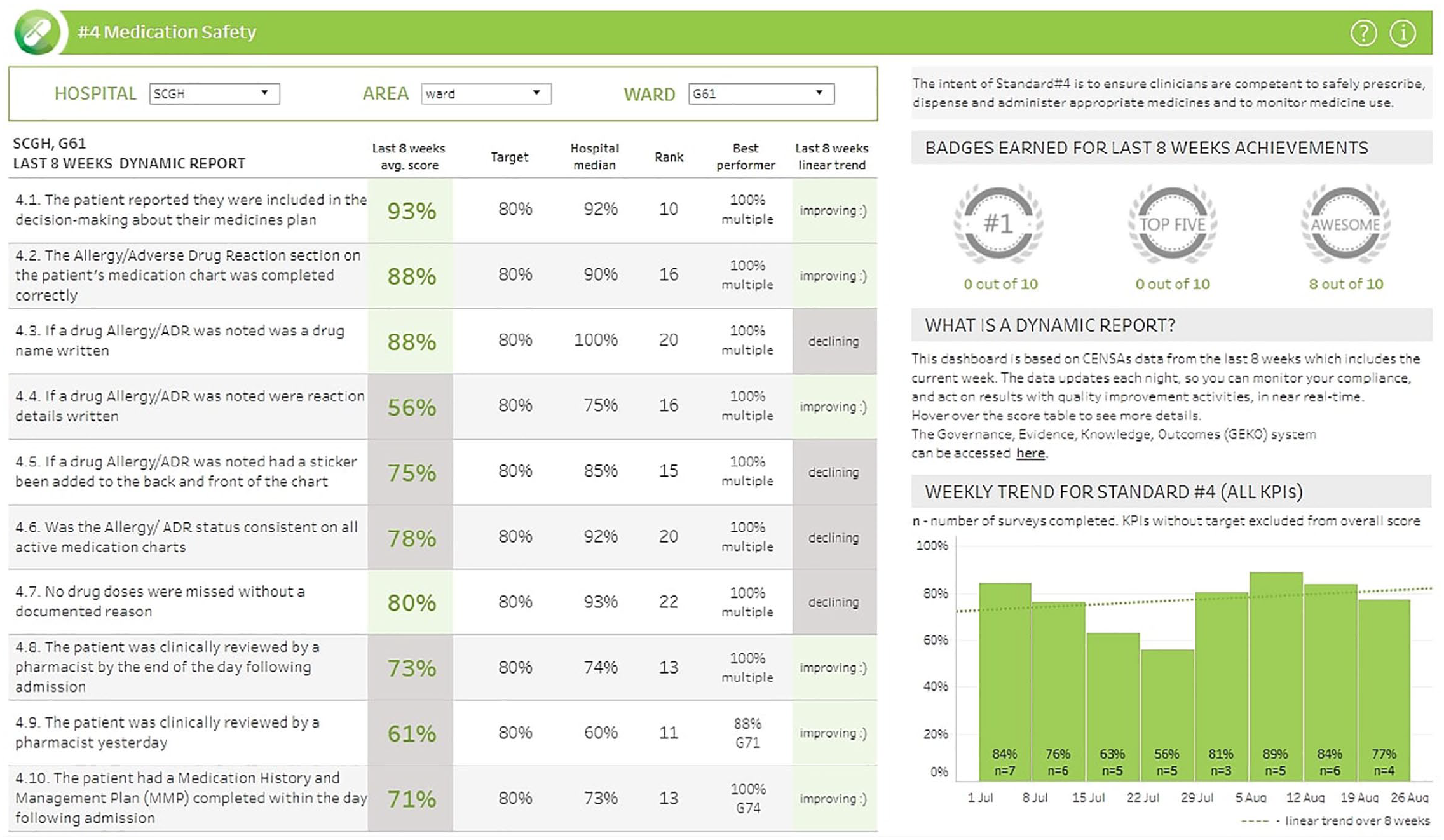
CENSAs Dashboard Standard 4 – Medication Safety.
CENSAs data collection and reporting tools were launched in May 2018 and August 2018 respectively. The quality indicators collected and reported by CENSAs were identified during a rigorous development process that was supported by expert clinical input. A set of criteria for selecting quality indicators was applied over a number of improvement cycles including: clinical impact and relevancy, monitoring feasibility and feasibility to action non-compliance. A process of validation and beta-testing was undertaken on three surgical and three medical wards. CENSAs was also linked to a quality improvement registry and management system to support staff addressing identified deficiencies in clinical practice.
There is some evidence that audit and feedback can improve compliance with desired clinical practice. 27 However, little is known about the effects of these programmes when coordinated at a hospital-level and directed at different domains of patient care, such as policy, patient safety culture, guideline adherence and patient outcomes.8,12 The increasingly widespread availability of electronic health records and web-based technologies also necessitates closer examination of e-A&F, as compared to audit and feedback more broadly. 28 One systematic review 29 attempted to summarise findings from healthcare e-A&F studies but due to the small number of published studies available and the high level of heterogeneity, it was limited in its ability to make conclusions on the effect size or recommendations on implementation approach and design features.
Study aims and objectives
The first aim of this study is to assess the effectiveness of an e-A&F tool, CENSAs, on patient safety in a tertiary hospital setting. The study will address this aim by evaluating the rates of hospital-acquired complications (HACs) pre- and post- implementation of CENSAs, and will determine the cost-effectiveness of the intervention. The study also aims to examine the potential factors influencing the effectiveness of CENSAs on patient safety, and add evidence to the existing literature on design recommendations of e-A&F systems. This aim will be achieved by comparing the features of the e-A&F system against the hypothesised CP-FIT, such as the characteristics of feedback, characteristics of the organisation and characteristics of the recipients.
Methods
Study design
Interrupted Time Series (ITS) analysis, a quasi-experimental approach, will be used to assess the change in the rates of HACs before and after the introduction of the e-A&F system. Subsequently, the Incremental Cost-Effectiveness Ratio (ICER) methodology will be used to assess the cost-effectiveness of any detected change in the rate of HACs. To help explain causes for the effectiveness of the e-A&F both ITS analysis and descriptive analysis will be used to compare the features of CENSAs against the hypothesised CP-FIT.
Setting
The study will be conducted at a 600-bed tertiary teaching hospital in Western Australia in which the novel e-A&F has been implemented. The hospital is representative of the breadth of tertiary healthcare in Australian hospitals including being equipped with: a 24-hour emergency department; an Intensive-Care Unit and other specialised units such as cardiac surgery, neurosurgery, infectious diseases and organ transplant. 30
Outcomes
The intention of the National Standards, which predominately relate to professional practice and clinical processes, is to reduce the occurrence of unnecessary harm. For example, Standard 3 – Preventing and Controlling Healthcare-Associated Infection, requires the implementation of practices and processes to reduce healthcare-associated infections, such as healthcare-associated urinary tract infection. It is then unsurprising that compliance with the National Standards has been illustrated to reduce the occurrence of a set of nationally recognised hospital-acquired complications (HACs) (see Table 2). 31 Outside the Australian setting comparable clinical practices and processes have also been shown to improve patient outcomes. 32 Therefore, CENSAs, aligned to the National Standards, could be expected to mediate the rate of HACs, an important priority for both healthcare providers and patients to reduce.
Hospital-acquired complications. 31

We will assess, as the primary outcome of this study, what the longitudinal effect of the implementation of CENSAs has been in the rate of HACs. In addition, CENSAs, as a point-of-care audit system, has anecdotally permitted timely intervention from healthcare providers where unsafe practices have been detected. As a result, as a secondary outcome, we will evaluate the patient-level, or the average effect that could be expected for an individual patient, of CENSAs on HACs.
We will use the results of these HAC analyses to inform a cost-effectiveness analysis, by using the avoidance of adverse events as the effectiveness value in the denominator, also as a secondary outcome measure. 33
A key aspect of the CP-FIT is a planned change in behaviour which leads to improvements in care delivery. 13 Thus, we will evaluate the change in the count of quality improvement activities commenced and completed by staff as a secondary outcome measure and a possible factor which could explain the effectiveness of the implemented system. Analysis of systematic staff behaviour change will be supplemented by descriptively exploring the features of the CENSAs system that could explain its effectiveness.
Data sources and sample
A number of retrospective datasets will be utilised for the analysis. These datasets will be extracted from the health service data warehouse. An inpatient administrative dataset, which contributes to the WA Hospital Morbidity Data Collection (HMDC), will be the primary data source for the HAC analysis. 34 The sample will include the 4.5-year pre-implementation phase (2014–2018) and 2.5-year post-implementation phase (2018–2020) for all overnight inpatients. Data fields to be extracted include perturbed medical record numbers, age, sex, admission and discharge dates, admission type, discharge specialty, diagnoses, procedure codes, hours spent in ICU and condition onset flags.
The entire CENSAs dataset will be extracted for analysis including perturbed medical record numbers, audit date, audit length, patient specialty, ward and categorical compliance measure fields. The CENSAs and inpatient datasets (for the post-implementation phase) will be linked for the patient-level HAC analysis. This data linkage process will utilise the unique patient identification codes and date fields with a probabilistic match algorithm.
We will utilise the approach of other cost-effectiveness studies by using the avoidance of adverse events as the effectiveness measure in the denominator. 33 Costs will be divided into intervention-related costs and outcome-related costs. The costs of HACs as adverse event outcomes will be approximated using the Australian Independent Hospital Pricing Authorities’ approach to HAC penalties. 35 The Australian Government approach to HAC penalties are that they reflect the extra cost of a hospital admission with a complication. 35 This additional cost may be the result of a more complex episode of stay or due to an increase in the length of an ordinary stay, and is adjusted based on a number of risk factors. 35 Key costs of the intervention will relate to the nursing time for audit data collection. 36 The additional nursing time for audit data collection will be determined by approximating the time required to complete an audit using the start and finish time stamps from the audit dataset. Other costs such as administrative, project, and overhead hospital costs will be estimated using the Australian National Hospital Cost Data Collection Cost Report.37,38
To evaluate the change in the count of quality improvement activities commenced and completed by staff between the pre- and post- implementation periods we will undertake an extract from the state quality improvement registry and workflow software. This system supports staff organisation to create, manage and record quality improvement activities. All submitted quality improvement activities undergo review and assessment by quality improvement committees to promote consistent quality data being recorded in the system. Data fields such as the activity type, specialty undertaking the activity, staff participating in the activity, the National Standard the activity aligns to, proposal approval date and activity completion date will be extracted.
To complement the assessment in change in quality improvement activities we will examine dashboard usage logs as a possible mechanism explaining the effectiveness of the implemented system. 39 This approach benefits from quantitative and unobtrusive insight into clinical staff behavioural processes. 40 We will extract from Tableau© (Seattle, WA) individual access data and the accompanying professional profiles of staff, including the area of employment and profession.
A clinical staff survey will also be undertaken using an online questionnaire tool that we will develop. Clinical staff active in governance structures and committees, such as senior nursing staff who are most likely to have had involvement with the system, will be in scope for participation in the survey. Governance structures and committees will be invited to nominate names of staff for participation. We will initiate contact with potential participants via email. Information about the purpose of the study and how the results will be used will be provided in this initial contact. Survey questions will be based on concepts from the CP-FIT, including the reception and context of health professionals receiving feedback. 13 Employee information (e.g. role, area of employment) will also be collected as part of the online questionnaire. We will pilot test the survey tool with clinicians for clarity, length and flow of questions with any amendments made as necessary. The online tool will be hosted on REDCap® (Research Electronic Data Capture), a secure, web-based platform.
Covariates
HACs will be identified using nationally agreed specifications of International Classification of Disease – Tenth Revision – Australian Modification codes, and condition onset flags.35,41 Condition onset flags can be used to help to distinguish pre-existing conditions from those arising during hospitalisation. 42 While a widely available source of clinical information, the limitations of administrative datasets to accurately and comprehensively record information such as secondary diagnoses is well established. 43
Nationally agreed risk factors that will be used as covariates in the patient-related analyses include: emergency admission status (‘yes’ or ‘no’), patient age group (in 5 year increments), Major Diagnostic Category, hours spent in an Intensive Care Unit, Diagnostic Related Group type (‘medical’ or ‘intervention’), Charlson Comorbidity Index Score, sex and transfer status (‘transferred from another hospital’ or ‘other’).35,41
Data analysis
We will use an ITS analysis to determine if specific time periods (across pre- and post-intervention periods) are associated with measurable changes in patient outcomes and staff behaviour. The benefits of the approach, as compared to other quasi-experimental designs, is that it avoids internal validity biases such as those related to secular trends.44,45 Time series plots will be used initially to explore the unadjusted effects of the intervention and presence of trends, cyclical patterns and outliers. 46 A segmented regression analysis will then be undertaken using discrete intercepts and slopes for the periods before and after the implementation of CENSAs.44,47 Results will be interpreted for both level and trend changes, from before and after the intervention, with 95% confidence intervals. 46 For the patient-level analyses we will perform multiple logistic regression analysis comparing the rate of HACs in audited and non-audited patients and controlling for risk factors. 35
We will assess the cost-effectiveness of CENSAs as an e-A&F intervention using the ICER methodology. ICER is useful in that it can examine both the marginal health benefits for increasing cost burden. 37 The ICER will be assessed using longitudinal multi-year time horizon perspective comparing the implementation of the e-A&F system to a scenario of a continuation of existing practice. All cost will be reported in 2020 Australian dollars.
Descriptive analyses will be undertaken to explore possible features of CENSAs that could explain its effectiveness. In reporting the behaviour of staff in their use of the dashboards we will focus on the extent to which each National Standard dashboard is used and how this varies between professions, clinical areas and over time. 39 In addition, CENSAs indicator data will be assessed to determine: if changes in patient outcomes are associated with performance with National Standards; how they vary between clinical areas and how they vary over time. These results will be reported alongside the results of the clinical staff survey that will focus on other aspects of the CP-FIT.
Statistical power
In the pre- and post- analysis the total rate of HACs across the intervention periods will be expressed monthly over 7 years (84 monthly time points in total). While there are no fixed recommendations on the minimum number of time points required for ITS analysis, as power is dependent on factors such as data variability and presence of confounding effects, some studies have suggested 40–50 observations as a guide.48,49 The count of quality improvement activities will be expressed bi-monthly over the same time period (42 time points), therefore also meeting guidelines for robust statistical ITS design analysis. 46
In addition, a minimum of 100 observations can improve the stability at each time point.46,50 From 2014 to 2020 there are expected to be approximately 210,000 episodes and 16,800 HAC endpoints. Therefore, a sufficient sample size to ensure stable estimates is expected. The minimum number of observations of quality improvement activities per time period is also expected to be met.
The analysis of the patient-level effect of CENSAs on the rate of HACs anticipates a small-to-moderate effect on patient outcomes (i.e. HACs). A 10% change from the baseline (of approximately 8%) is expected.8,11 To detect even this small-to-moderate effect a total of 10,000 audited patients will be sufficient, using a type I error (alpha) of 5%, and 80% power.
Statistical power and sample size considerations for cost-effectiveness analysis require the calculation of confidence intervals for the incremental costs and effects and thus will be performed following the preliminary analyses. 51 The remaining analyses will be reported descriptively and do not therefore do not require consideration of necessary sample sizes as no standardised rules exit.52,53
Conclusion
We propose to evaluate the effectiveness of an e-A&F intervention for patient safety in tertiary hospital care in an Australian setting. Quantitative analysis of time series data, controlling for historical outcome trends, will be used to provide evidence of the intervention’s impact. Staff behaviour and views will also be used to better understand the mechanisms responsible for any change in the patient outcomes from the intervention.
This study will provide insight into e-A&F organised at a hospital-level and directed at different domains of patient care.8,12 As an illustrative example and with many individual elements of CENSAs reproducible, results may provide a guide for other hospitals and healthcare organisations in the process of implementing and evaluating e-A&F. The results will also guide future research that aims to understand how to achieve improvements in patient safety more broadly.
Footnotes
Author contributions
JS conceptualised the project and drafted the manuscript. DP, KM and TM reviewed and edited the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Research Governance Office of the Sir Charles Gairdner Osborne Park Health Care Group approved the study on 29 January 2020 (reference: RGS0000003231). Research governance approval was also received by the University of Western Australia (reference: RA/4/20/5794). A waiver of consent was provided to utilize information from retrospective datasets. Participants in the survey will however be individually consented.
Patient and public involvement
The CENSAs system development and implementation has been overseen by a key hospital governance committee represented by a member of the hospital Consumer Advisory Committee. Research findings, in addition to dissemination via traditional academic processes, will also be shared through non-academic processes including to the Consumer Advisory Committee and patients for their consumption while visiting hospital.