
Abstract
Introduction
Audit and feedback is a widely utilised quality improvement strategy to improve professional practice in healthcare. 1 Fundamentally, audit and feedback involves informing health professionals that their clinical practice is inconsistent with a desired target, to prompt change. 1 Despite audit and feedback being widely utilised, a Cochrane review concluded considerable variability exists in its effectiveness, with sizeable interquartile range of 0.5 to 16.0% reported. 1
These findings suggest that by examining and emulating the features of those more effective interventions, a greater level of clinically significant improvements could be achieved. To date, evidence-based guidelines to support successful implementation of audit and feedback in healthcare have largely been lacking.2,3 To address this gap, recent feedback theories have been developed from findings of qualitative research. 4 These theories suggest that effective feedback works in a cycle over time. This cycle is influenced by variables related to the feedback itself, the recipient and the wider context. 4
At the same time, the digitisation of healthcare is increasing the availability of health data in an electronic format, which in turn has the potential for use for electronic Audit and Feedback (e-A&F). 5 By extension, there is evidence of this increasing integration of ICT into healthcare quality improvement strategies. 6 When health Information and Communication Technology (ICT) is used in conjunction with audit and feedback processes within clinical settings, it is commonly referred to as e-A&F.5,7 In this paper, we use the term e-A&F broadly to encompass all approaches which provide an electronic “summary of clinical performance of health care over a specific period of time to inform quality improvement actions”. 1
The potential benefits of the use of ICT for audit and feedback may mirror the greater adoption of digitisation in healthcare, including improving workflows, real time access and greater efficiency. 8 However, it has been established that the use of a computer or being online can influence behaviour. 9 Therefore, despite the potential benefits there could be expected to be differences in practice as compared to traditional audit and feedback.
Some research has commenced examining e-A&F across the healthcare sector. Key previous reviews have considered the healthcare sector more broadly, including aged, primary and hospital care settings.5,6,10 However, feedback in relation to a hospital setting requires specific considerations. Previous reviews have also identified studies to be highly diverse.5,6,10 So, efforts to develop evidence-based guidelines from standard systematic review methodology, such as meta-analysis, have been unreliable.5,6,10 Thus far, the only approach has been via narrative synthesis of the literature.5,6,10
As more than a decade has passed since the seminal Cochrane findings on audit and feedback, it is appropriate for a quantitative systematic review to be undertaken that focuses on the emergent literature. This includes literature with a particular focus on e-A&F in a hospital setting.
1
To achieve this aim, the following objectives will be pursued: 1. Scoping the existing research of contemporary audit and feedback systems for patient safety and quality in hospitals. 2. Quantitatively examining the features of these systems to determine if there is a link between the nature and pattern of these features and the effectiveness of systems.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement for reporting our systematic review. 11 Our approach was published on the International Prospective Register of Systematic Reviews (PROSPERO; registration number CRD42020167008). 12
Search and selection
Search criteria according to the population, intervention, comparator, outcome and study (PICOS) and typical exclusion examples.
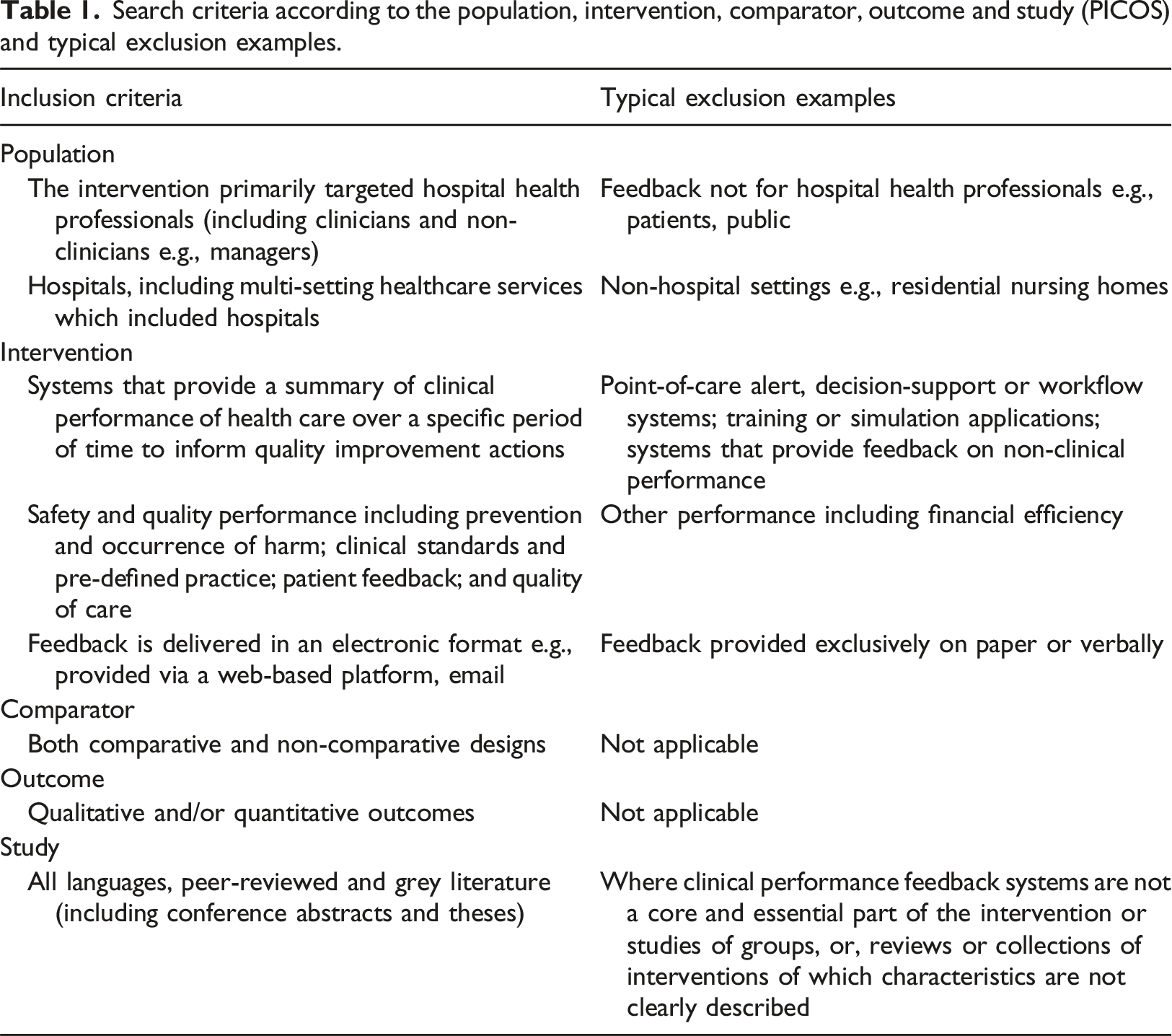
Full manuscripts of relevant papers were obtained by one reviewer, double checked by a second reviewer, with the inclusion criteria re-applied. Citation and reference list and related article searching were undertaken for all full publications meeting the inclusion criteria using the Web of Science. Reasons for deeming full publications to be irrelevant were recorded. During this step, to meet the first objective, basic characteristics of publications were extracted, including publication year, country of origin of study, feedback topic, targeted health professional category and publication type / study design. Where these characteristics were not stated, these were recorded as “unknown”.
Data extraction and analysis
Effect size study publication e-A&F system examples of strong and weak features.

To meet the second objective, to examine the association with effectiveness, these features were classified using a 0/1/2 scoring system. This was defined as ‘2 = Strong’ (substantive evidence that it met the definition of the feature), ‘0 = Weak’ (substantive evidence that it did not meet definition of the feature), and ‘1 = Neutral’ (either insufficient evidence to assess, or mixed weak and strong evidence).5,31 The primary outcomes were also coded as either positive, coded = P, (i.e., the outcome supported the hypothesis) or mixed/negative, coded = N, (i.e., the outcome did not support the hypothesis or there were mixed results). The mean score differences for positive and mixed/negative were compared to produce Cohen’s d effect sizes for each feature. These were interpreted using conventional thresholds – small (0.20), medium (0.50) and large (0.80).32,33
Risk of bias
Risk of bias for individual studies was assessed using the Mixed Methods Appraisal Tool (MMAT) by one review author and checked by a second reviewer for each criterion.34–36 Agreement was reached by consensus. In addition to the risk of bias at the individual study level, there exists the potential of a risk of bias across studies. The chosen methodology was expected to reduce the risk of the effect of positive publication bias. The methodology employed by other systematic reviews involves the aggregation of effect sizes across published studies to produce estimated pooled averages. Therefore, any presence of positive publication bias will ultimately bias the estimated pool average. 37 Our approach was to group and compare publications by the features of their interventions. We argue there is no clear reason why the features of an e-A&F intervention would systematically bias whether it was published. In addition, we chose to include grey literature and utilise a comprehensive search strategy. This broad scope would help in reducing the bias towards publishing positive outcomes only.
Results
The electronic bibliographic databases and additional searches (Google Scholar, citation and reference list searches) yielded an initial total of 5055 unique publications, of which 151 met the criteria for full text screening. After full review, 39 studies were excluded as a result of not meeting the eligibility criteria. Following the updated search in July 2022, a total of 152 publications were included in the descriptive synthesis, with 63 of these also in the effect size synthesis (Figure 1). Flow chart of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol. A total of 6018 were identified from database search and 31 from other sources. After removing duplicates 5055. Title and abstracts of 5055 were screened. Of these, 151 remained and were full-text assessed for eligibility. Of these, 112 were included in the descriptive synthesis. Following a database update search in July 2022 152 were included in the descriptive synthesis and 63 in the effect size synthesis.
Current state of e-A&F, number (%) of publications by characteristics.

From 2011 to 2021, the final full year of the study period, the number of publications increased annually, from six to 17, representing 3.9% and 11.2% of the total, respectively. During the same period, effect size study publications also increased annually, from two to 9, representing 3.2% and 14.3% of effect size studies, respectively. Taking into consideration the final year of the study included up to June, the number of publications overall was found to increase year-on-year, equating to an average change of 1.1.
For publications overall, close to half were found to originate from the United States (n = 76, 50.0%), followed by the United Kingdom (n = 19, 12.5%) and the Netherlands (n = 18, 11.8%). Countries of origin with small frequencies overall were grouped by geographic regions. One international study publication was categorised as having a Multi-country (n = 1, 0.7%) origin. Similarly, when effect size study publications were examined, the United States (n = 40, 63.5%) was the largest country of origin however this was followed by Europe - other (n = 7, 11.1%), United Kingdom (n = 4, 6.3%), and Canada (n = 4, 6.3%).
Categories were used to group the feedback topics of interventions into specific clinical processes, such infection control, or broad clinical specialties, such as cardiovascular. The largest feedback topics for publications overall were Anaesthesia and surgery (n = 21, 13.8%), Critical care and pain (n = 20, 13.2%), and Infection control (n = 19, 12.5%). Where an intervention covered more than a single feedback topic, this was categorised as More than one (n = 14, 9.2%). There was some overlap between the breakdown of the feedback categories overall and for effect size studies. For effect size studies, the largest feedback topics were Infection control (n = 14, 22.2%), Critical care and pain (n = 10, 15.9%), and Medications (including antimicrobials) and venous thromboembolism (n = 10, 15.9%).
Trends of health professional group targets of feedback were broadly consistent for publications overall and for effect size studies. Where feedback was specifically provided to a single professional group, this was most often directed to Doctors (n = 45, 29.6%). Single health professional groups associated with fewer interventions included Nurses (n = 15, 9.9%) and Pharmacists (n = 1, 0.7%). The largest cohort of interventions provided feedback to Multi-disciplinary health professional teams (n = 25, 16.4%). Other non-specific health professional groups targeted included Senior leaders and managers (n = 3, 2.0%), including administrative management. A sizeable number of publications, Unknown (n = 25, 16.4%), did not specify the health professionals who were the target recipients of e-A&F feedback.
Following Multi-disciplinary health professional teams, Doctors were the largest targets of interventions. Doctors were found to be disproportionally associated with a number of feedback topics. The proportion of Anaesthesia and surgery interventions which targeted Doctors (n = 13, 61.9%) was substantially higher than those that targeted Multi-disciplinary teams (n = 7, 33.3%). These differences also applied to Medications (including antimicrobials) and venous thromboembolism interventions which targeted Doctors (n = 10, 71.4%), compared to Multi-disciplinary teams (n = 3, 21.4%), and Clinical communication and patient flow interventions which targeted Doctors (n = 4, 50.0%) compared to Multi-disciplinary teams (n = 2, 25.0%). These findings were broadly similar for publications overall and for effect size studies.
Descriptive publications (n = 43, 28.3%) were found to be the largest publication types / study designs overall. These were defined as those that provided an account, such as the history of implementation of an e-A&F intervention. Protocol publication types (n = 12, 7.9%) provided detailed methods of a planned future study. Other publication types/study designs were categorised using the MMAT. Qualitative publications (n = 10, 6.6%) utilised qualitative methods (e.g., interviews) to provide an account of an e-A&F intervention while quantitative descriptive publications (n = 15, 9.9%) utilised quantitative methods (e.g., surveys) to provide an assessment of an e-A&F intervention.
Remaining publication types / study designs provided a comparison between interventions/exposures and provided an assessment of the size of the effect. These used random allocation experimental design, Randomised-controlled trials (n = 11, 7.2%), those without random allocation experimental design, Non-randomised study (n = 48, 31.6%), and those with a combination of designs, Mixed methods (n = 13, 8.6%).
Risk of bias was assessed using the MMAT publication type / study design categories for effect size study publications. The majority met the screening questions, ‘S1. Clear research questions’ (n = 48, 76.2%) and ‘S2. Data address research questions’ (n = 48, 76.2%). Those that met the screening questions were appraised using the MMAT, with variation found across specific methodological quality criteria (Figure 2). Risk of bias using the Mixed Methods Assessment Tool for effect size study publications. All effect size studies were screened against the screening questions S1 and S2. Publications that met the screening questions were grouped by type / study design – randomised controlled trials, non-randomised and mixed methods and assessed against five specific methodological quality criteria. Results are displayed as frequency (%) of ratings ‘Yes’ ‘No’ and ‘Can’t Tell’.
Comparison of association between positive and negative outcome effect size studies and evidence of intervention features.
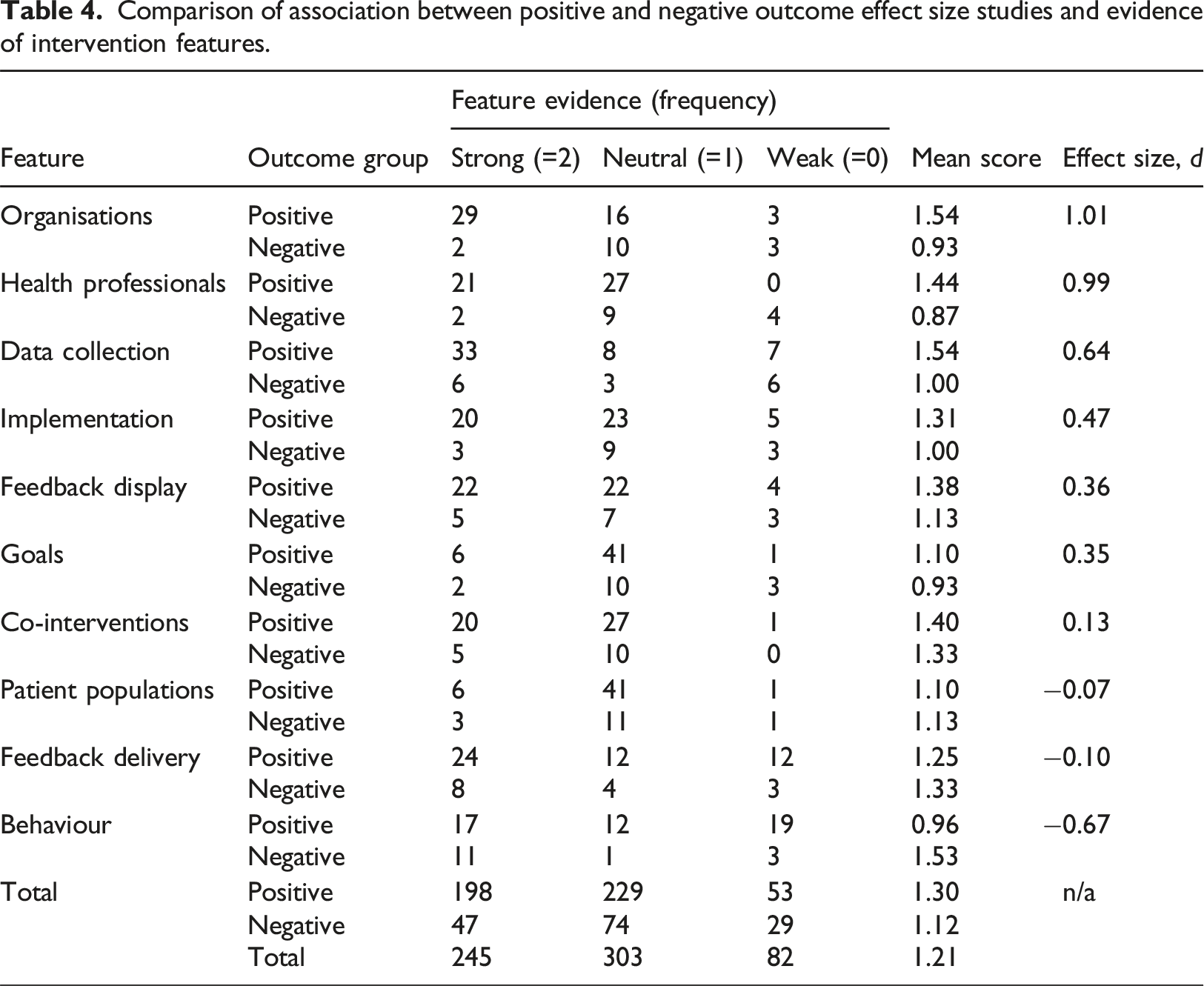
Cohen’s d was found to be above 0.8 (a large effect) for ‘organisations’ and ‘health professionals’. A total of 16 of effect size study publications, or 25.4%, were found to have strong evidence for both ‘organisations’ and ‘health professionals’. Cohen’s d was found to be between 0.5 and 0.8 (a medium effect) for ‘data collection’. ‘Implementation’, ‘feedback display’ and ‘goals’ ranged between 0.35 and 0.47 (a small effect). Three features had effect sizes less than 0.2 (a negligible effect) – ‘co-interventions’, ‘feedback delivery’ and ‘patient population’.
Only the intervention feature ‘behaviour’ was found to be negatively associated with effective e-A&F, Cohen’s d between −0.5 and −0.8 (a medium effect).
Mean differences of assessed features used to generate Cohen’s d were found to vary by year of publication. Year-on-year ‘goals’, ‘health professionals’, ‘organisations’, ‘patient population’, ‘behaviour’, and ‘co-interventions’ increased on average. Out of a maximum possible of 2, these increases ranged from ‘patient population’, 0.01, to ‘co-interventions’, 0.05. Year-on-year ‘data collection’, ‘feedback delivery’ and ‘implementation’ were found to decrease on average. These ranged from ‘implementation’, −0.01, to ‘feedback delivery’, −0.03.
Two pairs of publications were found to be related to the same research study.13,38 A sensitivity analysis was performed by removing one publication from each pair. It was found that the effect sizes of two features changed sufficiently to move them into the adjacent threshold group. These were ‘goals’ and ‘implementation’, which changed from a small to medium effect size (0.35 to 0.55, and 0.47 to 0.61, respectively).
Studies with positive primary outcomes broadly reflected the trends for effect size studies overall (see Table 3). This includes the largest category for each characteristic reflecting the findings for effect size studies generally, including year of publication, 2017 (n = 8, 16.7%), country of origin, USA (n = 40, 70.8%), feedback topic, Infection control (n = 13, 27.1%), target health professional, Multi-disciplinary teams (n = 21, 43.8%), and publication type, Non-randomised studies (n = 39, 81.3%).
Discussion
Principal findings
This review has undertaken a comprehensive search of the literature and by doing so has demonstrated the diversity of publications available on contemporary hospital e-A&F systems. These have been shown to vary across countries of origin, feedback topics, and the target health professional. While broadly consistent with publications overall, there were found to be some key differences when publications included an estimate of effect size, such as feedback topics interventions targeted. Expectedly, we identified differences in the topics of focus amongst specific target health professionals (e.g., doctors disproportionally associated with interventions related to anaesthesia and surgery).
Despite the comprehensive scope used, we found that the breakdown of the characteristics (e.g., feedback topics, target health professionals, publication types) of positive primary outcome studies broadly reflected the breakdown for effect size studies. This supports the generalisability of key results. These being that a common set of features of e-A&F systems (e.g., ‘organisations’, ‘health professionals’) influences effectiveness and ultimately leads to changes to patient care and outcomes.
Two features were found to be most associated with effective interventions. Supportive organisations, such as those who were found have to joined national quality improvement collaboratives, 24 were to be most associated with effective interventions. Targeting health professionals with positive beliefs about feedback and greater capability for quality improvement for the clinical topic in focus, such as those that provided practical skills sessions for quality improvement, 21 were also highly associated with effective interventions. Only one feature was found to be negatively associated with effectiveness. Rather than those targeting system-wide change as predicted by the ‘behaviour’ feature, when an e-A&F intervention targeted individual patient and local level change, such as for anaesthetic drug safety within a single clinical department, 23 it was found to be more likely to be effective.
Far from a stagnant science, the findings also provide insight into strategies for improvement. 39 There was also a surprisingly low level of overlap between interventions which scored strongly amongst the features most associated with effectiveness, ‘organisations’ and ‘health professionals’. This indicates that, at the individual level, there are tangible changes which could be made to many interventions to enhance the likelihood of success.
There also appears to be changes occurring overtime, with mean differences of assessed features found to vary by year of publication. This included that, in general, interventions are increasingly being undertaken to target system-wide rather than individual patient and local level change — defined as the ‘behaviour’ feature. Alarmingly, our findings suggest that those interventions with strong evidence of ‘behaviour’, targeting system-wide change, were associated with being less effective.
Strengths and weaknesses
As anticipated, publications were found to be highly diverse. The expected positive publication bias, reported to be in the order of 3.9:1 – similar to our findings of 3.2:1, was also found. 37 This would have made aggregation in a typical systematic review approach, such as meta-analysis, likely unreliable. 5 Instead, we adapted methodology to compare the features of e-A&F, on the basis of their effectiveness.5,31 While novel, the scoring method for the features of e-A&F was based on a robust theoretical framework. 4 It was, however, limited by the reporting within the papers and therefore could only consider explicit features, potentially omitting more complex and subjective characteristics that were less evidently reported.1,3,4,40
To ensure the statistical power would meaningfully quantify the relative effect sizes of contemporary feedback designs, it was necessary to impose minimal inclusion criteria restrictions. This tradeoff involved the inclusion of some publications with risk of bias. While the majority of effect size publications identified (n = 48, 76.2%) met the screening questions and were appraised using the MMAT, a proportion did not subsequently meet the quality criteria including blinding of assessors, accounting for confounders, and adherence to quality criteria.
Interpretation within the context of the wider literature
Evidently this is an emerging area of study, with an average change increase of 1.1 per year. It would appear that healthcare, like other industries, is increasingly shifting to using electronic means to increase its understanding of practice and outcomes. However, to our knowledge, we are the first to quantitatively review the effect of contemporary hospital e-A&F system. It is also to our knowledge the largest systematic review on e-A&F to-date.
We found evidence in the broader literature that supported trends in the characteristics of publications, such as for the countries of origin. 41 These trends of larger research volumes from specific countries may be the result of favourable local policy environments for health ICT. For example, in the United States the Federal Health Information Technology for Economic Clinical Health (HITECH) Act 2009 provided incentives for the meaningful use of electronic health records in the United States. 42 Similarly, e-A&F in the Netherlands may benefit from access to long standing national electronic data collections. 43
The findings provide support for the proposition that the examined features of e-A&F systems (e.g., ‘organisations’, ‘health professionals’) are driving the difference in effectiveness of interventions found. It also supports the hypothesis that wide variability in the designs exist, and there is a relationship with variability in effectiveness. 1 Therefore, the outcomes have been broadly confirmatory of previous work in this area, while providing nuance of the drivers of effective e-A&F.1,4,44,45
Implications for policy, practice and research
Completing this large and comprehensive systematic review is has been valuable in an environment with increasing interest in digitising healthcare. 41 The findings provide guidance for audit and feedback practitioners in where to focus energy and resources during the setup and implementation of e-A&F. Broadly, the setup and implementation should follow the features of e-A&F examined in this study, in particular the socio-technical features (e.g., ‘organisations’, ‘health professionals’).
There has been a dramatic rise in access to health data and technological advances to support its use, such as business intelligence tools. 6 Against this backdrop there has been much focus on the delivery of feedback to health professionals. However, our findings suggest that new technology, like business intelligence tools, do not on their own ensure effective e-A&F. Our findings suggest the focus of these tools should be on helping to reduce the burden of reporting and analysis (‘data collection’), or supporting timely reporting of current performance (‘feedback display’). 19
The negative association with the feature of ‘behaviour’ is possibly explained by the fact that action taken by recipients to make wider-level changes are resource-prohibitive and that individuals and small teams lack the requisite capacity to engage with them. In our view, this finding does not imply that system-wide e-A&F has no place. There are instances where system-wide e-A&F translates to benefits for features such as ‘data collection’. For example, for large, high-quality standardised data collections, which minimise the burden on health professionals for reporting and analysis, in which case interventions may still be effective. 30
Standardised reporting on e-A&F would help future efforts to confirm the findings of this study. What was often expected to be key background information included in publications was not always reported (e.g., category of health professional being Unknown in 16.5% of publications). To facilitate future comparison, the authors suggest in exploring the adoption of common points for inclusion in e-A&F research publications, analogous to the way SQUIRE 2.0 guidelines are applied to the reporting of quality improvement. 46 In contrast to existing reporting guidelines 47 this could include specific reference to basic intervention characteristics and the 10 intervention features examined.
In addition to an informed model for success, the authors have scoped the existing research on contemporary audit and feedback systems. Those embarking on the setup and implementation of e-A&F have available to them a collection of systems to emulate across a wide variety of contexts (see Appendix 2). Within this collection are also further research opportunities. This includes a total of 28 mixed methods and quantitative descriptive studies, some of which included assessing end-user reported usability. 48 The authors suggest in combination with these existing publications, and the intervention features examined in this review, it may possible to develop a standardised usability assessment tools. This could be used by audit and feedback practitioners to self-assess the likelihood an intervention will be effective.
Conclusion
A large and diverse group of e-A&F interventions were identified, which differed across countries of origin, feedback topics and target health professional recipients. Broadly, we found that published e-A&F interventions were associated with effectiveness where there was explicit evidence that the context and design reflected the features examined. Specifically, we found that interventions benefited from supportive organisations. An association with effectiveness was also found when the health professionals who were targeted had positive beliefs about receiving feedback and greater capability for quality improvement for the clinical topic in focus. Audit and feedback practitioners should focus energy and resources during the setup and implementation to emulate the features as recognised during this review.
Supplemental Material
Supplemental Material - Features and effectiveness of electronic audit and feedback for patient safety and quality of care in hospitals: A systematic review
Supplemental Material for Features and effectiveness of electronic audit and feedback for patient safety and quality of care in hospitals: A systematic review by James Soresi, Christina (Tina) Bertilone, Eileen Banks, Theresa Marshall, Kevin Murray, and David B Preen in Health Informatics Journal
Footnotes
Acknowledgements
No acknowledgments to declare.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Contributorship
JS, DP and KM conceptualised the project, reviewed the literature and drafted the manuscript. CB and EB reviewed the literature and drafted the manuscript. DP, KM and TM reviewed and edited the manuscript. All authors read and approved the final manuscript.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.