
Abstract
The objective of this study is to identify factors influencing unsafe use of hospital information systems in Malaysian government hospitals. Semi-structured interviews with 31 medical doctors in three Malaysian government hospitals implementing total hospital information systems were conducted between March and May 2015. A thematic qualitative analysis was performed on the resultant data to deduce the relevant themes. A total of five themes emerged as the factors influencing unsafe use of a hospital information system: (1) knowledge, (2) system quality, (3) task stressor, (4) organization resources, and (5) teamwork. These qualitative findings highlight that factors influencing unsafe use of a hospital information system originate from multidimensional sociotechnical aspects. Unsafe use of a hospital information system could possibly lead to the incidence of errors and thus raises safety risks to the patients. Hence, multiple interventions (e.g. technology systems and teamwork) are required in shaping high-quality hospital information system use.
Introduction
Most countries in Europe, as well as the United States, are progressively using health information technology (IT) due to the expectation that it can enhance health-care quality. 1 Unfortunately, most developing countries are faced with challenges, especially a lack of robust health IT infrastructure to overcome privacy, confidentiality, and security issues and ensure the continuity of patient health. 1 In Malaysia, the advancement of health information systems (ISs) by means of IT is one of the goals set out in Vision 2020. Telehealth was one of the Flagship Applications launched to provide an accessible, integrated, high-quality, and affordable health-care system, and the Ministry of Health Malaysia (MOH) has embarked on a project to introduce hospital information systems (HISs) into several public hospitals. 2
Despite the proactive implementation of health IT around the globe, recent studies indicate that health IT can result in errors including selection of the wrong patient or administering the wrong drug or the wrong dosage.3–6 These health IT–related errors can lead to patient harm, injury, disability, or even death.4,7,8 Errors can emerge from interactions between people and elements of the technology, tasks, environment, and the organization in which they work.9,10 There is a possibility of errors arising from the complex interaction between clinicians and computers. 11 In a 2015 study, 899 safety events associated with England’s national programme for IT (NPfIT) were analysed. 4 It was revealed that 3% of the safety events were associated with patient harm, including three recorded deaths. It was identified that the safety problems were associated with a technical problem and a human factor. Moreover, Castro et al. 8 identified that over half of the health IT–related events reported to the Joint Commission between January 2010 and June 2013 resulted in patient death, 30% caused unanticipated or additional care, and 11% led to permanent loss of function. It was discovered that the human–computer interface, workflow and communication, and clinical content–related issues are the most common contributing factors. Thus, it is necessary to understand the factors influencing unsafe use of health IT from a sociotechnical perspective.
There is a paucity of studies related to HIS safety in the Malaysian context. The majority of the research found was limited to the earlier stages that are concerned about identification of the risks and hazards. 12 In addition, most of the studies in health IT safety were conducted in western countries and, therefore, may not be sufficient or applicable to address HIS safety in the Malaysian context. Hence, this study intends to identify the factors influencing unsafe use of HIS based on a sociotechnical perspective in Malaysia.
Theoretical framework
This study adapted patient safety model, the Systems Engineering Initiative for Patient Safety (SEIPS) model, 13 and HIS usage model, the DeLone and McLean information system (D&M IS) success model, 14 to guide data collection and data analysis.
SEIPS model
The SEIPS model describes how the design of the work system will have an influence on the safety of the patient.15,16 The components of the work system include person, tasks, technology and tools, environment, and organization as illustrated in Figure 1.15,16 These components interact with and influence the patient-care process and consequently impact outcomes of care.
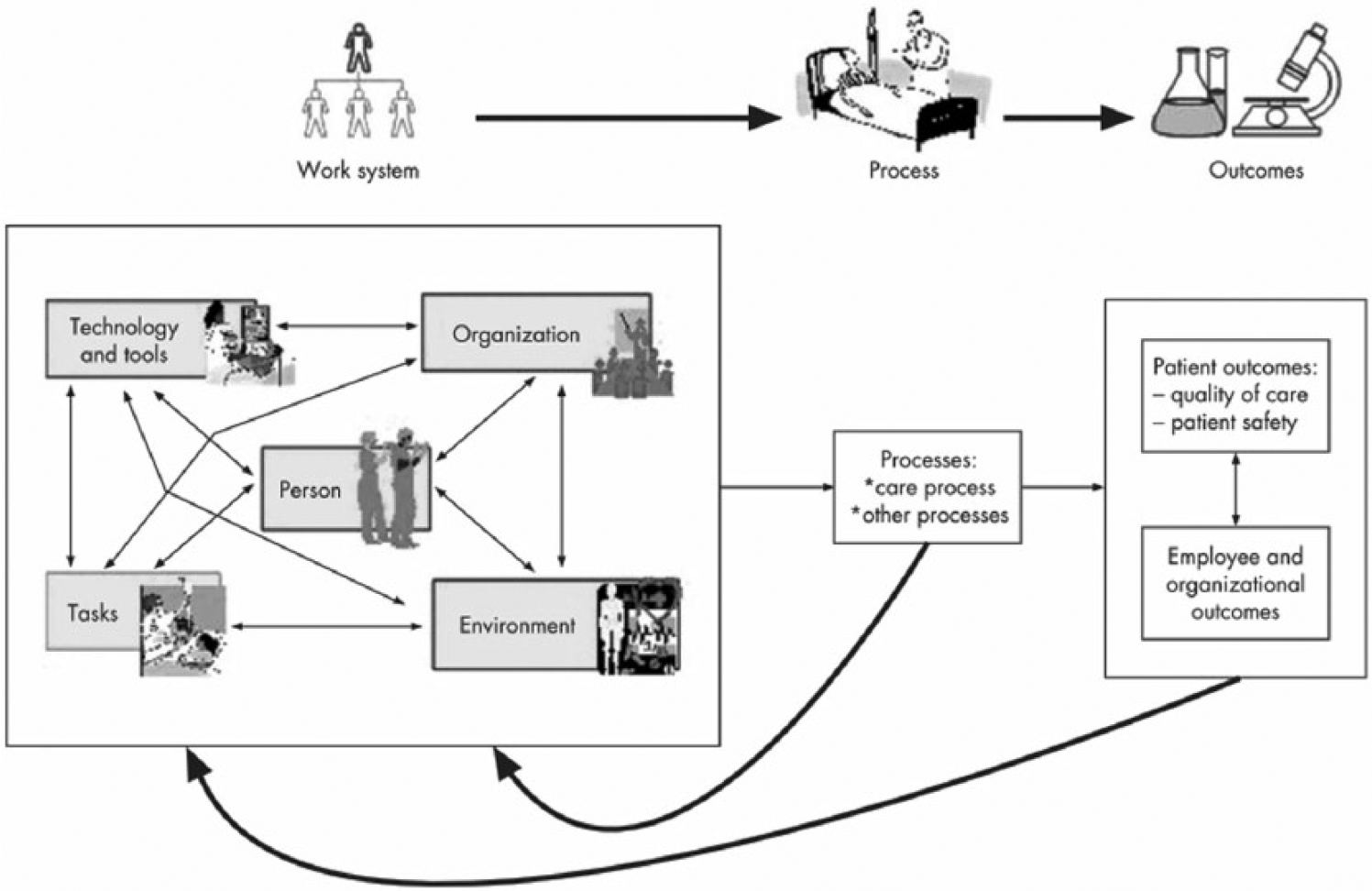
SEIPS model. 13
The SEIPS model can be adopted to analyse or classify the contributing factors of patient safety incidents, and anticipate the possible safety consequences of using the health IT. 10 The model has been used in numerous studies,17–19 concerning patient safety and the impact of health IT on patient safety. Hence, the work system in the SEIPS model is pertinent to this study to identify factors influencing unsafe use of HISs in Malaysian government hospitals.
However, the SEIPS model merely emphasizes the different components of a work system as well as its interactions and possible outcomes, but the specific elements of every single component of the work system are not detailed in the model. 13 For example, the technology and tool component merely lists examples of the technology and tools used in the health-care process. Furthermore, the SEIPS model was not specifically designed for an HIS, and specific elements required for an HIS are lacking in this model. However, the specific elements of an HIS are included in the D&M IS success model. Thus, a D&M IS success model is used to complement the SEIPS model.
D&M IS success model
The D&M IS success model provides a model to evaluate IS success, and due to its comprehensiveness and relative simplicity, extensions of the D&M IS success model are found repeatedly in IS studies conducted from 2003 to 2017. Figure 2 illustrates six interrelated dimensions in the D&M IS success model. These dimensions are (1) system quality, (2) information quality, (3) service quality, (4) use, (5) user satisfaction, and (6) net benefits. It describes how the system’s creation, represented by information quality, system quality, and service quality, influences the users to use the system. The net benefits will be positive or negative depending on the context, the system, and the interaction between the system and its users.
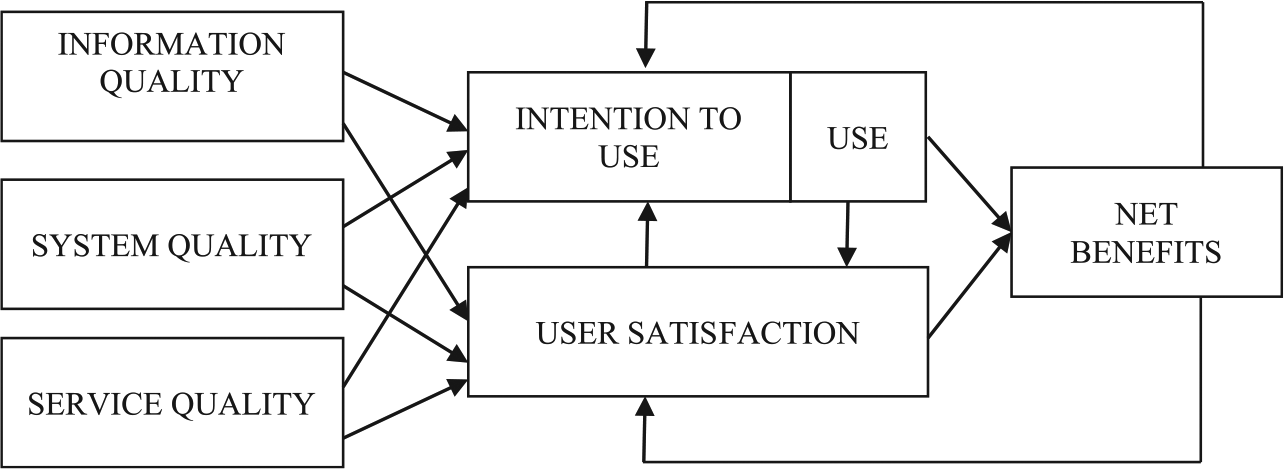
D&M IS success model. 14
The D&M IS success model has been used in various studies20–22 to assess the implementation of health IT. For an instance, an evaluation of an electronic health record (EHR) based on the D&M IS success model discovered that the EHR features such as flexibility and suitability of system functionality were the factors contributing to the positive outcome of the EHR implementation. 20 Conversely, inconvenient and inefficient to use of EHR, for example, poor interface design, mismatches between information flow in the EHR systems and the nursing staff’s workflow, and lack of functions resulted in the unintended adverse consequences. 21 Therefore, the D&M IS success model is relevant for system evaluation in the health-care domain. Only three components of the D&M IS success model, system quality, information quality, and service quality, are adopted in this study as they signify the technology component. The other D&M IS success model components, intention to use or the use of the systems, user satisfaction, and net benefit, were excluded from this study because they do not represent the technology attribute.
Methods
This study employed qualitative research methods to achieve the objective of the study. The following sections describe the research methods used in this study.
Setting and sample
A total of three Malaysian government hospitals implementing total hospital information systems (THISs) were selected for this study. A THIS is an HIS that integrates various hospital subsystems such as a laboratory information system (LIS), a pharmacy information system (PIS), a radiology information system (RIS), and a picture archiving communication system (PACS). A THIS is designed for a large hospital with more than 400 beds. Currently, THISs are only implemented in selected tertiary hospitals that are located mostly in the Klang Valley and in the northern and southern states of Malaysia.
The three selected hospitals are referred to as Hospitals A, B, and C. Hospital A has 562 beds, while Hospitals B and C have 620 beds. Hospital A is a national reference centre for haematology patients. Hospital B is a reference centre for cardiology, cardiothoracic, urology, and nephrology surgery. Hospital C is an excellent centre for infection diseases, neurosurgery, maxillofacial surgery, and plastic surgery, as well as for orthopaedic and trauma patients. The latter hospital implemented a complete THIS in February 2008, which is 2 months after Hospitals A and B. Therefore, all three hospitals are of similar size and have similar working environments and similar experience of a THIS implementation. Table 1 summarizes the criteria for the three Malaysian government hospitals selected for this study.
Criteria of selected hospitals.
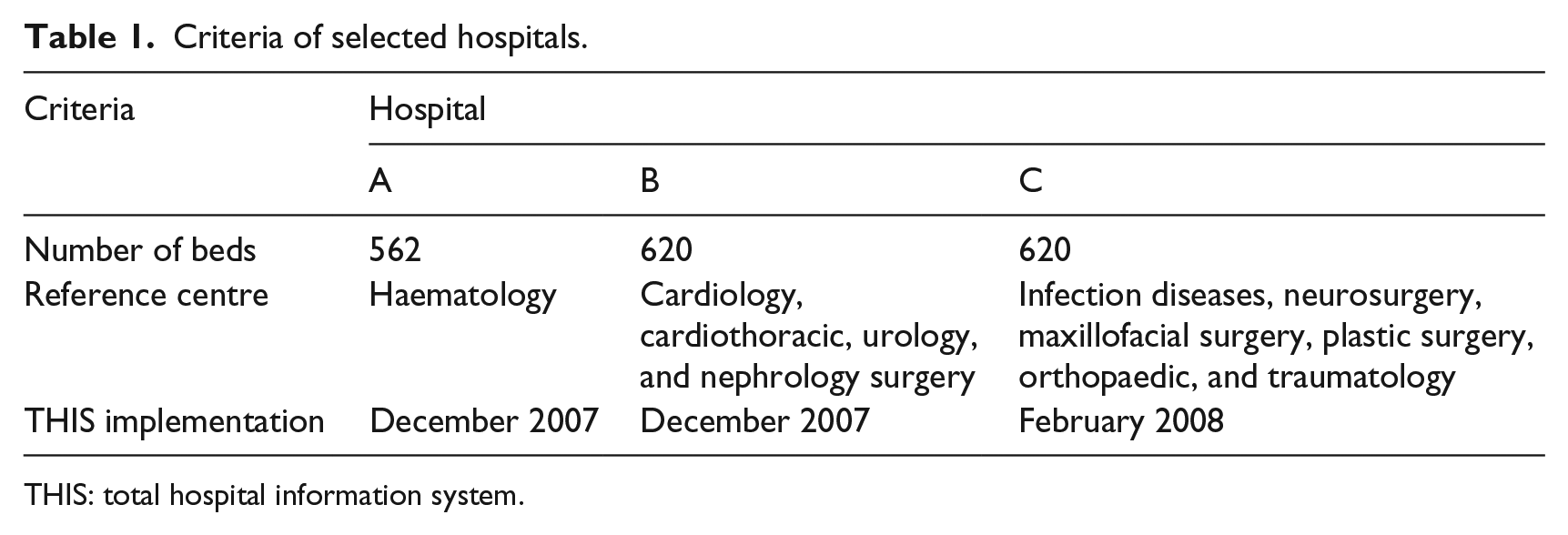
THIS: total hospital information system.
This study focused on doctors working in the selected hospitals who are also THIS users. Considering their important role in patient-care delivery and their routine use of the THIS, they can be considered an important in regard to the adoption of THIS use. Overall, the target population of this research includes all doctors in the selected hospitals, of which there were 770 in December 2014 according to statistics obtained from the human resource department of each hospital. Purposeful sampling was adopted for qualitative data collection because the aim was to provide rich information in context. The criterion for a sample selection was a minimum 1 year experience in using the THIS. In total, 31 medical doctors participated in the actual interview. There were 10, 9, and 12 participants from Hospitals A, B, and C, respectively. There were slightly more female participants than male, accounting for about 58 per cent. The participants were from various departments including emergency and trauma, medical, general surgery, paediatric, obstetrics and gynaecology, orthopaedic, otorhinolaryngology, ophthalmology, cardiology, nephrology, neurosurgery and neurology, haematology, psychiatric, and rehabilitation. Their experience in using the THIS is between 1.5 and 10 years. Hence, it was determined that the participants have sufficient experience to elucidate their views on the THIS implementation.
Data collection
The interview session involved doctors who have directly used the THIS. A semi-structured interview guide was designed to manage the discussion with the medical doctors (Appendix 1). The research model described in section ‘Theoretical framework’ and the findings from a systematic literature review conducted in the previous study 23 were used to guide and structure the qualitative data collection and data analysis. The interview questions contained neutral and open-ended questions to avoid eliciting socially desirable responses. New questions were permitted to arise as a result of the discussion. The interview study was conducted according to procedural steps as suggested by Hesse-Biber and Leavy. 24 Subsequent to the ethics approval from Malaysia’s Ministry of Health Medical Review and Ethics Committee (MREC), all the potential participants were contacted to request their agreement to participate in the interview, and they were given a brief explanation about the study and the interview. Once they agreed to participate, an interview appointment was scheduled as convenient for the participants. A follow-up reminder via phone was done a day before each scheduled session to remind participants of the session as well to confirm their attendance.
The semi-structured interviews were conducted between 23 March and 18 May 2015. Interviews were conducted by one researcher. Face-to-face interview sessions were conducted at the participant’s work place. A mix of both English and Bahasa Malaysian language was used in the interview. Permission to tape-record the discussion was requested prior to the interview. Each interview lasted between 15 and 90 min with a total duration of approximately 14 hours. A small gift was given to each participant as a token of appreciation for their participation.
Data analysis
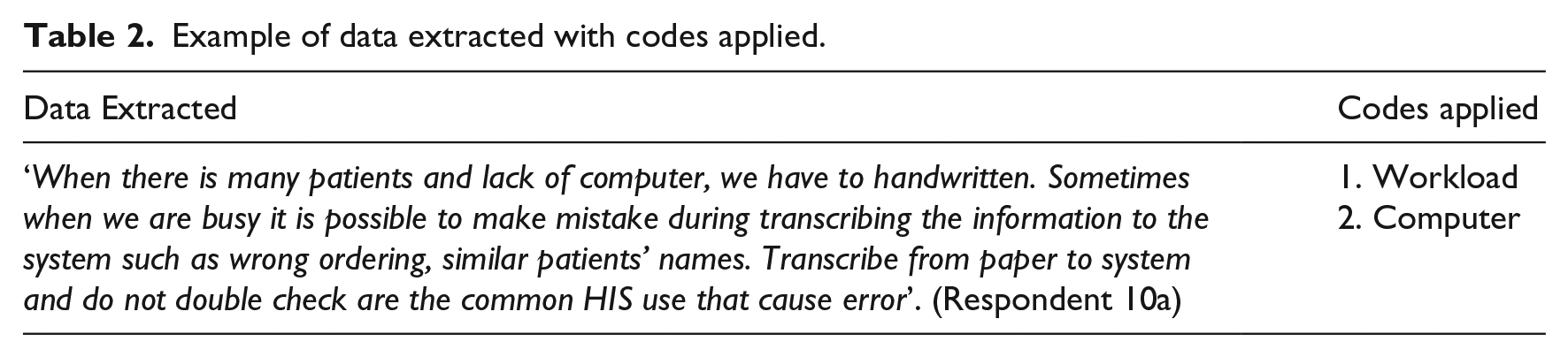
The analysis comprised four phases: transcribing, organizing, coding, and theme building. 25 First, recorded audio data and handwritten notes from the interviews were transcribed to word processor text. Transcripts of interviews were then presented to the respondents for validation purposes to ensure the interviewer had captured the respondents’ intended meaning. Then, the interview transcripts were organized into sections for easy retrieval in the organizing phase. Subsequently, the transcribed interviews were coded using the qualitative data analysis software, ATLAS.ti. In the coding phase, the transcripts were read repeatedly to highlight parts of the text and to emphasize the sections and issues that seemed to be important and relevant. Deductive coding was used to start the analysis. The SEIPS model and D&M IS success model, as well as safe use of HIS antecedents identified in the previous study, 26 were used as a guideline to code the data. However, as the analysis proceeded, additional codes were created when new factors were identified. All collected data relevant to safe use of HIS antecedents were extracted and mapped to the developed codes. The interview transcripts were divided into text segments, and these segments were labelled with the codes. Table 2 presents an example of codes applied to a short segment of data.
Example of data extracted with codes applied.
The coded data were reviewed to identify areas of similarity and overlap between codes. In this step, any overlapping and redundant codes were eliminated. Finally, similar codes were grouped together as a theme or category to form a major idea in the theme building phase. Codes that seemed to share some unifying feature were clustered into a theme. 27 The relationships between codes, between themes, and between different levels of themes were explored. Thematic maps were used as visual representations to help in sorting the different codes into themes. Figure 3 shows the thematic map for unsafe use of HIS antecedents that shows the relationship between themes (shown as circles) and codes (shown as rectangles) deduced from the thematic analysis. Subsequently, all the themes were reviewed and discussed among the team member to confirm that the themes meaningfully capture the important and relevant elements of the coded extracts and the entire data set. Any difference in interpreting the findings was resolved by discussions until consensus was reached. Themes that were deemed not relevant were discarded.
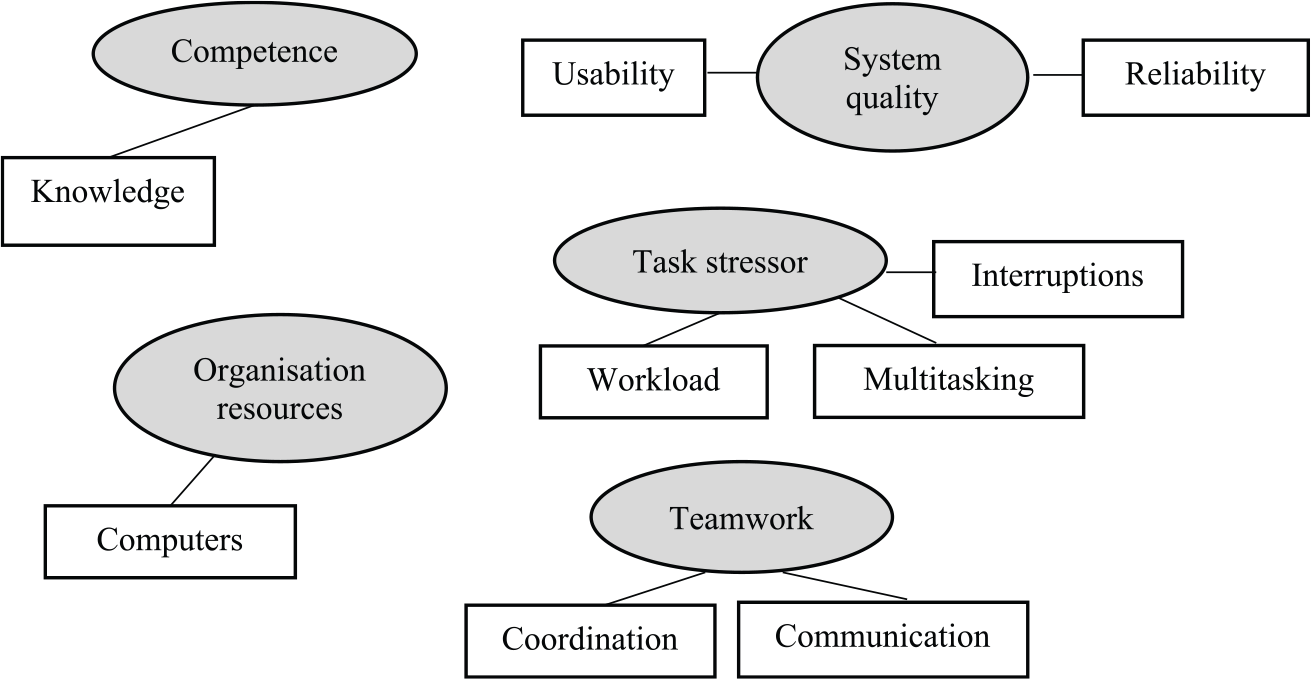
Thematic map of unsafe use of HIS antecedents.
Results
A total of five themes emerged as the factors influencing unsafe use of HIS which consist of (1) knowledge, (2) system quality, (3) task stressor, (4) organization resources, and (5) teamwork. The findings are consistent with our previous systematic literature review findings deliberated in Salahuddin and Ismail. 26 Representative quotes organized by themes are presented in Table 3. Only the selected quotes that appropriately represent the themes were presented in this table.
Representative quotes.
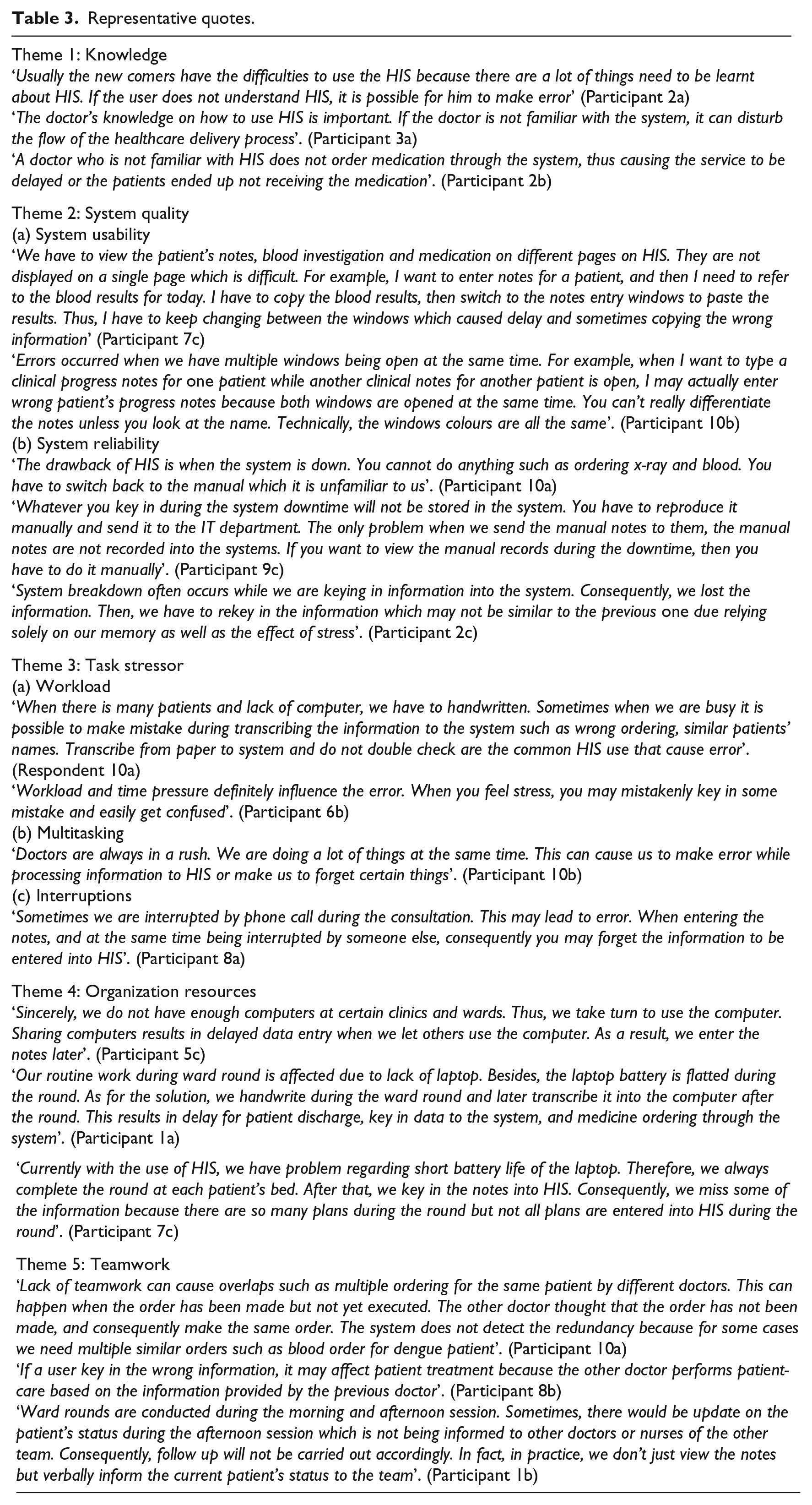
Knowledge
The interviews revealed that users who are not familiar with the HIS can make errors. New staff are prone to making errors, owing to their lack of experience and knowledge on the HIS. In addition, participants stated that lack of HIS knowledge could affect the flow of the health-care delivery process. It is essential for users to know the step-by-step process of how to use the HIS and its limitations to enable them to complete their tasks appropriately. Users with inadequate HIS knowledge would not be able to fully utilize the HIS. Thus, certain procedures may not be performed completely, resulting in delays in patient care and posing risk to patients.
System quality
From the interviews, it was found that system usability and system reliability were the factors related to system quality influencing unsafe use of the HIS. It was discovered that the concern about system usability relates to the user interface design. Participants indicated that the graphical user interface (GUI) of the THIS displays different information such as patient notes, blood investigation, and medication on different windows. Nevertheless, the system will allow users to open only a limited number of windows concurrently. As a result, users have to memorize, write down, or copy and paste the necessary information before switching to another window. This tedious procedure is prone to result in delay and mistakes. In addition, the THIS design permits users to simultaneously open multiple patients’ notes, and participants remarked that opening notes for multiple patients could lead to viewing or updating the wrong patient’s notes. In a similar vein, a participant pointed out that the THIS design does not offer a function to distinguish different patients’ notes. Instead, users need to be aware that they were switching between the notes of different patients by looking carefully at the patient’s name on each window.
A majority of the participants claimed that system being down or hanging is one of the major problems pertaining to system reliability. Their patient-care tasks are completely reliant on the HIS since all the information related to patient care is stored in the system and doctors directly key in information into the HIS. It was noted that paper-based documents were not prepared as a backup and that the hospitals did not have a backup system to be operated when the HIS was down. During HIS unavailability, doctors would manually record new information related to patient care. Nevertheless, the IT department of each hospital performed system backups regularly to back up the files and data of the HIS.
It was noted that system downtime could obstruct the doctors’ work such as ordering x-rays, blood tests, and medication. Participants claimed that they were not able to view in the system the notes of patients who were admitted while the system was down because the manual notes made by the doctors were not entered into the system after access to the system was restored. The manual notes were not transcribed to the system as the doctors were not obliged to transcribe them because no relevant policy existed. Thus, any such notes needed to be accessed manually. Additionally, system downtime could result in lost data as the system had no auto save function to automatically record the information being entered by the doctors. Therefore, users had to retype the information that was not saved during the system down. To do this, they would need to rely on their memory because they did not write down manual notes as backup if they actually entered it into the system. Hence, the information being entered for the second time may not be the same, or as complete, as the information first entered. This need to re-enter information could also affect users by increasing their frustration and stress.
Task stressor
The interview findings show that high workload, multitasking, and interruptions, which are associated with the task stressor, can influence the unsafe use of the HIS. It was found that workload is increased when there are too many patients at the clinic or in the ward. As a result, doctors are likely to make mistakes. High workload subsequently results in stress, lowered concentration, and limited time to complete tasks. All these factors may lead the doctors to make mistakes while using the HIS. Common errors include keying in the wrong information, updating the wrong patient’s record, and ordering medication for the wrong patient. In addition, participants remarked that data entry is delayed when there are many patients as they do not have ample time to immediately enter the patients’ notes. As a result, they may miss some information or another doctor might receive the plan late. Patient-care tasks require doctors to multitask, and focusing attention is crucial while multitasking. Thus, multitasking can possibly cause doctors to unintentionally make errors while operating the HIS. Moreover, the interview findings revealed that interruptions can disrupt the doctor’s concentration while entering notes into the HIS. Consequently, the doctor may forget to perform certain tasks or tend to make errors.
Organization resources
The participants commented that there are limited computers to support their routine work; hence, they have to share computers with other staff. Sometimes, they have to compete to use the computers. This could result in delays in data entry, and therefore, tasks cannot be done on time. Consequently, they have to write down their notes while waiting for their turn to use the computer.
The participants noted that laptops were being carried from bed to bed during ward rounds in the early implementation of the HIS. Hence, patient notes could be viewed on the HIS at patient’s bed, and patient-care plans could be entered immediately. However, the participants commented that most of the laptops were more than 3 years old, and therefore, the laptop batteries no longer lasted very long. As a result, the laptops often had flat batteries and needed to be constantly plugged into the power source. Hence, this causes a change in the process for the doctors to enter or update their patient-care plan, whereby the plan would be written down on paper during the ward round and later entered into the HIS after the round. This would result in a delay in the patient-care delivery such as the discharge of the patient, data entry into the system, and medicine ordering. Moreover, entering data for most patients at the end of the ward round may lead the doctors to miss entering some of the information.
Teamwork
The interview findings revealed that lack of teamwork could cause the doctor to duplicate orders because he or she is not aware that the same order has already been made by his or her colleague. It was also discovered that any mistake or error made by a teammate could easily be propagated to other members. The doctors usually refer to the information provided by other teams in order to perform patient care. Therefore, doctors may make mistakes as a result of following erroneous information. Furthermore, a lack of communication or a miscommunication may result in a task not being carried out which could cause more problems. For instance, follow-up might not be done if other team members, for example, doctors or nurses working the next shift, are not informed of the patient’s status. There were also cases when the team overlooked changes on the patient-care plan because they were not aware of the changes made due to a doctor forgetting to notify them verbally of the changes.
Discussion
This study identified five themes describing the sociotechnical factors influencing unsafe use of an HIS. These themes are knowledge, system quality, task stressor, organization resources, and teamwork. The findings were found to be generally consistent with previous health IT safety studies conducted around the world. The consistency of the findings may be due to the similar nature of the health-care environment that involves complex activities, high degree of uncertainty, frequent interruptions, heavy workload, and interactions with and inter-reliance on various other health-care professionals. However, the key issues appeared to be more focused in Malaysian government hospitals implementing a THIS.
The interview findings indicate that insufficient knowledge about the HIS resulted in the doctors not completing certain procedure in the HIS. They were also more susceptible to making mistakes. This finding is consistent with a previous study that reported that poor knowledge of the prescription ordering mechanism resulted in prescription errors. 28 The finding of this study suggests that knowledge of the HIS is a perquisite for each doctor to enable them to utilize the HIS appropriately. They can become equipped with this knowledge via formal training, knowledge sharing among colleagues, and variety of communication mediums such as notices, posters, and newsletters.
Our interview findings also indicate that system quality is the technology component that can have an influence on the unsafe use of an HIS. System quality is linked to the system usability and the system reliability. Poor system usability such as complicated design and multiple windows leads to the HIS is not being used as intended and may require the user to memorize, write down, or copy and paste the necessary information. Moreover, the HIS design allows users to concurrently open multiple patients’ notes. As a result, doctors are prone to making mistakes by viewing or updating notes for the wrong patient. In accord with our findings, previous studies indicated that poor usability is one of the crucial barriers for optimal quality and safe use of health IT systems.3,29 This finding indicates that the HIS should be designed to be user-friendly and uncomplicated in line with the nature of patient care in hospital that is hectic, has repeated distractions and interruptions, and requires multitasking. The design should not be confusing and require additional cognitive effort to avoid errors from happening. Indeed, improving the usability of EHR systems is recommended by the American Medical Informatics Association (AMIA) to enhance patient safety and quality of care. 30
Furthermore, health-care organizations need to be well prepared to face system downtime. System backup and auto save function should be made available to avoid from discontinuity of accessing HIS and loosing data.
It was discovered that high workload, multitasking, and interruptions are associated with the task stressor, and all have potential for resulting in errors. High workload leads to stress, lower concentration, and limited time to perform tasks. Multitasking requires the user’s focused attention and results in a high level of cognitive load. Memory lapses easily arise when doctors need to juggle multiple tasks. 6 Reliance on memory could lead doctors to inadvertently make errors when using the HIS because humans are only capable of remembering a limited amount of information in their working memory at one specific time. Interruptions can disrupt the user’s concentration while keying notes into the HIS, thus limiting their capability to meet the required vigilance when processing HIS. The task stressor resulted in the doctors being more likely to make mistakes, forget to perform certain tasks, or miss some information. The result is congruent with a study that reported that interruptions in addition to adding to the time pressure resulted in health-care practitioners inadvertently ordering medication for the wrong patient. 31 Another study reported that 81% of wrong-patient electronic orders were due to frequent interruptions and the ease of switching between patient screens in computerized health-care systems. 32
A focus on organization resources in this study found a shortage of computers and laptops with a short battery life. Due to an inadequate number of computers, doctors have to share computers with other staff to access the HIS, resulting in data entry delay and tasks not being done on time. In addition, laptops need to be constantly plugged into the power source due to short battery life. Hence, doctors have to go back and forth from the laptop to the patient bed to access information on the HIS. This also means that patient notes and patient-care plan must be written down on paper during the ward round and then transcribed into the HIS at the end of ward round which may lead the doctors to forget to enter some of the information. Similarly, previous studies reported that a lack of portable computers hindered health-care practitioners from issuing electronic orders during the ward round and, therefore, holding up the order entry process until they returned to the workstation.21,33–35 This finding points out that sufficient computers as well as well-functioning computers are key factors that influence the way the HIS is utilized. Doctors devised a workaround to deal with these resource deficiencies, which potentially endangers patient safety by failing to enter information or delaying the data entry process which could delay important orders for medications or tests. Hence, health-care organizations should ensure they provide sufficient computers and perform regular computer maintenance to allow for safe use of the HIS.
Teamwork is important to ensure safe patient care. The interview findings show that lack of teamwork could cause duplicated tasks such as performing multiple of the same order in the HIS. Doctors usually refer to the information provided by other teams to perform patient care. Hence, any mistake made by a teammate could simply be propagated to other members. Furthermore, lack of communication or miscommunication may result in a patient-care plan not being carried out. Doctors may verbally interact less frequently with team members about patient issues or patient-care plans as interactions among team members have become more electronic in nature rather than verbal. Reduction in communication among team members can possibly result in misunderstanding and poor coordination of patient care. Similarly, previous studies reported that communication shortage increased the possibility of errors and safety incidents due to miscommunication, delayed in initiating and executing orders, and fewer team discussions on planning and coordination of care.36,37 Realizing the importance of teamwork for the safe use of the HIS, hence, there must be some consideration of approaches to build up the team spirit and morale as well as to inspire cooperation and communication among the team members.
Conclusion
This study identified the main factors influencing unsafe use of an HIS. Conceptual models from patient safety and HIS usage were used to facilitate the data collection and analysis processes. The findings of this study suggest that both technological and social aspects affect the safe use of an HIS. The results showed that insufficient knowledge of the HIS could result in errors, delays in the flow of health-care delivery process, and pose risks to patients. Furthermore, the presence of task stressors such as high workload, multitasking, and repeated interruptions has a significant impact on the doctors’ concentration and emotional well-being. Task stressor could possibly result in doctors making errors while using the HIS such as keying in wrong information, updating the wrong patient’s record, or ordering medication for the wrong patient. This study also indicated that organization resources have a significant impact on the way the HIS is utilized in hospitals. Doctors adapting informal work processes or workarounds to overcome resource deficiencies or cope with difficulties in their workflow can burden themselves with extra time and effort or endanger patient safety. For instance, when patient-care plan is written down on paper during the ward round and then transcribed into the HIS after the round. Lack of teamwork is another factor revealed in this study that could possibly lead to errors and endanger patient safety. System quality is an important technological aspect affecting the safe use of HIS. This study demonstrated that poor system usability resulted in the HIS not being used as intended as well as workarounds in the HIS such as to memorize, write down, or copy and paste the necessary information from one screen to another in the HIS. Moreover, poor system reliability could obstruct patient-care service and result in a loss of data. To conclude, it is highly suggested that hospitals nation-wide and HIS developers take into consideration both the technological and social aspects of the health-care system when developing and implementing an HIS in order to realize the full benefits of the HIS. The findings from this qualitative study can facilitate hospital management in designing HIS implementation strategies to establish safe HIS adoption by taking into consideration the sociotechnical aspects.
Footnotes
Appendix 1
Acknowledgements
The authors would like to thank the 31 medical doctors who gave their time to participate in the interviews and the officers of the clinical research centres for their assistance in conducting the interviews.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Universiti Teknologi Malaysia (UTM) research grant Q.130000.2538.11H82, Universiti Teknikal Malaysia Melaka (UTeM) and Ministry of Higher Education (MOHE) Malaysia.