
Abstract
The aim of this study was to explore the effects of web-based education in the field of drug utilization on elderly individuals’ knowledge of, concerns about and self-assessed understanding of drug utilization. The 260 included participants were randomized to a control group or an intervention group. To assess drug utilization literacy, we used a questionnaire containing 20 multiple-choice questions on drug utilization and ten statements about drug utilization (to which participants graded their response using a Likert scale: two about common concerns and eight about their self-assessed understanding of drug utilization). The Beliefs about Medicines Questionnaire-General was also used. The intervention group scored higher on the knowledge questions (p < 0.001) and on six of the eight statements about self-assessed understanding of drug utilization at the first check after 2 weeks (p < 0.05). At a second check 6 months later, the difference remained for the knowledge questions, but there was no difference in self-assessed understanding of drug utilization between the groups. There were no differences in the concerns about drug utilization or beliefs about medication at any time. We conclude that a web-based education can improve drug utilization literacy in elderly individuals and might contribute to the safer use of medications.
Introduction
Among the elderly, improved knowledge about their medications is one of several factors that can contribute to the safe use of these medications. 1 Patients with insufficient knowledge might not be able to manage their medications as intended. This increases the risk of inappropriate medication use, for example, erroneous practical handling of medications 2 or suboptimal adherence, 3 and limits the ability of patients to make informed decisions about their medication. 4 The consequences of inappropriate medication use include reduced therapeutic effectiveness, increased occurrence of adverse effects and increased drug-related hospitalizations. 5 Besides affecting the individual, inappropriate medication use also contributes to the economic burden of society 6 in terms of medication wastage and increased use of medical resources.7,8
The concept of medication literacy refers to the ability of the patient to obtain, comprehend and process specific information about their medications in order to use them safely and effectively, 9 that is, the concept mainly relates to each individual’s own prescribed medications. In this paper, we use “drug utilization literacy” to describe the ability of patients to manage their medication process, that is to understand the pharmacy services, where to find answers to questions and how to find information about their medications. It is particularly important to improve the drug utilization literacy of the elderly and other patients exposed to polypharmacy since they have a high risk of drug-related problems, 10 and usually have a poor understanding of drug indications and side effects. 1 In addition, elderly patients exposed to polypharmacy have expressed a desire to learn more and to question the doctor’s actions, 1 requesting more easily accessible information. 11 The elderly often have unanswered questions, not only about specific medications but also about the health-care system, the pharmaceutical companies, and the reasons for generic drug substitutions. 11 Educating 12 and involving patients in their own health care and treatment decisions 5 could increase patient safety and satisfaction. 12 Educational interventions for the elderly regarding specific medications can improve their knowledge about their medications, recognition and management of the medications as well as improving adherence to the dosage regimen.13,14,15,16 However, research in the broader context of drug utilization is scarce.
When educating patients, both oral and written information are important but, as oral information may be forgotten, it is an advantage if patients have the opportunity to access information when it is needed, either on paper or digitally. 5 Studies on the effect of written information for patients about medications show mixed results regarding their positive impact on knowledge. 17 A review of multimedia patient education interventions about medications suggests that the effects of multimedia education is at least equivalent to other forms of education, including written education and education provided by a health professional. 18 There are potential advantages of multimedia education programs over traditional forms of information delivery but more studies evaluating multimedia educational interventions are required. 18
In a pilot study, web-based education modules about drug utilization appeared to be useful for distributing information to the elderly; the participants found the education process a positive experience in the main. 19 However, that pilot study did not investigate the actual effects of web-based education on knowledge of and concerns about drug utilization. The aim of this study was to investigate the effects of a web-based education module on drug utilization literacy among the elderly. More specifically, the objectives were to investigate the effects of web-based education on elderly individuals’ knowledge of, concerns about, and self-assessed understanding of drug utilization, as well as on their general beliefs about medicines, using the Beliefs about Medicines Questionnaire (BMQ)-General.
Method
Study design
This was a single-blind, randomized, controlled study with two parallel arms of equal size, conducted in elderly people in the county of Småland, Sweden, during 2016. The regional ethical board in Linköping, Sweden, approved the study (2014/472-31). Participants were recruited from pensioner and patient associations. The local divisions of the two main pensioner associations and patient associations with a high probability of including elderly members (according to diagnosis) were contacted by the research group. The following patient associations were excluded: associations for children, young individuals or parents, for visibly impaired, for those with hearing problems, cancer, mental illness or a disease not usually treated with drugs. In total, 30 local associations, 20 for pensioners and 10 for patients, allowed the researchers to approach their members. The members of those pensioner and patient associations were informed about the study at one of their meetings and potential participants were provided with written and oral information. The individuals who agreed to participate signed an informed consent document. The recruitment of participants lasted from April 2015 to January 2016. Inclusion criteria were: age ⩾65 years and being able to speak and understand Swedish.
Web-based education modules
The web-based education course comprised ten modules; the first (1) provided an introduction to the topic; the next eight provided information on (2) over-the-counter medication and food supplements, (3) generic drug substitution, (4) medication lists, (5) the Pharmacy Benefit Scheme, (6) devices to help with the administration of drugs, (7) adverse drug reactions, (8) drug interactions, and (9) the effects of and how to utilize medications; and the last (10) gave a list of frequently asked questions. Each module consisted of slideshows with pictures, text and sound and was arranged as a short online lecture. It took approximately 1 hour in total to complete all the modules. It was possible to access the educational website from any location, provided a computer with an internet connection was available. The modules had been initially used in the former pilot study, which showed that they were suitable for the study population. This procedure has been described in more detail by Throfast et al. 19
Randomization
The participants were randomized 20 1:1 to the intervention group (IG) or the control group (CG) in blocks of ten individuals (five patients receiving the intervention; five controls) using the opaque sealed envelope technique where the participants are given randomly generated allocations within sealed envelopes. 20 The purpose of this randomization design was to obtain equally sized study groups despite the sequential and relatively extended period of inclusion. In all, 260 individuals agreed to participate in the study. After randomization, an information letter was distributed to the participants. The letter to the participants in the IG included the link and a password for access to the web-based education modules together with instructions and study information. The participants in the CG received a similar letter but without the link and password. The participants in the IG had access to the modules during the whole study and were instructed to familiarize themselves with the web site and pursue the education at their own pace, in a place that suited them, and to repeat the modules if needed.
Questionnaire for outcome evaluation
The questionnaire comprised three parts in addition to background data. The first two parts evaluated drug utilization literacy, concerns about drug utilization, and self-assessed understanding of drug utilization. Part one consisted of the knowledge test; 20 general, multiple-choice questions on drug utilization (the primary outcome measure of the study). The knowledge test was designed so that the multiple-choice questions covered the content from all modules, where the answers to all questions could be found. The multiple-choice questions had two or three alternative answers, only one of which was correct. Each question had a “do not know” alternative and included the possibility of adding a comment in free text. There was also a separate field at the end for the participant’s comments about the multiple-choice questions in a free-text format. The answers to the multiple-choice questions were scored by the researchers; the maximum score was 20. Questions with a wrong answer, with a “do not know” answer, or with missing data (no answer filled in) were given a score of zero.
Part two of the questionnaire consisted of ten statements in total, two regarding concerns about medicines (Table 3, statements 3 and 10) and eight regarding self-assessed understanding of drug utilization (Table 3, statements 1-2 and 4-9). The statements were constructed by the researchers. The respondents scored their degree of agreement with the statements on a 6-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree). All statements were analyzed separately.
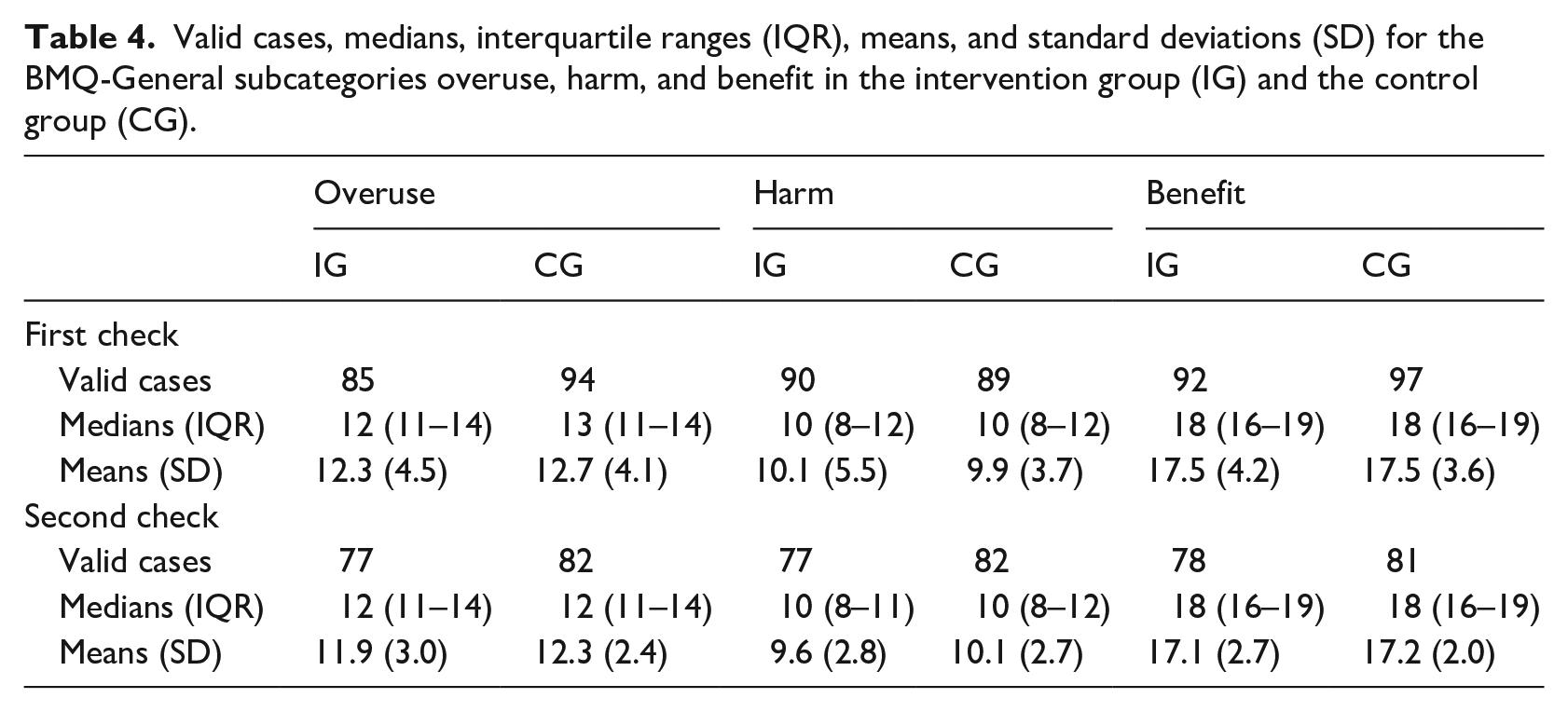
Part three of the questionnaire consisted of the 12-item version of the BMQ-General. 21 The BMQ-General was scored on a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The statements measured three aspects of medication use: General-Overuse covered beliefs about whether medications are overused, General-Harm covered beliefs about the harmful effects of medications, and General-Benefit covered beliefs about the benefits of medications. 22 The BMQ-General subscales were scored from 4 to 20. The summed scores were computed for each patient, along with the mean score, the standard deviation (SD), the median score and the interquartile range (IQR) for each subscale. Higher scores indicated greater agreement with the construct represented by the scale. 21 If one or more answers were missing, the total score of the corresponding BMQ subscales was excluded for that respondent.
Five individuals from the research group evaluated the content validity of the questionnaire in terms of accuracy and relevance. To further ensure the validity regarding the knowledge questions and the concerns about and self-assessed understanding of drug utilization, these parts were piloted in a small test group comprising ten individuals aged ⩾65 years.
The questionnaire was sent with the information letter described above to both the IG and the CG. The participants were asked to complete it no later than 14 days after the start of the intervention (first check). The questionnaire was redistributed by mail with a reminder letter to individuals who failed to answer within a 3-week period. The first check included the first responses to the questionnaire as well as demographic data. There were no baseline measurements before the educational intervention. The researchers were blinded to the originators of the answers in the returned questionnaires. All participants received the questionnaire a second time, 6 months after the education initiation (second check). After completing the study, the participants in the CG also received the password to the educational modules.
Statistical analysis
The effect size (d) was set to 0.4, resulting in a sample size of 98 individuals in each group, with a power of 80%. 23 The effect size was utilized to ensure the reliability of the study. To account for 35% dropouts, we needed to include 260 participants. As a certain number of participants were included in the study at the same time (for each association), inclusion was stopped when we had exceeded 263 participants. Group comparisons of the baseline characteristics were conducted using two-tailed independent t-tests or the Chi2 test. Analysis of the primary outcome measure at the first and second checks was performed by Welch’s t-test when variances were unequal for IG and CG, or by the two-tailed independent t-test when variances were equal. Within-group comparisons of knowledge test scores based on educational level were conducted using one-way ANOVA and Tukey’s post hoc test. Since the statements outlining concerns about and self-assessed understanding of drug utilization and the BMQ-General were analyzed as ordinal data, the Mann–Whitney U test was used to compare group differences for the first and second checks. The statistical significance for all analyses was set at p < 0.05 (two-sided) with a power of 80%. SPSS Version 25.0.0.1 for Windows (SPSS Inc. Chicago, IL, USA) and GraphPad Prism version 7.05 for Windows (GraphPad Software, La Jolla, CA, USA) were used for all analyses.
Results
A total of 260 participants were consecutively recruited and randomized. At the first check, 195 individuals (75%) responded to the questionnaire (Figure 1) and at the second check, 163 individuals (63%) responded.
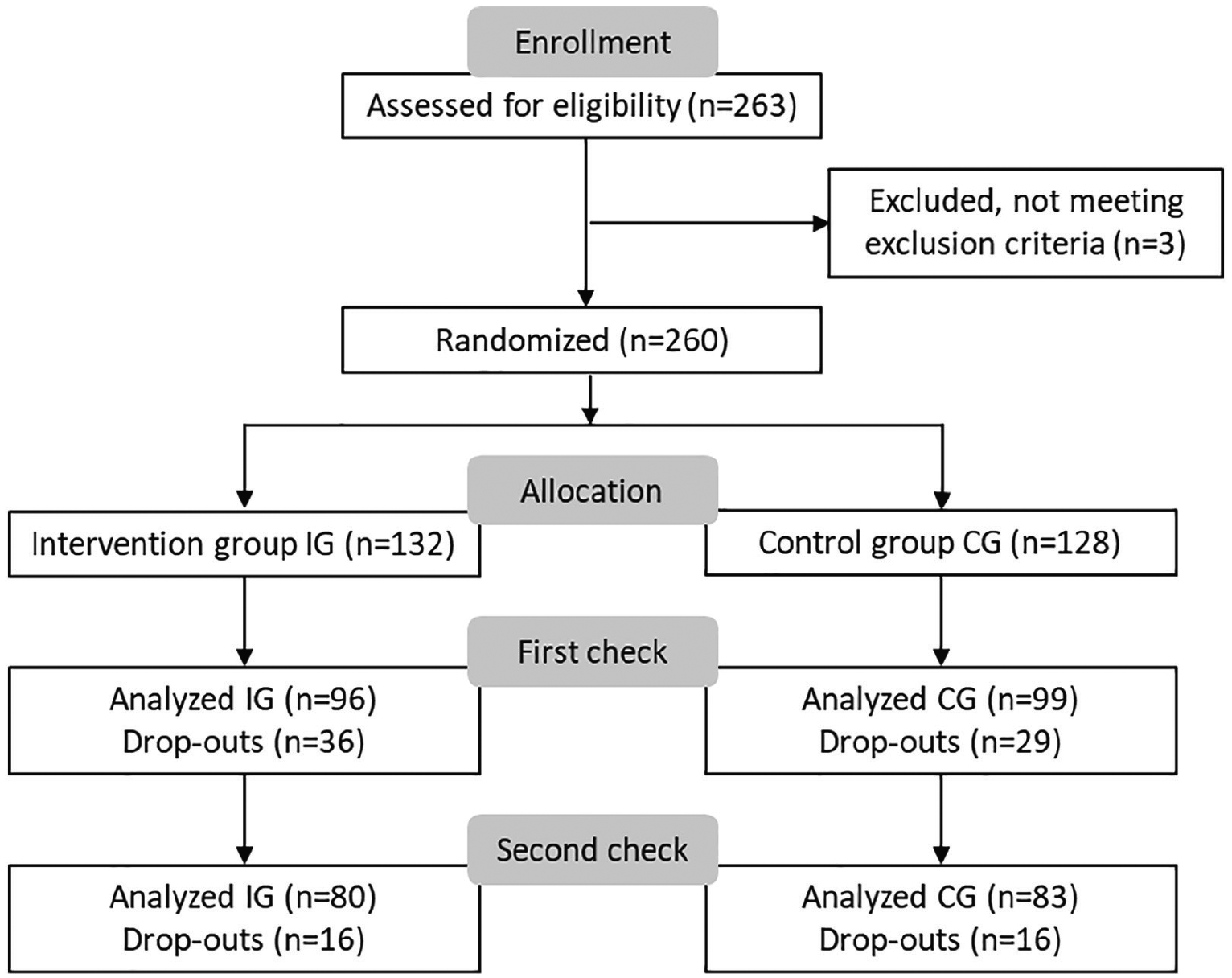
Flow chart of participant enrollment, randomization, and analysis at the first and second checks. Participants were randomized to the intervention group (IG) or the control group (CG). The first check occurred no later than 14 days after the start of the intervention and the second check at 6 months post education.
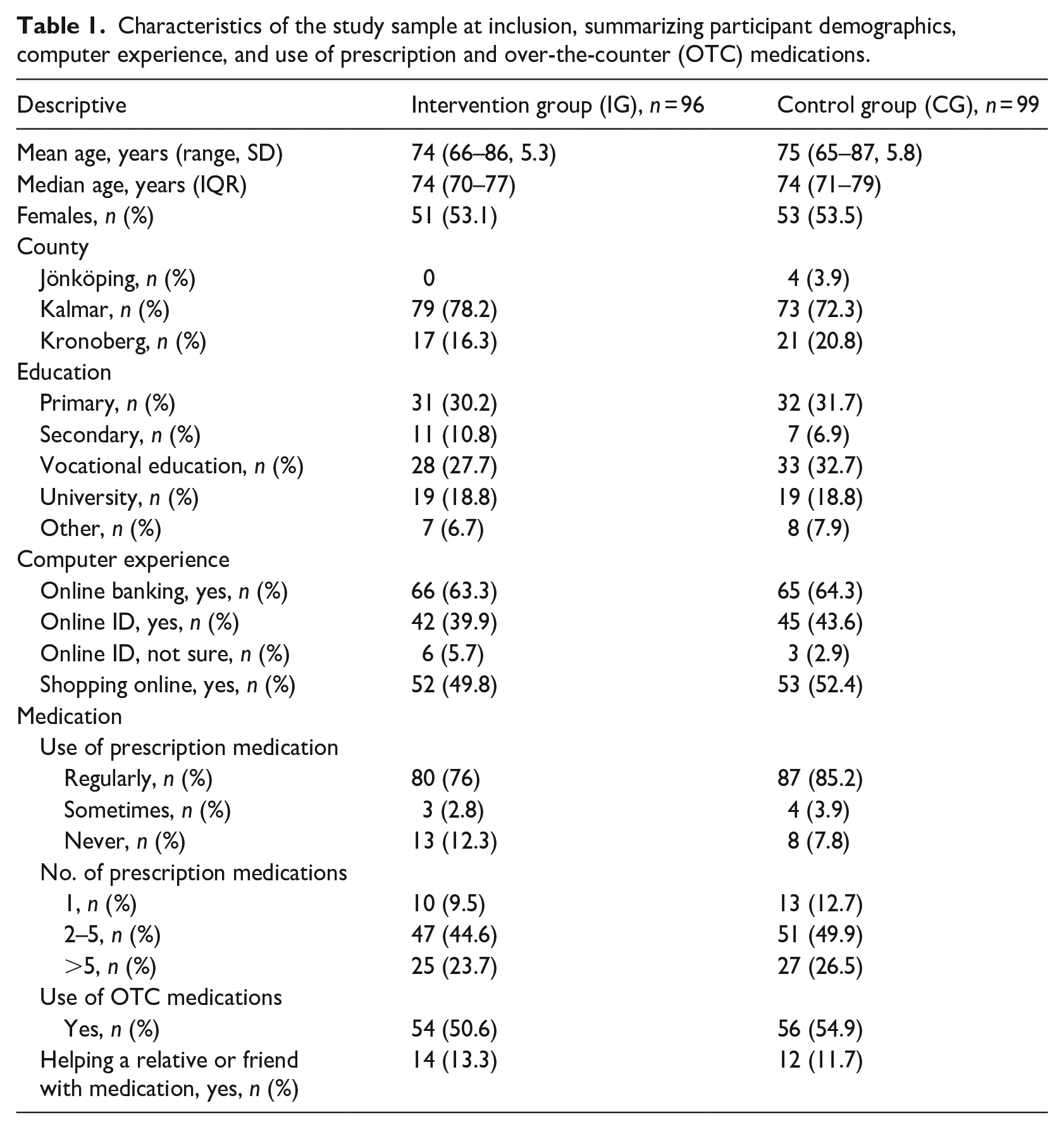
Table 1 presents the demographic characteristics of the study groups (IG and CG) at inclusion. Among the participants, the mean age for the IG was 74 (SD 5.30) years and that for the CG was 75 (SD 5.84) years; 52.0% and 52.5% were women. The participants’ computer experience was exemplified by 60% of them using online banking, 50% using an online ID and nearly 50% having experience of shopping online. There were no differences (p > 0.05) between IG and CG in demographic characteristics at inclusion (Table 1).
Characteristics of the study sample at inclusion, summarizing participant demographics, computer experience, and use of prescription and over-the-counter (OTC) medications.
The knowledge test
The web-based education had an effect on the participants’ multiple-choice scores at both the first and second checks (Table 2). The proportion of questions answered with the “Do not know” alternative was 6.3% for the IG and 17.5% for the CG at the first check. The corresponding figures at the second check were 12.3% for the IG and 18.2% for the CG.
Mean total scores and mean scores based on the age of the participants in the intervention and control groups regarding the multiple-choice questions at first and second checks.
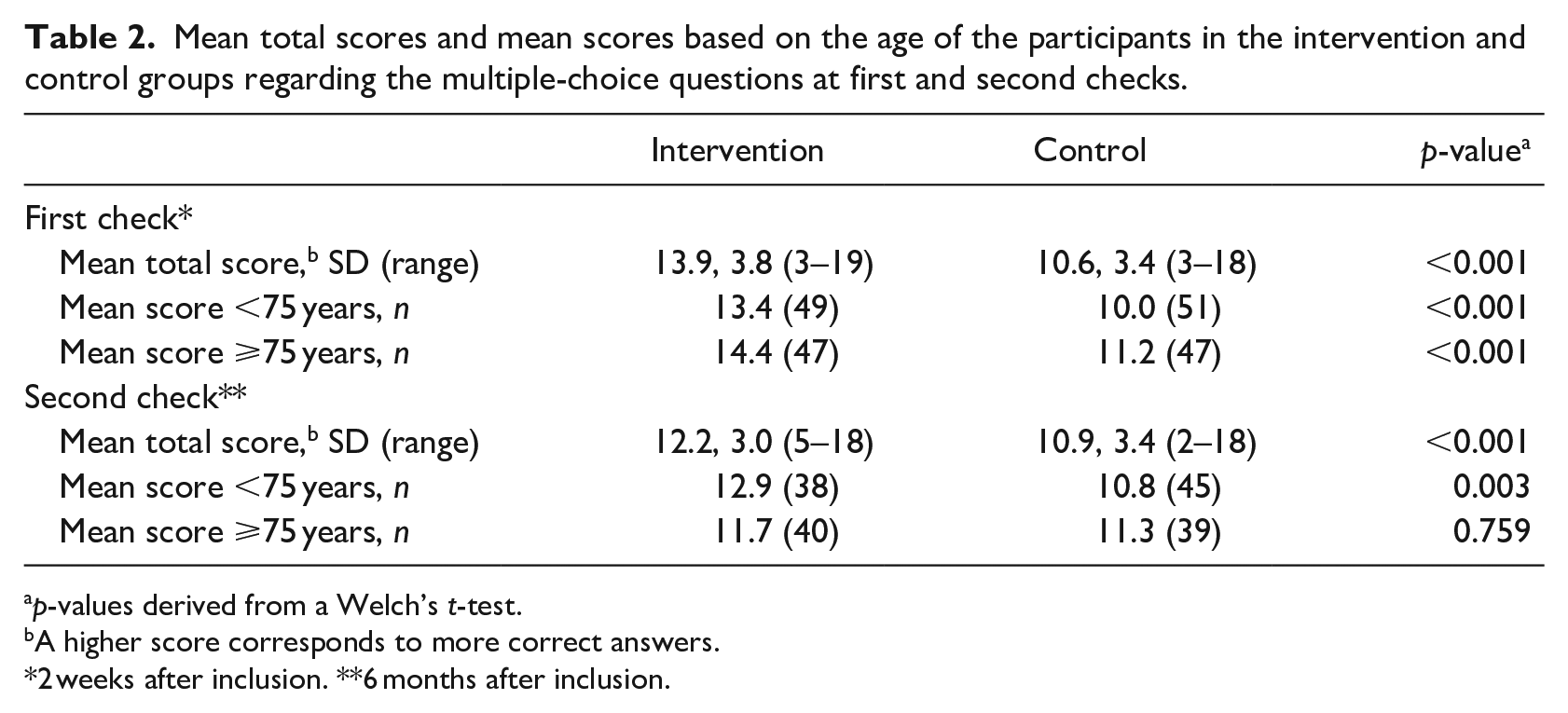
p-values derived from a Welch’s t-test.
A higher score corresponds to more correct answers.
2 weeks after inclusion. **6 months after inclusion.
At the first check, ten of the 20 questions were correctly answered by 75% or more of the participants in the IG. Those questions were derived from the following five modules: generic drug substitution, the pharmacy benefit scheme, drug interactions, medication lists, and frequently asked questions. In the GC, three questions from two modules were correctly answered by at least 75% of the participants: the pharmacy benefit scheme and medication lists.
Analysis based on age
When the IG and CG were dichotomized by age, that is <75 years and ⩾75 years, both age groups in the IG scored higher in the knowledge test than the corresponding age groups in the CG, except for participants aged 75 years or older at the second check (Table 2).
Analysis based on educational level
When the participants were categorized based on educational level, the IG participants, in all educational groups except secondary school, scored higher for the knowledge test (p < 0.05) than the CG participants at the first check (Figure 2). At the second check, there was a statistically significant difference between the IG and CG only in the primary school category.
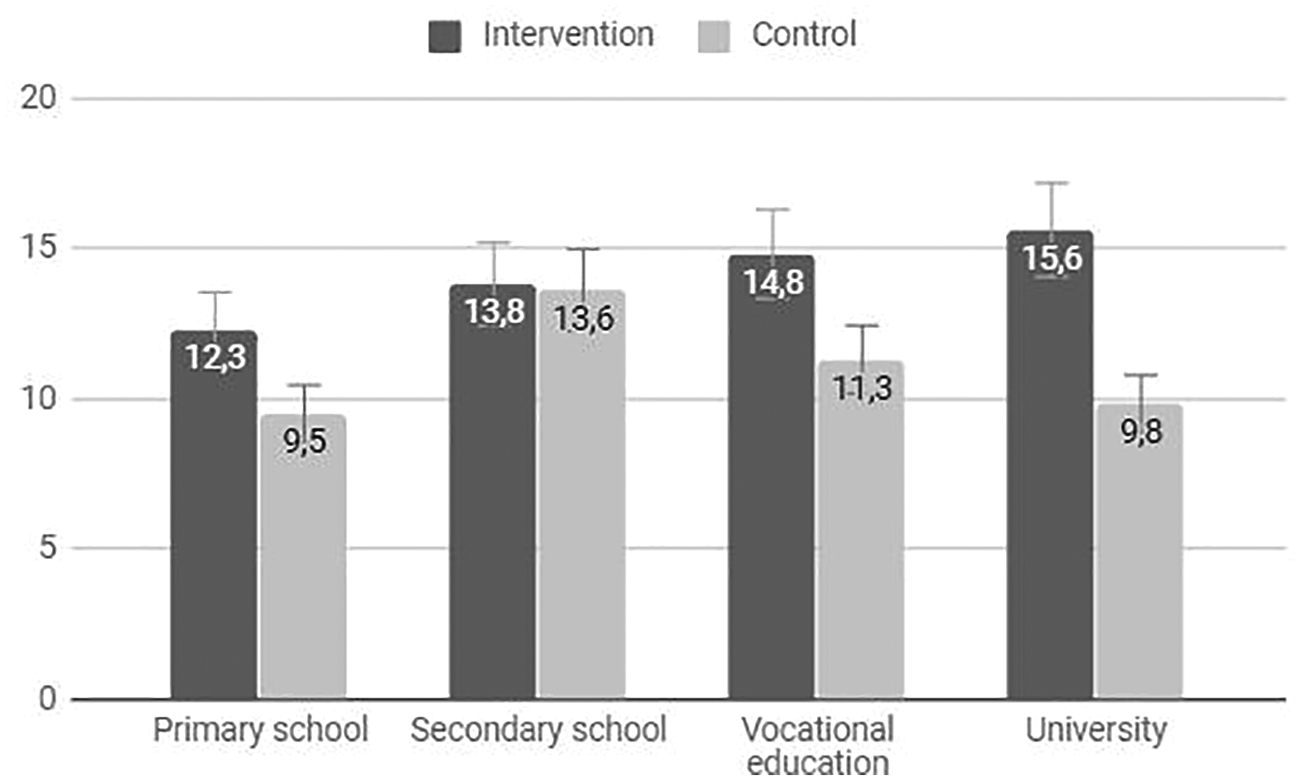
Distribution of the scores (means and standard deviations) for the knowledge test according to educational backgrounds in the intervention and control groups at the first check, that is, 2 weeks after inclusion.
Within-group differences based on educational levels were found as follows (Figure 2). Within the IG, those with a university or vocational education scored higher than those with a primary education (p < .05). Within the CG, those with a secondary school education scored higher than those with a primary school education (p < 0.05). There were no within-group differences at the second check.
Free text comments
The participants wrote 41 comments, 28 at the first check and 13 at the second. About half concerned generic drug substitution, and all of these were associated with a negative perception of generic drug substitution. Five comments concerned side effects, with all expressing the view that side effects caused great harm. Seven comments concerned general perceptions of aging and medications, medication costs, and communication with healthcare professionals. There were also five comments about the educational content of the modules, most of which indicated that the content had an interesting pedagogical approach.
Concerns about and self-assessed understanding of drug utilization
There was a significant difference between the IG and CG at the first check for six statements of self-assessed understanding of drug utilization. These included the statements related to finding answers to questions about how to use medications; how the generic drug substitution system works; where to find information about specific medications, non-prescription medications in relation to other medications, and whether a pharmacy has a medication in stock; and the impact of aging on the effects of medication (Table 3). The number of participants who responded to the statements ranged from 81 to 93 in the IG and from 80 to 95 in the CG. The distribution of the answers to statements regarding concerns about and self-assessed understanding of drug utilization in the IG and CG at the first check is shown in Figure 3. At the second check there were no statistically significant differences between the groups.
Responses to statements regarding concerns about and self-assessed understanding of drug utilization at the first and second checks (at 2 weeks and 6 months post initiation) using a 6-point Likert scale ranging from 1 (strongly disagree) to 6 (totally agree).
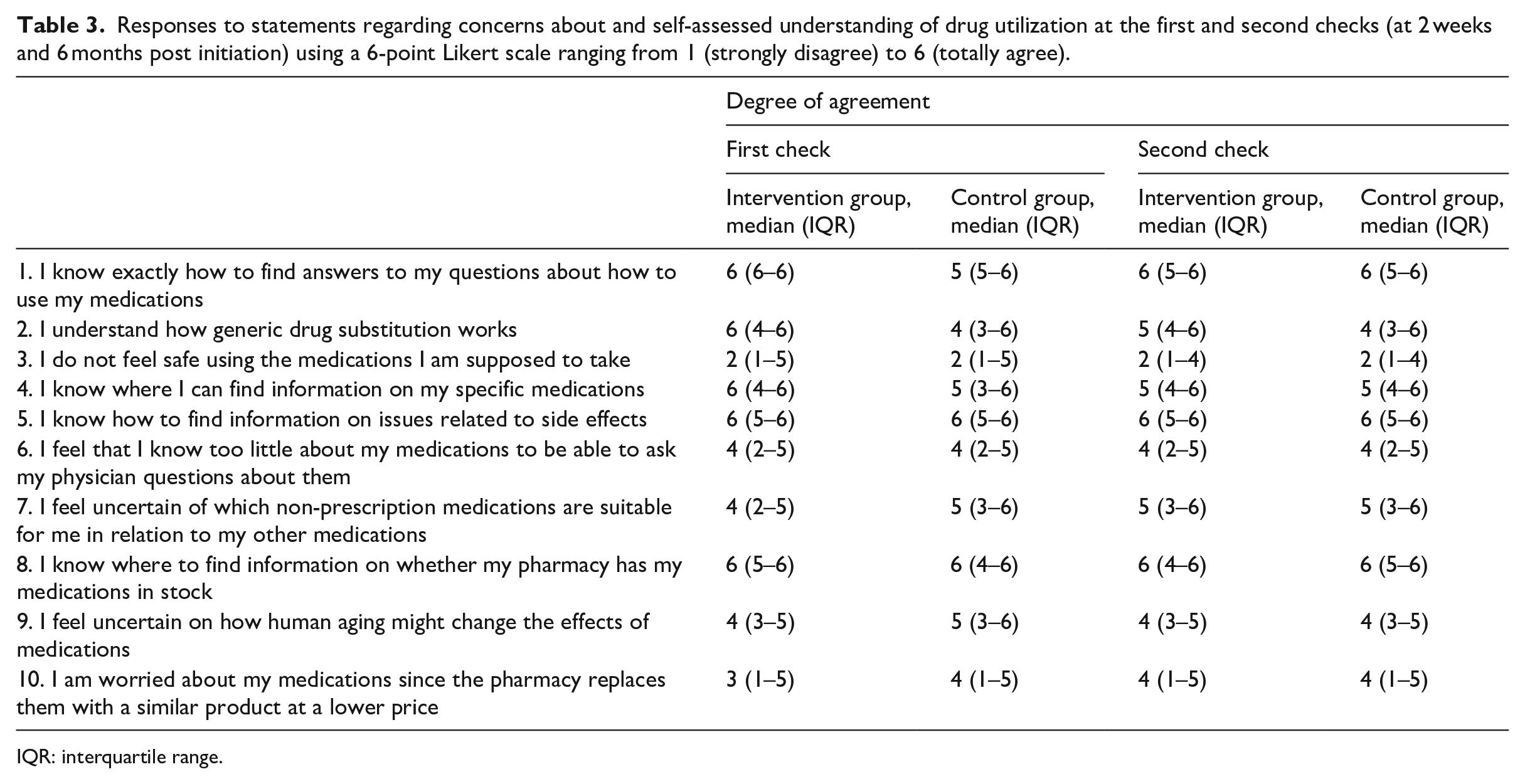
IQR: interquartile range.
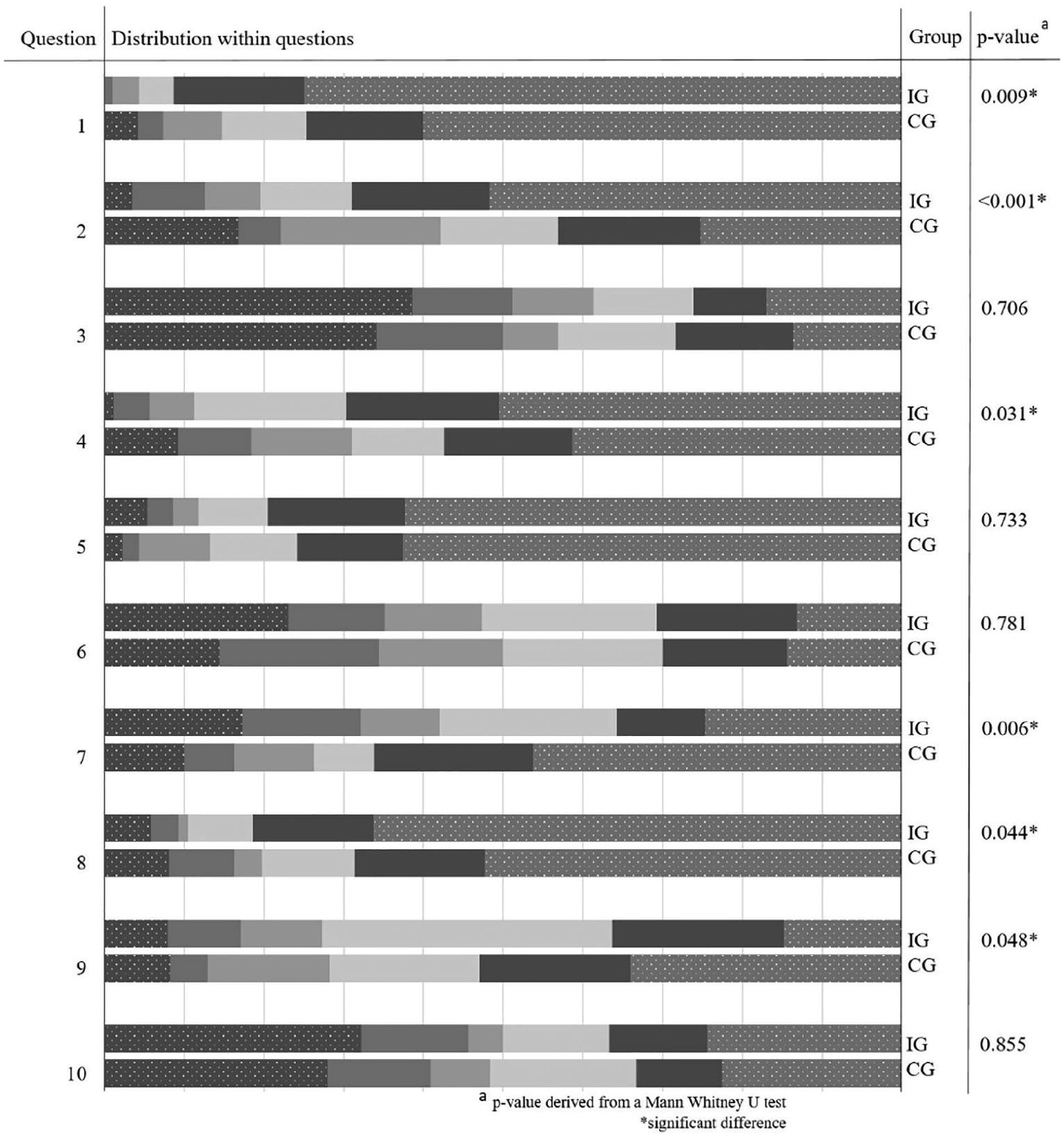
Distribution of answers to statements regarding concerns about and self-assessed understanding of drug utilization in the intervention group (IG) and the control group (CG) at the first check; comparison question-wise between groups. The degree of agreement was scored on a 6-point Likert scale ranging from 1 (strongly disagree) to 6 (totally agree).
BMQ-General
There were no differences between the IG and the CG in any of the BMQ-General subscales Overuse, Harm, or Benefit at either the first or second checks (p > 0.05). The participants agreed most with statements regarding Benefit, less with statements regarding Overuse, and least with statements regarding Harm (Table 4; higher scores indicate better agreement).
Valid cases, medians, interquartile ranges (IQR), means, and standard deviations (SD) for the BMQ-General subcategories overuse, harm, and benefit in the intervention group (IG) and the control group (CG).
Discussion
This study shows that the use of web-based education can improve drug utilization literacy in elderly individuals. The IG scored higher on the multiple-choice test at both the early check, 2 weeks after initiating the course, and the late check, 6 months after initiating the course. The web-based course also had an effect on the participants’ assessment of their own understanding of drug utilization after 2 weeks. However, the education program did not appear to affect the concerns of the participants about drug utilization or their general beliefs about medications.
Benefits of web-based educational interventions
Web-based patient education has been proven to increase patients’ knowledge and satisfaction in several fields,24,25 including that of health literacy. 26 However, there seems to be a gap in the research on web-based educational interventions in the context of drug utilization. It has been suggested that non-web-based educational interventions could have positive effects on knowledge about medications.15,14,16 Knowledge-enhancing interventions have been directed toward the elderly regarding correct medical use in general as well as more practical issues such as the ability to read information on and open containers. 16 Educational content regarding medication is often paper-based, a format that may not be fully understandable by all elderly people.27,28 A web-based education can be offered to patients or there closely related as a complement to other ways of informing about medications. The education course on drug utilization in this study could complement person-centered medication counseling by healthcare professionals. The online format is advantageous since the course can be accessed at a time and place that is convenient, can be viewed at a pace that suits the user and be repeated as required. 18 The audiovisual content can overcome barriers that poor literacy creates for some makes the course more memorable. 29 Still, traditional non web-based education might be preferred by some individuals.
Role of drug utilization literacy
Drug utilization literacy is important for several reasons; for example, it is important for patients to be able to use their medications as intended 9 and more knowledgeable patients are expected to be more confident in decision-making about their medications. 4 Improved medication literacy, which mainly refers to the patient’s own medications, correlates to a lower risk of patients experiencing negative consequences as a result of the unsafe use of medications. 30 Drug utilization literacy could also impact on medication use, although the relationship between drug utilization literacy and clinical outcomes needs further investigation.
The focus of this study was the education of elderly patients, an important group to target since polymedicated elderly patients notoriously have poor medication literacy. 1 The sub-group of the oldest participants (⩾75 years) had similar multiple-choice scores at the knowledge test to those of the younger sub-group (<75 years) at the first check. However, 6 months later, the effect of the intervention in the oldest group did not remain, in contrast to the younger group. This may have been because the oldest old do not recall as much information as the younger old, even though all participants were free to repeat the education course whenever needed. We were unfortunately unable to collect information about the extent to which the intervention group accessed the website during the 6-month study, preventing further analysis. However, we chose to give the participants unrestricted access to the modules as this simulates reality better than predefining a certain “dose” of education. Additionally, the group comparisons of the knowledge test scores based on educational level revealed that all participants in the intervention group, except those who went to secondary school, scored higher in this test than the control group participants. This might indicate that educational level does not have any substantial impact on the ability to gain knowledge from the course. However, the largest difference between the IG and CG groups occurred in those with a university education, so it may be that education favors those with higher educational levels, to some extent.
Generic drug substitution
The study found that self-assessed understanding of drug utilization was affected by the course. For example, the participants in the IG felt more knowledgeable than participants in the CG about how generic drug substitution works. Nonetheless, although the present study appeared to improve understanding of generic drug substitution, most of the free text comments in the questionnaire were negative regarding this subject. Furthermore, about half of the participants in both groups agreed that they were worried about their medicines because of generic substitution. Since generic drug substitution has previously been recognized as causing patients worry and confusion, 31 this might indicate that there is a need for the generic drug substitution system to be further evaluated from a patient’s perspective.
Patients’ beliefs about medications
Concerns about prescribed medications are commonly related to worries about long-term effects, side effects, risks of dependence, and medication costs. 32 Improving patients’ beliefs about medication might be important since patient’s beliefs about medication seem to influence drug utilization 33 and the involvement of patients in active disease management. 34 However, there could be reasons for changes in beliefs about medication other than having taken part in educational web-based modules. For example, general beliefs about medication could be affected by the individual’s medication use, educational level, 35 and general attitudes toward medicine, science and medication, by the media and by previous experience. 36
Strengths and limitations
One of the strengths of this study was the choice of methodology. Randomized controlled trials are the most suitable study design for determining whether there is a relationship between the intervention and the effect. 37 Since the kind of information doctors want to give and the kind of information patients want to receive appears to differ, 38 taking into account the views of patients is another strength of the study. It is also important that both the patients’ actual knowledge and their self-reported knowledge were measured, and that there was a relatively long follow-up between the first and second checks.
There were some limitations in the study. Firstly, because the participants were recruited from pensioner and patient associations, the sample might not be representative of all elderly. For example, the participants might have had better health literacy than individuals who were not members of pensioner or patient associations. Secondly, participants from only one region were included and our sample may have differed from those in other regions as a result of cultural differences. Data on patients’ knowledge about drug utilization before the education were not collected. Because of the randomized design, demographics in the groups were similar at baseline, and one could expect also pre-intervention knowledge to be similar between groups. Still, some participants might not have had any advantage of the course because they already had high knowledge. Lastly, individuals with poor digital literacy may not have been able to take advantage of the course because of the format.
Future studies
Further study is required on the effects of web-based education on clinical outcomes such as adherence, adverse events and drug-related problems. Future studies should also evaluate the effect of providing the education course in different formats or designs (such as interactive modules, which would enable discussion with other patients). There is also a need for investigation of different effects in relation to general health literacy and digital literacy, as well as research into optimal ways of implementing the course with respect to setting, participants and timing.
Conclusion
We conclude that web-based education modules can improve drug utilization literacy in elderly individuals. The IG scored higher on the multiple-choice test at both the first and second checks after the course. The web-based course also affected the participants’ self-assessed understanding of drug utilization. However, there appeared to be no effect on their concerns or general beliefs about medications.
Supplemental Material
sj-docx-1-jhi-10.1177_1460458220977585 – Supplemental material for Web-based education of the elderly improves drug utilization literacy: A randomized controlled trial
Supplemental material, sj-docx-1-jhi-10.1177_1460458220977585 for Web-based education of the elderly improves drug utilization literacy: A randomized controlled trial by Maria Qvarfordt, Victoria Throfast, Göran Petersson, Tora Hammar and Lina Hellström in Health Informatics Journal
Footnotes
Acknowledgements
The authors acknowledge the support of Aziz Ali Abdul, Lena Fossdal Finnas, Bo Hovstadius and Lisa Ericson for statistical, administrative and inspirational support, respectively.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The regional ethical board in Linköping, Sweden, approved the study (2014/472-31).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Kamprad Family Foundation. The funders were not involved in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.