
Abstract
The abstract of this article was orally presented at American Public Health Association Annual Conference Health Informatics Information Technology Section in Philadelphia, PA, USA, November 2009.
The literature suggests that there is a need for measuring public health informatics (PHI) competency to further understand whether current educational modules and modalities meet the needs of PHI practitioners and researchers to perform their jobs more effectively, particularly for mid-tier practitioners that constitute the majority of public health workers in the USA. The present study seeks to update current knowledge of the perceptions and experiences of PHI competencies proposed by the U.S. Council on Linkage in Public Health specifically for mid-tier PH practitioners and researchers. The results were collected and analyzed by using a Web-based survey (WBS) method administered among both practitioners and researchers. Researchers first compiled a draft list of candidate competency set by incorporating existing competency areas provided by: 1) the Council on Linkage; and by 2) those proposed by the USA’s Centers for Disease Control CDC Public Health Informatics Work Group. Nine sets of competency statements with 120 competency items and demographic information of respondents were included in the WBS. The online survey instruments were pilot-tested accordingly to incorporate feedback from respondents of the pilot. Fifty-six subjects were recruited from PH experts who were: 1) members of the Health Informatics Information Technology (HIIT) group of American Public Health Association; and, 2) members from the Community of Science (COS) Website who were the first authors published in the PHI field from PubMed. The sample included diverse backgrounds of PHI workers. They expressed an increased need for training to improve their PHI competencies. Respondents agreed that four competency sets should be adequately represented, including Leadership and System Thinking Skills (82%), followed by Financial Planning and Management Skills (79%), Community Dimensions of Practice Skills (77%), and Policy Development/Program Planning Skills (63%). The findings parallel current literature indicating that there exists an expressed need for clarification of the public health practitioner’s job-specific informatics competency. Findings of expressed needs for basic computer literacy training and community-based practice were consistent with those of the literature. Additional training and resources should be allocated to address the competency of leadership, management, community-based practice and policy advocacy skills for mid-tier public health practitioners to perform their jobs more effectively. Only when healthcare organizations properly identify PHI competency needs will public health practitioners likely improve their overall informatics skills while improving diversification for contribution across multiple settings.
Background
Computer and information technology (IT) have been employed to improve traditional public health practice for many years. Health informatics applications have gained heightened attention in recent years as a result of unprecedented public heath challenges of our times. These challenges include, but are not limited to, widening health disparities, increased natural and human-made disasters, and effective management of public health practice. Public health informatics (PHI) is the systematic application of information and computer science and technology to public health practice, research and learning. 1 Many public health practitioners are applying IT-related skills at work and, as such, it may be helpful to further understand PHI skills and competency in order to perform their jobs more effectively. PHI competency is directly related to a public health worker’s observable or measurable performance, skills or knowledge related to systematic application of information, computer science and technology to public health. 2 Further understanding of PHI competency could potentially provide guidance for developing PHI instructional modules and modalities and for realigning resource allocation relevant to this emerging field of importance. However, there is a paucity of literature in this area, as the definition of PHI competencies and a clear demographic profile of PHI working professionals in the field remain unclear. The following summarizes current knowledge based on the available literature.
PHI is a relatively new field of inquiry and practice as an independent discipline, although its applications have been widely adopted in the field. Informatics competencies in health have been proposed by many specialties and allied health professionals.3–7 Health informatics (HI) professionals have addressed HI challenges for them to fulfill their roles. 4 According to the literature, HI competency appears to be further developed in the biomedical and allied health field, with a primary focus on computer skills 8 and community-based practice. 9 For instance, the biomedical informatics community has defined core knowledge and skills of the field. 5 Dental researchers produced a working document to assist dental students and dentists to use the IT. 6 The nursing profession focuses on how the nurses use IT in their workplace and published the nursing informatics competencies.7,10–11 Most of the work in assessing informatics competencies to guide development of the training curriculum is in the biomedical, 12 nursing informatics 13 and dental 14 sciences. These studies underscored that: 1) there is a tremendous need to further develop training programs to meet the demand; and that, 2) materials varied widely within limited training modality in health informatics. The literature revealed that limitations exist in that they were either based on observational studies or survey sampling of limited subjects, thus limiting the potential of informing the development of PHI competencies for public health practitioners. However, until recently, there has not been generally agreed-upon appreciation of specific informatics competencies that various public health professionals embodied to effectively conduct informatics business. In 2002, the U.S. Centers for Disease Control and Prevention (CDC) Public Health Informatics Competencies Working Group drafted a set of PHI competencies for general public health professionals,2,15 which was a key component of a national agenda for PHI 16 that represents the first version of competencies for PHI practitioners in the USA. In addition, the Academia and Public Health Practice [Council on Linkages (COL)] developed and proposed a general set of core competencies for public health professionals. 3 Since then, PHI has grown rapidly, and substantial progress has been made in the application of IT to preventive health and healthcare through the development of the field of health informatics. For instance, the Electronic Health Record (EHR) is widely adopted as an important tool to support high quality healthcare 17 ; health information exchange (HIE) provides potential solutions for remote medicine, and geographic information system (GIS) is an emerging spatial analyst tool for information display and exchange. At the same time, the infrastructure for, and investment in, PHI has grown exponentially 18 . There are several centers of PHI at the federal and local levels, including the National Center for Public Health Informatics, PHIConnect Center for Public Health Informatics, and the CDC Public Health Information Network PHIN, to name a few. On the other hand, recent convergence of the rapid development of health informatics, specializations of PHI and an increased interest and investment in this emerging field call for further understanding of PHI competencies. However, several dimensions of this workforce remain less clear, including a demographic profile of the PHI workforce. As discussed above, the 2002 version of proposed competencies did not define PHI competencies for core identity and expertise in informatics. The literature also suggests that there is a need for a set of PHI competency statements to address mid-tier PH practitioners, who comprise a majority of public health workers in the USA.19,20
A comparison and contrast of the knowledge of informatics competencies would help address the increased demand for updated knowledge on PHI competencies and would be beneficial for guiding educational delivery and resource allocation. The present study was implemented to assess whether the informatics dimension of public health competencies are adequately represented. The competencies are a set of skills, knowledge and attitudes necessary for the broad practice of public health. These competencies are required to foster workforce development by helping academic institutions and training providers develop curricula and course content, as well as to evaluate public health education and training programs. The competencies are also used in practice settings as a framework for hiring and evaluating staff and assessing organization-wide gaps in skills and knowledge. The present study, targeted at a mid-tier public health work force, assessed those core ‘informatics competencies’ essential to help ensure competent and engaged employees. In the context of the present study, mid-tier public health professionals are defined as those workers with an MPH (or related degree) and five years of work experience, or individuals not having a public health degree but having at least 10 years of public health or public health-related work experience. 21
Objectives
In response to the initiative of the COL between Academia and Practice in Public Health to revise the standard set of core competencies, the present study aimed at further understanding and updating the knowledge of whether PHI is adequately represented in public health core competencies by surveying practitioners and researchers on their perceptions and experiences. A secondary research question was to learn the professional profile of PHI respondents in this study. This was accomplished through administering a Web-based survey (WBS) method to gather responses from practitioners and researchers working in the field.
Materials and methods
Study design
This study was conducted in 2009 by a team of researchers and practitioners of PHI, employing a cross-sectional survey design. The survey population was designated to be mid-tier PH professionals, including PHI practitioners, researchers and members of the American Public Health Association (APHA) Health Informatics Information Technology (HIIT) Group. Almost all respondents had hands-on experience of PHI. Subject matter experts were identified from three sources: 1) members of the aforementioned APHA HIIT Group; 2) the Community of Science (COS;www.cos.com) Website; and 3) first authors published in the field of PHI, as identified from the PubMed database (www.pubmedcentral.gov). A total of 240 eligible practitioners and researchers with relevant experience were recruited via email to participate in the online WBS.
Survey instrument
The survey instrument was administered through a WBS data collection system developed in-house by the research team to collect data for the revision of PHI competencies. The system included Web page forms (developed in ColdFusion™; San Jose, CA, USA) and a database (Microsoft™ Access™; Microsoft, Redmond, WA, USA) that enables users to enter data via the Internet from their own computers. Each respondent received an email with a unique identifier [i.e. study identification (ID)] for them to log onto the survey system. The instruments consisted of 9 sets of competency domains incorporating 76 competency items drafted based on: 1) the 2008 core competencies by COL; and 2) the AMIA Workgroup Proposed Public Health Informatics Competencies, with additional demographic information of respondents. The competency items were divided into the following nine domains: 1) analytical assessment skills; 2) policy development/program planning skills; 3) health communication skills; 4) cultural competency skills; 5) community dimensions of practice skills; 6) public health sciences skills; 7) financial planning and management skills; 8) leadership and system thinking skills; and 9) other skills. The first eight domains corresponded directly to the draft competency sets proposed by the COL. The additional category of ‘other skills’, which included a set of skills, knowledge and abilities more specifically related to health informatics, was derived from AMIA Workgroup proposed public health informatics competencies. The response options included both Likert-type, categorical scales and free-texted, open-ended questions for additional response/feedback. The survey instruments are shown as a screenshot in the Appendix section.
Data collection procedures and methods
The study was approved by the University of Texas Health Science Center’s Institutional Review Board. Each potential respondent was invited to participate in the online survey by receiving an email invitation, such as the one shown on the following Web page: http://www.utsurvey.org/phicompetenciessurvey2008_dev/welcome/index.cfm?id=test
Survey participants were assigned unique ID numbers that would authenticate them to access the survey Website to participate in the study. No financial incentive was offered to those chose to participate in this study. Participants also read and electronically signed the informed consent form at the start of the online survey.
In March 2009, the first batch of emails was sent to COS members and PHI experts and a follow-up reminder email, identical to the first, was sent a week later. For the APHA HIIT Group, the initial email was sent on 23 March 2009 and a follow-up reminder sent on 30 March 2009. Data were analyzed using SPSS 11.5.0 (Chicago, IL, USA). Analyses included simple descriptive statistics and crosstabs were employed to determine the distribution of responses to the research questions.
Results
The survey universe included 240 potential participants. Tables 1–3 describe the demographic characteristics of the respondents. A total of 56 full and valid responses were completed, representing a 23.3% response rate. The survey participants indicated that they were male (42.9%, n = 24), female (33.9%, n = 19) and the rest (23.2%, n = 13) did not respond to the gender question. The COS members and PHI experts (21.4%, n = 12) formed the smaller group of respondents and APHA HIIT members (78.6%, n = 44) were the majority.
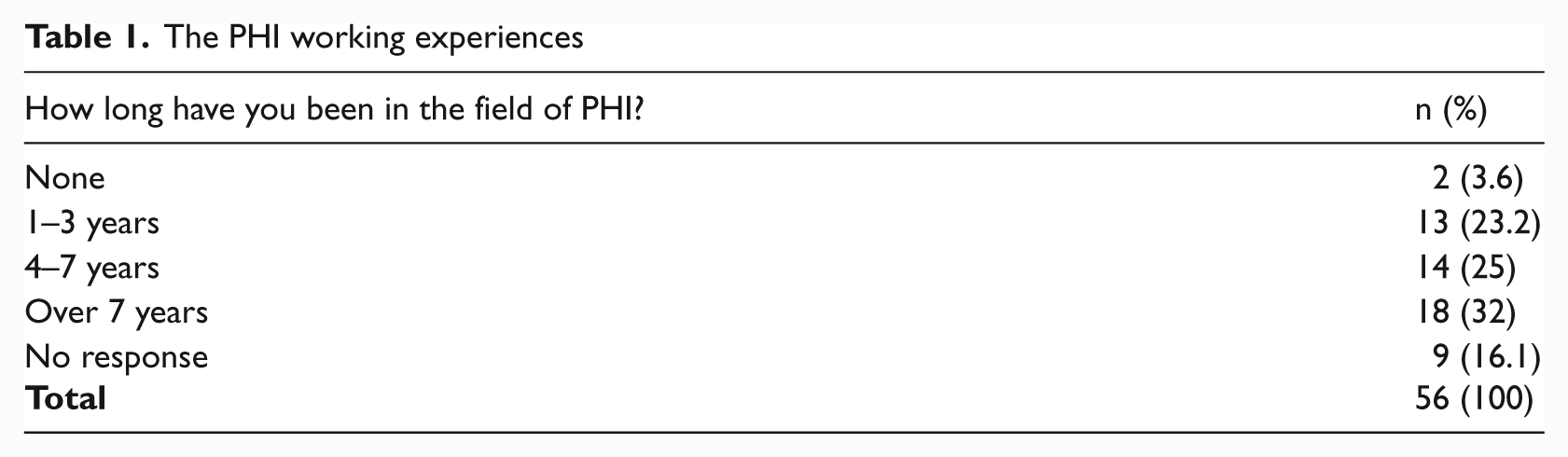
The PHI working experiences
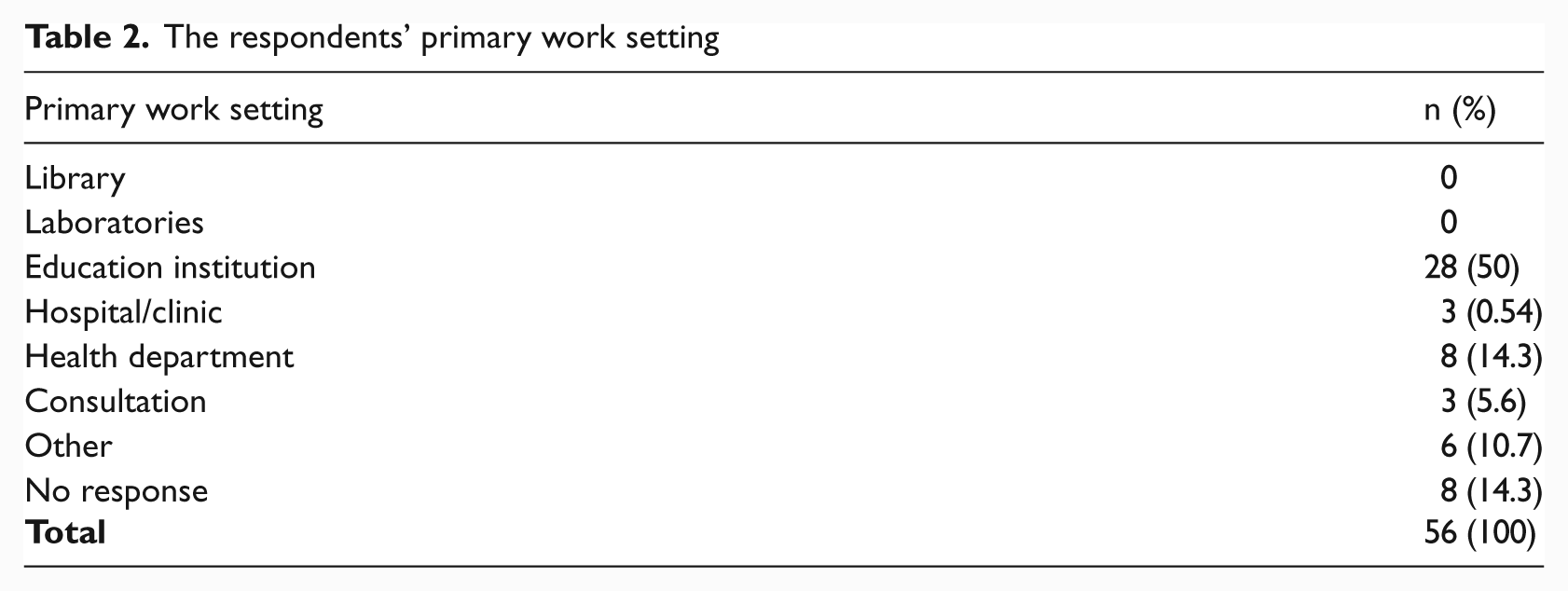
The respondents’ primary work setting
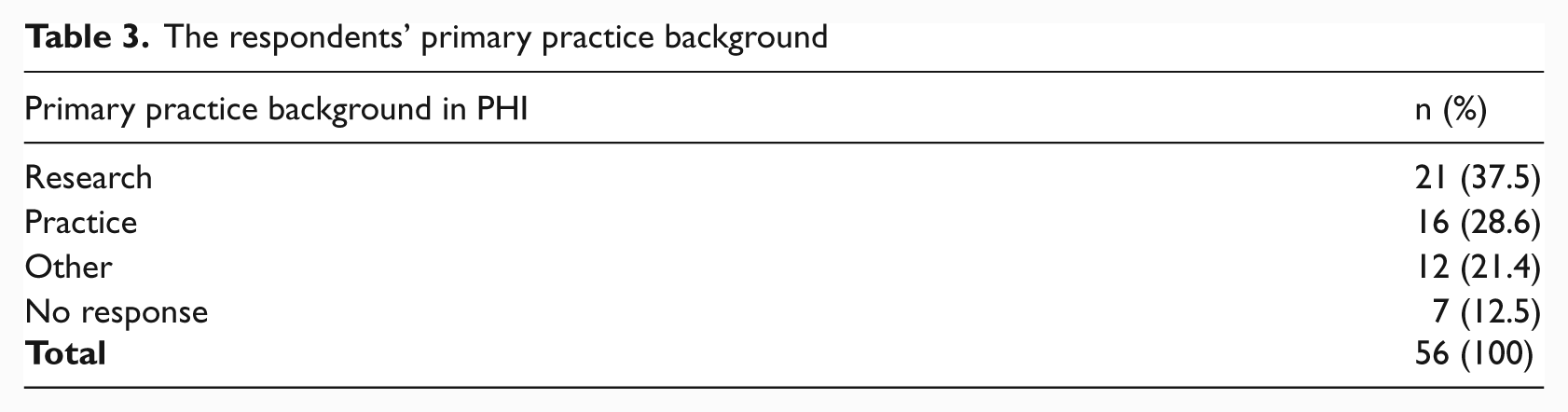
The respondents’ primary practice background
The relatively low valid response rate (23.33%, n = 56) is consistent with the average expected rate for an unsolicited and no-incentive WBS. Thirty-six percent (n = 22) of the respondents to the survey provided information regarding their previous occupational backgrounds if not in informatics. Their responses grouped by theme are listed below:
education (four responses);
medicine (four responses);
public health (seven responses);
data analyzer (two responses);
- IT (two responses).
Age range, race and ethnicity, education and experience
In terms of age distribution, just over two-fifths (42.9%, n = 24) of respondents were between the ages of 35–49, under a fifth (19.6%, n = 11) were aged between 18 and 34 and a quarter (25%, n = 14) were 50 years old and over but younger than 65 years old. With regards to race and ethnicity, the majority of those that responded to the race question were white (42.9%, n = 24), followed by Asian (19.6%, n = 11) and black (17.9%, n = 10);the largest ethnic group was non-Hispanic or Latino (75%, n = 42). In terms of highest educational attainment, most respondents possessed advanced degrees with graduate school (85.7%, n = 48) being the most frequently selected answer. When asked about years of practice experience, over two-fifths of respondents (41.1%, n = 23) indicated that they had a previous background that was not in informatics. A quarter (25%, n = 14) of the respondents had 4–7 years of experience in PHI, as highlighted in Table 1. Those who had over seven years of experience represented approximately a third (32%, n = 18) of the respondents, followed by 4–7 years (25%) and 1–3 years (23%). Half (50%, n = 28) of the respondents who chose to respond worked for an education institution (Table 2); the next largest group worked for a health department (14.3%, n = 8).
Twenty-one (37.5%, n = 21) of the respondents indicated that their primary practice background in PHI was in research and 16 of them are in the practice (28.6%, n = 16; see Table 3).
Competency domains
The survey instruments enquired as to whether PHI was adequately represented in the 2008 core competencies drafted by the COL for mid-tier public health practitioners. Almost half of the respondents (48.2%, n = 27) agreed that ‘Analytical Assessment Skills’ are an important skill-set for a mid-tier PHI practitioner (Table 4), followed by the competency domain of ‘Policy Development/Program Planning Skills’—almost two-thirds (62.5%, n = 35) of the survey participants agreed that this is an important competency set. ‘Communication Skills’ are viewed with almost equal relevance (37.5%, n = 21) and irrelevance (35.7%, n = 20) from the responses given. Regarding the ‘Cultural Competency Skills’ domain, almost half (46.4%, n = 26) of those surveyed concurred with its importance. A three-quarters majority (76.8%, n = 43) agreed that the ‘Community Dimensions of Practice Skills’ are an essential part of the mid-tier PHI practitioner’s repertoire. A slight majority (41.1%, n = 23) of the respondents viewed ‘Public Health Sciences Skills’ as necessary and almost four-fifths (78.6%, n = 44) believed that ‘Financial Planning and Management Skills’ are also important. The highest number of affirmative responses (82.1%, n = 46) by the survey participants was for the domain of ‘Leaderships and System Thinking Skills’. Under the category of ‘Other Skills’ exactly half (50%, n = 28) of the respondents agreed that the qualities described under this domain are relevant.
The respondent rate for each domain of the survey
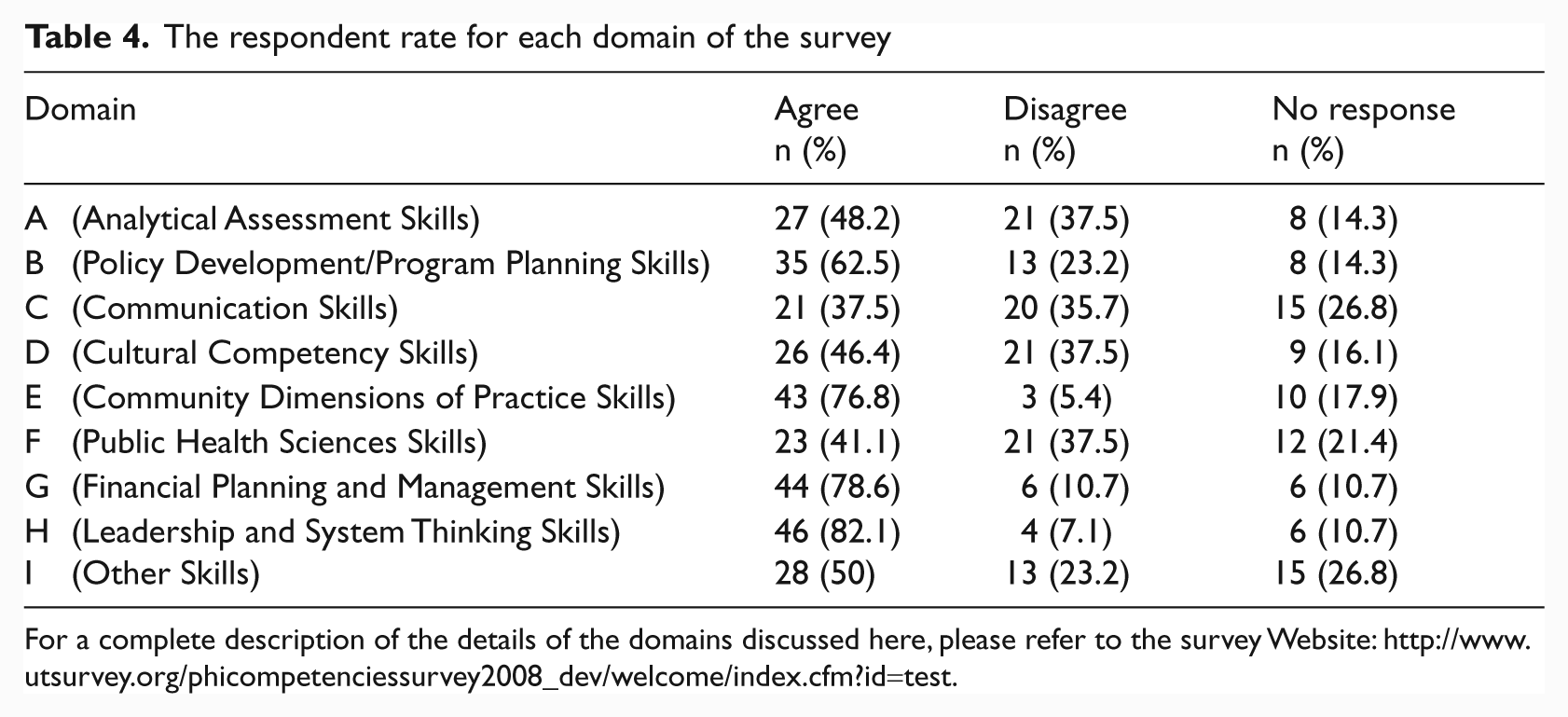
For a complete description of the details of the domains discussed here, please refer to the survey Website: http://www.utsurvey.org/phicompetenciessurvey2008_dev/welcome/index.cfm?id=test.
Discussion
With respect to the nine domains of competencies focused on in this survey, we rank ordered the responses in the affirmative in descending order, i.e. from highest to lowest for whether the competency set are adequately represented.
Leadership and System Thinking Skills (82.1%)
Financial Planning and Management Skills (78.6%)
Community Dimensions of Practice Skills (76.8%)
Policy Development/Program Planning Skills (62.5%)
Other Skills (50%)
Analytical Assessment Skills (48.2%)
Cultural Competency Skills (46.4%)
Public Health Sciences Skills (41.1%)
Communication Skills (37.5%)
The respondents suggested that ‘Leadership and System Thinking Skills’ is the most important set of core competencies and ‘Communication Skills’ the least important. Consistent with the literature, community-based practice and computer skills (listed as ‘Other Skills’) were perceived as a critical competency for PHI. Interestingly, exactly 50% (n = 26) of the respondents agreed that the domain of ‘Other Skills’ was ranked most important, while the other half of the respondents did not agree. Examples of questions asked under the ‘Other Skills’ domain were as listed below:
identifies interoperability issues and understands related knowledge;
supports efforts to harmonize PHI with other informatics domains;
supports use of informatics to promote disease prevention at the clinical health environmental and personal health interface;
supports establishment of systems to improve public health through access to clinical information;
perform basic health computing functions.
Respondents were also given the opportunity to provide their own explanations of additional skills that they perceived a mid-tier general public health practitioner should have. Some suggestions given were:
Support data linkages among public health programs.
Involvement with clinical integration would depend on priorities for the health department and readiness of the community. Mid-tier professionals do not have a lot of latitude to be on the leading edge of clinical data exchange or bioinformatics.
The skills ‘Supports use of informatics to promote disease prevention at the clinical health, environmental, and personal health interface’ and ‘Supports establishment of systems to improve public health through access to clinical care information’ can be put under public health sciences.
The core competencies of ‘Analytical Assessment Skills’, ‘Communication Skills’, ‘Cultural Competency Skills’ and ‘Public Health Sciences Skills’ had a surprisingly high disagreement rate amongst the respondents, with more than a third ranking them as both most important and least important. In addition to the high rate of disagreement is the apparent consistency in terms of the number of disagreeing respondents ranging from 20–21. Further investigation may reveal that it is the same respondents from similar backgrounds and practice areas that share this opinion.
Respondents were also given the opportunity to add additional comments to each core competency domain; their suggestions are cataloged as follows:
Analytical Assessment Skills
I would eliminate ‘Develops the methods and instruments for collecting quantitative and qualitative data’ and ‘Applies data collection processes, information technology applications, and computer systems storage/retrieval strategies’ from the competency domain. General understanding of integration challenges should be included in the competency domain. Explicitly mention the need to obtain and use data from the private healthcare delivery system to support public health aims. Contributes previous experience (if any) working in information systems in fields different than public health. Software project management for development and migration projects. ‘A person who could do all of this would also be able to walk on water. It is not clear how you expect these will be used. No one can do all of these well’.
Policy Development/Program Planning Skills
Policy issues related to informatics-oriented interests. Skills should include budgeting and risk assessments and remediation. Training courses for public health practitioners.
Communication Skills
Should leverage existing public health IT infrastructure and seek ways to reduce licensing and hardware costs. Is aware of emerging methods of electronic communication, e.g. social networking and considers how to make use of them. Some of these may or may not be relevant to mid-tier positions depending on responsibilities and responsibilities of senior level staff.
Cultural Competency Skills
I agree with the above but what do they have to do with cultural competencies? They refer more to ethical issues. Everyone should always do these two. These are important competencies but I am not sure they should be included in this section. Security might require a section of its own.
Community Dimensions of Practice Skills
Delete ‘Assesses the community from an ecological perspective’ from above. Understands the methods that communities and groups within them use IT to communicate and collaborate. Is able to subtract, understand and communicate to others the information gathered on a determined community based on it’s own rules
Public Health Sciences Skills
I support the above IT competencies but I am not sure if general public health professionals will have the time and resources to acquire knowledge and implement them in their every day practice. Understands the general methods of linking data resources for creating information. Some of these, again, should be done by everyone. Some are tasks for a job description, rather than competencies required to perform the tasks. Some of the Fs can be under program planning, some under leadership and systems thinking. Uses IT to assure openness of public health agency processes and responsiveness to the electorate and the public.
Financial Planning and Management Skills
Uses appropriate IT to create and manage budgets. Understands proper procedures for applying for grant-funded projects. Understands the financial and political processes associated with funding and budgeting for PHI projects. Communicate the needs and proposed solutions to leaders in public health and elected officials effectively.
Leadership and System Thinking Skills
Addresses IT development, using principles of systems engineering and systems thinking. Contributes to the consideration of the best IT and systems to use by the enterprise.
The additional suggestions and comments demonstrated the diversity of opinions and thought processes that practitioners utilize in the definition of what they perceive the core competencies of a public health informatician to be.
Limitations
Limitations exist in the present study. First, because this study was exploratory in nature, and the fact that the purpose of the study was to update knowledge of existing competency sets, the survey items were limited in scope. A more comprehensive instrument might include, for example, additional demographic questions on education, professional specialty and personal characteristics; similarly, follow-up questions on specific subject areas (such as public health preparedness and response) would have provided more accurate information about participants’ experience and training needs. Our results suggest that the practitioners that we surveyed have most training needs for leadership and management skills, yet many did not provide information on the specific training modules. Second, given that the study captured only a quarter of the potential study population and the fact that the data was collected through a WBS (in which the sample was self-selected to participate), the results should be generalized with extreme caution. Nevertheless, it should be noted that although the study focused on mid-tier practitioners, the results may provide reference points to learn more about other public health practitioners in general. Additional studies should explore this issue. Third, some participants did not respond to several key questions which resulted in missing responses. Lack of knowledge of what these missing values limit the ability to extrapolate the results. Further investigation should be made to determine why so many veterinarians chose not to answer these questions.
Footnotes
Acknowledgements
The participation of RD and DJ in this study was made possible, in part, by the National Public Health Leadership Institute through the U.S. Centers for Disease Control and Prevention.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.