
Abstract
Increased pressures from multiple sources are leading to earlier patient discharge following surgery. Our objective was to test the feasibility of self-care web applications to inform women if, when, and where to seek help for symptoms after hysterectomy. We asked 31 women recovering at home after hysterectomy at two centers to sign into a website on a schedule. For each session, the website informed them about normal postoperative symptoms and prompted them to complete an interactive symptom questionnaire that provided detailed information on flagged responses. We interviewed eight women who experienced an adverse event. Six of these women had used the web application regularly, each indicating they used the information to guide them in seeking care for their complications. These data support that self-care applications may empower patients to manage their own care and present to appropriate health care providers and venues when they experience abnormal symptoms.
Keywords
Introduction
Hysterectomy is one of the most common surgical procedures performed on women in developed countries. 1 There are 650,000–700,000 hysterectomies performed in Canada and the United States each year.2,3 Hysterectomy can lead to major peri-operative morbidity, including urinary tract and bowel injury, infection, hemorrhage, thromboembolism, and death. 4 A prospective clinical audit of 1330 hysterectomies with a form specifically designed to record complications from hysterectomy demonstrated that 26.4, 23.9, and 17.0 percent of patients with abdominal, laparoscopic, and vaginal hysterectomies, respectively, experienced adverse events. 5 A larger prospective cohort study with detailed questionnaires on 5279 hysterectomies demonstrated complication rates of 19.2, 15.4, and 11.7 percent in patients with abdominal, laparoscopic, and vaginal hysterectomies, respectively. 6 Because adverse events following hysterectomy can be common and some of the adverse events can be serious, we need excellent pre-surgical/in hospital patient education by health professionals and reliable methods of providing accurate information to women and their families once they return home.
Adverse events and their consequences after elective hysterectomy can be significant and costly for patients, surgeons, the health care system, and society. Diagnosing and managing serious adverse events often requires multiple outpatient and inpatient laboratory, imaging, medical, and surgical resources. 3 These investigations and procedures are uncomfortable, associated with their own risks and side effects, and costly. 3 Major adverse events after hysterectomy can negatively and permanently impact an individual’s length and quality of life. Even non-serious adverse events, such as urinary tract, wound, or pelvic infections, can cause discomfort, stress, and anxiety for patients. These less severe adverse events may also be inefficiently and ineffectively managed if patients present to inappropriate health care venues for evaluation and treatment. A recent retrospective chart review of laparoscopic hysterectomy and same-day discharge found that the most common reasons for visiting the emergency department within 48 h were pain and nausea. 7 The study concluded that detailed postoperative instructions may have prevented many of these early postoperative visits. 7
Gap in recovery information provided to patients
At present, informing and educating patients about their surgery and postoperative recovery consists of preoperative visits with their surgeons and nurses along with verbal and written instructions provided at discharge. At most Canadian hospitals, preoperative teaching is done by a registered nurse usually during a pre-admission visit a week or more before scheduled surgery. The majority of postoperative teaching in hospital is provided by nurses and is usually done as the patient is being discharged from hospital. Although this is the standard of care for Canadian postoperative patients, it is sometimes ineffective as women are often experiencing pain, and may be under the influence of anesthetic and narcotics, as well as feeling anxious or rushed about their discharge. Increased emphasis on cost-savings has reduced the amount of time spent in preoperative sessions with nurses. 8 About one-third of 102 hysterectomy patients surveyed felt that they had been provided insufficient information. 9
Patients are increasingly supplementing verbal and written information with online resources. The use of Internet-based self-management tools has improved the health status of patients with chronic disease when compared to standard non-Internet self-management programs. 10 Online tools have been developed to educate women about family planning 11 and to help quit smoking during pregnancy. 12 Online patient portals developed by hospitals to manage chronic diseases such as diabetes in children have been studied and found to have potential. 13 Electronic support tools available for aiding in recovery from surgery include the website Hystersisters.com, which has information that is not created by health care professionals but is instead centered on peer-support. In a study of 137 women who used the Hystersisters.com website, women found the information about recovery helpful; however, 39 percent found some aspect (often negative postings from some members) of the website not helpful in their recovery. 14 One study demonstrated that patients who used Hystersisters.com valued some information more if it was provided by a member perceived as knowledgeable. 15 A meta-analysis of 191 studies found that increased patient education shortens length of stay in hospital by an average of 11.5 percent and has beneficial effects for recovery, pain, and psychological distress. 16 A recent randomized controlled trial has shown that orthopedic patients who were given supplemental online information from authoritative sources to research on their own prior to their surgery modified their decision on spinal versus general anesthesia. 17 All of these studies suggest there may be a gap in the knowledge that patients have about their surgery and that it may be possible to help fill that gap with authoritative and reliable online or mobile app resources. With adverse events after hysterectomy occurring at home being relatively common and potentially serious, we also need to ensure these resources provide accurate, timely, and reassuring information tailored to their concerning symptoms and type of surgery.
Efficient navigation of a complex health care system
The Canadian health care system—with its many types of care providers and multiple access points for care—may leave patients uncertain as to where they should go when they experience symptoms of adverse events at home after surgery. 18 Early presentation, diagnosis, and treatment of evolving adverse events are critical steps in limiting their short-term and long-term sequelae. Early diagnosis and treatment of an adverse event also has a positive effect on the health care system, as early intervention can often prevent a hospital admission. Currently, no formal screening mechanisms are in place to survey patients quickly, routinely, and comprehensively for specific symptoms of adverse events after hysterectomy and to advise them when and where to go for appropriate care.
Proposal to fill information gaps
In response to all of these information needs and health systems gaps, we created the SAFER (Studying Adverse Events From Elective Surgery Research) web application. 19 The application consisted of surgery-specific, interactive applications designed to inform and empower patients to better care for themselves after surgery. We conducted a small study on 31 abdominal hysterectomy patients to see if they would access the self-care application from home after surgery and use the information to assist them in caring for themselves. Here, we report on 11 of the 31 women who suffered adverse events during the study and how using the application impacted their care and outcomes.
Materials and methods
Gynecologic surgeons met and determined the initial approach and content for the abdominal hysterectomy applications. The content was broken down to include a 2-min checkup to screen for symptoms, recovery advice on what is normal and not normal (specific to the patient’s day of recovery), as well as background educational content on hysterectomies. A medical writer and computer programmer transformed this information into the SAFER Abdominal Hysterectomy Self-care Web Application. Designed to be accessed regularly by patients recovering at home after surgery, the modules were concise and specific to abdominal hysterectomy and to the day of recovery after surgery. The self-care application was intended to be accessed daily during the first week at home and then twice a week for three more weeks. During each session, patients received brief, timely advice about how to care for themselves and were asked to answer 18 screening questions about specific symptoms after surgery (Appendix 1). Patients who gave a positive reply to a symptom question were provided additional information about the possible significance of the symptom and where they should go for further evaluation. They also had the option of accessing the symptom information without providing a positive reply to the screening question. Detailed information on the development, design, and implementation of the tool, including screenshots and patient feedback on the overall design, has been previously reported. 19 Here, we focus on the experience and outcomes of those who used the application and experienced an adverse event. These results will be used to support efforts to launch a larger study into the effect of these types of tools on adverse event rates and patient satisfaction.
After approval from the IWK Health Centre institutional review board, five women having abdominal hysterectomy enrolled in a small feasibility cohort. Women who had Internet access from home, who were comfortable using the Internet for basic services (e.g. banking, bill payment, and/or shopping), and who could speak and read English were included. These women were approached to join the study by a preoperative clinic nurse who was already scheduled to conduct the patient’s regularly scheduled preoperative appointment. The total number of patients approached by the preoperative clinic nurses was not recorded.
A research nurse gave a brief introduction and demonstration on how to use the website to the five women prior to their surgery. While recovering at home after surgery, they were asked to sign-in to the SAFER modules and complete the specified activities. These activities consisted of reading the daily recovery advice, answering the 18 symptom questions (Appendix 1), and completing a short free-text entry if they had to seek health care advice or treatment for a problem. Other activities included a preoperative questionnaire to record their demographics, information sources, expectations, and a postoperative questionnaire to record their satisfaction and health care access.
At the conclusion of their participation, all five women provided detailed feedback by taking part in a semi-structured telephone interview. We took into account patient feedback from this small cohort of five patients by modifying the content and utility of the application based on their comments and suggestions. This detailed patient feedback from these five women has been previously reported by the authors. 19
After obtaining institutional review board approval from the IWK Health Centre in Halifax and the Ottawa Hospital Research Institute in Ottawa, we tested the revised version of the online self-care application in a second small pilot cohort involving 26 women having abdominal hysterectomies at either of these two sites. These 26 women were asked to complete the same activities as the women in the feasibility cohort. For all women in the first (feasibility) cohort (n = 5) and the second (pilot) cohort (n = 26), we collected baseline demographic and usage rates for the web application. Adverse event occurrence was determined by medical research staff completing a medical chart review and contacting each participant to capture adverse events not documented in their medical chart. All 31 women were contacted 6 weeks post-surgery to inquire if they had experienced any other problems that required them to access the health care system. Qualitative details about these health problems were recorded. With the sample sizes being too small to draw definitive comparisons between groups and the fact that the pilot cohort largely followed the same methodology with minor revisions following the feasibility stage, all 31 women’s experiences are reviewed as one cohort in this article.
Results
Demographics
Figure 1 contains a flow chart of participant enrollment, compliance, and adverse event occurrence. Table 1 provides the demographic characteristics, broken down by adverse event occurrence, of the women who used the web applications and completed the demographic questionnaire.
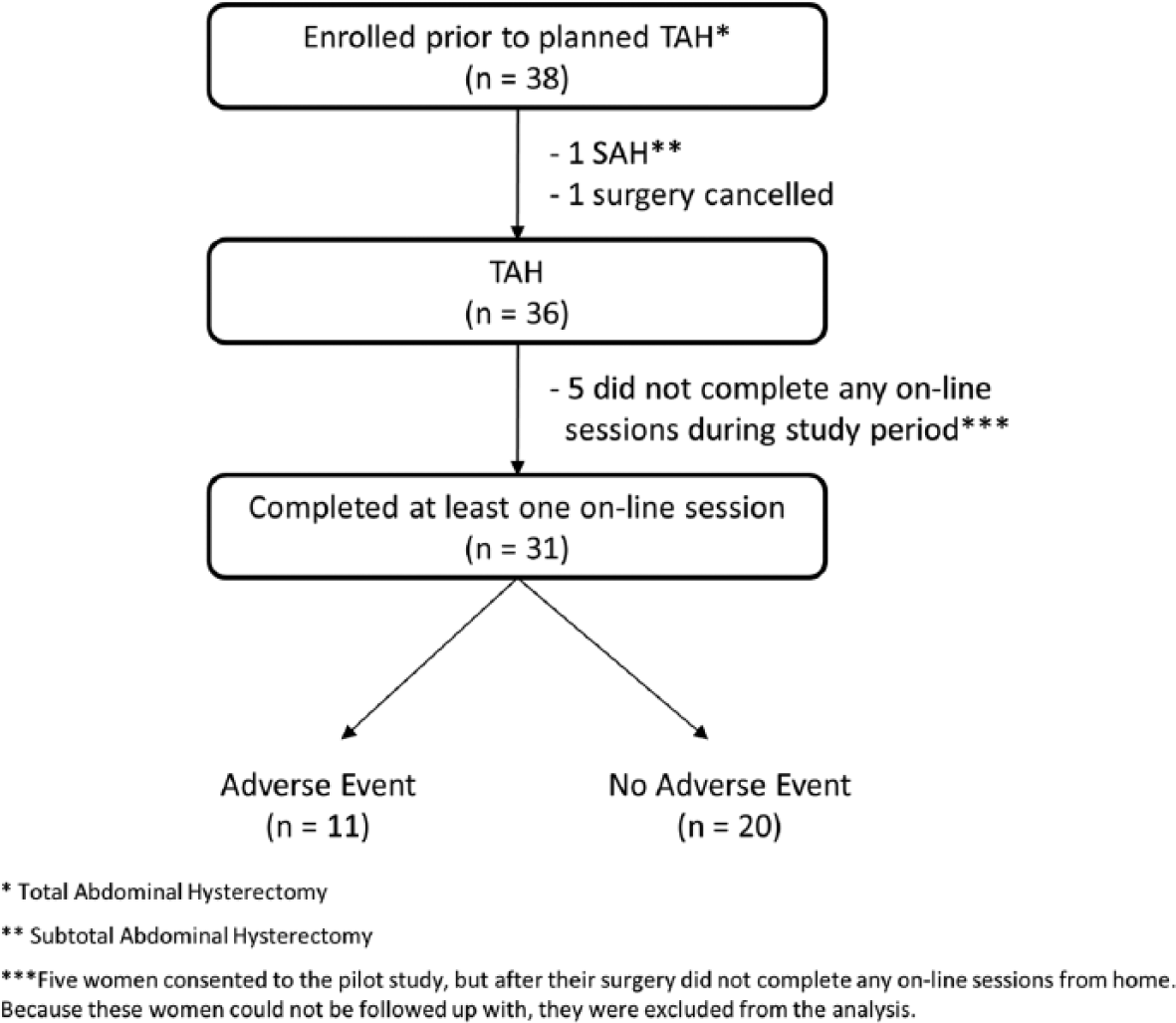
Flow chart of enrollment of study participants.
Demographic information of women who used the postoperative self-care web applications and completed the demographic questionnaire.
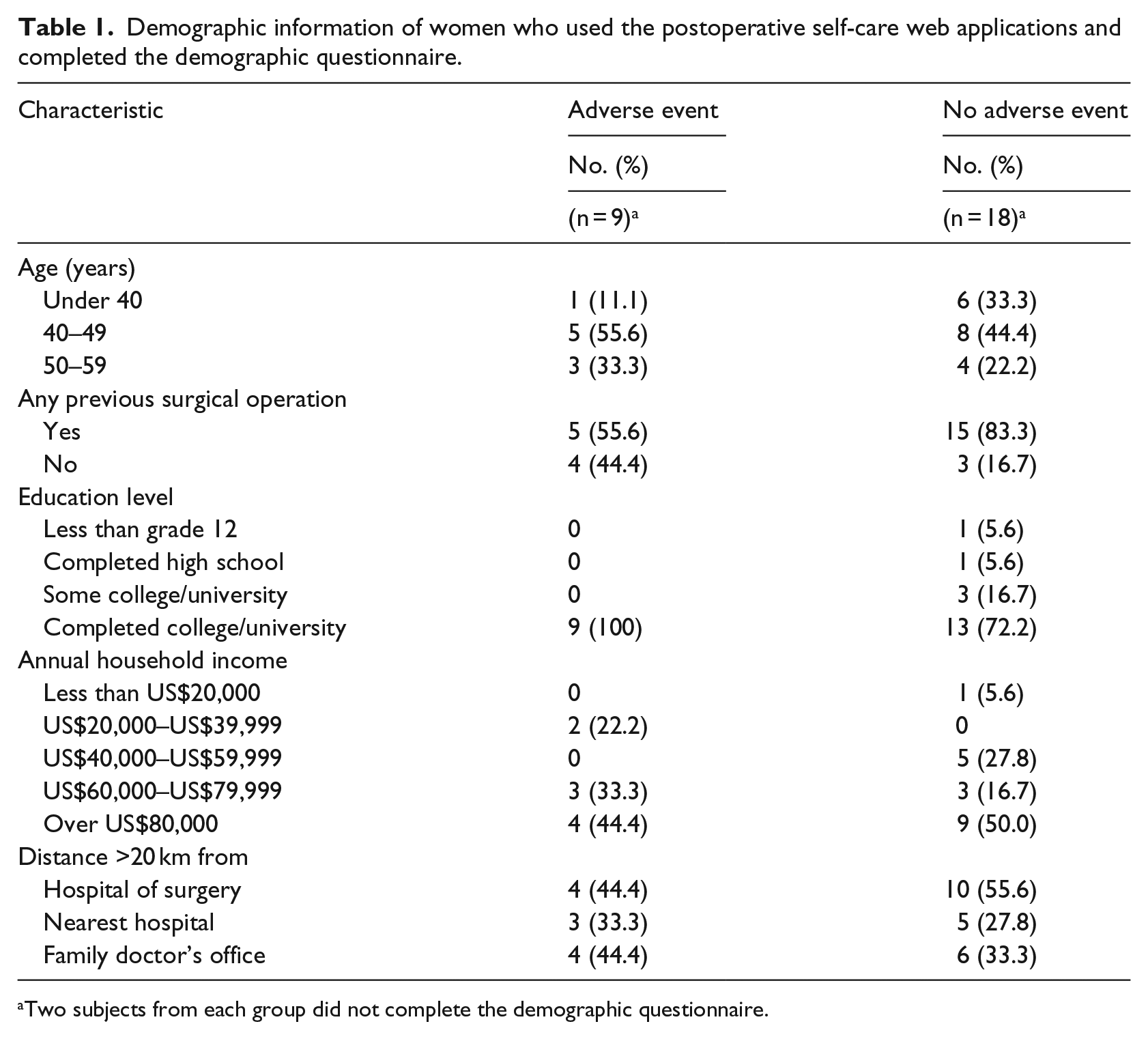
Two subjects from each group did not complete the demographic questionnaire.
Participants experiencing adverse events
Eleven (35%) of the 31 women who used the website suffered an adverse event after surgery. These adverse events consisted of one ureteral fistula, four wound complications, two vaginal vault complications (vault hematoma and vault cellulitis), and four urinary tract infections. No patient suffered more than one adverse event.
We were able to contact and interview 8 of the 11 women who experienced an adverse event. Three of the 11 women could not be reached for an in-depth interview. These three women had a urinary tract infection as their adverse event. For the eight women interviewed, Table 2 presents their diagnosed adverse event, the frequency of their web application usage, and whether the online material had influenced their decision to seek additional care.
Number of online sessions completed by eight participants a who experienced an adverse event and whether the information influenced their decision to seek additional care.
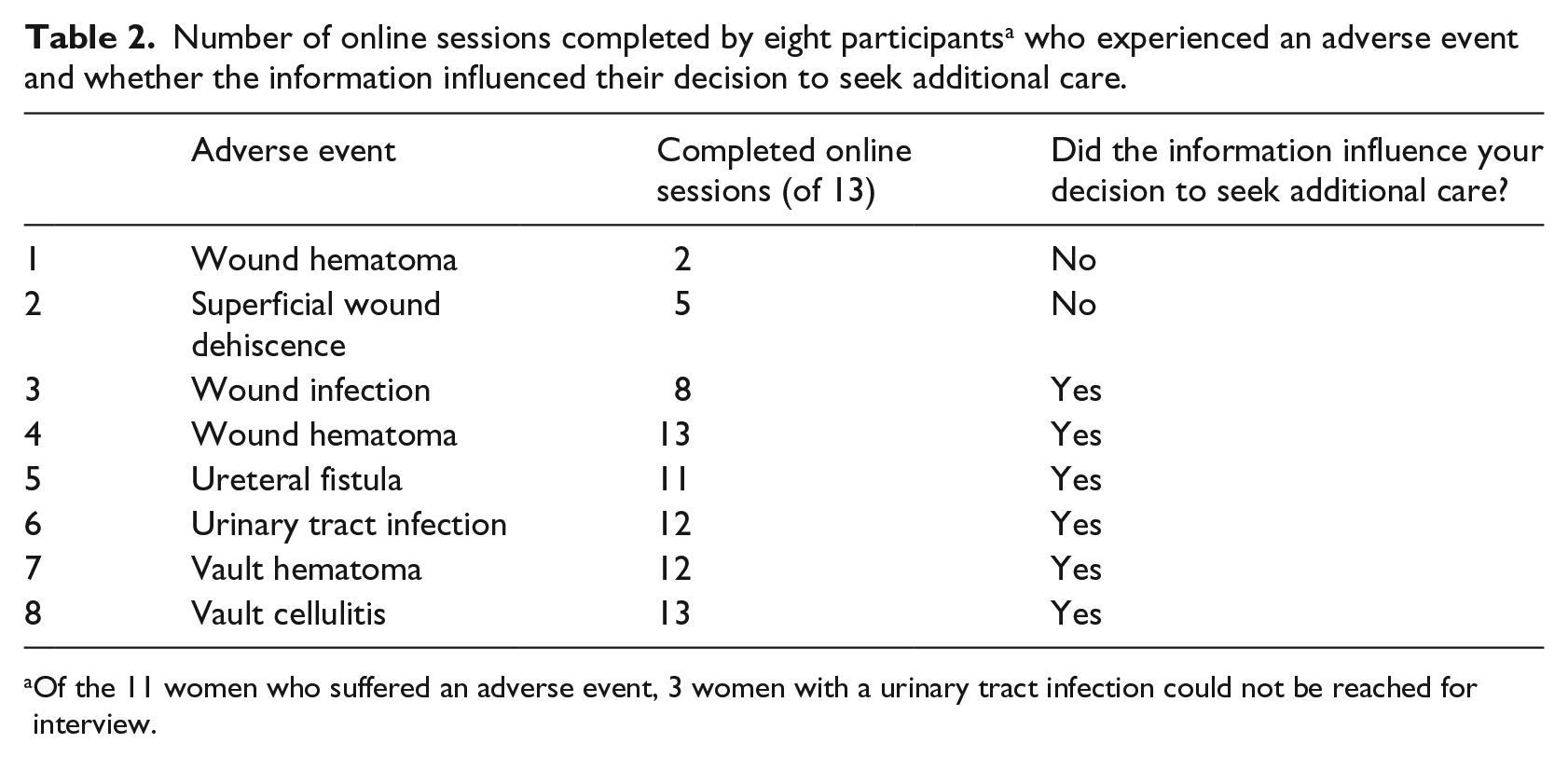
Of the 11 women who suffered an adverse event, 3 women with a urinary tract infection could not be reached for interview.
Two participants who experienced an adverse event, rows 1 and 2 in Table 2, felt that the website did not affect their treatment decision, due to the symptoms being obvious or occurring at a regularly scheduled follow-up appointment with their own physician. The other six women who experienced an adverse event used the applications regularly and to guide their decision making about whether to seek additional care and where to go for this care. Two participants with an adverse event, rows 3 and 4 in Table 2, felt the website confirmed and reassured their own decision to seek help, with the second woman stating it hastened her decision. One participant experienced a ureteral fistula, row 5. After following the website information and presenting to an Emergency Department, she had an initial misdiagnosis of acute cholecystitis. She felt her uterovaginal fistula might have been diagnosed and treated sooner if the website had provided even more information on what her symptoms meant so that she could have communicated this to her health care providers. Other comments from these eight women include that the web application was helpful, easy to use, clear, and reassuring. They also noted the website was credible due to it coming from their health care centers and providers.
Barriers to use
Six of the 31 women (19%) did not use the web applications regularly (completed <50% of the sessions). To understand why women did not use the applications, we approached all six women for interviews and four agreed. Two of the women interviewed had also suffered an adverse event (Table 2, first two entries). For three of the women, their reasons for not using the online applications were related to issues of access. Two women reported that, because their computers were set up on a different floor than where they spent the bulk of their recovery time, it was difficult and/or painful to get to their computer. One woman experienced such debilitating pain (from her wound hematoma) that she could not get to her computer to complete the applications. The fourth woman reported being too overwhelmed by the demands of single parenting and postoperative recovery to be able to use the applications consistently.
Patient overall experience
The website’s post-surgery questionnaire recorded patients’ opinions about their experience during recovery, their satisfaction with their surgery outcome, and usefulness of the web applications. Women who experienced an adverse event tended to give higher scores for the questionnaire items assessing the helpfulness and usefulness of the web applications (Table 3). Fisher’s exact test was performed on a comparison of Agreement (⩾4) versus No Agreement (<4) in the two groups. No significant differences were found as all p values were above 0.19 on this small sample size.
Satisfaction with the applications for women who suffered and did not suffer an adverse event (AE), on a 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree).
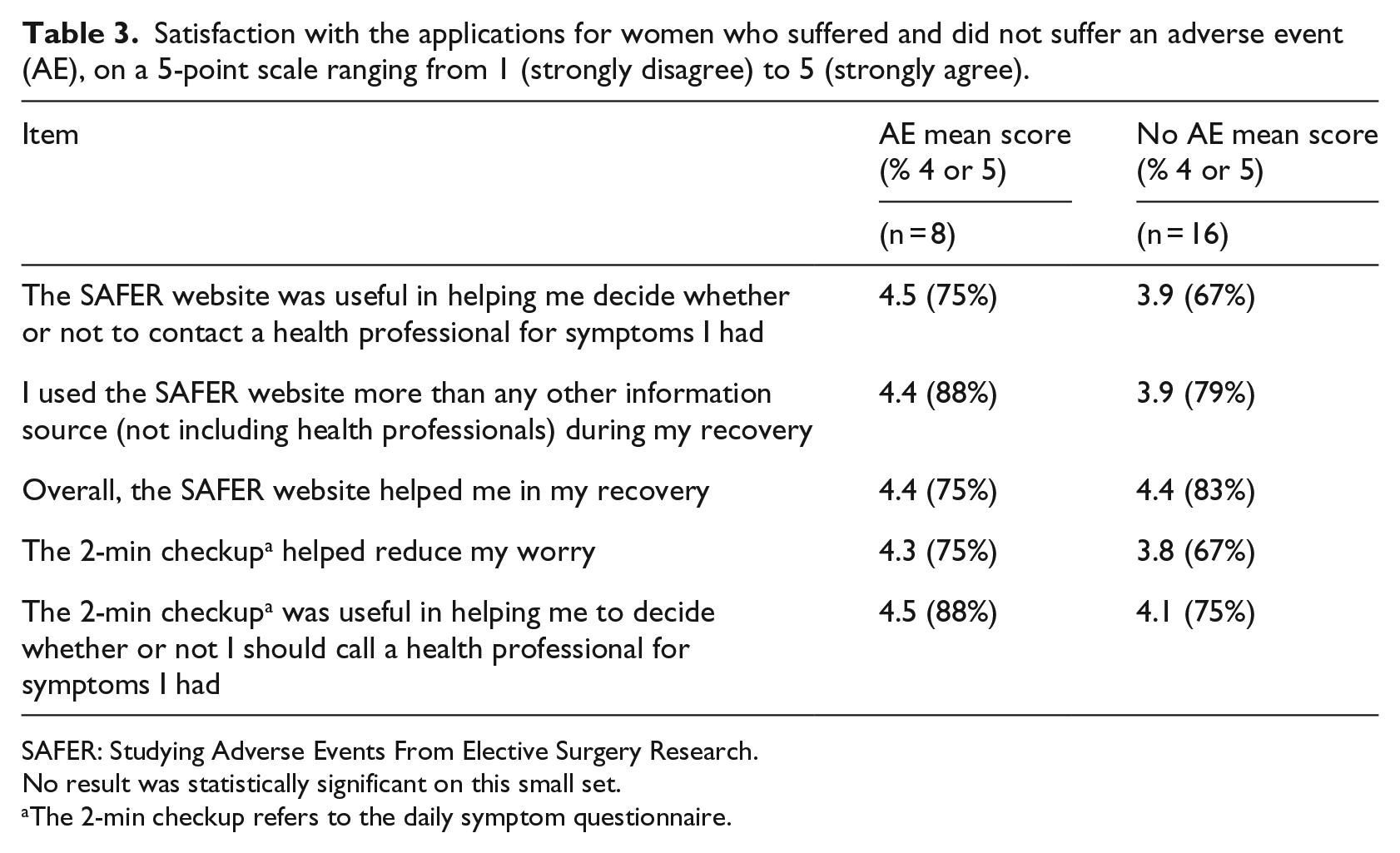
SAFER: Studying Adverse Events From Elective Surgery Research.
No result was statistically significant on this small set.
The 2-min checkup refers to the daily symptom questionnaire.
Discussion
The SAFER applications were designed to provide timely and accurate information to patients recovering from hysterectomy. This information helped educate patients about normal and abnormal symptoms as well as guide their decision making around accessing health care when experiencing these symptoms. In this report, we focus on the experiences of women who experienced adverse events in our small population, with common ones including infections and wound complications. Although these complications may not have progressed into something more serious, early intervention is critical for successful management. Early, outpatient management of wound complications and infections is less costly to the health care system and patients than unmanaged complications that may progress and require acute care. To this end, the web applications prompted and informed patients on every sign in to remind them about concerning symptoms and, importantly, informing them when and where to go if they had these symptoms.
Mobile app to address barriers to use
A primary goal of this study was to test the feasibility of web-based self-care applications for patients recovering from surgery, complementing standard pre- and post-operative teaching. More than 80 percent of women used the applications regularly, that is, more than half (7) of recommended sign-ins (13). This high usage rate suggests that self-care applications are feasible as a method for helping patients care for themselves at home after surgery. Women who did not use the applications regularly were usually constrained by access to a computer. A recently reported comparison of effectiveness of mobile versus traditional monitoring for weight-loss programs confirms that mobile device versions could be an effective means to increase compliance in some groups. 20 In 2010, 78 percent of Canadian households had a mobile phone, an increasing trend. 21 Data from this small study suggest that a mobile option may help both with physical access and time restrictions by allowing the applications and questionnaires to be completed anywhere. A mobile phone option may also give greater access to those who live in rural areas without Internet access over land lines but who do have mobile phone coverage. For maximizing compliance with self-management system protocols, easy access from many locations, including bedside, is key. To this end, we have created a mobile-optimized version of the self-care applications which is ready for trial with a larger sample size.
High socioeconomics of small sample size
Most of the participants were relatively young, well educated, and Internet savvy. Selection bias may have occurred in that only women with these characteristics were enrolled or only women with these characteristics had the ability to complete the study because they were required to have home Internet access and familiarity with using the Internet. Due to the social determinants of health, older and low-socioeconomic groups may be at slightly greater risk of adverse outcomes post-surgery. However, a majority of Canadians aged 35–54 (87.8%) and 55–64 (71.1%), as well as low-income (76.2%) Canadians, use the Internet regularly. 22 There is also a demand for relevant, accurate, online health care information among the Canadian female population—74 percent of Canadian female Internet users search for medical or health-related information. 23 Web-based self-care applications can fill this demand by providing patients with reliable, surgery-specific information, reiterating and emphasizing the information provided by their nurses and physicians when patients need it most, namely when they are at home, recovering from surgery, and having problems. The applications also fill the gap after hours and at night when women may feel most vulnerable, have additional questions, and fewer health care professionals are available.
Adverse event rates
Even with the small sample size and the relatively high socioeconomic status of the subjects enrolled in this study, adverse events after abdominal hysterectomy in these subjects were common. Over one-third of participants in this small study experienced an adverse event. Approximately half of these adverse events were infection-related, most commonly urinary tract infections. Large prospective audits and studies with specific measures and questionnaires to capture adverse events unique to hysterectomy also demonstrate adverse event rates of 26.4 and 19.2 percent after abdominal hysterectomy, with most of these adverse events being wound and infection-related.5,6 With approximately one-fifth to one-third of patients experiencing adverse events after abdominal hysterectomy, the delivery of timely, accurate information about symptoms of possible adverse events and where to go for treatment are needed. Since the application is tailored to the specific day following surgery, the information may be better received and understood because it appears at a relevant time for women seeking the information.
Empowerment of patients
Several aspects of the SAFER website align with previously identified components of patient empowerment. 24 Although the original conception and design of SAFER predates this article (i.e. it was not followed as part of our methods), the daily tip and background information improves communication skills by increasing knowledge of specific questions to pose to health care providers. The 2-min checkup increases knowledge and insight regarding abnormal and normal symptoms, increasing education and health literacy. The daily tip featuring normal and abnormal recovery information specific to the patient’s day of recovery gives information about the patient’s personal health situation. This advice plus providing daily goals for the patient to strive for, helps with supporting self-care. The 2-min checkup gives participants specific guidelines of when and where to seek care for flagged symptoms. A final component of patient empowerment identified by the article could be part of future work, namely the encouragement and enabling of having patients communicate with one another. These features strive to help empower patients to care for themselves more effectively.
Additional information and coordination may be required
Although the web applications were helpful for most of the women who experienced an adverse event, one subject who followed the website advice and sought care for her symptoms at local emergency departments still experienced a delay in diagnosis and management of her ureteric injury. This delay was partly from the challenge of diagnosing a small hole in her ureter that presented with non-specific symptoms. There is a need, beyond the currently studied web tool, to co-ordinate surgery-specific self-care information with emergency room physicians and family physicians so that any patients who continue to present to emergency departments or family physicians’ offices with ongoing symptoms are referred to appropriate surgical care teams. These teams are experienced in the types of adverse events specific to hysterectomy, which may result in quicker diagnosis, management, and resolution of those adverse events.
Conclusion
Adverse events after abdominal hysterectomy are common. At present, they are not optimally screened and cared for in the Canadian Healthcare system. Self-care applications that are completed regularly while recovering at home after surgery are a feasible method to further educate patients about when and where to go for appropriate evaluation and care beyond the information provided by physicians and nurses at the hospital.
More work still needs to be done with implementation and evaluation—the development of a mobile-optimized app should help with increasing accessibility for recovering patients, which was identified as a barrier to use. Moving from the pilot study stage into a larger trial will allow us to quantify the effect of these applications on adverse event outcomes with statistical support. As we integrate these and other similar applications into health care, we hope to empower patients, decrease adverse event severity, optimize surgical outcomes, and improve the overall health of our population.
Footnotes
Appendix 1
Participants were asked to answer “yes” or “no” for the questions below on days 4–10, 13, 16, 20, 23, 27, and 30 after surgery. If they gave a positive reply, they were provided information about the possible significance of the symptom and where to go for assessment. Participants were also given the option of requesting more information about the symptom, without giving a positive reply.
Acknowledgements
The authors would like to thank Nicola Sweeney for her assistance with enrolling subjects and collecting data and Melanie Jollymore for her assistance with compiling and revising web-application content for patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Medical Protective Association Competitive Grant Program, the Canadian Foundation for Innovation, the IWK Research Foundation, and the Nova Scotia Health Research Foundation.