
Abstract
Objective
This study is a control group intervention study to determine the effect of web-based education on diabetes self-management in individuals with type 2 diabetes.
Methods
The study was conducted in the Training and Research Hospital Diabetes Education Unit of Hitit University. The study was completed with 75 people (intervention 38, control 37). The data were obtained in the web site through patient identification form, self-management perception scale in diabetes, diabetes attitude, self-care scale and HbA1c, HDL, LDL values were followed by providing training and counseling. The values followed were viewed at the third and sixth months. Written permission was obtained from ethics committee and participants. The data of the study were evaluated with number, percentage, mean, pearson chi-square, independent t-test, repetitive analysis and variance analysis.
Results
Statistically significant decrease in HbA1c and LDL values, diabetes self-management scale, diabetes attitude scale and self-care scale scores were found to be significantly different between the intervention and control groups.
Conclusion
Web-based education and follow-up studies are effective in decreasing HbA1c values in increasing diabetes self-management skills of individuals with type 2 diabetes. It is recommended to use as a complementary tool in health care services for type 2 diabetes management.
Introduction
The person diagnosed in chronic diseases should be included in a training program for coping with the chronic disease. In the literature, data are showing that the education given with the aim of improving individual self-care skills after diagnosis has more positive social and psychological effects in reducing acute or chronic complications.1–3
Although patient education styles are changing, the positive benefits of technology have begun to be integrated into education methods.4,5 One of these training methods is web-based training. In the web-based education process, people can become qualified and competent by accessing educational materials whenever they want and wherever they are convenient. In the literature, it has been shown that the use of technological methods such as the internet, text message and smart phone alone or in combination have a positive effect on reaching the glycemic control goals of individuals with diabetes and increasing their diabetes self-management skills.6,7
With this training method, which can be followed interactively with consultants, problems can be solved quickly as a result of communicating with health professionals in a shorter time. It can also provide cost-effective support by reducing acute or chronic complications related to type 2 diabetes.6–8
Considering that type 2 diabetes is a disease with acute and chronic complications, 9 it is thought that the positive effect of education programs that provide effective and constantly education opportunities for people with this diagnosis cannot be denied. The effect of improving self-care skills in the management of diabetes on disease morbidity and mortality cannot be ignored.6,7,9
In recent years, there has been a need for various interventions that are effective, low-cost, understandable and usable by the society as tools to increase diabetes self-management skills. Nurses, who have many roles and responsibilities in maintaining and improving the health of the individual, such as providing care, education, counseling, and decision-making, can ensure that individuals with diabetes receive low-cost, effective and high-quality care with web-based education application.10–12
In this study, which was carried out within the scope of this information, it was aimed to evaluate the effect of web-based education on diabetes self-management, attitude and self-care skills of individuals with diabetes. It is thought that the results obtained from this study will contribute to facilitating the education and follow-up of individuals with diabetes who have problems in accessing health services, and to provide an effective nursing service.
Methods
This study was a non-randomized experimental study and was conducted to determine the effect of web-based type 2 diabetes education on diabetes self-management in individuals with diabetes.
The study was carried out between 1 March and 15 September 2018 in Endocrine Clinic at a University Hospital. The sample of the study included who was diagnosed with type 2 diabetes in the last year [February 2016- February 2017], was between the ages of 40 and 64, had HbA1c > % 7, received basic diabetes education within 6 months, received oral antidiabetic and/or insulin therapy, could use computer and internet, and had at least Individuals who are primary school graduates and can speak Turkish and have blood glucose measurement tools at home were recruited [N = 416].
Individuals with retinopathy, neuropathy and nephropathy, who use insulin pumps, who have chronic diseases other than diabetes, who are pregnant, and who have mental and communication problems were not included in the study. In addition, individuals who wanted to leave the study moved to another city during the follow-up period, and died during the follow-up period were excluded from the study.
Diabetes Education Unit Electronic Patient Information System was used to determine the sample of the study. It has been determined that 416 individuals between the ages of 40 and 64 with the diagnosis of type 2 diabetes were registered in this system in the last year. According to the exclusion criteria in the sample; of 416 diabetic individuals, 56 were diagnosed with retinopathy, 69 with nephropathy, 28 with neuropathy, 66 with hypertension, cancer, asthma, chronic obstructive pulmonary disease, and hypo-hyperthyroidism. In addition, it was determined that 24 people did not have a registered phone number.
After screening according to the sample exclusion criteria, individuals [n = 173] were called via telephone. It was determined that 21 of them did not have internet, 10 of them could not use the internet, 11 of them did not want to participate in the study, 8 of them were illiterate and 6 of them could not reach/work via phone numbers. As a result of these evaluations, it was determined that 117 individuals with diabetes were suitable for sample selection. The sample of the study was determined by a power analysis based on a two-unit decrease in the HbA1c variable in a similar study, 13 taking into account a 5% margin of error and a 90% confidence interval. According to the power analysis, 68 people were sufficient for the sample of the study. However, to increase the power of the research and to consider the individuals who had to leave the study, 80 people were included in the study. Then, individuals with diabetes who met the sampling criteria were assigned as the intervention and control groups by using the Power and Sample Size menu in the Minitab 15 program in the computer environment, ensuring homogeneity in terms of age, gender and HbA1c levels [Figure 1]. After the group assignment was structured, groups of 40 people were assigned as the intervention [n = 40] and control [n = 40] groups.

Consort flow table.
In the second stage of the study, two participants in the intervention group wanted to leave the study, and three people in the control group did not come to the control appointment. Therefore, the study was completed with n = 38 people in the intervention group and n = 37 people in the control group. As a result of the posterior power analysis, the power of this study was found to be 94% with an effect size of 0.90 and a margin of error of 5% [Figure 1].
Written permission was obtained from the Provincial Public Health Directorate, the individuals who accepted the research and the ethics committee.
The data obtained from the study were evaluated using the SPSS version 20 program. The conformity of the data to the normal distribution was examined using the Skewness-Kurtosis, Histogram, Box-Plot test, Normal Q-Q graph and Kolmogorov-Smirnov [p = 0.200] test together. The Cronbach's alpha coefficient was used to evaluate the reliability of the Diabetes Self-Management Perception Scale, the Diabetes Attitude Scale, and the Self-Care Agency Scale. Independent samples t-test was used to evaluate the homogeneity of the intervention and control groups in terms of number, percentage and numerical characteristics, and Pearson chi-square analysis was used for categorical characteristics. Independent samples t-test was used to compare the mean scores between groups in the intervention and control groups, and analysis of variance for repeated measurements was used to compare the mean scores within the group. Post-hoc Bonferroni test was used to determine within-group differences. P < 0.05 was taken as statistical significance level.
Data collection tools
Individual Identification Form [IIF]: One of the data collection tool IIF was created by making use of the relevant literature.7,8,10 In this form: There are nine questions about age, gender, education level, marital status, treatment for diabetes, regular use of medications, regular exercise, compliance with nutrition program and perception of health status.
The Perceived Diabetes Self-Management Scale [PDSMS] was developed by Wallston et al. 14 The validity and reliability study of the Turkish PDSMS was performed by Çevik. 15
Diabetes Attitude Scale [DAS]: It was used to evaluate individuals’ attitudes towards diabetes. This scale was developed by the National Diabetes Commission in the USA. The validity and reliability study for its use in our country was performed by Özcan in 1999. 16
Self-Care Agency Scale SCAS): Consisting of 43 items, the scale was developed by Kearney and Fleicher 17 to measure the ability of a person to look after him/herself or in other words his/her self-care agency. 17 The scale was adapted by Nahcivan in 1993 for Turkish and reduced to 35 items. 18
Creating the web page
Website used by the intervention group
The training and follow-up of the intervention group was carried out through the website “www.diyabetizle.com”, which was established as a diabetes follow-up site.
The configuration process of the diabetes follow-up site:
Technical support was received from Hitit University Computer Engineering Unit, based on the principles developed for worldwide accreditation by Health on The Net Foundation [HON], which ethically examines health-related websites in the creation of the web page.
This Web page was run on two different panels, the admin panel [researcher] and the user panel [intervention group].
The admin panel was controlled by the researcher. The administrator was responsible for the technical management of the website, content editing, participant information registration/tracking, diabetes education tracking, blood values monitoring and communication with the participants.
Intervention Group User Panel;
This panel consists of four separate sub-panels. The sub-panel titles were classified as patient education, biological value input, data collection tools, question-answer, and feedback.
Patient education sub-panel
This sub-panel included visual videos and written materials in which the participant learned about diabetes and could facilitate diabetes management. Educational materials and videos to be used in the study were prepared by the researcher in line with the literature and guideline of the Turkish Society of Endocrinology and Metabolism5,19,20 and expert opinions were obtained from five faculty members specialized in Internal Medicine Nursing, Public Health Nursing and Diabetes Nursing. The website creation process was completed by making adjustments in line with the comments received.
Subject headings; basic information about diabetes (duration = 10’ 32'’), diabetes and nutrition (duration = 14’ 14'’), treatment process in diabetes (oral and subcutaneous drug use; duration = 35’ 47'’), diabetes and exercise (duration = 8’ 31'’), biological control of diabetes (duration = 10’ 23'’), foot health in individuals with diabetes (duration = 10’ 54'’), diabetes and special conditions (travel, invitations, fasting/Ramadan; duration) = 11’ 53'’), what to do in case of hypoglycemia (duration = 3’ 47'’), blood glycemia measurement method (duration = 10’ 55'’), and insulin administration technique (duration = 10’ 15'’).
Biological value input
Preprandial and postprandial blood glucose, HbA1c, LDL, HDL, triglyceride and blood pressure values were monitored in this sub-panel. During the follow-up period, preprandial and postprandial blood glycemia monitoring was made according to the diabetes guideline of the Turkish Society of Endocrinology and Metabolism.
19
In patients using only oral antidiabetic, glycemia monitoring was arranged as 3 times preprandial and 1 time postprandial in a week. It was performed 3 times a day preprandial and 1 time postprandial in those using basal-bolus insulin therapy. In addition, measurements were made at bedtime once a week (on Mondays) and once a month (on the 15th day of each month) between 02:00 and 04:00. None of the participants used an insulin pump. Again, according to the same guideline, within the scope of glycemic target values, the preprandial glycemia cut-off point was 130 mg/dL and the postprandial glycemic cut-off point was 160 mg/dL.
19
Other biological data were monitored at baseline, 3rd month and 6th month in three monthly periods. A face-to-face training and written user guide were given to the intervention group by the researcher about making the biological value entries. The cut-off values of the values in the biological value entry sub-panel were defined and warning messages were sent to the administrator's e-mail when there were deviations from the determined values. When there were problems in the data entry of the individuals included in the intervention group, the individuals were called by phone and the data entry was reminded or the reasons for not entering were learned. These reminders and follow-ups were continued until the 3rd and 6th months. Thus, the continuity of data entry was ensured.
Data collection tools Question-answer and feedback
This sub-panel included IIF, PDSMS, DAS and SCAS. Individual Identification Form was initially active once. Other scale tools were active three times in quarterly periods.
The purpose of this sub-panel was to facilitate communication between the intervention group and the administrator.
Intervention
Intervention initiation process
Stages of the Study.

Before starting the three-stage evaluation, on website using training was given to the intervention group between February 27 and March 2, 2018. The individuals in the intervention group included in the study were divided into groups of 10. The seminar room belonging to the Nursing Department of Hitit University was used as the training area for the ease of transportation of the participants. The participants were given web site usage training in the intervention group, with two classes consisting of one class hour of 45 min by the researcher. In the first lesson of this training content; information was given about the purpose of using the web-based system, its benefits, and how to use it. During the second lesson, the use of training videos on the website, pre-postprandial blood glucose data entry process, how to use the blood values entry screen, blood pressure monitoring, how to record on the nutrition and exercise screens were detailed. After the training, the website registration of the intervention group participants was done by the researcher.
Initial assessment: T0
First stage for interventin group; website usage was launched on 6 March 2018. HbA1c, LDL, HDL, triglyceride and blood pressure values of the initial measurement of the intervention group, as well as IIF, PDSMS, DAS and SCAS scales were evaluated on this date. Written and visual training materials were started after this date.
Control group participants were asked to have their baseline pre-postprandial blood glucose, HbA1c, LDL, HDL, triglyceride and blood pressure values checked before coming to the appointment via phone call. In the first stage of the study for the control group; initial blood parameters, IIF, PDSMS, DAS and SCAS were evaluated. This evaluation was recorded by the researcher in the Diabetes Education Unit between 6 and 9 March 2018 by interviewing the control group participants face to face. No training or consultancy initiatives were made. In the control group, an appointment was made by calling only by phone to collect the data for the study.
Second assessment: T1
During the first trimester for the intervention group; pre-postprandial blood glucose and blood pressure values were completed via the website. During the duration of the study; reading and watching the training materials of the intervention group was monitored by ticking the boxes placed on the training screen. In the first trimester of the application, the training videos were watched 730 times through the website. Each training video has been watched at least once. Written training materials were read at least once by the participants.
When the participants recorded their blood glycemia values on the website, an e-mail warning message was sent to the system administrator when a result exceeding the cut-off values was detected. Upon the warning messages sent to the system administrator, the factor(s) that caused the warning message to be sent were queried by communicating via the feedback sub-panel and/or telephone connection. As a result of this questioning, the factor that could cause the participant's blood glycemia value to be higher than the target values was determined, and she/he was ensured to watch and read the training materials related to the subject at least once again.
At the end of the first trimester, the HbA1c, cholesterol panel results of the intervention group were requested. Evaluation of PDSMS, DAS and SCAS scales was done via the website by the participants on 5–6 June 2018 (T1). During the second assessment of the study, there were two people from the intervention group who did not continue the study.
At the end of the first trimester for control group data were collected through face-to-face interviews between 5 and 8 June 2018 (T1). At the end second assesment of the study, there were three people from the control group who did not continue the study. An appointment was made for the control group for 11–14 September 2018. One week before the appointment, they were reminded by phone and asked to have their blood laboratory values and blood pressure values measured. No training or consultancy initiatives were made.
Third assessment: T2
During the second trimester for the intervention group, pre-postprandial blood glucose and blood pressure values of the intervention group were monitored as in the first trimester. Differently in this period, the training videos were watched 679 times, and each video was watched at least once and the written training materials were read at least once.
At the end of the second trimester, the HbA1c, cholesterol panel results of the intervention group were requested. Evaluation of PDSMS, DAS and SCAS scales was done via the website by the participants on 11–12 September 2018 (T2).
At the end of the second trimester, control group data were collected through face-to-face interviews between 11 and 14 September 2018 (T2). One week before the appointment, they were reminded by phone and asked to have their blood laboratory values and blood pressure values measured. No training or consultancy initiatives were made.
Results
According to the data obtained from the study, there was no statistically significant difference between the groups according to the descriptive characteristics of the intervention and control groups (p > 0.05). Data on socio-demographic characteristics are given in Table 2.
Distribution of descriptive characteristics of the intervention and control group (n:75).

Intragroup and intergroup statistical analysis information regarding the PDSMS, DAS, SCAS scale mean scores of the intervention and control groups are given in Table 3, Table 4, and Table 5.
Intragroup and intergroup comparison of the PDSMS score averages of the intervention and control groups according to the follow-up process (n = 75).
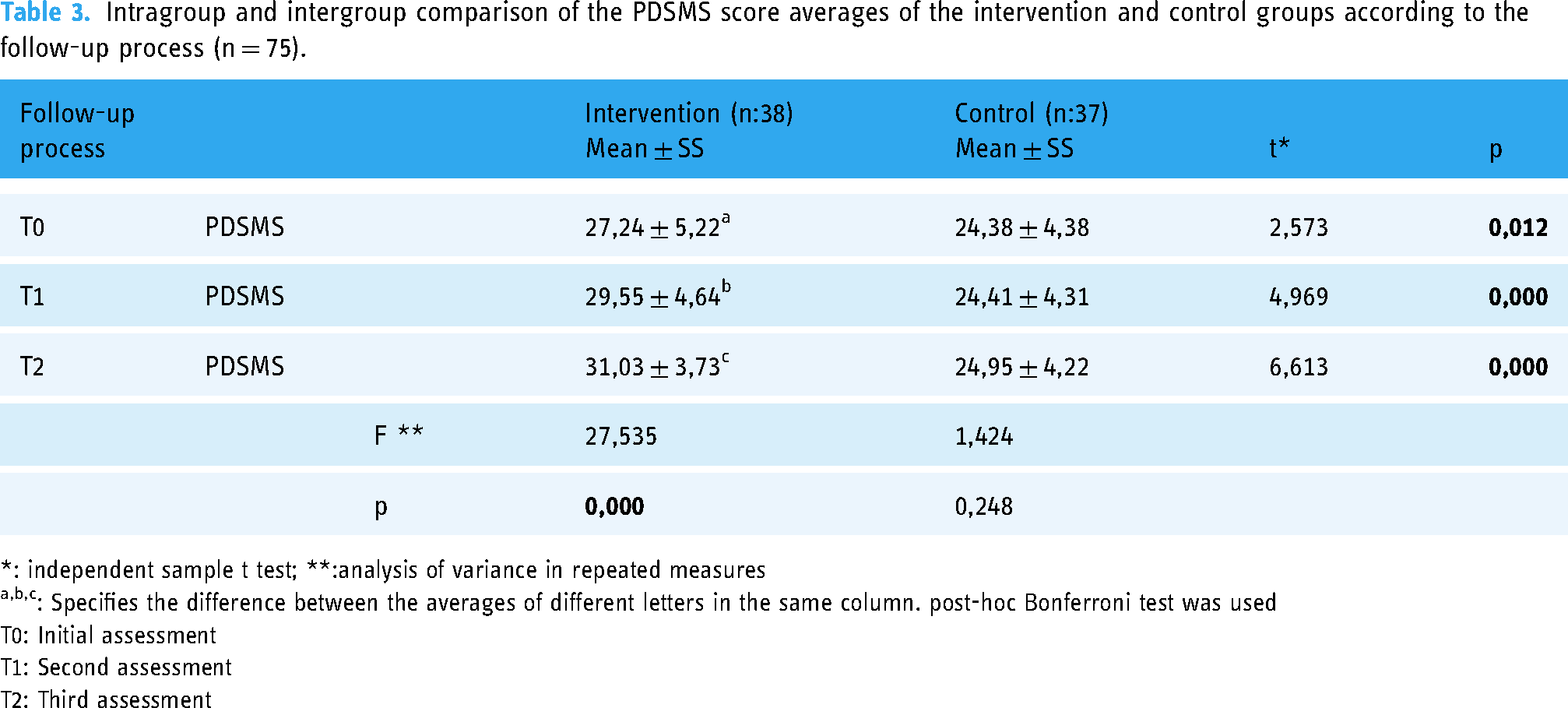
*: independent sample t test; **:analysis of variance in repeated measures
: Specifies the difference between the averages of different letters in the same column. post-hoc Bonferroni test was used
T0: Initial assessment
T1: Second assessment
T2: Third assessment
Intragroup and intergroup comparison of the DAS score averages of the intervention and control groups according to the follow-up process (n = 75).

*: independent sample t test; **:analysis of variance in repeated measures
: Specifies the difference between the averages of different letters in the same column. post-hoc Bonferroni test was used
T0: Initial assessment
T1: Second assessment
T2: Third assessment
Intragroup and intergroup comparison of the SCAS score averages of the intervention and control groups according to the follow-up process (n = 75).

*: independent sample t test; **:analysis of variance in repeated measures
: Specifies the difference between the averages of different letters in the same column. post-hoc Bonferroni test was used
T0: Initial assessment
T1: Second assessment
T2: Third assessment
Table 6 shows the comparison of the intragroup and intergroup of the intervention and control groups HbA1c, HDL, and LDL meansaccording to the T0, T1, and T2.
Intragroup and intergroup comparison of HbA1c, HDL and LDL variables of the intervention and control groups according to the measurement times (n = 75).

*: independent sample t test; **:analysis of variance in repeated measures
: Specifies the difference between the averages of different letters in the same column. post-hoc Bonferroni test was used
T0: Initial measurement
T1: Second measurement
T2: Third measurement
Table 7 shows comparison of the intervention and control groups’ declarations about diabetes management at T0, T1, and T2 assessment times.
Comparison of the intervention and control groups’ declarations about diabetes management at T0, T1 and T2 assessment times (n:75).

*: Oral Antidiabetic Drug
T0: Initial assessment
T1: Second assessment
T2: Third assessment
Discussion and conclusion
Discussion
The process of managing diabetes well is difficult and complex. This approach promotes the self-management abilities of people with diabetes in controlling the disease and includes adjustments to lifestyle, achieving glycemic targets for diabetes control, learning problem-solving techniques, and minimizing diabetes-related risk factors. According to the findings of both national and international studies, patients’ knowledge of managing their diabetes is not at the desired level. As a result, difficulties are encountered in achieving goal values for glycemic control factors as well as lifestyle adjustments.21–23 Due to untreated diabetes, morbidity and mortality rates are rising globally as a result.9,24 In this study, a statistically significant difference was found between the intervention and control groups in terms of regular use of medications, regular exercise, compliance with the nutrition program and perception of health status in relation to diabetes management. There was no significant difference between the groups according to the diabetes treatment used by the intervention and control groups. These findings show that web-based education given to the intervention group positively affects diabetes management in individuals with diabetes. The reason for this positive development in the intervention group is thought to be the effective participation of the participants in the diabetes management process and the increase in their awareness through web-based training.
It is known that chronic diseases affect the lifestyle, quality of life, social and work life, and mental states of individuals. Therefore, due to the fact that type 2 diabetes is a chronic disease, the need for multidimensional management of the disease emerges.21,25–27 In the literature, the importance of self-management support in the management of diabetes is emphasized.25,28–30 In studies examining the effects of web-based education given to individuals with diabetes on lifestyle changes in individuals with diabetes, it is reported that there is an average of 12 weeks of improvement.6,13 After the intervention in this study, an undeniable improvement was found in the use of medications, regular exercise and perception of health status in three months, and in compliance with the nutrition program in 6 months. In a study by Ramadas et al. 8 in which they examined the effect of web-based diet intervention on health perception and glycemic control in individuals with diabetes, they found a significant improvement in the ability of individuals to comply with the diet program in a 6-month period. 8 In this study also shows parallelism with the literature findings showing the positive effects of education programs applied on individuals with diabetes on diabetes management skills.
It has been reported in the literature that motomod interview techniques or training given in plain text do not make a significant difference in glycemic control variables in the long time. 31 However, it has been reported that the use of internet interface programs and web-based training programs provide diabetes self-management skills in the long run.31–33 Jaipakdee et al. 32 reported a significant improvement in patients’ glycemic control variables, self-management and quality of life in their randomized controlled study in which they examined the effectiveness of computer-assisted education program conducted by nurses. 32 In this study findings are also consistent with the literature findings, and a statistically significant increase was found when the diabetes self-management perception scale T0 score average of the intervention group was compared with the T2 score average, but no difference was found in the control group. This result is thought to be due to the fact that the web-based type 2 diabetes education support given to individuals with diabetes supports the self-management of the patients by ensuring the active participation of the participants in the diabetes management process.
It is reported in the literature that individuals with a positive attitude towards diabetes have better glycemic variables and self-care skills, sufficient knowledge about diabetes.34,35 Chawla et al. 33 reported that a significant difference was observed between the intervention and control groups in a randomized controlled study in which they examined the effect of health education on diabetes-related knowledge, attitude, practice, and glycemic control in type 2 diabetes patients. 33 In this study, it was found that the diabetes attitude mean score was statistically significant according to the intervention group follow-up times. It is thought that the web-based type 2 diabetes education given to the participants improves the diabetes attitudes of the participants by increasing their knowledge about diabetes management and supporting their self-confidence, and as a result, HbA1c, HDL, and LDL approach the target values. In the experimental study conducted by Okuroğlu and Alpar, 36 it was reported that the diabetes attitude scale mean scores of the intervention group increased, but there was no significant difference. 36 Despite this study conducted in our country, the fact that the web-based type 2 diabetes education used in this study positively improved the attitude scale scores of individuals with diabetes and created a significant difference compared to the diabetes attitude scale score averages of the control group shows that a pleasing result has been reached.
Since the nature of diabetes makes it difficult to cope with the disease, it becomes even more difficult for individuals with diabetes to acquire self-care skills. 34 However, it has been reported that an increase in self-care skills is also observed in a diabetic with advanced diabetes self-management and attitude.34,35 In the literature, it is stated that in the experimental studies examining the effectiveness of internet/web-based diabetes education, statistically positive developments were detected in the self-care skills of individuals with diabetes.37,38 In the web-based randomized controlled studies conducted by Pacaud et al., 31 it was reported that the group who received educational support via the website had improved diabetes knowledge, self-care behaviors, and decreased HbA1c values. 31 In this study, in which results consistent with the literature were reached, it is thought that the statistically significant increase in the self-care power scale mean scores of the intervention group participants is due to the effectiveness of the web-based type 2 diabetes education applied.
In the literature, HbA1c, HDL, and LDL values are specified in diabetes diagnosis, treatment, and follow-up guidelines as variables that should be followed for the control of type 2 diabetes.33,39 These variables have taken an important place in controlling the risk factors of diabetes and diabetes-related complications. It has been reported in the literature that keeping HbA1c, HDL, and LDL values within the target value ranges reduces the risk of diabetes-related complications.10,28 In this study, a statistically significant difference was found between the T0 and T2 measurements of the intervention HbA1c, HDL, and LDL variables. In the comparison of the intervention and control groups, a statistical difference was observed in all measurements of T1 and T2 in HbA1c and LDL values, and although there was an improvement in HDL value, no difference was detected. This improvement is thought to be supported by watching the “Module 2: Diabetes and Nutrition” and “Module 4: Diabetes and Exercise” videos 172 and 129 times, respectively, among the intervention group participants. In the randomized controlled studies of Hansel et al. 39 conducted to develop web-based support tools for the improvement of lifestyle habits, significant differences were found in HbA1c value, diet, and exercise habits between the groups, and no statistical significance was observed in HDL and LDL values. 39
Ramadas et al. 8 reported that they found a significant decrease between baseline and 12th month HbA1c values in their study to examine the effect of web-based diet education on HbA1c, dietary knowledge, attitudes, and behaviors in individuals with type 2 diabetes. 8 In addition to these results, a statistically significant difference was found between the intervention and control groups in terms of regular use of medications, regular exercise, compliance with the nutrition program and perception of health status in relation to diabetes management of the participants in this study. These findings show that web-based type 2 diabetes education given to the intervention group positively affects diabetes management in individuals with diabetes. In line with these results, which were found to be compatible with the literature, it was determined that the web-based training given to individuals with diabetes strengthened the glycemic control values of the intervention group participants in this study. It can be said that the web-based education given to the intervention group in this study helped to control blood lipid and glucose levels by increasing the compliance of the patients to the nutrition and exercise program from lifestyle changes.
Conclusion
As a result of this study, it was observed that web-based type 2 diabetes education had an effect on diabetes self-management and glycemic control and it provided a 2.32 ± 0.65% decrease in HbA1c value and a statistically significant increase in diabetes self-management perception scale mean scores. In line with these positive results, it can be said that web-based education is a method that can be used for nurses and other health professionals as an evidence-based intervention.
Practice implications
In line with the results obtained from the study, the following suggestions were made:
Educating individuals with diabetes on diabetes self-management by health professionals Supporting the continuous education of individuals with diabetes with visual education materials Creating support environments by telephone in web-based education applications Integration of increasing technological infrastructure formations into health care methods Providing information, support and opportunities to the nurse group about web-based education for individuals with diabetes. Development of nursing interventions using the evidence of nurses’ web-based education studies on diabetes. Providing and disseminating web-supported professional counseling services that individuals with diabetes can access at any time. Conducting qualitative studies on the opinions of individuals with diabetes on the use of web-based monitoring sites.
Footnotes
Acknowledgements
No financial disclosure was declared by the authors. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors for the web site setup and study. No conflicts of interest was declared by the authors. Informed consent was obtained from all individual participants included in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Limitations of the study
The most important limitation of this study is that it works with a small sample group. Therefore, it cannot be generalized to the general population.