
Abstract
Physicians increasingly use medical applications to facilitate clinical information management. The respective effect on clinical communication and quality of healthcare provision has not been studied in the Austrian context so far. Thus, the current cross-sectional online study analyzed prevalent medical applications use and views on clinical communication competence in everyday medical practice among Austrian physicians (n = 151) and validated the survey tool. More than half of the participants used medical applications in daily clinical practice. The top three benefits of medical applications use were higher quality of healthcare, location-independent health service access, and higher efficiency in healthcare resource allocation. Moreover, study participants felt that communication competence acquired during medical studies inadequately prepared them for daily clinical practices. Medical applications use certainly affects the therapeutic alliance between patients and physician. This study supports the importance of initiating an open, constructive discussion among healthcare stakeholders and developing according to evidence-based guidelines.
Introduction
Clinical communication as detailed diagnostic–therapeutic face-to-face conversation between doctor and patient is an integrated vital therapy component. 1 The conversation lasts on average 10–15 min and is usually performed in a designated medical room. Its main purpose is to extent and to deepen the mutual understanding of the transition between health and disease processes beyond the information provided by preexisting health records. It is known since the 1980s that on average, patients speak for 18 s until the doctor interrupts them, hence limiting a bidirectional communicative flow. 2 The medical monologue and instructions are thus often overwhelming for patients who rarely have the chance to get involved in therapeutic decisions.
Clinical communication is inseparably interlinked with clinical decision-making, therapeutic options, and patient compliance. As communication is seen as purposive, communication competence can be taught in medical education and postgraduate trainings; respective tasks and skills are described in well-established consultation guidelines.1,3 For successful relationship building, interplay of different communication process tasks, for example, gathering medical information, and behavioral skills, for example, attentive listening, is required.
Due to the ongoing digitalization of every aspect of modern life, the significance of mobile digital devices in healthcare and medical information processing has vastly increased in recent years. During medical encounters, these devices especially improve doctor–patient relationship, patients’ knowledge, and quality of social healthcare. 4 Given that effective communication is important for healthcare delivery, it is critical to understand how these technologies impact communication and care processes. Smartphones are nowadays the most popular mobile communication devices, mainly replacing the former feature phones. 5 Smartphones fulfill the users’ need for a personal computer enabling personalized communication and data management. The success of smartphones was especially triggered by the implementation of built-in applications (apps), self-contained software pieces created for specific aims. 5 Medical apps thus are designed to facilitate point-of-care decisions such as drug dosing by presenting relevant information in an aggregated and easily graspable format.6,7 These apps assist in providing evidence-based, patient-centered care while decreasing error rates and face increasing popularity among healthcare professionals worldwide.8–12
Given the significant current and future investment into technology adoption and implementation in the healthcare sector, the extent to which medical apps support care and doctor–patient communication should be examined.13–20 Studying physicians’ attitudes toward medical apps and their use in clinical settings is essential to identify and address barriers to their use and to create targeted education programs. As little is known so far about the Austrian healthcare sector, we developed a German survey tool including scenario-based communication settings, which we validated using principal component analysis (PCA). In a cross-sectional online survey, we (1) assessed the prevailing frequency and predictors of medical app use among Austrian physicians. This allowed us to acquire a snapshot of current medical app use and elucidate whether socio-demographic characteristics influence respective views and practices in the study sample. Furthermore, we (2) collected views on communication competence in general and medical app use specifically to investigate how digitalization might potentially influence clinical communication.
Methods
Study population and data collection
We conducted an online cross-sectional survey among a purposive sample of Austrian physicians including general practitioners and medical specialists. Potential participants were recruited by distributing the link to the online survey via the bimonthly newsletter and the official website of the medical chamber in Austria. All medical doctors working in Austria in any healthcare area—both panel and private doctors—are members of the medical chamber and were thus eligible to participate in this validation study. Based on previously published research, we developed a German study questionnaire including three hypothetical scenarios.16–20 We performed a pre-test among participants with (n = 23) and without medical background (n = 12) to ensure general comprehensibility, face validity, and content validity and integrated the feedback of these people into the final study questionnaire.
The study was approved by the ethics committee of the Medical University of Vienna, Austria (matriculation number no. 1633977) on 21 December 2017 and conducted in accordance with the guidelines of the Declaration of Helsinki. The online survey was enabled by the web-based survey tool SoSci Survey 21 and was open and accessible from 30 January to 10 March 2018. We did not offer any incentives for participation. The survey included a cover page informing about the study aim. As participation was anonymous and voluntary, consent was explicitly obtained by survey participation. Respondents had the possibility to review and change their answers through a back button. An electronic cookie ensured single participation, and IP check prevented multiple entries from the same individual. Survey data were stored securely and were only accessible for members of the research team. Collected data were finally retrieved as a SPSS file (SPSS Inc., Chicago, IL, USA) from SoSci Survey. Only complete questionnaires filled out by Austrian German-speaking healthcare professionals were eligible for analysis.
Study questionnaire
The online questionnaire assessed socio-demographic characteristics including age (in years), gender, place of residency on region level, and status of being a statutory health insurance physician (SHIP, yes vs no).
We asked for medical app use frequency (“How often do you use medical apps during everyday clinical routine?”) to distinguish frequent medical app users (several times a day, once a day, several times a week; designated as users) from rare/nonusers (once a week, less than once a week, very rare, never; designated as nonusers).
We further assessed perceived benefits of medical app use. The multiple choice question “In your opinion, which statement applies to the use of medical apps?” offered six options as well as the options “no benefits” and “other” and a free text comment box for additional benefits.
We also asked participants to indicate their agreement (don’t agree, neutral, agree) with the following three statements: “I believe that communication skills for everyday clinical practice can be learned,” “I feel well prepared for everyday clinical practice with the communicative competence acquired during medical studies,” and “I would like to receive offers for advanced training to acquire communication competence in everyday clinical practice.”
Three distinct hypothetical scenarios assessed attitudes toward communication training (i.e. Scenario 1—Communication Training, possible response choices: yes, no, I would prefer a flexible online course, I don’t know), strategies to deal with poor native language skills of patients (i.e. Scenario 2—Language Skills), and medical information retrieval strategies during clinical practice (i.e. Scenario 3—Information Retrieval). For Scenarios 2 and 3, participants were invited to rate their approval of each of the five different action strands (don’t agree, neutral, agree).
Statistical data analysis
The online survey link was opened 1104 times, 203 individuals started the survey, and 151 participants fully completed the survey (completion rate: 13.7%). On average, full survey completion took 7.2 min (standard deviation (SD) = 1.8). We conducted all statistical analyses using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). Median splitting created a dichotomized variable for age, that is, a younger age group (44 years and younger) and an older one (older than 44 years). We descriptively summarized the collected data to present categorical data as absolute and relative frequencies and continuous data as mean and SD, and determined respective subgroup differences for age (young vs older), gender (male vs female), and SHIP (yes vs no) using Mann–Whitney U tests. Binary logistic regression analysis assessed the association between medical app use (dependent variable, use vs nonuse) and the independent variables age group, gender, SHIP, and place of residence. We used PCA with varimax rotation to analyze the factor structure of the 10 items building Scenarios 2 and 3.
Results
The average age of the participants was 45.0 years (SD = 12.0, range = 24–71 years) and 45.0 percent were males (Table 1). The minority of participants was statutory health SHIPs (27.2%) and lived in the capital Vienna compared to the rest of the country (44.3% vs 65.6%). In our sample, nearly half of the participants were designated as either medical app users (n = 78, 51.7%) or nonusers (n = 73, 48.3%). We did not detect statistically significant differences regarding gender and SHIP, but for age groups, 64.5 percent of younger versus 38.7 percent of older participants were users (p = 0.002).
Socio-demographic characteristics of the study population and binary regression analysis for medical app use.
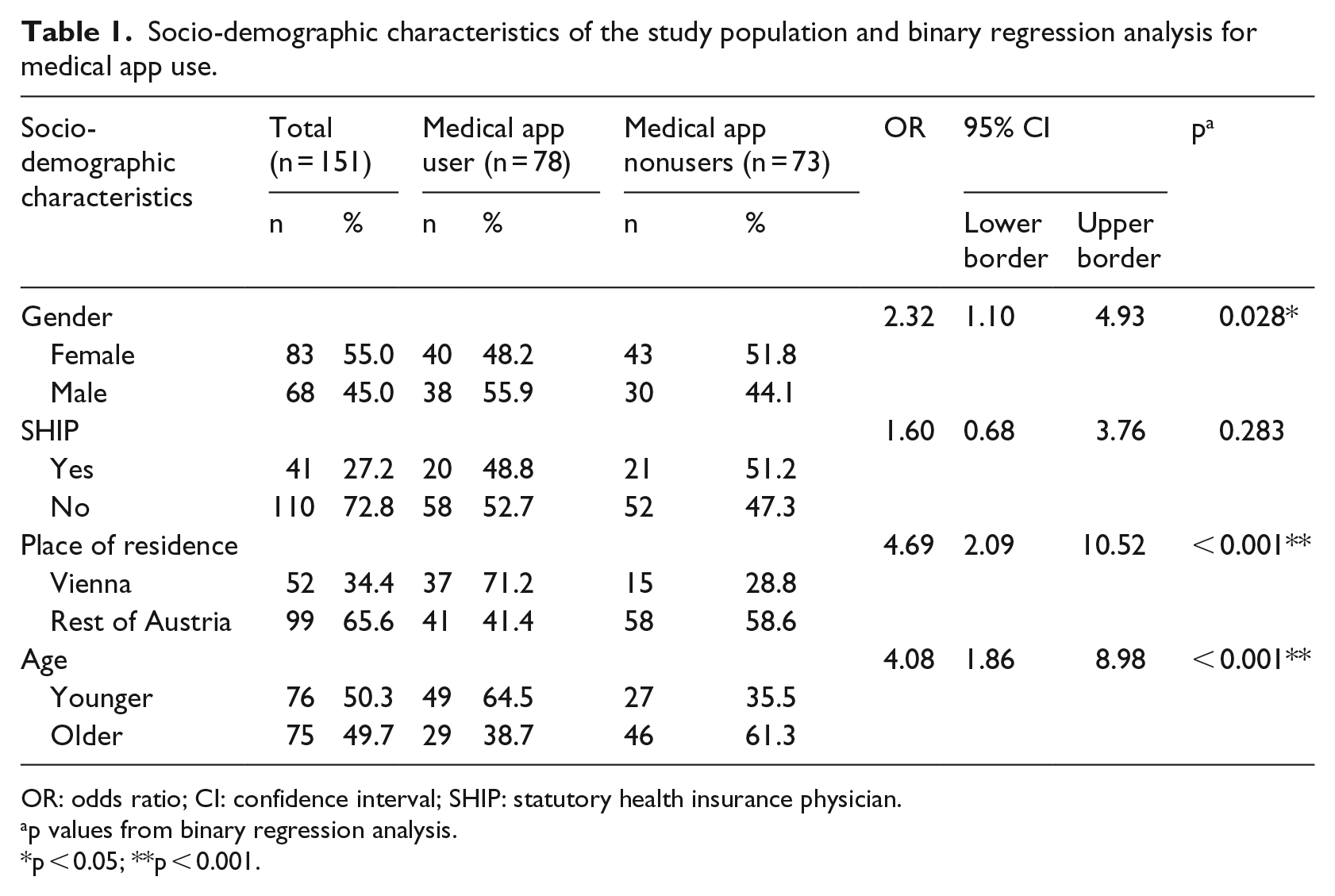
OR: odds ratio; CI: confidence interval; SHIP: statutory health insurance physician.
p values from binary regression analysis.
p < 0.05; **p < 0.001.
Binary regression analysis assessed the predictive value of socio-demographic characteristics on medical app use (use vs nonuse, dependent variable, Table 1). We calculated crude and adjusted regression models and reported results of the adjusted odds ratios (OR) and 95 percent confidence intervals (CI) with the following measures—χ2: p < 0.001, log-likelihood: 180,565, Cox & Snell R2: 0.173, Nagelkerke’s R2: 0.230, and predictive value: 66.2 percent.
Predictors of medical app use were gender, with 55.9 percent of males (OR = 2.3, 95% CI = 1.1–4.9; p < 0.05) compared to 48.2 percent of females, place of residence, with 71.2 percent of Viennese participants (OR = 4.7, 95% CI = 2.1–10.5) compared to 41.4 percent of those living elsewhere in Austria, and age, with 64.5 percent of younger participants compared to 38.7 percent of older ones (OR = 4.1, 95% CI = 1.9–9.0; both p < 0.001) being medical app users.
Table 2 shows perceived benefits of medical app use. The majority of respondents (78.8%) chose up to three different advantages of medical app use (mean = 2.4, SD = 1.5, range = 1–6 options). The top three options were higher quality of healthcare (53.6%), location-independent access to health services (53.0%), and higher efficiency in healthcare resource allocation (41.1%). Subgroups did not differ statistically significantly in their ratings.
Perceived benefits of medical app use.
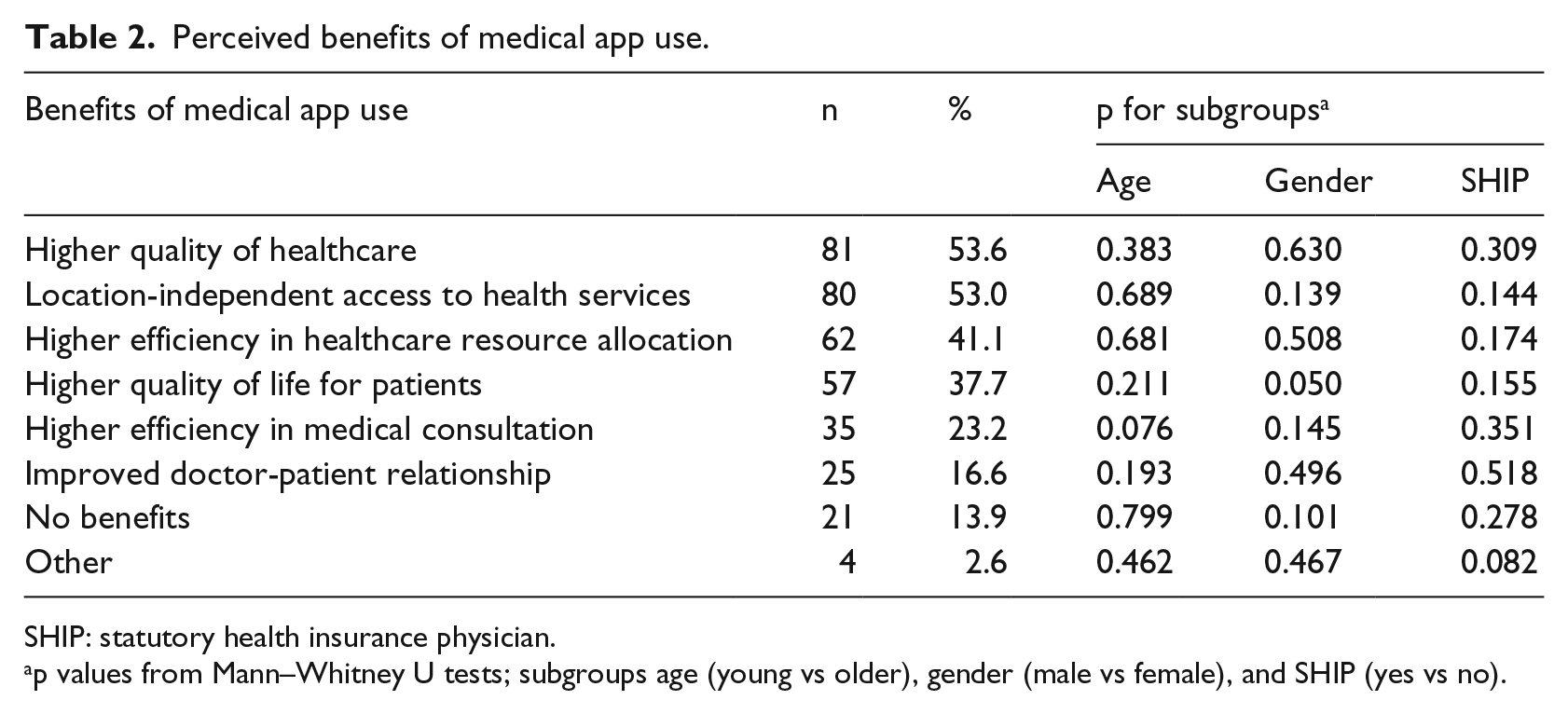
SHIP: statutory health insurance physician.
p values from Mann–Whitney U tests; subgroups age (young vs older), gender (male vs female), and SHIP (yes vs no).
For 13.9 percent of participants, medical app use did not have any benefits, as they explicitly stated in the free text question. Only four further participants used the free text box to announce additional benefits, which verbatim were “supplement to homepage, email, telephone, and fax,” “fresh guidelines,” “sound knowledge enhancement,” “health literacy,” and “cohorts from real life.”
Table 3 shows respondents’ views on clinical communication competence. Most participants were undecided with a trend toward a positive attitude regarding the statement that clinical communicative competence could be learned (62.3%, mean = 2.1, SD = 0.6), perceived that medical studies did not adequately prepare them for their clinical work in regard to communicative competence (64.9%, mean = 1.5, SD = 0.7), and thus would like to receive offers for advanced training to acquire respective skills (66.2%, mean = 2.5, SD = 0.7). Subgroups did not differ statistically significantly regarding their ratings.
Views on communication competence.
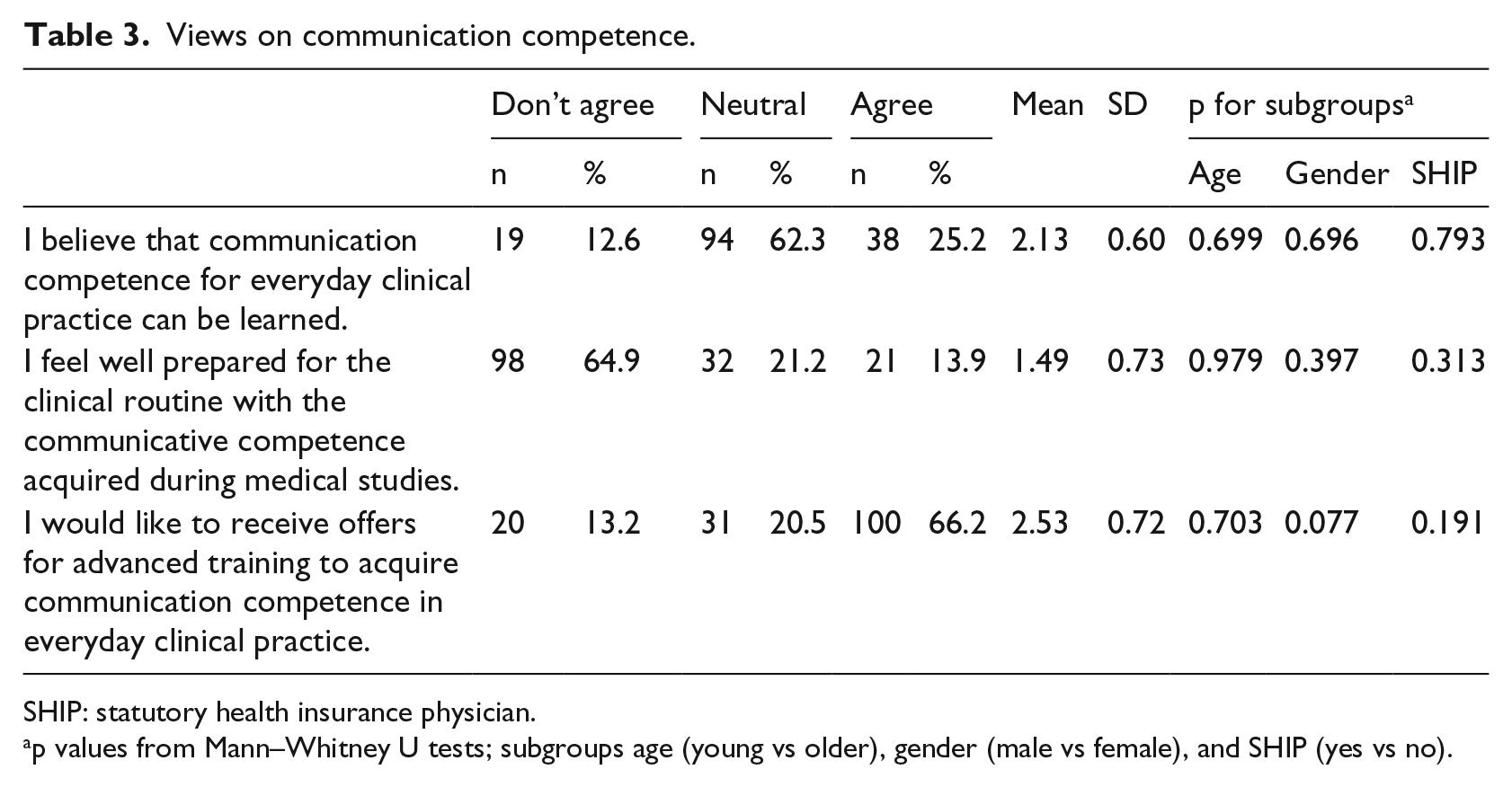
SHIP: statutory health insurance physician.
p values from Mann–Whitney U tests; subgroups age (young vs older), gender (male vs female), and SHIP (yes vs no).
We employed three hypothetical scenarios to capture participants’ most likely behavior when experiencing probable events in everyday clinical practice. While Scenario 1 assessed need for communication training (Table 4), Scenarios 2 and 3 assessed communication strategies in a clinical setting that is, for lack of native language skills and medical information retrieval (Table 5). As for Scenario 1, nearly half of the participants (47.7%) would attend the communication training course, whereas 23.8 percent would not do so and 10.6 percent were undecided. A minority of participants (17.9%) would rather prefer a flexible online course. Gender as well as SHIP did not influence indicated responses, whereas 56.0 percent of the older versus 39.5 percent of the younger age group would participate (p < 0.05), while the younger generation was by trend more intended to choose the online option (21.1% vs 14.7%, p = n.s.).
Scenario 1—Communication training.
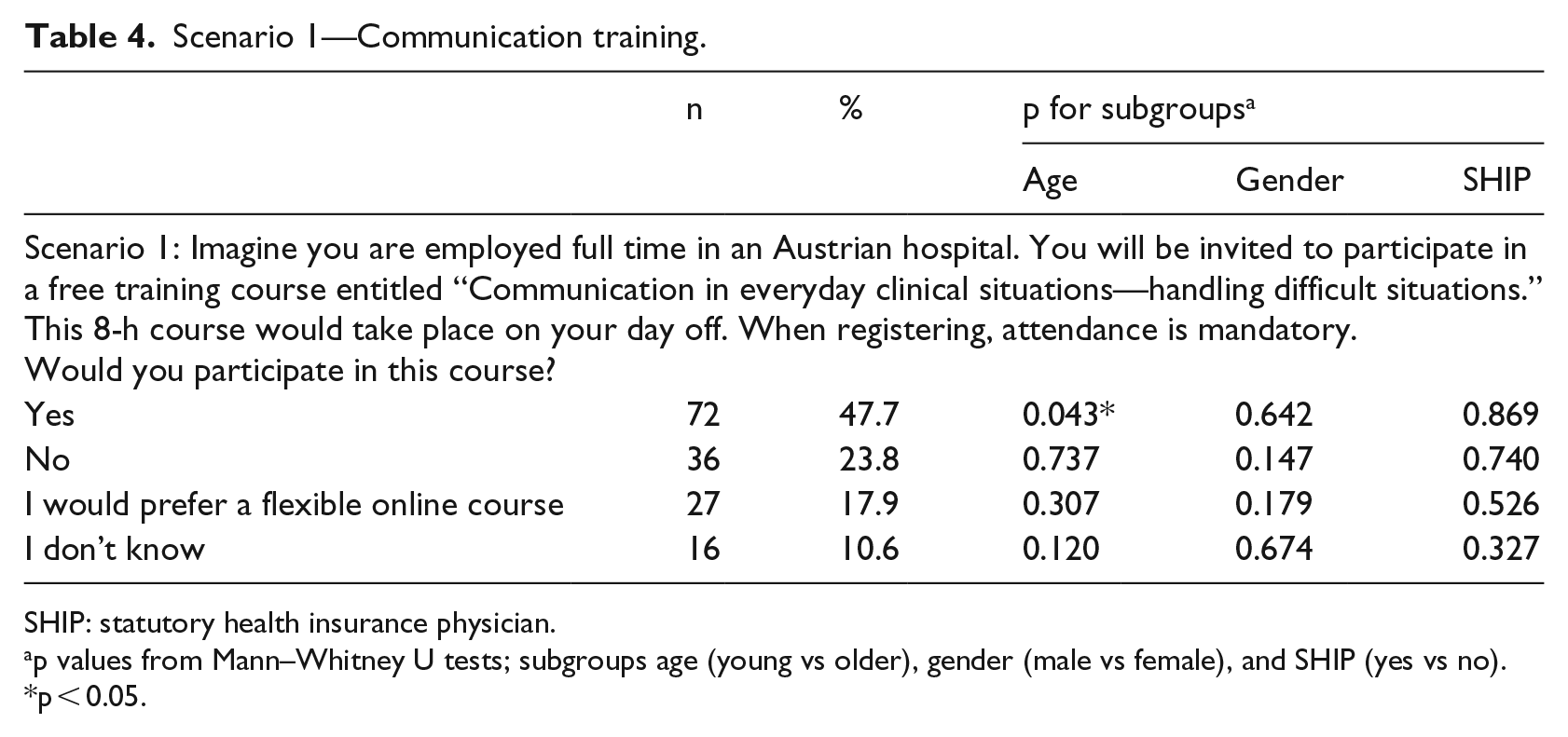
SHIP: statutory health insurance physician.
p values from Mann–Whitney U tests; subgroups age (young vs older), gender (male vs female), and SHIP (yes vs no).
p < 0.05.
Options for potential activities to address problems described in Scenario 2—Language Skills and Scenario 3—Information Retrieval.
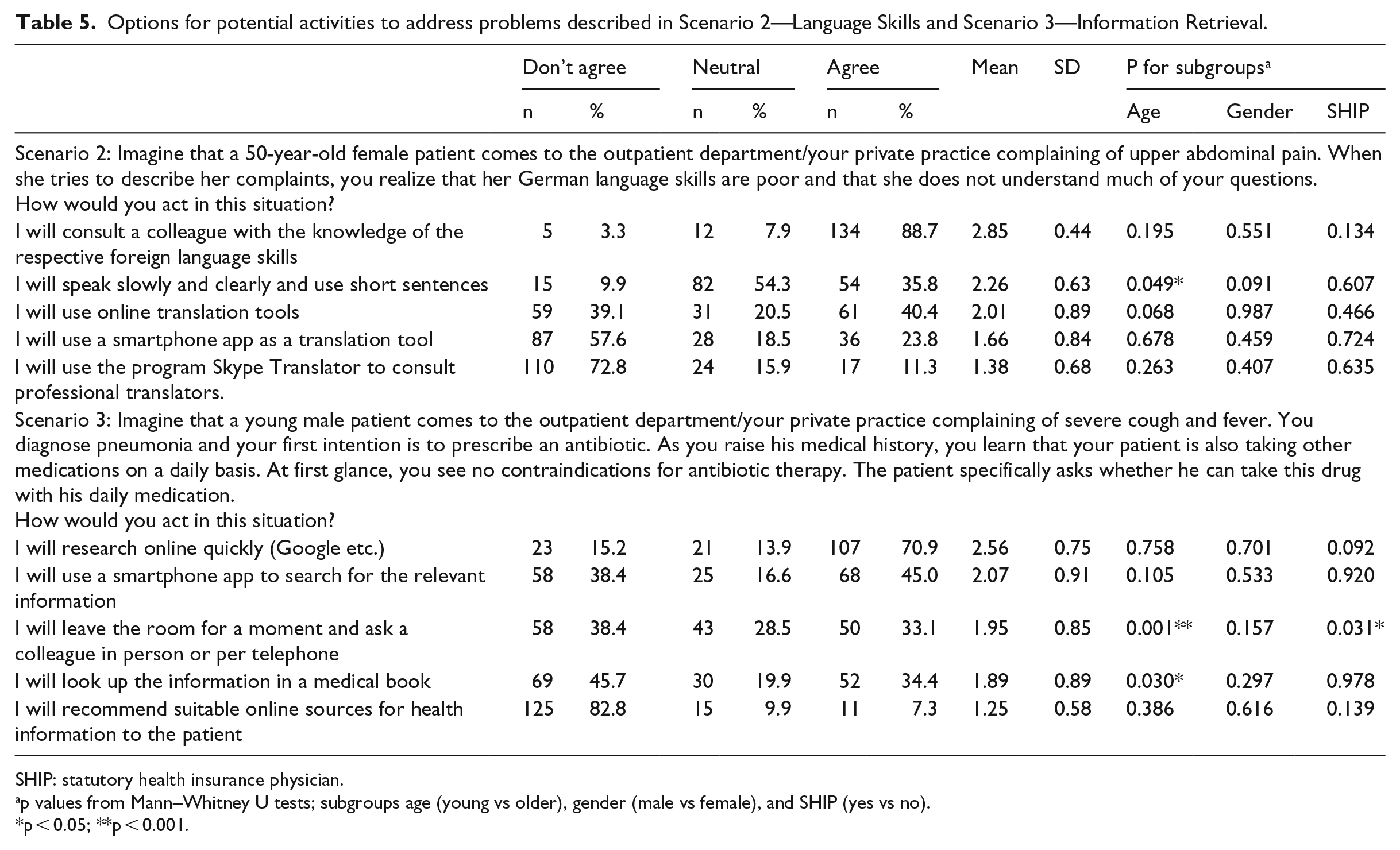
SHIP: statutory health insurance physician.
p values from Mann–Whitney U tests; subgroups age (young vs older), gender (male vs female), and SHIP (yes vs no).
p < 0.05; **p < 0.001.
The most common way to address the need for a translating support when facing a patient in need for medical advice with poor native language skills as exemplarily described in Scenario 2 would be to consult a colleague with respective foreign language skills (88.7%), and the least common option would be to use Skype Translator (11.3%). In case of consulting on potential drug interactions as exemplarily described in Scenario 3, most participants (70.9%) would prefer a quick online search, whereas very few participants would recommend suitable online sources for health information to the patient (7.3%).
Younger participants were more likely to choose the option “I speak slowly and clearly and use short sentences” in Scenario 2 compared to older ones (mean = 2.4, SD = 0.6 vs mean = 3.2, SD = 0.6, p < 0.05) and also “I leave the room for a moment and ask a colleague in person or per telephone” in Scenario 3 (mean = 2.2, SD = 0.8 vs mean = 1.7, SD = 0.8, p < 0.001). Younger participants were less likely to “look up the information in a medical book” in Scenario 3 than older ones (mean = 1.7, SD = 0.9 vs mean = 2.0, SD = 0.9).
Whereas gender did not differ regarding any of their most likely performed actions, we found a single difference regarding SHIP status as SHIP-participants were less likely to “leave the room for a moment and ask a colleague in person or per telephone” in Scenario 3 (SHIP: mean = 1.7, SD = 0.9 vs non-SHIP: mean = 2.0, SD = 0.8, p < 0.05).
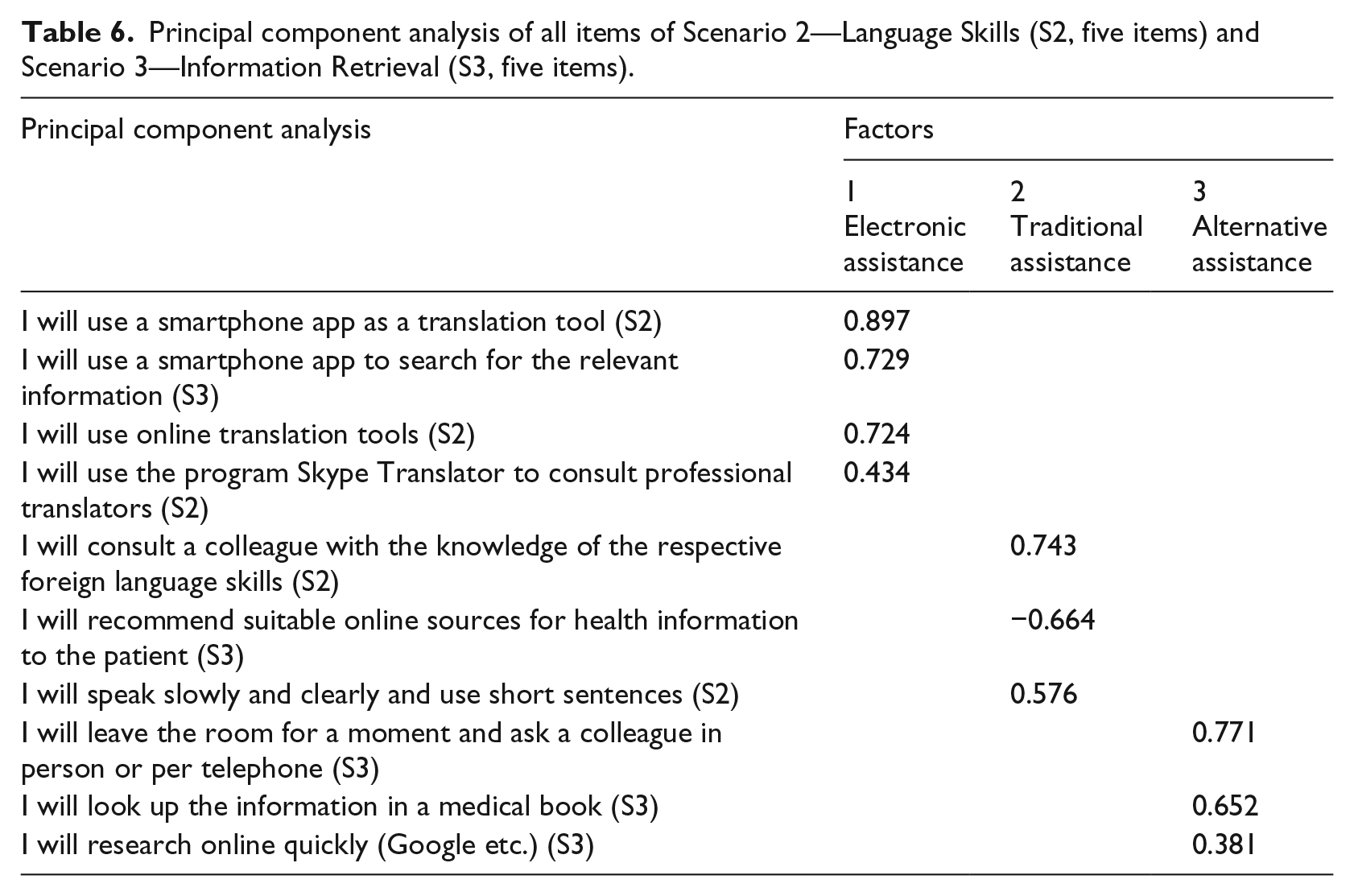
PCA assessed the factor structure of all ten items of Scenarios 2 and 3. Our data met the assumptions for this procedure, as the Kaiser–Meyer–Olkin test of sampling adequacy was greater than 0.5 (0.588), and the Bartlett’s test of sphericity was significant (χ2 = 214.237, df = 45, p < 0.001), indicating correlations in our data that are appropriate for factor analysis.22,23 PCA revealed a three-factor structure of these items, explaining 51.1 percent of the variance (Table 6). The first factor, electronic assistance, included three items of Scenario 2 and also one item of Scenario 3, all of which deal with mobile or online electronic search strategies. The second factor, traditional assistance, included two further items of Scenario 2 and one item of Scenario 3, mainly describing traditional information retrieval strategies. The Scenario 3–based item “I recommend suitable online sources for health information to the patient” showed a quite high but negative factor loading of about −0.7. The third factor, alternative assistance, included three further items from Scenario 3 describing alternative search strategies in contrast to the aforementioned innovative electronic and more traditional concepts of information acquisition.
Principal component analysis of all items of Scenario 2—Language Skills (S2, five items) and Scenario 3—Information Retrieval (S3, five items).
Discussion
In this study, we sought to determine the prevalence and views of medical app use and clinical communication competence independently and also integrated it by means of intended search for assistance in response to hypothetical scenarios. Use of smartphone and apps in everyday life is extremely popular. However, awareness of the potential use of mobile devices in clinical care facilitation and quality of care enhancement has not yet arrived in the minds of the public and stakeholders of the healthcare system. 24 Due to the lack of funding and guidelines, medical app use currently falls into a legal gray area. 18 Also, a range of practical and ethical issues have to be addressed, including bacterial contamination of mobile devices, 13 distraction of the physician, 14 error sources, and data security and privacy issues.15,21,25,26 The principal implications of medical app use and its impact on the patient–doctor relationship are complex and go beyond confidentiality concerns and are thus poorly researched yet. 15 However, an increase in medical app use could be perceived as the most promising digital tool for health prevention and therapy.
International studies already found a high level of smartphone ownership and medical app use among healthcare personnel, especially among medical students and junior doctors.8–12,27 In our study, use of medical apps was common, with more than half of the participants frequently using them several times a week up to several times a day. Only 14 percent of participants perceived that medical app use explicitly did not have any benefits.
Healthcare professionals have been consistently shown to express halting attitudes toward health-related technological innovations.4,24 Effects of socio-demographic characteristics such as age and gender on technology acceptance are evident, with traditionally lower use among older individuals and females.17,19,28 To account for the special situation of a high amount of private practitioners in Austria and the currently lack of funding for eHealth-related medical services and adequate business models, we were also interested in investigating potential differences regarding private and panel doctors (SHIP status). 18 Illiger et al. 27 found that age, professional experience, and function did not influence mobile device use among medical professionals, which was, however, more common among male doctors. In our study, male gender, younger age, and place of residence, that is, living in an urban environment, predicted medical app use.
Physicians tend to take an active role in controlling quantity and content of information provided by the patient—interrupting the patient and directing questions toward a specific concern—which results in potential loss of relevant information. 2 In general, this controlling aptitude is not very likely to enhance patient empowerment as well as mutual trust and clinical decision-making. Nowadays, pressure toward high quality of medical consultation and empathic conversation skills is even increased by online patients rating portal and forums such as DocFinder, 26 one of the most popular search engines in Austria. So, favorable ratings of users increase the competitive advantage of doctors accordingly and are thus powerful tools.
We used a scenario-based evaluation to elucidate potential real-life actions of physicians in even more advanced problems in need for preferably fast solutions. Scenario-based assessments are used in a variety of research areas, for example,. to capture public views and preferences on healthcare reimbursement, 29 dentists’ drug prescription patterns, 30 future implementation of health technologies, 31 or quality of physician practice. 25 It is not clear whether responses to hypothetical scenarios over- or underestimated the actual utilization of digital devices, online sources, and medical apps. Also, medical professionals might perceive that their clinical communicative skills are excellent, whereas the patient feels left alone with complex therapeutic options. Nevertheless, scenarios allowed us to present identical patient information to all participants, thereby reducing bias possibility and allowing estimating actual practices on the basis of collected survey data. Furthermore, Peabody et al., 25 suggested that scenarios might provide a more accurate measure of quality of care than medical records.
We found that only about half of the participants would actually attend a communication competence training on a day off to ensure that clinical schedules and well-being of patients would be impacted by the doctor’s absence. According to doctors’ law, Austrian physicians have to provide evidence for continuing professional education by regular attendance to medical training courses. 32 Thus, Austrian-employed healthcare professionals are allowed to attend trainings during working time, provided formal application for release from work and an adequate substitute. However, physicians with private practices might be more likely to choose evening or weekend courses to fulfill their obligatory amount of continuing professional education to avoid loss of earnings. For most physicians, flexible online courses might be a cost-effective and time-efficient way to increase their state-of-the-art knowledge. Also, virtual training courses are widely used already in graduate and postgraduate medical education and have been shown to be effective tools for continuing education with high satisfaction levels among participating doctors. 33 Our results showed, however, that the respondents’ attitudes were quite halting regarding this option. It could be an interesting research question addressed by future studies to elucidate ways to increase attractiveness and adoption of online courses for Austrian doctors. In synopsis with our findings on the impact of place of residence on app use with a higher proportion among the urban study population, online options could create equal opportunities for education in rural and urban areas.
Low native language proficiency and a preference for an indirect communication style have been shown to inhibit ethnic minority patients’ participation during medical counseling. 34 As proposed by Schinkel et al., 34 raising awareness about language barriers and cultural value differences, and increasing doctors’ cultural competencies to communicate adequately with ethnic minority patients could increase their health literacy, participation, and empowerment. In our study, the most common way to organize translating support (Scenario 2) would be consulting a colleague with respective language skills, speaking slowly, and using online translation tools. To investigate drug interactions (Scenario 3), consulting online sources and medical apps was a popular approach, whereas very few participants would recommend online sources to the patient. In this clinical vignette, it is potentially very unlikely that the patient is left alone with a legitimate question on potential drug interaction. Doctors might not perceive that the patient would feel uncomfortable when searching for an evidence-based solution using electronic devices in this use case. 14 Goldbach et al. 6 demonstrated that medical apps are very suitable to evaluate medical and drug information at the point of care in resource-limited settings. Medical apps were superior to PubMed abstracts in regard to answering questions related to clinical vignettes, suggesting a high accuracy and usability in clinical practice.
Nowadays, doctors frequently discuss online health information with their patients with partly contradicting perceptions of benefits and content reliability.5,35Assisting patients in finding reliable online health information might be seen as time-consuming, and no incentives are provided. 36 We found a low adoption of recommending suitable online sources for health information to the patient in a hypothetical setting as described in Scenario 3. Non-adherence caused by an imbalance between perceived need for medication and concerns about taking it could be avoided by patient-centered communication techniques to engage the patient in shared decision-making about medication. This is especially relevant in the case of prescribing antibiotics given rising awareness for increasing bacterial antibiotic resistance and the need for their rational use. 37 However, evaluating a patient’s stage of readiness to adopt self-management practices is often difficult and time-consuming. 38 To avoid the danger that the patient is confused of health information retrieval via Dr. Google and health forums, these recommendations could additionally be given to increase transparency and mutual trust. 39 This finding is in line with results of a previous study among Austrian inhabitants reporting that doctors rarely recommend health-related websites and that the effects of prescription or nonprescription medicines are commonly searched online. 17
We performed a PCA for the items of Scenarios 2 and 3 to validate our survey instrument and to check whether scenario-based evaluations presenting clinical vignettes were suitable to test point-of-care behavior and whether variable reduction could be reasonable. Indeed, the three-factor structure revealed categories reflecting electronic, traditional, and alternative assistance preferences. While the sample size was adequate for PCA, 23 the low response rate could have introduced a nonresponse bias, adversely affecting reliability and validity of our study.
We developed a German study questionnaire specifically for online surveying, including scenario-based assessments. This instrument might be a useful tool for future research to investigate more fully the effects of mobile medical apps on critical thinking, decision-making, and their impact on performance and patient outcomes. To describe a complex clinical setting, we asked participants how they would react in hypothetical application scenarios. While this approach can be useful for obtaining qualitative data about attitudes toward real life use of medical apps, it may not reflect real actions by physicians. Also, the introduced scenarios cannot be generalized beyond the context of the study. Unfortunately, we received a low number of free text comments, so we mentioned them for the sake of completeness without interpretation attempt.
Given the rapid speed of technological development and constraints in healthcare provision in an aging population facing doctors’ shortage, identifying gaps and capitalizing on digital opportunities to improve clinical communication are important. Future research approaches could use qualitative or mixed-methods designs to elucidate more in-depth motives regarding medical app use and their impact on clinical communication. Large-scale representative surveys should be conducted to further refine the methodology applied in this study, and longitudinal studies using our research instrument could observe trends in medical app use.
Also, established conceptual models could be translated into measuring aspects of medical app–based healthcare delivery. Exemplarily, the theory of swift and even flow highlights two fundamental concepts, namely, the degree of variability in the quality, quantity, and timing of information, and the availability of evidence-based information at point of care to maximize information utility. Through medical apps, all tenants of this theory are supported as variability and errors, for example, in therapeutic decisions; documentation time could be reduced; and quality in information management process and patient care time could be increased. 40 So, it is very likely that medical app use is capable of streamlining hospital efficiency and performance by enhancing doctors’ communication competence at point of care.
Conclusion
Doctors are already increasingly discussing online health information with patients. Medical apps definitely have the potential to save physicians’ time by efficient information gathering and increase quality of care. In general, it is assumed that this area of research will gain more attention in the future, as especially younger doctors represent a convenience-driven, technology-affine, and internet-savvy generation. The full potential of medical apps is not exploited yet in face-to-face medical consultation. Notably, shared efforts by public and private organizations, app developers, mass media representatives, and individuals are needed to increase feeling of safety, legal security, and usability of medical apps in their use during patient contact. This study contributes to our understanding of doctors’ prevailing views and perceptions on benefits and which barriers might be encountered when implementing a national strategy for using medical apps in clinical settings.
Footnotes
Acknowledgements
The authors sincerely appreciate the contribution from all participants of the online survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.