
Abstract
This study aims to investigate healthcare practitioner behaviour in adopting Health Information Systems which could affect patients’ safety and quality of health. A qualitative study was conducted based on a semi-structured interview protocol on 31 medical doctors in three Malaysian government hospitals implementing the Total Hospital Information Systems. The period of study was between March and May 2015. A thematic qualitative analysis was performed on the resultant data to categorize them into relevant themes. Four themes emerged as healthcare practitioners’ behaviours that influence the unsafe use of Hospital Information Systems. The themes include (1) carelessness, (2) workarounds, (3) noncompliance to procedure, and (4) copy and paste habit. By addressing these behaviours, the hospital management could further improve patient safety and the quality of patient care.
Introduction
Health information technology (HIT) is the overarching term applied to various information and communication technologies used to collect, transmit, display, or store patient data. 1 HIT, which includes hospital information systems (HIS), electronic health record (EHR), computerized physician order entry (CPOE), electronic prescribing (e-prescribing), clinical decision support systems (CDSS), and bar-coded medication administration (BCMA), has been widely implemented in healthcare organizations to support healthcare services. HIT is expected to increase the quality and safety of healthcare services by improving communication, patient delivery time, and documentation. Despite the benefits, HIT could also introduce consequences when it is poorly designed, implemented, and used. Problems related to HIT can disrupt healthcare delivery, harm patients, and even cause death. For instance, a retrospective analysis of all reported safety events from 2005 to 2011 under the Clinical Safety of England’s national programme for information technology (IT) found that three deaths were linked to software-use errors and pending test result from previous hospitalization record that was not visible to the relevant clinicians. 2 A more recent study on EHR-related medication errors in two ICUs (intensive care units) revealed that 34 per cent of the medication events included orders with omitted information and duplicated orders. 3 These EHR-related errors had greater chances of harming the patients and they occurred more frequently at the ordering stage compared with other events. In addition, the human–computer interaction problem was the most frequently reported, associated with HIT-related patient safety incidents. 4
Previous studies have looked at the sociotechnical factors affecting safety including people, technology, tasks, organization, and the environment. Hautamäki 5 reported usability issues such as information on multiple views, the reliance on healthcare practitioners’ memory to execute daily tasks, and issues with patient identification caused usage errors that led to patient safety incidents. Moreover, the results from the system’s literature review and interviews with medical doctors showed that knowledge, system quality, information quality, service quality, training, organization resources, teamwork, task-related stressor, physical layout, and noise as the sociotechnical factors influencing the safe use of HIT.6,7 However, little is known about the specific nature of healthcare practitioner behaviours affecting unsafe use of HIS in clinical settings. Hence, this study addresses the question: How do healthcare practitioners use HIS that pose risk to patient safety and quality of care? The aim of this study is to identify healthcare practitioner behaviours that influence the unsafe use of HIS. Medical doctors who have adequate experience in using HIS in Malaysian government hospitals participated in the semi-structured interview. This study believes in the safe use of HIS as the prevention of errors, accidental patient harm, and adverse events within the care process by using HIS.
Methods
Semi-structured interviews were conducted to identify healthcare practitioner behaviours that influence the unsafe use of HIS. Details of the research methods used for this study are explained in the following sections.
Sample and setting
Semi-structured interviews were conducted in three Malaysian government hospitals located within Federal Territory and the Selangor state. The hospitals were selected based on their experience with HIS implementation, hospital size, and working environment. These selected hospitals implement Total HIS (THIS) to support their healthcare services. THIS integrates various hospitals subsystems such as Laboratory Information System (LIS), Pharmacy Information System (PIS), Radiology Information System (RIS), and Picture Archiving Communication System (PACS). All the chosen hospitals had implemented the same version of THIS. Therefore, the design and implementation of THIS follow a similar standard. Both Hospitals A and B had completely implemented THIS in December 2007, whereas Hospital C implemented it 2 months after Hospitals A and B. At the time of data collection, Hospital A, a national reference centre for haematology patients, had 562 beds. Hospitals B and C shared the same number of beds at 620. Therefore, it is anticipated that all the three hospitals have a similar working environment and experience of THIS implementation.
This study primarily focused on doctors who are also THIS users. Considering their important role in patient-care delivery and their routine use of the THIS, they can be considered crucial research subjects. THIS use is mandatory to all doctors in the selected hospitals. Moreover, THIS training was also provided to all the doctors. Purposeful sampling was adopted to select the suitable candidates to participate in the interview, because the aim was to provide rich information in context. The criterion for the sample selection was a minimum of 1-year experience in using THIS. According to the statistic obtained from the human resource department of each hospital, the total number of doctors working in the three hospitals was 770 in December 2014. In total, 31 medical doctors participated in the interview, in which 10, 9, and 12 doctors are from Hospital A, B, and C, respectively. About 58 per cent of the participants were female doctors. The participants were attached to various departments, including emergency and trauma, medical, general surgery, paediatric, obstetrics and gynaecology, orthopaedic, otorhinolaryngology, ophthalmology, cardiology, nephrology, neurosurgery and neurology, haematology, psychiatric, and rehabilitation. Their experience in using THIS was between 1.5 and 10 years.
Data collection
Semi-structured interviews with 31 medical doctors at the three hospitals were held between March and May 2015. An ethics approval from Malaysia’s Ministry of Health Medical Review and Ethics Committee (MREC) and the participated hospitals were obtained prior to the data collection. A semi-structured interview guide was designed to manage the discussion with the medical doctors (Appendix 1). The interview questions contained neutral and open-ended questions to avoid eliciting socially desirable responses. New questions were permitted to arise as a result of the discussion. The data collection method used an interview protocol developed by Hesse-Biber and Leavy. 8 Potential participants were approached at their workplace to get their agreement to participate in the interview. They were given a brief explanation about the study and the interview. Once they agreed to participate, face-to-face interview was conducted at the participants’ workplace on a date and time that were convenient for them. A mix of both English and Bahasa Malaysia languages were used throughout the interview. The interview questions consist of neutral and open-ended questions. The interview sessions were audio-recorded, except for two sessions which were manually recorded because the participants were reluctant to audio-record their discussion. Each interview session took around 15–20 min, and the total duration of all the interviews was approximately 14 h.
Data analysis
The analysis of the interview data was conducted according to the steps suggested by Creswell. 9 First, recorded audio data and handwritten notes from the interviews were transcribed to word processor text. Transcripts of interviews were then presented to the interviewees for validation purposes to ensure the interviewer had captured the respondents’ intended meaning. Then, the interview transcripts were organized into sections for easy retrieval. Subsequently, the transcribed interviews were then coded using the qualitative data analysis software, ATLAS.ti. The interview transcripts were divided into text segments and these segments were labelled with the codes. Table 1 presents an example of codes applied to a short segment of data. The transcripts were read repetitively to highlight parts of the text and to emphasize the sections and issues that appeared to be significant and relevant. Deductive coding was used for the analysis.
Example of data extracted with codes applied.
The coded data were studied to detect areas of similarity and overlap between codes. All overlapping and redundant codes were removed. Finally, similar codes were grouped together under theme or category to form a major idea. Codes that appeared to share some unifying feature were clustered into a theme. 10 Thematic maps were used as the visual representations to help sort the different codes into themes. Figure 1 shows the thematic map that shows the relationship between themes (shown as circles) and codes (shown as rectangles) deduced from the thematic analysis. All the themes were reviewed and discussed among the team members to confirm that the themes meaningfully capture the important and relevant elements of the coded extracts and the entire data set. Any variance in interpreting the findings was fixed through discussions until consensus was reached. Themes that were deemed not relevant were discarded.
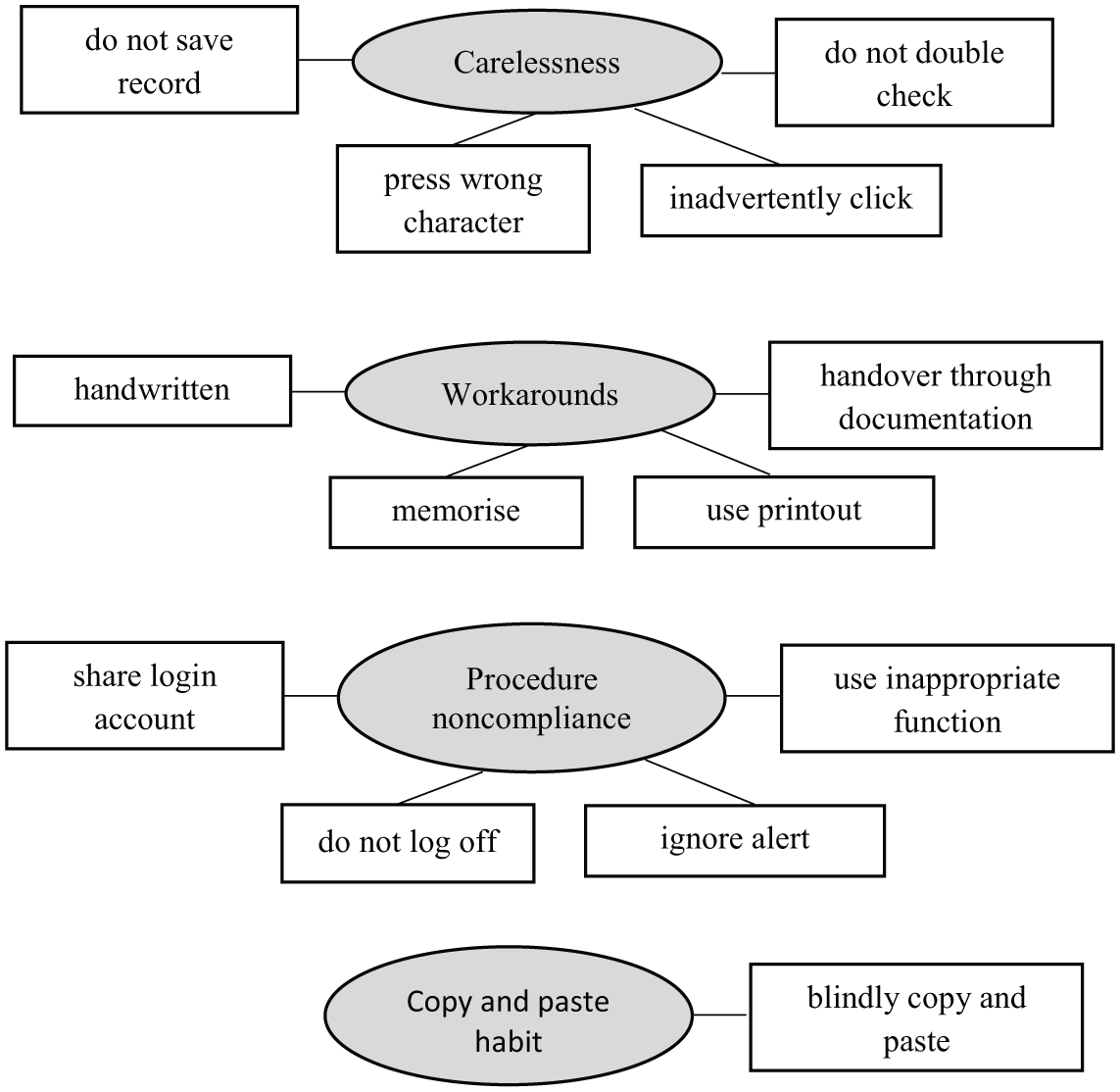
Thematic map.
Results
The interview sessions revealed four themes that emerged as healthcare practitioner behaviours that influence the unsafe use of HIS. The themes include (1) carelessness, (2) workarounds, (3) noncompliance to procedure, and (4) copy and paste habit.
Carelessness
From the interview, the respondents stressed that being vigilant by double-checking everything is very important to avoid errors while using HIS. This is because HIS does not have error-check feature. Therefore, healthcare practitioners need to double-check their own work. The points are highlighted as follows: Currently the system does not offer the check and balance system, thus you should use the system carefully. You are prone to make mistakes if you do not double check your work. Therefore, doctors should double check their own work. (Respondent 8b) The most important thing to avoid making error in the use of HIS is to be aware and more vigilant. You are the only one accessing the patient; no one is going to remind you. (Respondent 8a)
It is essential for healthcare practitioners to double-check patient names because there may be patients with similar names. Carelessness can possibly cause the healthcare practitioners to inadvertently select or enter notes on the wrong patient. Respondents explained their views as follows: Sometimes when there are patients with the same name, we inadvertently click on the wrong patient when we are actually seeing a different patient’s profile. (Respondent 3a) To me, the main problem is in terms of work attitude such as not being careful and alert. Sometimes we login to the HIS using others’ account, we enter notes to the wrong patient that has similar patient’s name because we do not look at the names carefully. (Respondent 6c) We have to double check the patient’s name. If we have the RN, we must make sure the number tallies because we can have similar patients’ names, but they are different persons. After you key in the entry, re-read the entry at least once so that we do not inadvertently enter the wrong information or wrong patient’s record because sometimes we open two to three patients’ records at the same time. (Respondent 9c)
The respondents also remarked that errors can possibly happen due to an inadvertent click on the wrong item from the option lists. For instance, the healthcare practitioners might click the wrong medication, dosage, or patient record. Besides, healthcare practitioners are also prone to press the wrong characters on the keyboard. Hence, healthcare practitioners are advised to always double-check before signing notes and make corrections after committing any mistake. Respondents expressed this inference in the following ways: Sometimes errors happen when we select the items by clicking from the list to order medication. The common errors include wrong medication and dosage. In terms of ordering, the errors are always caused by viewing at the wrong patient ID or inadvertently clicking on the wrong record. The reason is more on the individual carelessness. (Respondent 5a) You should double check the patient’s name, select the correct record, and order the right dosage. In general, you should always double check before confirming or signing the notes. Amend the notes whenever you do mistake. HIS needs to be used carefully. (Respondent 6b) You have to double check. It is easy to inadvertently click on the wrong option or cause typing error on HIS. For some people, it is not because they do not know how to spell the word; it is just because they accidentally pressed the wrong character on the keyboard. (Respondent 7c)
Moreover, some healthcare practitioners forgot to save notes entered in HIS. Hence, they need to retype the unsaved record. This problem will cause problems for other doctors viewing the notes or the patient-care plan. Respondents highlighted the issues by saying: Double check everything we do on HIS. Sometimes when we are in a hurry, we may forget to click the record button. As a result, the entered data might disappear and not be saved in the system. Thus, we have to redo. (Respondent 4a) You must make sure the data are recorded in the system so that it is not lost. Sometimes we have to retype because we forget to save it. (Respondent 5c) A doctor might enter the patient’s notes but forget to sign the notes. Thus, other doctors won’t be able to view the notes or instruction because the notes are not saved in the database. Consequently, other doctors could not carry out the order. (Respondent 2b)
Workarounds
Based on the interview, it was revealed that healthcare practitioners do not immediately enter or update patient-care plan on HIS during the ward round. Instead, they would transcribe the information into HIS after the ward round. All information is temporarily handwritten while the ward round is being conducted. It is possible to make mistakes when transcribing the information such as wrong ordering, and wrong data entry for the patients’ record. Respondents emphasized their views as follows: In terms of documentation during the rounds, we handwrite or memorise the information and later transcribe them into the system. Sometimes we may key in the r wrong patient’s record. (Respondent 4a) When there are many patients and lack of computers, we have to handwrite. Sometimes when we are busy it is possible to make mistakes when we transcribe the information into the system such as wrong ordering, mistaking similar patients’ names. Transcribing from paper into the system then, not double checking is the common HIS misuse that causes errors. (Respondent 10a) It is not very convenient to carry a computer from bed to bed. Of course, it will take a bit of time to re-key in and look for this and that. Therefore, what we do is we write our plan for the patients and everything else on a small piece of paper. When there is a computer available for use only then, we key in the information. (Respondent 8c)
Some of the respondents expressed that the ward round is carried out fast, thus constituting to the reason that some healthcare practitioners prefer to enter notes or plan after the round. Moreover, healthcare practitioners do not have sufficient time to immediately key in the notes during the ward round. Therefore, they write down the necessary information on a paper before transcribing it into HIS. Respondents expressed their views by stating that: When the ward round is conducted quickly, the junior doctor or HO sometimes do not have enough time to key in the notes immediately. They usually write down on paper and key in later. (Respondent 9a) Ward round is fast. We do not have enough time to type during the round. Therefore, we use both the paper and HIS. Usually the data entry will be continued after the round by referring to the manual notes recorded by the colleague. (Respondent 7b)
The presence of too many patients is another reason for healthcare practitioners to transcribe the patients’ notes from paper into HIS afterwards. There is a possibility that the healthcare practitioners might miss or forget to key in some information into the patients’ notes as they are all transcribed into the systems after the ward round. Respondents pointed out their views as follows: When there are too many patients, we do not have the chance to enter all patients’ notes each time during, or immediately after consultation. When this happens, we will write down the important notes on paper so that we do not forget to transcribe them into HIS afterward. (Respondent 9b) Sometimes when there are too many patients, you have to gather all the patients’ notes and transcribe it later into the system at once. Of course, there is chance that you may miss or forget to key in some information. It all depends on the person and their notes. They have to write everything they remember. Then, it will be much easier. (Respondent 8c)
Besides that, the interview findings show that memorizing is another workarounds strategy to overcome the problems or constraints associated with HIS usage. For instance, healthcare practitioners memorize the information to be entered due to the problem of entering notes. Apart from that, healthcare practitioners memorize patients’ information before the ward round. Sometimes, it could lead to error because the information is not presented during the ward round. Respondents expressed their views as follows: The annoying part is that when the system is slow starting at midnight until 2.00am. Sometimes, I cannot enter the notes. I have no time to wait, so I memorize it and come back later. (Respondent 4b) In terms of viewing the patient’s notes, we usually read all the patients’ notes in the morning for about 30 minutes to an hour before the ward round. Especially on Monday since we do not know what went on during the weekend. Thus, we have to read their medication, investigation, and blood results before the round. We normally memorize the information. We do not print because it wastes paper and ink. Thus, sometimes it can cause error because the information is not physically there during the round. (Respondent 7c)
However, some healthcare practitioners choose to printout the information from HIS for their reference during the ward round, but HIS is still not used during those times. In this situation, the printed paper may be misplaced, and consequently exposing the patient’s information to others. In addition, notes are not entered immediately during the ward round. Therefore, it could result in some missing information. Respondents explained this view as follows: I have seen a lot of HO printing out the case notes before ward round so that they can keep it as reference during the round. It is not right because it can end up anywhere. This is legal medical document because patients’ information such as name, identification number, and notes are there. Let say you misplace it and end up with someone else, things can go wrong. By right, it is the wrong thing to do, but then, a lot of people are doing it because it saves time and is easier to keep as you cannot remember every single patient’s story. (Respondent 5b) We usually print the patients’ notes or view their record from the computer prior to the round. We do not refer to the computer during the round. Instead, we write down their progress notes. Sometimes we may forget to key in certain information because we do not update the notes immediately. (Respondent 2c)
Some of the healthcare practitioners also sometimes write notes on the printout due to the rush in ward round. The data entry for all patients will be done afterwards. Transcribing notes from handwritten documents into the HIS is proven to double the healthcare practitioners’ work. A respondent explained the view: Sometimes we write notes on the printout. If it is not a rush round, we can see the patient and type the notes there, but when it is too fast, you cannot. Therefore, you write down all the details and plan on a piece of paper. Then, you sit down and submit the entry for everyone. It doubles the work. (Respondent 5c)
In addition, it was revealed that sometimes, discussion among doctors from different departments regarding referral patients is done through HIS. The notes or plan is handed over merely through documentation. Hence, verbal communication does not happen. Conversely, if the referred doctor meets the corresponding doctor to verbally discuss about the case based on the manual approach, the referred doctor immediately writes down the notes into a file after the meeting. However, through HIS, the corresponding doctor only refers to the plan that is sometimes submitted late on HIS. Respondents expressed this inference in the following way: For example, if the patient is referred to a doctor from another department, the way of communication is through HIS, if verbal communication does not occur. We depend on the plan or notes entered in HIS. We have to wait until they enter the plan into the system. Sometimes when they are very busy, the data entry could be pending until the evening. As a result, we receive the plan late in the evening. Otherwise, sometimes the doctor will meet us to inform or discuss about the plan verbally. (Respondent 9a) The communication is merely through documentation. Previously, we had our discussion verbally. Even with the other department, it is just based on the referral letter. Unlike last time, the referred doctor came to meet the related doctor to give feedback on the patient verbally then, they would write the notes into a file. Currently, the referred doctor just attends to the patient then, enters the notes at any computer. The related doctor waits for the notes to be entered into the system. Sometimes, the referred doctor attends to the patients in the morning but only enters all the patients’ notes later, in one shot. Thus, the related doctor can only view the notes in the evening. Unlike in the manual system in which the referred doctor has to immediately write in the file before they leave. Less communication and errors can happen. (Respondent 6c)
Procedure noncompliance
For the best use of HIS, it is essential for healthcare practitioners to follow the appropriate HIS procedure. The interview findings show that some healthcare practitioners shared their HIS login account or used their colleague’s account. This will make it difficult to trace back to the responsible person when problems occur if a healthcare practitioner let their colleague use their account. Hence, it causes problem and delay to patient delivery. For instance, a pharmacist detects a wrong medication order and confirms it with the doctor based on the logged account, but often times the doctor would not admit the mistake. Respondents conveyed this view as follows: It took long time to open the system. During the grand ward round, the round is done in group that involve consultant, specialist, MO, and HO. Thus, the HO type in using his colleague account. Nevertheless, when there is problem in the notes entry such as incomplete or wrong information, we cannot trace the HO who done the entry. (Respondent 1b) The main concern and issue in the hospital is that sometime doctors use other doctors’ HIS account. Let’s say the doctor wrongly order a medication, the pharmacist will call the doctor based on the login account. The doctor whose account is logged into will not admit that he is the person who made the order. It then, causes problems and delays to patient delivery. (Respondent 10a)
Besides, a respondent stated that some specialists simply give their authorized account’s password to doctors for making order. However, it may turn out to be a problem if the doctors misuse the password for other unrelated orders: Some orders such as CT scan can only be ordered by the specialist. This results in delay as there is a need to request for authorization from the specialist. Hence, some doctors are given the specialist’s password. It becomes a problem when the doctors misuse the password for unethical purposes. (Respondent 2b)
The respondents also pointed out the need to always immediately log out from HIS account to avoid other healthcare practitioners from using it. Respondents expressed this view in the following ways: Make sure that we log out after each time we log in to the system. Often, we do not log out. Thus, others can use our account to access HIS. (Respondent 3a) We are so used to handling HIS, we straight away find a computer and type into it without actually realizing that we are using someone else’s account. It is actually not good for both parties. (Respondent 5b)
Ignoring alert is another issue related to the noncompliance to procedure discovered from the interviews. In most cases, healthcare practitioners tend to ignore the alert or do not read the alert carefully because the alert frequently shows up and is always unnecessary. Respondents reported this view as shown below: There are too frequent and unnecessary alerts especially for the medication ordering. Some doctors tend to ignore the message. (Respondent 8b) We have many alerts regarding to the medication ordering because patients’ safety is more related to the medication. We are so used to it and simply ignore it and tick at the box. (Respondent 12b)
Moreover, some healthcare practitioners tend to use inappropriate functions to perform a particular task on HIS. For instance, a healthcare practitioner uses progress notes function to enter new patients’ notes. However, in practice, healthcare practitioners actually have to enter the new patient’s notes under clerking notes function, but they avoid using it because it is time-consuming to enter lengthy information. This comment was made by respondents who stated that: For new patient, the system requires us to fill in every detailed information in multiple pages which is time consuming. Thus, I use progress notes function instead of clerking notes function even though it is for a new patient. (Respondent 3b) We have functions for clerking and entering progress notes. The entry has more details for the clerking function than the progress notes. Thus, we interchange between clerking and progress notes entry. For the rehab department, the examination is from head to toe. If we key in every detail under clerking notes, it may take up to two hours and therefore, delaying the patient-care. (Respondent 2c)
Copy and paste habit
From the interviews, it was also revealed that the copy and paste habit contributes to the unsafe use of HIS. Copying and pasting have become the habit and trend among HIS users. In this case, respondents remarked that copy and paste is not a problem as long as healthcare practitioners understand the case and do not copy and paste blindly, as shown below: There are doctors who misuse the function by copy-pasting all the information. This is common. We can copy and paste but we must understand the condition of the patient. If we do not understand, there will be the same information being copied for a one-week progress. (Respondent 4a) Copy paste is becoming a trend. In reality, you will definitely copy and paste. No one will key in from A to Z because the problem is already summarized on HIS. The problem is that the new doctors will blindly copy and paste. So, nothing new is updated or translated into the documentation. Copy and paste is fine, but you have to do it wisely. (Respondent 9c)
Patients’ medical status may change after a long stay in the ward. However, some healthcare practitioners do not update the initial progress according to the current status. They merely copy the initial progress notes and simply add new progress notes to it. Eventually, other doctors who refer to the notes may not understand it. A respondent expressed this by saying: Copy and paste is a disadvantage of HIS when everyone does it blindly. Some people just copy and paste the initial story and just add the current progress of the patient. However, the initial story can change because for patients who stay longer in the ward, many things can happen to them. The minor things should be changed, but they just copy and paste from the previous ones making you unable to understand because you see different patient every time. (Respondent 5b)
A respondent also highlighted that copy and paste without updating the necessary information could result in lengthy documents: Copy and paste has become a habit. However, copy and paste is very dangerous. The nurses merely copy-paste and add their own notes at the bottom. In fact, they can edit the copied information at top. This results in lengthy documentation. (Respondent 6c)
The act of copying and pasting blindly without double-checking the information may repeat the error done by others. This implication was highlighted by a respondent below: Most of the doctors copy and paste the information from others. The information typed previously may not all be correct. If the doctors merely copy and paste without double checking the information, the mistake will be repeated. (Respondent 8b)
Discussion
The qualitative study had successfully identified the significant healthcare practitioner behaviours in adopting HIS that possibly affect patient safety and quality of care. The unsafe behaviours include carelessness, workarounds, noncompliance to procedure, and copy and paste habit. The themes are consistent to the systematic literature review carried out by Salahuddin et al. 6 It is important to note that vigilance is able to prevent mistake while using HIS. Wrongs in patient’s record, data entry, selection from dropdown menus, and file uploads were the most commonly reported mistakes that led to clinical errors such as assigning the wrong dose and wrong instructions.5,11 Similar to Ash et al. 12 study, carelessness resulted in healthcare practitioners to inadvertently click on the wrong item and misspelling when performing data entry. Selection errors were found to be the most frequent errors in using HIT, especially electronic prescribing.13,14 Healthcare practitioners did not perform any confirmation on the default value or forgot to delete or change auto-populated information that may cause patients to receive wrong medication dosage. The healthcare practitioners did not double-check and, subsequently, commit errors due to performing tasks urgently to meet the organizational demand as well as the time pressure. There is also a possibility for healthcare practitioners to forget to enter the patients’ notes.
The workarounds are associated with memorizing or writing down notes before transcribing them into HIS, writing notes on HIS printout, and completely relying on HIS for information handover. In accordance with the findings of Or et al., 15 healthcare practitioners wrote down all related data on paper and re-transcribed the data into the system later due to inconvenient access of the system at the patients’ bedside. Occasionally, the healthcare practitioners were unable to recall some of the details when entering the data into the system as well as having delayed data entry. Niazkhani et al. 16 identified that lack of mobile computer devices, time-consuming process of order entry, busy work schedules of physicians, and lack of adequate coordination between team members were the factors of workarounds. The workarounds resulted in physicians relying merely on their memory, handwritten notes prior to transcribing into HIT, and delayed order entry. Reliance on memory resulted in healthcare practitioners not recording necessary information in the system or recording a wrong medication dose, unit, administration route, or schedule into the system. 5 Moreover, very similar to Saleem et al.’s 17 study, healthcare practitioners used the printout of information from HIS for their reference and also wrote notes on the printout to make up for the restraints of the HIT implementation. Workarounds manifested when HIT failed to support physicians in their work. 18 Our qualitative data indicates that the workarounds can cause undesirable negative effects on patient safety and quality of care.
Simply by using others’ HIS account, the habit of not logging off, ignoring alert, and using inappropriate function, these acts can be identified as misconducts of the working procedure. Login and alert features are the primary designed for safety purposes. However, healthcare practitioners may get annoyed with these features and, consequently, bypass these features when they are poorly integrated with their workflow. Wentzer et al. 19 revealed that time-consuming login procedure and systems did not adequately support the mutual dependencies of physicians and nurses’ workflow, which had led some of the physicians to share their login account with nurses. Besides that, many healthcare practitioners used other healthcare practitioners’ accounts that are already logged in during previous sessions instead of using their own account when attending to the urgency in providing medical care due to a time-consuming login procedure.20,21 Moreover, the pop-up alerts call for healthcare practitioners’ attention to carefully consider whether a process could be harmful. The sheer numbers of alerts, inconsequential alerts, and the way these alerts are designed have influenced the way healthcare practitioners respond to alerts. 22 Practitioners distracted by too much irrelevance alerts may ignored the alerts. This sometimes causes an important alert to be missed, which potentially can endanger patient’s safety.20,23 Misconduct of the working procedure may indicate that the procedures to perform tasks using HIT were lacking, impractical, or poorly understood. 24
In addition, the copy and paste habit may result in errors, outdated information, and lengthy documents. Similarly, copy and paste habit issues have been addressed in a study carried out by Holden, 25 who reported that copied and pasted notes do not provide new information, contain redundant copy-pasted information, and made it difficult to know what colleagues were thinking because notes became less meaningful. Hence, copy and paste reduced the quality of notes entry. Aita and Belvedere 26 revealed that a new prescription order generated as copy of previous prescription resulted in errors of over/under dosage, due to failure in updating the dose. Therefore, the copy and paste habit becomes a constraint in the implementation of HIS by posing risks to the safety and quality of patient care. In a more recent study, Tsou et al. 27 showed that 66 per cent to 90 per cent of clinicians regularly use copy and paste. Copy and paste can cause internal inconsistencies, error proliferation, and documentation in the wrong patient chart.
The results from this study are valuable for providing in-depth knowledge of how healthcare practitioner behaviours can influence patient safety and quality of care. However, this finding is characterized by a number of limitations, which need to be considered when interpreting this work. The qualitative data is only from the viewpoint of doctors. Other groups of HIS users, for example, nurses and pharmacists were not considered in this study. Their inclusion may provide broader and more in-depth information to the study. Besides, the findings of this study are purely based on the views of HIS users. No hospital records or evidence of safe practices or patient outcomes was investigated in this study. A combination of observation and document review analysis are suggested for future study to gain in-depth understanding and stronger evidence concerning the healthcare practitioner behaviours towards safe HIS use.
Conclusion
This study provides important practical examples of how healthcare practitioner behaviours could result in unintended consequences of the HIS. The findings of this study help illuminate current challenges to the HIS implementation and provide a platform to better design HIS that is integrated with clinical needs and workflow to support healthcare practitioners in the delivery of quality and safe patient care. Moreover, insights into these contextual issues can help healthcare organizations, healthcare practitioners, and HIS implementers to understand the in-situ operation of HIS in its usage context, and help to design strategies to lessen the number of unsafe HIS adoption and their possible negative consequences.
Footnotes
Appendix 1
Acknowledgements
The authors would like to thank the 31 medical doctors who gave their time to participate in the interviews and the officers of the clinical research centres for their assistance in conducting the interviews.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Universiti Teknikal Malaysia Melaka (UTeM) and the Ministry of Higher Education (MOHE) Malaysia.