
Abstract
This article attempts to define functions and applications of telemedicine and telehealth in order to achieve a simplified and comprehensive taxonomy. This may be used as a tool to evaluate their efficacy and to address health policies from the perspective of the centrality of information in the healthcare. Starting from a lexical frame, telemedicine or telehealth is conceived as a communication means and their action as a communication process. As a performance, the communication is related to the health outcome. Three functions (telemetry, telephasis, and telepraxis) and nine applications are identified. Understanding the mechanisms of telemedicine and telehealth effectiveness is crucial for a value-driven healthcare system. This new classification—focusing on the end effect of telemedicine and telehealth and on the type of interactions between involved actors—moves toward a new and simplified methodology to compare different studies and practices, design future researches, classify new technologies and guide their development, and finally address health policies and the healthcare provision.
Introduction
Dramatic changes in the economic, regulatory, political, technical, cultural, and social environments in which healthcare organizations operate suggest that healthcare providers may need to re-examine their healthcare-delivery approaches for future success and survival. 1
The promise of improved quality, greater and fairer access to care, timeliness of service, shortage of medical personnel, and costs savings in healthcare provision has led to swift development of telemedicine and home-telecare services worldwide.2–7 Today, it is difficult to find a country without an established telemedicine program or plans for developing a telemedicine capability. 8 A commitment to increased utilization of technology in healthcare was announced in the United States 9 and in European Union. 10 Moreover, “technology has become a basic factor determining the quality of the health services.” 11 (p. 79)
Given this, and related significant financial investments, it is surprising that new applications are not rigorously evaluated. 12 Several challenges should be carefully considered before adopting technology: for example, strategic alignment, process management, patient satisfaction, performance measurement, and project management. 1
In the last two decades, several authors13–17 suggested the need of researchers to further explore issues concerning the effectiveness of information and communication technologies (ICTs), especially as a process enabler in healthcare organizations. 1
This demands “innovative and interdisciplinary approaches to address efficiency, productivity, and quality of the health delivery.” 5 (p. 591) However, it is difficult to address the complexity of ICTs systems 18 and make “valid generalizations about the effectiveness […] across disparate health services, technological configurations, and settings,” 19 (p. 317) without a unified classification as the basis for an evaluation framework. Indeed, the lack of a taxonomy limits the full understanding of the scientific and sociological issues impacting ICTs’ use in the healthcare. 20
Previously, ICTs were classified by user, purpose, operating method, type of technology, and field of application.8,21–23 Two of the oldest and most famous criteria relate with the transmission of data:2,4,5,8,24,25 timing (synchronous or asynchronous) and channel (e.g. wireless or wired). Another taxonomy for telehealth 26 considered four categories determining a telehealth encounter: type of interaction, location of controlling medical authority, emergency of care, and timing. More complex and structured classifications8,25 labeled ICTs by clinical and non-clinical practices, diagnostic and monitoring uses, medical specializations, and organizational dimensions.
Nevertheless, a lexical confusion8,27 still spreads in this field, even because of the continuous introduction of new terms (like mHealth or uHealth), often interchangeable and incorrectly used as synonymous.8,27,28 The major reason of such a continuous evolution is probably the technology itself, 6 which has developed rapidly during the last decades in the healthcare sector, as in other fields of modern society. 3 Therefore, while any attempted taxonomy should not be based on a descriptive approach 29 —a technology-based lexicon, simply describing ICTs from a technological point of view, or considering the technological forms of their use (e.g. timing or type of interaction)—it must remain flexible and dynamic 20 at the same time.
The standpoint is that when we don’t know which name we should give to things, and how they are ordered in their relationships, our problem is theoretical. But it has at least two practical consequences: it prevents us from drawing comparisons and adopting repeatable methods in […] research; and it hinders the identification of the most appropriate […] application in healthcare.”
29
(pp. 601–602)
Without a unified, shared classification, we cannot frame the true mechanisms underlying the effectiveness and efficiency of interventions.29,30 We also cannot understand whether the real scope of ICTs is to measure biological parameters, to enhance communication and relationship, or to trigger and to support behaviors. Actual taxonomies do not give us an answer. 29
A basic conceptual framework for a new classification was provided by a previous study. 29 It starts from the core meanings of ICTs lexicon, acquired through an etymological analysis. Before all, it considers a domain (telehealth) and a subdomain (telemedicine), denoting the semantic background that justifies the use of ICTs. Even if there is not a uniform telemedicine application, telemedicine can be conceived as a subset of telehealth.6,31 The prefix tele- implies above all a spatial distance between two actors (doers). (The two actors are not necessarily two individuals. As in the Shannon–Weaver model of communication, in order to perform a communication, we need at least a sender and a receiver. However, each of these two doers can be intended as collective entities. For example, the receiver may be a group of people or a population, as it occurs in media campaigns.) However, a “socioeconomic distance,” for example, a “divide” caused by personal demographics, should be included as well: in this case, ICTs contribute to face disparities and inequalities in accessing healthcare services.5,11,29,31 The point is “a separation of patient and doctor” 6 (p. 575) that is bridged through technology. 6 Because of such a distance, the healthcare action cannot be afforded without the help of ICTs.
An action qualifies both domain and subdomain, characterizing the relation between actors, “two different entities [who] are bearers of consumer and provider roles.” 23 (p. 1108) When performed, the end user (the recipient, for example, a patient or a person without a disease but requiring some kind of assistance) must always be involved directly in the action; in other words, he is necessarily one of the two actors. 29 Even if a patient is lying inside a computerized tomography (CAT) scan, waiting for the execution of a tele-diagnosis, he is a doer: he is contributing to the action because the action cannot be accomplished (the content of the communication, the “image,” cannot be taken nor exists) without him. Moreover, the other actor is always appointed by the health system to attend the action. 29 Therefore, contrary to other taxonomies or perspectives,5,26 medical education, which occurs without a patient as a doer, is not considered here as a form of telemedicine, but rather as a form of tele-education about medicine, for example, the so-called telementoring; 2 it could be said the same of a consultation among physicians or specialists 31 (it does not necessarily involve the patient as a doer) or of an automated in-home monitoring system (it does not necessarily involve a health professional).
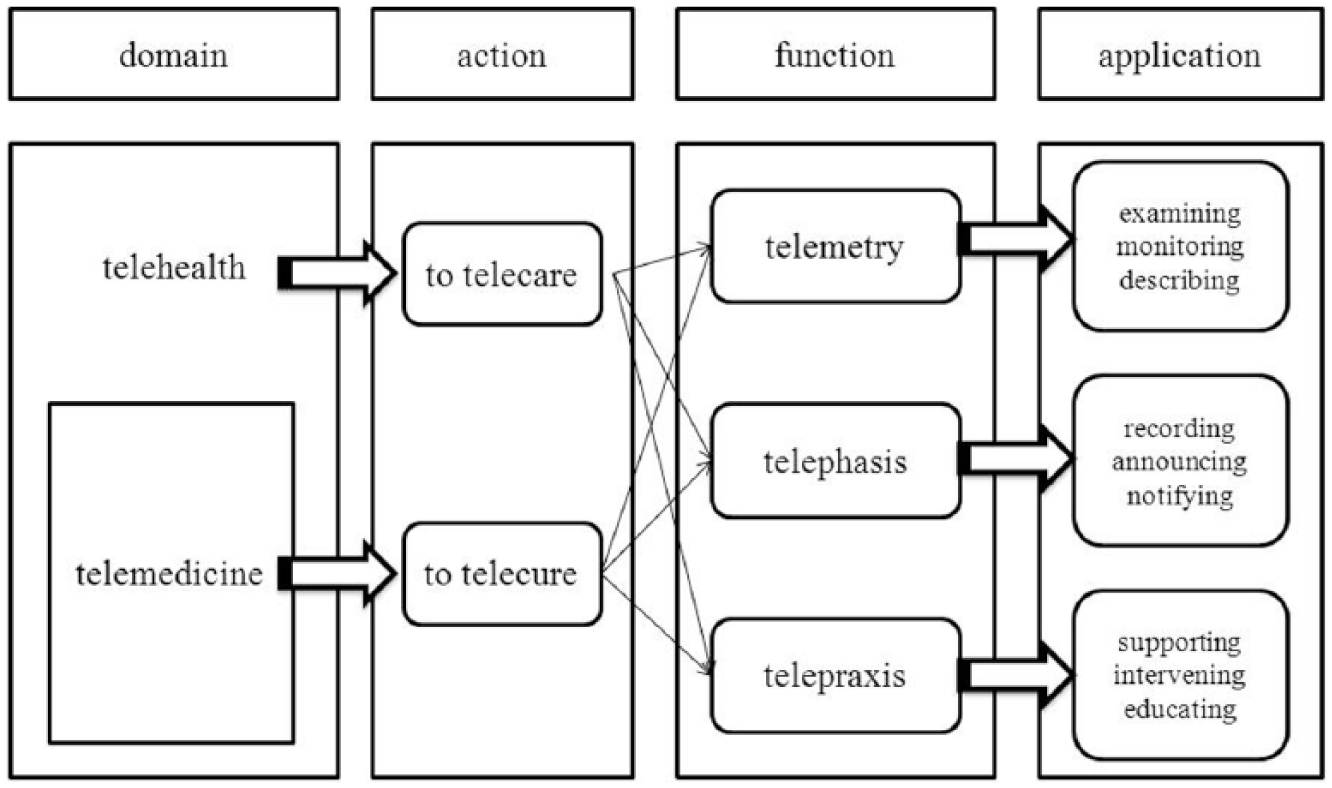
Actions 29 are as follows (Figure 1): (1) Telecare—it occurs when someone advances a generic (health-related) request for assistance. A disease is not necessary to evoke such a request, and the other actor is not necessarily a health professional. (2) Telecure—it characterizes the action of taking charge of a specific problem (a disease). Since it implies a specific expertise (curing, treating, or managing a disease), the other actor must be a healthcare professional. This perspective fits with the idea of “telemedicine as practice of medicine” 6 (p. 575) and is the most common among the definitions of telemedicine in the literature. 6
The classification: domains, actions, functions and applications.
Having established a semantic hierarchy in the lexicon of ICTs, the next step is to define functions and applications for the two actions or, in other words, their operative rules and purposes. In particular, the proposal of this study is the theoretical attempt to pursue a comprehensive classification which may be used to compare ICTs-based programs, achieving an improved evaluation of their efficacy, in order to address new health policies. This perspective is crucial for a value-driven healthcare system: The centrality of information in health systems … means that information and communication technologies (ICTs) that ensure the timely and accurate collection and exchange of health data are likely to foster better care, and the more efficient use of resources.
32
(p. 12)
Methods
Other taxonomies in the medical literature
Before all, classifications or taxonomies for ICTs’ use in the healthcare were searched in PubMed and Google Scholar, using the following keywords in titles: taxonom* (Boolean operator OR) classif*, catalog*, categor* matched with (AND) information technolog* (OR) telemed*, telecar*, telemonit*, telehealth, ehealth, mhealth, telesurg*, teleconsult*, teleadv*, and remote. Also, in PubMed, two Mesh keys were used: “Telemedicine/classification” or “Medical Informatics/classification.” Eight papers4,8,20,21,23,25,26,33 focusing on ICTs classification, or addressing it, were considered.
An etymological starting point
Since words are the structural elements of every taxonomy, the conceptual framework of this classification will start again from the etymologies of ICTs lexicon, as previously attempted in another study: 29 this allow us to find out those intrinsic, non-contingent characteristics categorizing the essentials of ICTs phenomenon.
As mentioned above, the classification will be based on four categories:
Domains;
Actions;
Functions;
Applications.
This scheme finds analogies in the method for building systems already used for ICTs. 34 Since domains have been described elsewhere, 29 here we start from the second category.
The term “action” relates to the idea of motion: it comes from the Latin verb agere, “to do,” literally “to lead, to drive, to carry forward.”35,36 Therefore, we may consider an action as a communication between two actors: it is a communication because it is a shared function, something that is put in common (communis, coming from Latin preposition cum-, “with, together,” and the noun munus, “function, task”).35,36 Indeed, its effect goes from an actor to another.
Instead, a function—from the Latin verb fungor, “carry through, to an end” 36 or “to make a boundary” 35 —may be seen as a relation of any type, that occurs according to an intrinsic property. In mathematics, for example, it is a link between two variables determining the properties of a geometric entity (e.g. the equation of a parabola). Therefore, a function is a rule inherently capable of describing the non-contingent elements that an action owns. In particular, functions are relations developing in a communication process; 37 in the ICTs use, they occurs as the “exchange/sharing of information.”
In this classification, while the operating mode of these exchanges is called “function,” the concrete fulfillment of a function, according to its purpose, is called “application.” In fact, “to apply” indicates precisely to juxtapose two things (from the Latin verb applicare, to “bring into contact”;36,38,39 by extension, “to assign, to attribute”). In the mathematical language, the application would be the co-domain, that is, an element associated with a domain (health or medicine) through a function.
Summarizing, in a given domain, an action is a motion from an actor to another: this creates a relation characterized by a property (function) and a purpose (application).
A matter of communication
Such a conceptual framework, however, relates to the following perspective: what mainly characterizes ICTs is a transmission (the “motion’ we spoke about). Indeed, they remotely deliver a message or an “information by electromagnetic means.” 40 However, ICTs are more than mere means: at a second sight, behind them we can see a real action, a performance; or, better, a process, that is a sequence of aimed actions.
Here, we consider ICTs as activities that integrate, store, analyze, retrieve, or transfer information.41,42 The information processing and the resulting communication are aimed, as we said, they are used for problem-solving and decision-making in the healthcare sector,5,43 for example, in order to generate knowledge, manage healthcare, or to make an event possible (an intervention, a medication, etc.). That is to say that the communication, in this situation, is strongly related to an outcome. Therefore, understanding the communicative aspects of ICTs in the healthcare sector is probably the key in determining their success
5
or, in other words, their effectiveness. As previously noticed, ICTs are used to support the provision of health care services—that is, to support communication … [In order] to reach that goal one must first understand what the communications are, and which related clinical tasks are actually involved in health care delivery process.
44
(p. 30)
Given such premises, and moving beyond the etymological analysis, ICTs can be conceived essentially as a communication strategy for sending messages remotely: because they perform an information exchange between a sender and a receiver, and in order to analyze them, we need to focus on the underlying communication process. Consequently, functions will be conceived as the communication rules of the actions, and applications as the concrete finalization of a single communicative act through ICTs.
For communicative functions, three levels 45 are identified, depending on the degree of complexity of related transmission:
Integrated data. Raw data have “no intrinsic meaning when standing alone.” 43 (p. 361) However, they can be composed according to rules that specifying relations between signs (syntax) make them intelligible. A typical “data only modality” 5 (p. 593) of communication is telemonitoring.
Meaning. A meaning is attributed to the integrated data, according to the relation between signs and their designated objects (semantics). This happens when “data are endowed with relevance and purpose.” 46 (p. 129)
Behavior. It occurs when the meaning of the data comes into a relation with a human interpreter (pragmatics), eliciting a performance.
The usefulness of this frame relates with the idea that the assessment of the efficacy of ICTs in the healthcare should discern between the mere information level and the level where we may find a modification of a condition—a health result or a health behavior. 33
Results
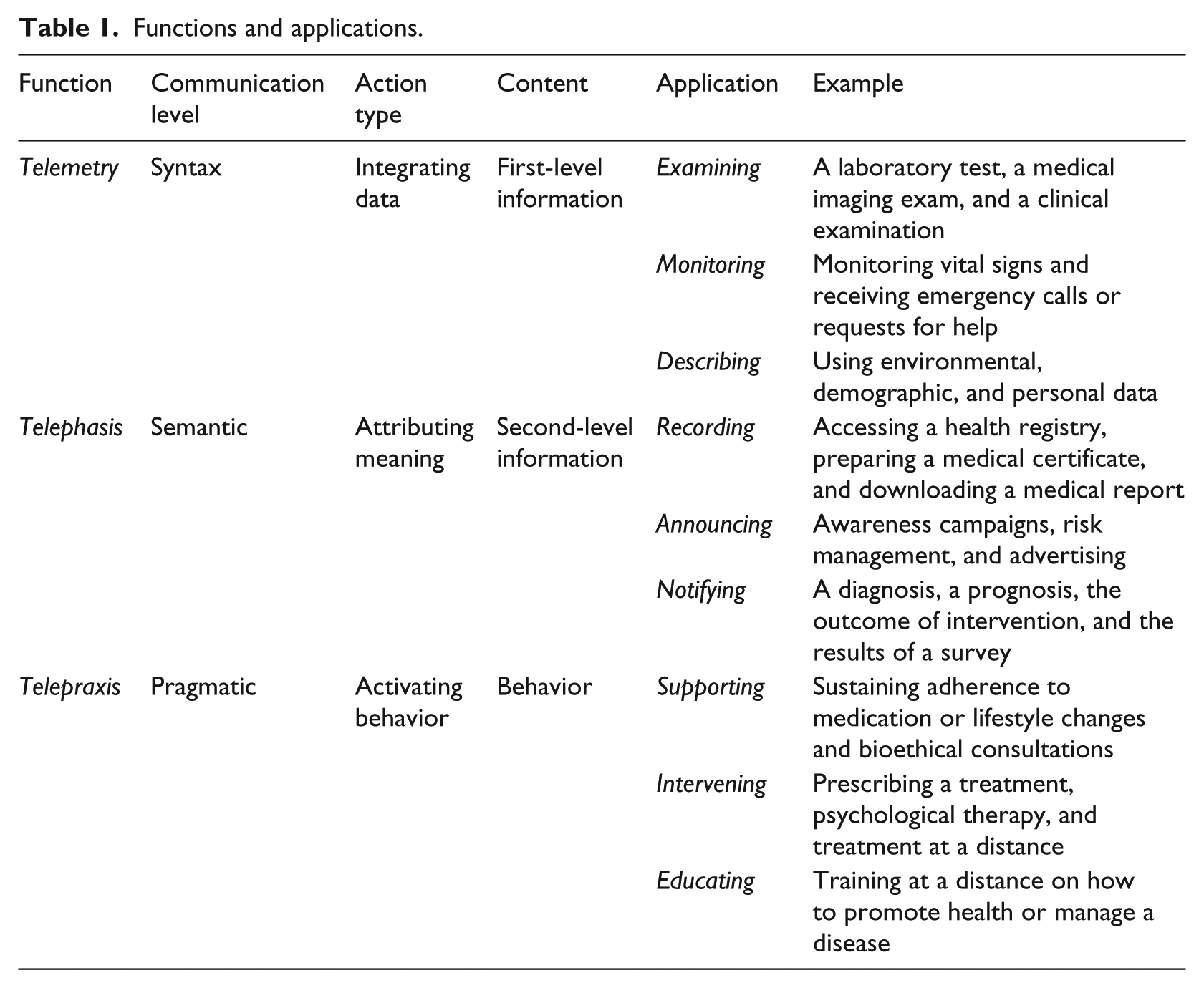
In this proposal, a specific function encompassing all possible remote applications for the communicative act is defined for each level of a communication process (Table 1). The three functions are given as follows (Table 1):
Telemetry (from Greek, tele- + metron, “measurement at a distance”).47,48 This function integrates simple data according to pre-established rules, so a first-level information is collected and transmitted. It encompasses activities such as monitoring, collecting a medical history, completing a questionnaire, and performing a CAT scan. The first step of a medical (or a healthcare) practice is collecting data, in order to address the cure/care action. Data are provided to generate knowledge. Also, we may consider a single or a continuous collection of data and their whole framing and organizing in a complex net of relationships. Related applications are therefore as follows:
Examining. In Latin, an examen is the “tongue of a balance,”35,49,50 so this term expresses the attempt to test and quantify data. Monitoring. This term is chosen because of its common sense in the healthcare field: “to check for, to control, to oversee.” In Latin, a monitor is properly “one who reminds”
49
(p. 996) an adviser.
36
Describing. In the sense of “to draw, to mark, to describe,”36,50 to portray entirely an environment, an individual, a population.
Telephasis (from Greek, tele- + phasis, “to declare, to make known, to show at a distance”).47,48 From previously gathered data (first-level information), this function generates a more complex and meaningful second-level information. Information is generated in order to be recorded, indifferently spread to some recipients, or transmitted to the recipients who have intentionally asked for it. Related applications are as follows:
Recording: through this action something can be remembered, recalled to mind.36,49,50 This includes several administrative applications.
2
This application is mostly focused on registering, storing, and retrieving information. Announcing: literally, “deliver a message to.”36,50 Here, for example, information is used to raise awareness in the population, through a media campaign. This application is mostly focused on spreading information. Notifying: literally, “to make known.”49,50 For example, in this case, information is used to express a clinical evaluation or a diagnosis. This application is mostly focused on the comprehension of information that is relevant to the end user, because it is the outcome of the healthcare assistance he requested.
Telepraxis (from Greek, tele- + praxis, “accomplishment, activity, practice from a distance”).47,48 This function uses the first- and/or second-level information to trigger and develop behaviors, to maintain them, or the transmitted information is the behavior itself (as discussed above, there is a correspondence between communication and performance;
37
in the healthcare system, this clearly occurs when the communication performs an intervention, for example, in telesurgery). Related applications are as follows:
Supporting: from the Latin supportare, “to carry near,”49,50 to convey tailored information in order to sustain and give positive reinforcement to behaviors,
51
for example, periodic messages about a healthy lifestyle. Intervening: literally, “to come between, interrupt.”49,50 It denotes an act or an event that change the natural course, and thus the outcome, of a condition or a disease (e.g. prescribing a treatment during a videocall, or remotely schedule a medication and release it through a delivery unit). Educating: literally, “to bring out,”36,49,50 “nurture.”
35
It is the act to train and empower individual or communities—developing knowledge, skills and capability to use healthcare services—in order to improve health.
52
Since telemedicine is a subset of telehealth, some functions relate to both, while others are specific: for example, telemetry can be used to monitor the progresses of a health promotion program (telehealth) or the progression of a disease (telemedicine); healthy people as well as patients may require a health/medical certificate (recording, telephasis), but prescribing a medication at a distance (telepraxis) is specific to telemedicine. Obviously, in all these functions, one of the actors must always be the end user.
Functions and applications.
Summarizing, the last structural elements of this new classification are (Figure 1) as follows:
Three functions: telemetry, telephasis, and telepraxis.
Nine applications.
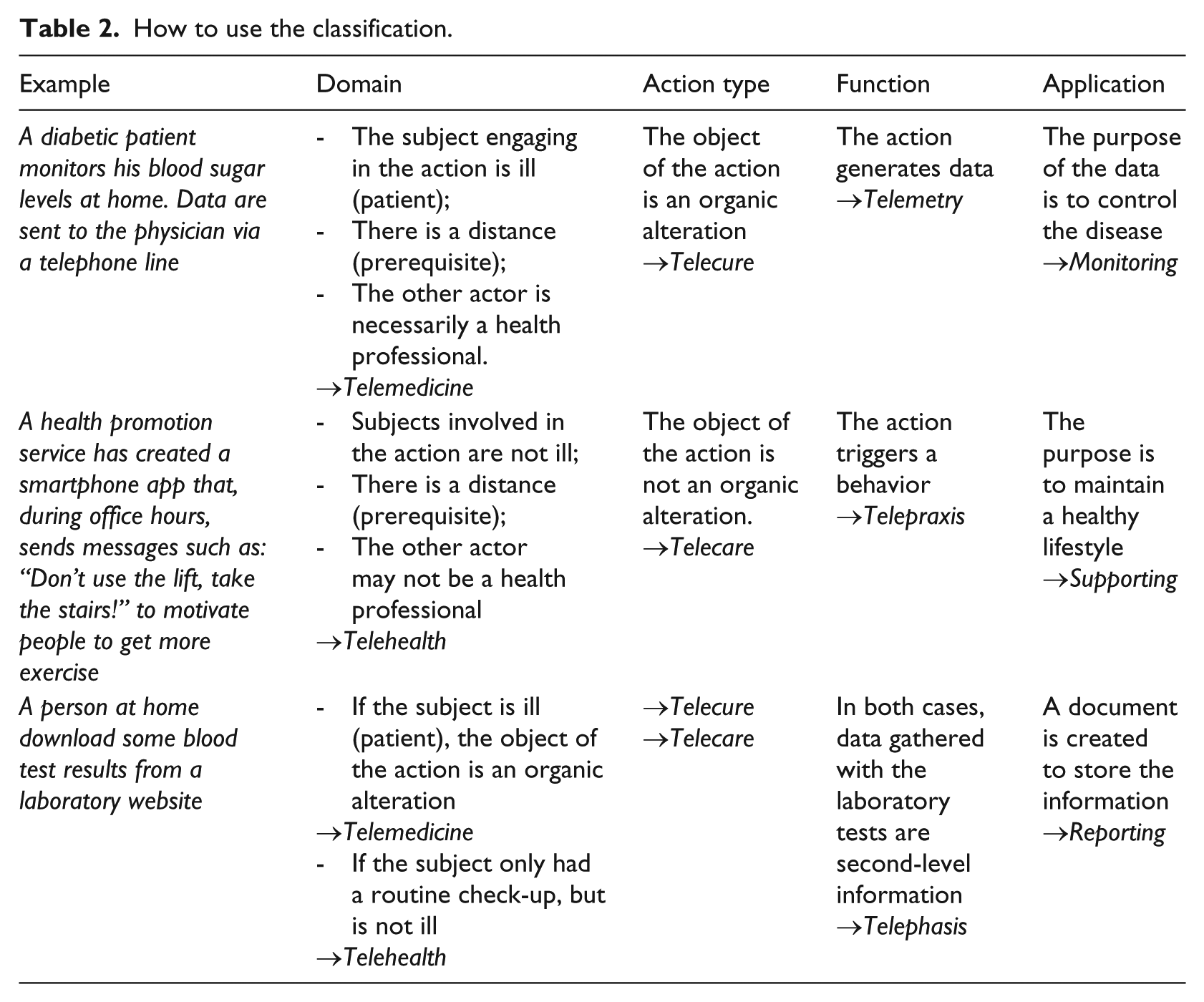
Table 2 shows some examples about how to use the classification.
How to use the classification.
Discussion
Framing eHealth
The term eHealth was deliberately not included, because it is the paradigm of a lexicon describing a phenomenon from a merely technological perspective. 29 This term comes from merging “health” and “electronic.” An electric circuit only carries electricity to power or actuate an activity. An electronic circuit (a type of electrical circuit), because it processes electromagnetic informative signals, performs a communication activity.53–55 Thus, a washing machine is electric and a smartphone is both electric and electronic. The term eHealth denotes everything capable of generating health-related information by electromagnetic means.
In the scientific literature, eHealth characterizes virtually everything computer related. 56 It is like the other “e-words” (e-commerce, e-mail) used to describe Internet application, 56 as Internet expanded in the late 1990s—the term eHealth came into use in the year 2000, 57 and the World Health Organization (WHO) approved its eHealth resolution in 2005. 58 Even one of the best-known definitions of eHealth—“intersection of medical informatics, public health and business, referring to health services and information delivered or enhanced through the Internet and related technologies” 56 —implies the ICTs use in the broadest sense.57,59
According to another definition, telemedicine is one eHealth-specific application. 11 (p. 80) Probably, eHealth is a hyperonym encompassing both telemedicine and telecare. 57 But, if eHealth “refers to all forms of electronic health care delivered over the internet,” 2 (p. 31) and telemedicine is something related to a professional, 29 eHealth could be driven by non-professionals, 2 including patients themselves58,59 and also businesses and consumers. 2
A systematic review 60 identified 51 different definitions of eHealth and no clear consensus on its meaning. However, two common themes emerged: health and technology. The former was mainly used to discuss the health service delivery, or the care process (it is related more to services and systems than to individual’s health). Wellness was seldom evoked, and only one in four definitions focused on outcomes such as cost-effectiveness and efficiency. So, eHealth refers to “health care as a process rather than to health as an outcome.” 60
If eHealth is seen as a way to use Internet in the health sector, the word is merely a descriptive term identifying a communication channel or a technological means. In this case, it stands out of this new classification. 29 But if it identifies the use of “electronic technologies” in a broader sense and if (1) it is linked to health as the whole health sector, “health as a world” (systems, processes, organizations, as well as specific caring and curing activities) and (2) it does not necessarily depends on the concept of “distance” (tele-), then eHealth should actually be understood as the greater hyperonym to which telehealth and telemedicine belong, and with which they share a communication activity. 57 In this sense, this word describes all the actions that telecare and telecure encompass and some actions that they do not encompass, when
There is only one actor, the end user, for example, an individual seeking health information through Internet.
No end user is involved in the action, for example, a consultation between two health professionals or a surgical intervention in which one surgeon gives another surgeon instructions (tele-/e-consultation) and academic lessons (tele-/e-training, tele-/e-learning, tele-/e-conference).
The two actors are both end users, for example, exchanges of information within a social support groups or a virtual community.
The two actors are a patient and a physician, but there is no distance, for example, during a face-to-face anamnesis, the physician records the clinical history on a tablet (this may be defined an “e-medicine” application).
Information comes from impersonal actors, for example, monitoring air pollutants, an engineer collects data remotely by means of sensors.
For all these reasons, the term eHealth was not included: it is only indirectly linked to the concept of health, as previously discussed, 29 and it does not necessarily implies a distance, nor an end user.
Why do we need a new taxonomy?
The first argument is simplification. Although this classification introduces new terms (Figure 1), it is based on 16 “words” (17 if we include the prerequisite “tele-”), encompassing both telehealth and telemedicine. The most developed taxonomies we considered uses 158 or 1425 elements to classify only telemedicine (the former provides three additional domains—telehealth, eHealth, and mHealth—each owning four elements). So, we found a more comprehensive simplified structure that works following a linear, hierarchical, one-directional flow, while other taxonomies are three-dimensional.
Second, this classification will ease comparison between different studies and various ICTs practices. It is an urgent need to compare trials with a rational, orderly, and reproducible method. Published studies present interventions with a high variability of components. Reviews usually group and compare them using a common contingent element (e.g. a disease, a technology, and a content); however, this is an empirical strategy, applied without considering critical components as actors’ involvement, type of performed action, and underlying mechanism. As long as we compare studies relying on descriptive elements, it is hard to understand why an intervention is effective. For example, trials are often described focusing on technology, as it was effective by itself; instead, we should analyze them examining what technology makes happen61,62, the communication process (i.e. the interaction between actors) that ICTs allows and strengthens (Table 1). This classification goes beyond the communication channel or type of technology involved: if we consider a behavior supported by a text message, an app, a telephone call, or an e-mail, these different means all imply the same communication process, the telepraxis function. If a medical report is sent by e-mail, but is received and read on a smartphone, it is not a matter of eHealth or mHealth: despite the combined technologies, a common purpose classifies the intervention as a recording application (see Tables 2 and 3 for further examples). We can also compare ICTs regardless of setting. For example, it is useless to distinguish between home-provided or workplace-provided telecare, as some papers claimed: 63 the setting, like the demographics of the actors involved, is a contingent element. It may influence the efficacy of the action, but it does not qualify the action itself.
New methods to compare ICTs-based interventions.
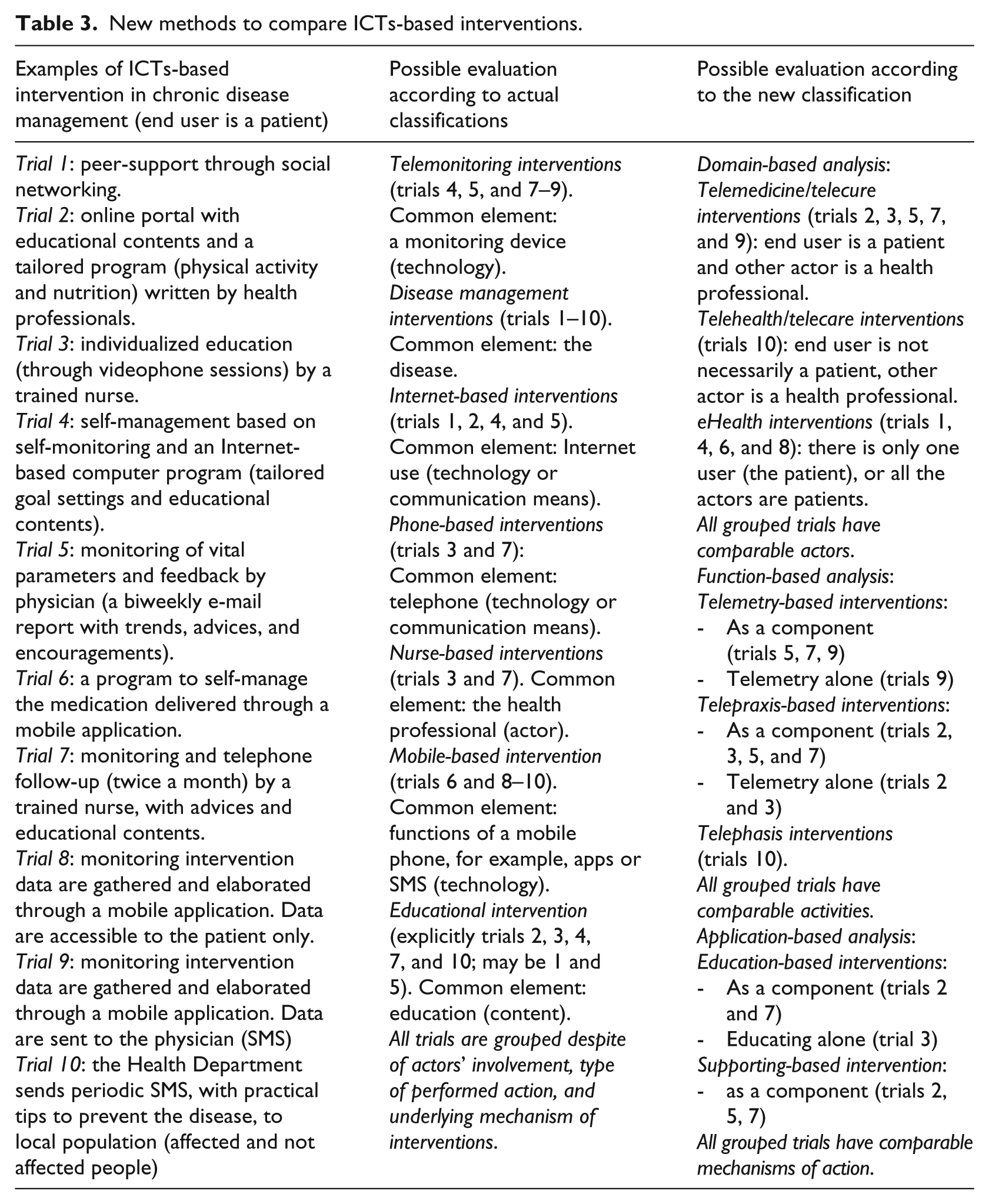
The third argument is the chance of a new methodology, a framework that may “be used as a reference for evaluation studies.” 33 (p. 191) Because the need to understand the true mechanisms of effectiveness should be the main aim of research on ICTs, this classification may guide in designing trials and reviews, focusing on the end effects (application) and on the type of interactions between actors (functions). Indeed, other methods (Table 3) compare interventions with different components, each of them potentially affecting outcomes, with a loss of information and the risk of confounding. Such a new proposal provides a more detailed analysis degree, because it examines an intervention discriminating its underlying process separately and progressively, limiting or avoiding overlapping, but allowing different combination of categories (components) to form “complex networks” 33 of ICTs-based interventions (see Table 3):
In domain-based analysis, grouped interventions have comparable actors.
In function-based analysis, grouped interventions have also comparable activities (here, the focus is on the type of action performed, that is, the dynamics of interaction between actors).
In application-based analysis, grouped interventions have comparable mechanisms of action (the focus is on the purpose of intervention, the pursued effect).
Finally, assessing ICTs under an “actions and functions” perspective may allow to identify more accurate indicators for measuring outcomes, leading to an improved decision-making process when planning an intervention is crucial.
Once clarified the role of functions and applications in affecting effectiveness, further research may address the role of other components as setting, target, organizational model, and patients’ and providers’ perspectives. This study does not intend to address this topic: if anything, such an objective will be the next step of our research; moreover, in another study, our aim is to show the effectiveness of this new taxonomy in reviewing telemedicine and telehealth applications.
At present, therefore, we hope that this new approach will help researchers in developing more studies and evaluations on this topic and clinicians and health providers in making decisions about which telemedicine or telehealth intervention is the most suited to implement, according to the action and the purpose they pursue.
Some other theoretical issues
As previously discussed, 29 the opposition between health and medicine 8 is solved, and the latter is integrated in the general dimension of the former.
The lexical reduction was achieved at the expense of some words often used in the medical literature. It seemed inappropriate to include contingent terms such as “mHealth.” Technologies change faster than concepts like health and medicine, so merely descriptive terms should not be considered as structural elements in a taxonomy. If new ICTs (or new medical specialties) will be invented and introduced in the future, this classification may be flexible enough to accommodate them, without adding new categories. Historical terms, such as telemonitoring, may be included in the classification according to their function and purpose (for telemonitoring, these are telemetry and monitoring, respectively), but only as descriptive terms, not as categories.
The greatest limit of any classification based on words lies in the words themselves. This classification is grounded in a Greek-Roman or English lexicon, and it may not be adaptable to other cultures or languages. 29 This can pose a challenge, as already identified for the general use of ICTs. 64
Conclusion
In this new classification, telehealth and telemedicine are qualified as a communication strategy involving an action (to care or to cure) taken remotely. This action has three main functions, corresponding to the level of complexity of the communication process.
The terms telemetry, telephasis, and telepraxis are introduced to describe such functions, each further defined by applications and their specific purposes. The stability of the new classification depends on the stability of the meanings of its words. The structure is built on a logic pathway, proceeding from core meanings to purposes: thus, the ICTs phenomenon is theoretically justified and not only described from a technological perspective. It analyzes the underlying communication process, that is, the action itself, and therefore is related to the health outcome: this allow to better evaluate the ICTs’ effectiveness. Finally, the simplified comparison of different ICTs-based practices will be useful for further research in order to address health policies and the healthcare provision, classify future ICTs, and guide their development for a better response to the health need.
Footnotes
Acknowledgements
The authors thank Tim Kaywort for his valuable support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.