
Abstract
Health self-management has become a new trend in healthcare management due to its effectiveness in improving patient health, quality of life, and life satisfaction and simultaneously reducing the cost of care. To evaluate the potential of mobile health, we developed an online health self-management system for mobile or desktop environment to help patients self-manage their health in home settings. Certain elements (e.g. education, entertainment, and rewards) were built into the system to encourage patients to both adopt and continue using it. The system was shown to two groups of patients: an Internet-panel group of 198 patients with one or more serious chronic illnesses and 83 peripheral arterial disease patients in an in-person study group. A statistical model based on Unified Theory of Acceptance and use of Technology in a consumer context was used to analyze the results. The results from both groups confirmed that such systems, from the perspectives of patients (in a “pre-use” stage), are useful, beneficial, and rewarding to use.
Background and significance
According to many sources,1 –3 self-management for chronic conditions implemented correctly is capable of reducing hospital admission and readmission, improving patients’ quality of life, elevating the level of life satisfaction, and reducing care costs. It is psychologically, socially, and financially beneficial for patients to self-manage their health.
Among many published studies of online health self-management support, few have evaluated patient adherence or intervention sustainability. A systematic review of mobile healthcare (mHealth) interventions for cardiovascular disease self-management 4 found that only one of seven intervention studies lasted as long as 1 year. A systematic review of 107 studies of adherence to mHealth tools 5 found that there was mixed evidence of effectiveness, and more research was needed. Our research is specifically oriented toward health self-management sustainability, with the goal of chronically ill patient acceptance and continuing use of online tools.
Strategies for implementing self-management include the following: (1) self-management targeting behavior change, (2) advice-giving interventions, (3) education/training interventions, and (4) motivational approaches. 6 mHealth technology can play a major role where mobile devices such as tablets, smartphones, and laptops can support collection, storage, and transmission of health data, and real-time monitoring and self-care of patients. 7 A recent survey found that technologies US adults aged 18 or older use to manage their own health include websites (56%), smartphones or tablets (45%), and wearable technology (33%). 8
For our study, an online support platform for chronic conditions was developed, with both mobile and desktop versions. To support self-management strategies through a patient-centered approach, support and sustainability elements were included. Healthcare support elements include (1) education and training: online or face-to-face; (2) decision support: to help patients handle daily decision-making tasks; (3) family and community support: through family care partners; and (4) patient self-monitoring tools: to monitor symptoms and conditions. Sustainability elements to promote their continuing use of the system include (1) entertainment: videos, games, and so on; (2) patient rewards system: patients can accumulate points by system use; and (3) online social network forums: to socialize with other patients.
All data collected in the study reported here were from patients in the “pre-use” stage. This helps to predict acceptance of a system but does not include results from actual users. In a forthcoming study, a 12-month randomized controlled trial (RCT) will test an advanced version of the system. It will involve 200 outpatients with peripheral arterial disease (PAD). One hundred intervention participants will use an advanced version of this system that includes more content, functionality, and mobile devices, and there will be 100 usual care patients. The RCT will assess the relevance of each of the system elements to patient self-management. If this research study shows significant outcome improvements, clinical certification of the system will be sought.
Objectives
The objectives of this study are (1) to describe briefly the relevant functionalities of the online health self-management system and (2) to report on a statistical model analysis of feedback obtained from chronically ill patients who interacted with online functionalities of the system.
The following sections provide a brief review of self-management, its components, issues, and barriers. Then, the health self-management system is introduced, along with an adapted Unified Theory of Acceptance and use of Technology in a consumer context (UTAUT2) 9 statistical model of relationships among the functionalities. A statistical analysis of results collected from two groups of users is presented, along with discussion and conclusions.
Patient health self-management support
Health self-management support is a complex task (see Figure 1) that has four internal components: 10 (1) self-monitoring, (2) self-care, (3) adherence, and (4) decision support. There are three external components that can help support and sustain patients: (5) family and community support, (6) education and training, and (7) sustainability elements (entertainment, social network, etc.). Figure 1 is a conceptual model that demonstrates those components and their relationships.
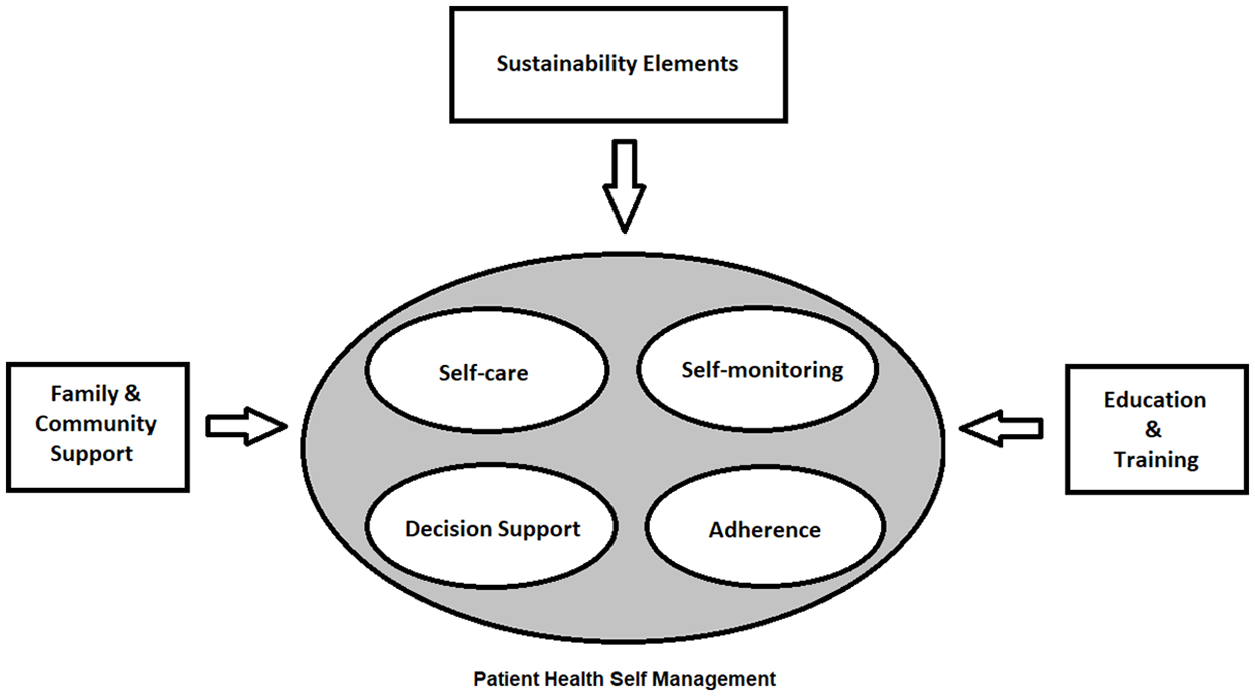
Patient health self-management support—a conceptual model.
Health self-management
Health self-management is what individuals can do or what community and family can do to support them on a regular basis, to feel better and pursue the life they desire. 11 Self-management support is how an individual can use support systems or how family members, care providers, and others can support individual self-management. 11
Self-care
Riegel et al. defined self-care as “a naturalistic decision-making process that patients use in the choice of behaviors that maintain physiological stability (symptom monitoring and treatment adherence) and the response to symptoms when they occur.” 12
Self-monitoring
Self-monitoring is defined as
the continuous and ongoing assessment and monitoring of the symptoms of a certain health condition (problem or disease), as well as other important factors (such as weight, sleep, etc.) at any place other than a clinic (e.g., home, workplace, etc.) by patients or their care partners (possibly a family member).
13
Adherence
Adherence is defined as the degree of a patient’s compliance to medical advice, consumption of medications, correct use of medical devices, self-care, self-monitoring, self-directed exercises, or even going to regular therapy sessions. 14
Decision support and health decision support systems
Decision support in the health and clinical context can provide clinicians, staff, patients, or other individuals with knowledge and person-specific information, intelligently filtered or presented at appropriate times, to enhance health and healthcare. 15 A health decision support system (HDSS) compiles useful information based on raw data, treatment guidelines, acceptable ranges for patient vital signs (heart rate, blood pressure, blood sugar, etc.), and other status indicators (bodyweight, etc.) to help patients make better decisions. 16
Family and community support
Active involvement of at least one family member as a care partner in the disease management and treatment process can be the key to achieving successful psychosocial interventions. 17 Community network support (relatives, friends, etc.) can also be an important factor in helping to support chronically ill patients, 18 including improved patient dietary behaviors. 18 Help and support of a family care partner as well as the community can assist in the achievement of treatment goals.
Education and training
To self-manage a chronic condition, patients make many daily decisions and perform complex care activities specialized according to the disease(s) afflicting the patient. Education and training include knowledge, skills, and abilities necessary for self-management, self-care, and self-monitoring, as well as any activities to assist patients in implementing and sustaining the behaviors needed to manage their conditions. 19
Sustainability of the intervention
Patients must be willing to adopt health self-management system use, and they must be strongly motivated to continue with its use. Sustainability is defined as “the continued implementation of a practice at a level of fidelity that continues to produce intended benefits,” becoming a desired goal for successful disease intervention or prevention 20 (p. 179). Sustainably adhering to treatment plans, 21 through at least one element of chronic care model (CCM), 22 has resulted in significant positive effects on quality of care.
Users often lose interest in adhering to treatment regimens. 23 To assure sustainability, both intrinsic and extrinsic motivation must be fully engaged. “Intrinsic” motivation is driven by an intense involvement and interest in the activity itself. “Extrinsic” motivation is driven by the desire to achieve some specific external reward which is apart from the activity itself, such as deadlines and money. 24 Sustainability requires that patients must receive positive motivation whenever they interact with the system. Motivation to continue should not depend solely on healthcare benefits that patients receive, since this is an intrinsic motivation that might not be strong enough to encourage continuance. Extrinsic motivation appears to work in some cases—for example, by providing patients with small rewards for continuing. 25
Online social networks
A recent systematic review 26 suggested that social media has promising outcomes for self-managing chronic conditions.
Entertainment
Health games can have an impact on the cost, effectiveness, and availability of both preventive and remedial healthcare and well-being. 27 Playing recreational games and getting in contact with friends often promote adherence and long-term sustainability of patient self-management programs. 28
Patient rewards
A reward system that motivates patients to keep using a system that promotes positive lifestyle changes can stimulate continued use, leading to sustainable outcomes. 29
System features and functionalities
Our initial system was developed and tested using guidelines for Class II medical devices. 30 Figure 2 shows the landing page of the original system on a desktop computer.

System desktop landing page.
Differences among patient capabilities, abilities, and disabilities may be considerable, especially for older patients. Some patients may also suffer from multiple chronic conditions. All these factors were considered in the design of the system. The system enables the patients to securely collect, store, review, manage, or share their health information with whomever they wish (typically their physician and family caregivers). Figure 3 demonstrates the flow of data from and to the participants.
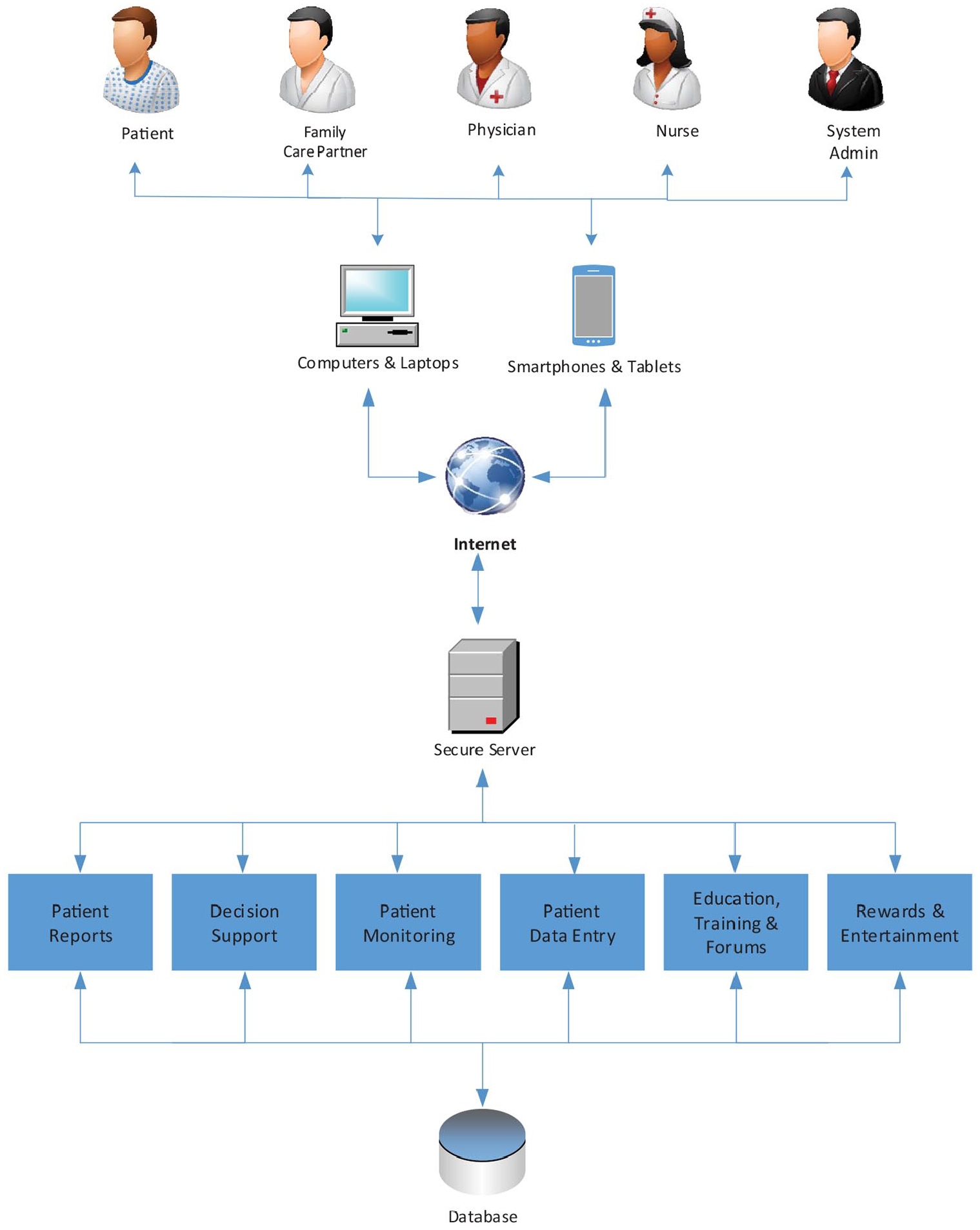
System feature overview.
The system will
Keep patient records online centrally, with 24/7 access;
Track and help patients manage condition(s) and symptoms;
Provide tailored advice for healthy diet and exercise;
Provide access under patient control for chosen care partner(s) and physician(s);
Allow patients to socialize with other people with similar condition(s);
Raise the patient level of knowledge about their condition(s) through education;
Entertain patients with recreational materials;
Accumulate points for users, exchangeable for gift cards.
A patient-centered system approach
Patient-centered care is defined as “a quality of personal, professional, and organizational relationships.” 31 For a system to be patient-centered, patients, their families, and care partners must play an integral role in designing the system.32 –34
System overview and specifications
Stakeholders
System stakeholders include the following:
Patients: They are given access to their personal health records (PHRs) to input all monitoring data and view status and outcome measures. They will access system decision support functionality and sustainability components.
Care partner(s): Voluntary care partners (children, spouse, close friends) will be regularly in touch with patients in some specified capacity.
Care providers: They may use the system to monitor the progress of their patients but will also see patients at regular appointments.
System administrator(s): They monitor and manage the system.
System menus and functions
The system provides secure access to several menus and functions: (1) patient profile (created and maintained by the patient); (2a) all patients: patient monitoring (blood pressure and heart rate, exercise, pain level, weight, diet); (2b) specific patients: blood glucose, smoking. Reports, graphs, and charts can be displayed from all these functions. Figure 4 shows an example patient access page, in this case used for entering data and displaying their history of heart rate and blood pressure.
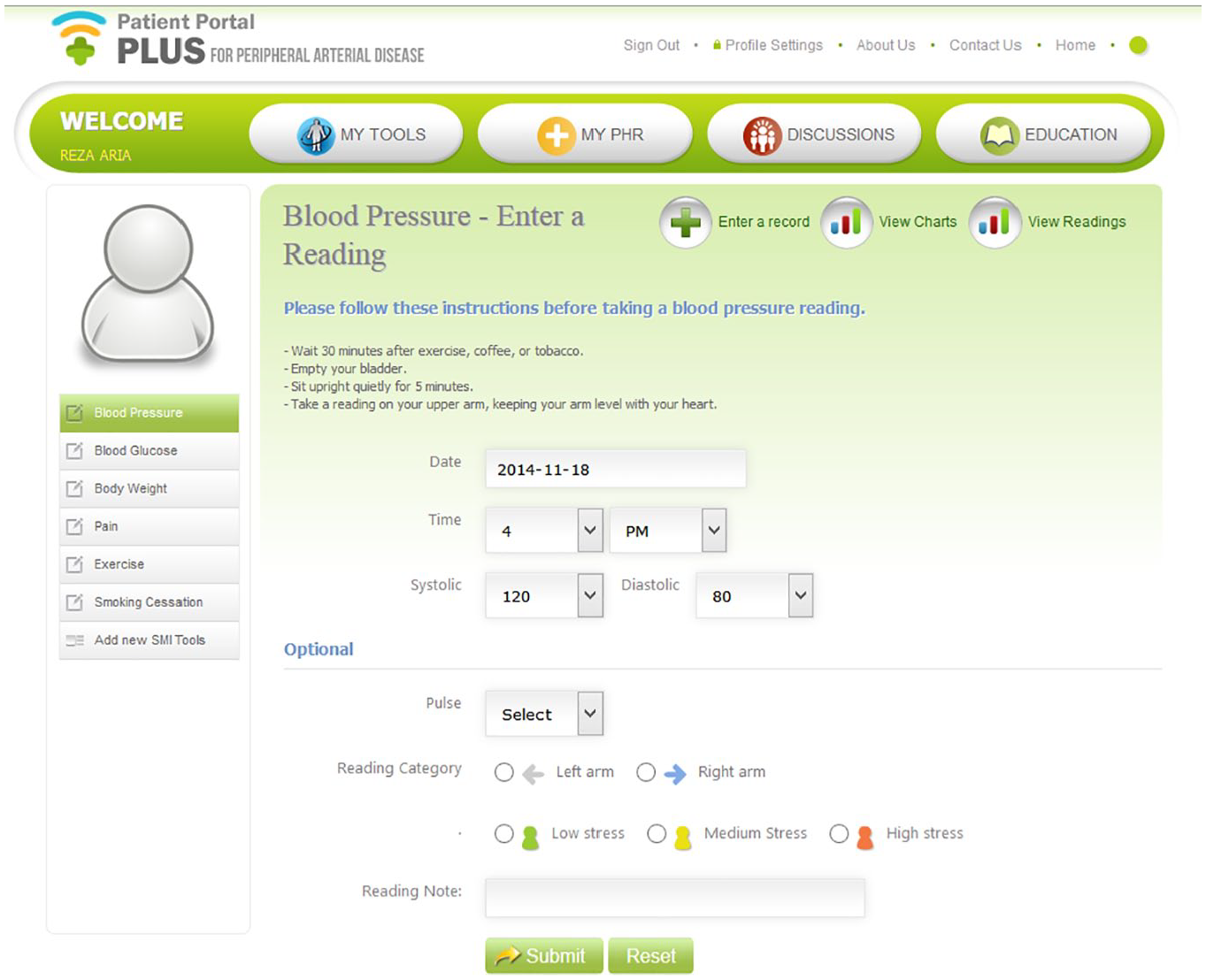
Blood pressure and heart rate entry.
Education
Multiple studies have provided an abundance of evidence that patient support programs (including educational programs, training, short courses, etc.) are essential in elevating the level of patient adherence to the prescribed treatment regimen, as well as clinical and humanistic outcomes. 35 In our system, educational programs are available online for patients and their care partners to understand the nature of illnesses and their treatment. Online training is available online to empower patients to deal with their tasks. Short courses will be available online in such areas as treatment, medication, symptoms, and managing symptoms (under development). The short courses will focus on both patients and their care partners separately. For care partners, the focus is on (1) educating them on how to treat their patient partners and support them emotionally and (2) the condition(s) that their partners have (e.g. its nature, symptoms, effects on patient daily lives). For patients, the focus is on (1) becoming educated about their own condition(s) and (2) how to effectively manage their own conditions.
Forum
A managed forum is available so that patients can exchange experiences and socialize.
Decision support and guidance
The decision support system (DSS) will render guidelines, offer specific options when a decision is supposed to be made, provide suggestions for exercise and diet, and generate plots for patients and their care partners, using color-coding for each situation. White, yellow, and red zones will represent acceptable, high risk, and critical conditions, respectively. Boundaries will be set by care providers, according to specific patient conditions. The system will warn the patient, or care partner, to contact physicians or emergency services in case of emergencies. Figure 5 shows a sample of how this DSS might work.

Blood pressure and heart rate plot for several days.
My conditions
Patients can add time-stamped notes about their current conditions.
Statistical model development
UTAUT2 was used to create a structural equation model (SEM) of the system. For testing user perceptions, some UTAUT2 constructs did not play a role. 36 Facilitating conditions and social influence, two contextualizing constructs of UTAUT2, 37 were dropped. The reason was that data were being collected in the pre-use stage and we did not want to introduce any type of facilitating factors to avoid affecting user perceptions about such factors. Social influence and habit constructs were dropped since participants did not have any prior experience with such a system. The price value construct was dropped since participants were not informed about service pricing. Age, gender, and experience are also considered to be moderators in the model.37 –39 These revisions ensured proper model contextualization and face validity of the study. 40 The simplified UTAUT2 model in the SEM form is demonstrated in Figure 6. Table 1 shows the definitions for each model construct. 36
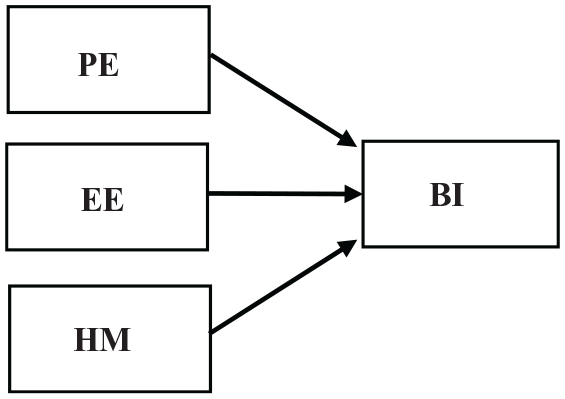
Simplified UTAUT2 model. 36
Construct definition. 36
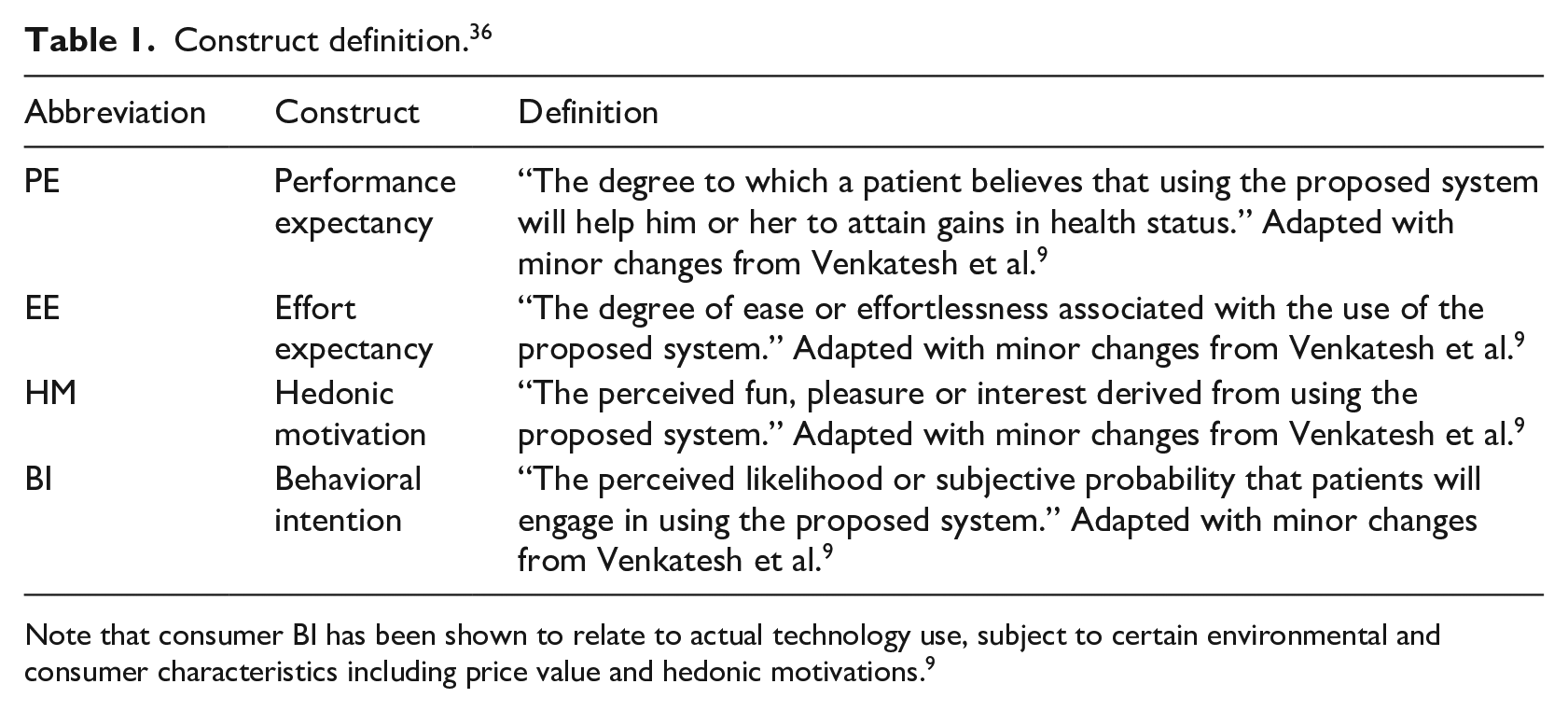
Note that consumer BI has been shown to relate to actual technology use, subject to certain environmental and consumer characteristics including price value and hedonic motivations. 9
Methodology
A 9.5-min video clip describing the initial version of the system was produced to introduce it to potential users. The video tells viewers “what the system is?”, “why has it been built?”, and “how does the system work?” (or in simple terms, how it helps them), through narrated text, pictures, and animation. 36
Two sets of data were collected, from an Internet-panel group and an in-person group (employed using a simple random sampling method), 41 after they viewed the video, through an online questionnaire. Both studies were approved by research ethics boards. The Internet group study tested user perceptions toward the system, including shortcomings or lack of interest from users. The in-person group was recruited over a period of 12 months from PAD outpatients arriving for regular appointments at a vascular clinic.
Sessions for each person in the study groups began with demographic questions, followed by 13 statements on health self-management, answered on a 5-point Likert-type scale. After viewing the short video, participants answered 27 statements about the system and how it might help patients, also on a Likert-type scale. This was followed by four open-ended questions where participants could express their opinions about system improvements, including the following:
“Do you think you would be interested in starting to use the system that was just demonstrated to you? Please tell us why.”
“Do you have any suggestions for making the system more interesting, more useful, easier to understand, or easier to use?”
“Do you think you would be able to find time to access the system at least once a day on a regular basis? Please explain how.”
“Do you think you would be interested in using the system over a long period of time? Please explain your decision.”
The purpose of having these open-ended questions is to provide additional insights and thereby enrich the quantitative results. Responses to these questions were studied in terms of demographics and summarized in terms of the reasons provided for using or not using the system. Partial least squares (PLS) with the SmartPLS software package was used to analyze the data and evaluate the model 42 from each group. For each model, R-squared (R2), 43 PLS path estimates (β), 43 effect size (f 2), 43 predictive relevance (Q2), 43 and finally, goodness of fit (GOF) 44 were calculated. Data collected were pre-use, and the focus was on the perceptions of participants toward the system.
Results
Internet-panel group
A commercial research firm drew a random sample of 204 patients, including females and males suffering from at least one type of serious chronic disease, from their North American database. Each patient was compensated by the firm for participation. Six cases were either incomplete or their responses were contradictory and were removed, resulting in 198 valid completions (104 males and 94 females). Demographics of this group appear in Table 2.
Internet-panel demographics.
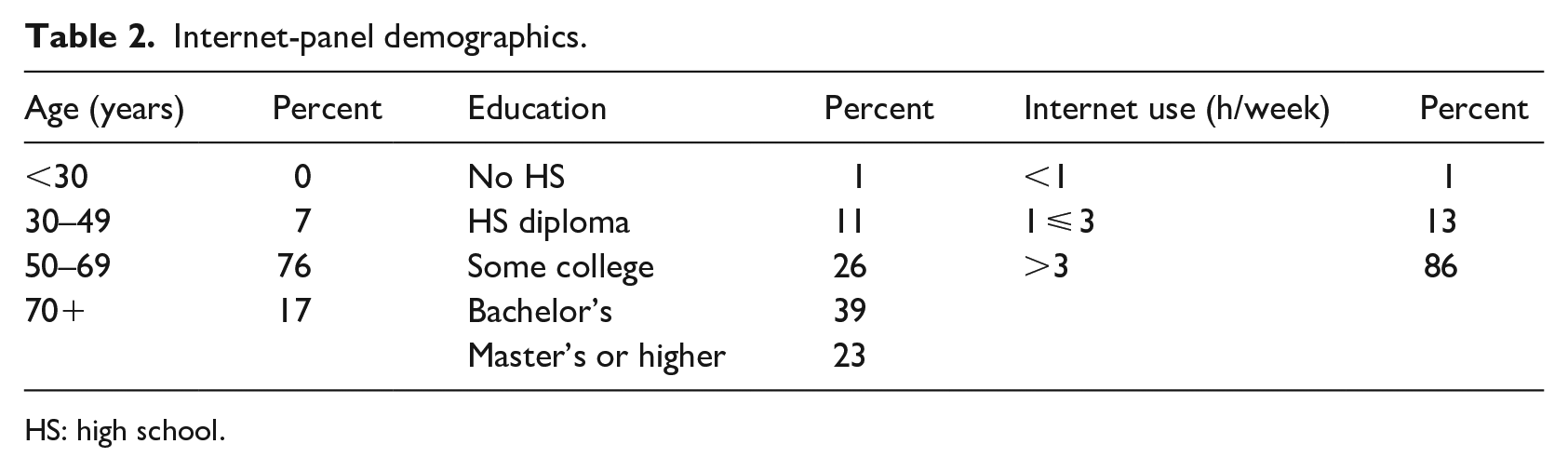
HS: high school.
Figure 7 shows the PLS results for this group. Table 3 shows the effect size of variables on behavioral intention (BI), and Table 4 shows predictive relevance Q2 of model variables. Values above 0.02, 0.15, and 0.35 for Q2 indicate small, medium, and large predictive relevance for selected constructs, respectively. Overall predictability of the model in both measurement and structure is GOF of the model, 44 in formula (1)

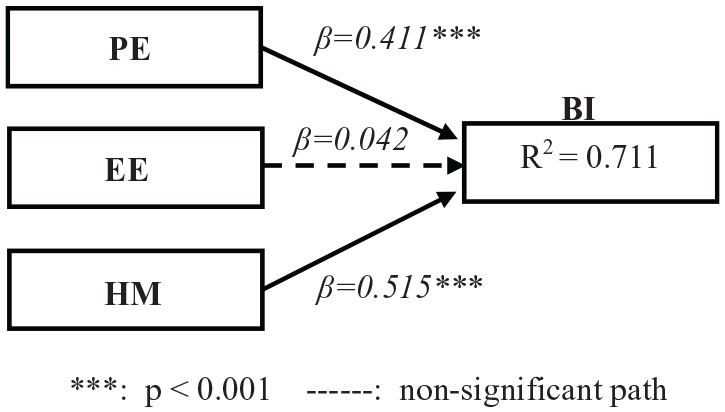
PLS results from the proposed model—Internet-panel group.
Effect size of the variables—Internet-panel group.
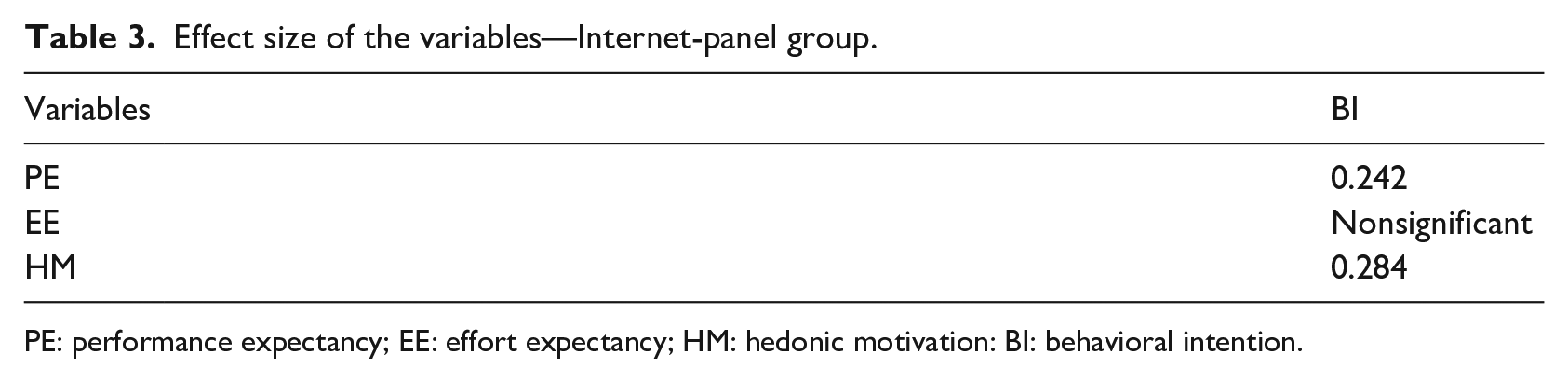
PE: performance expectancy; EE: effort expectancy; HM: hedonic motivation: BI: behavioral intention.
Predictive relevance of the model variables—Internet-panel group.
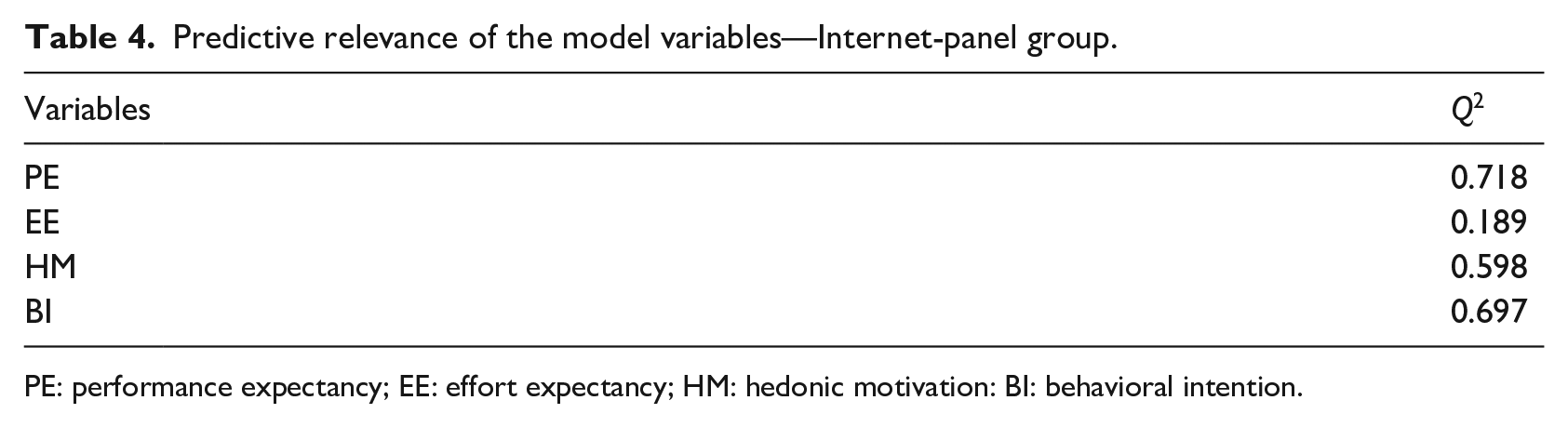
PE: performance expectancy; EE: effort expectancy; HM: hedonic motivation: BI: behavioral intention.
In-person group
Patients with PAD were chosen for the in-person test. PAD results in obstruction of blood flow in the arteries, exclusive of the intracranial and coronary vessels. It can affect the upper extremity arteries, extracranial carotid, and mesenteric and renal circulation and cause chronic arterial occlusive disease in leg arteries. 45 A convenience sample was taken from 400 PAD day clinic outpatients over a 1-year period at the hospital. They were recruited by a study nurse who offered opportunities to participate. Eight-four patients agreed. One was incomplete and hence discarded. Of the 83 participants, there were 36 females and 47 males; see Table 5 for other in-person group demographics.
In-person group demographics.
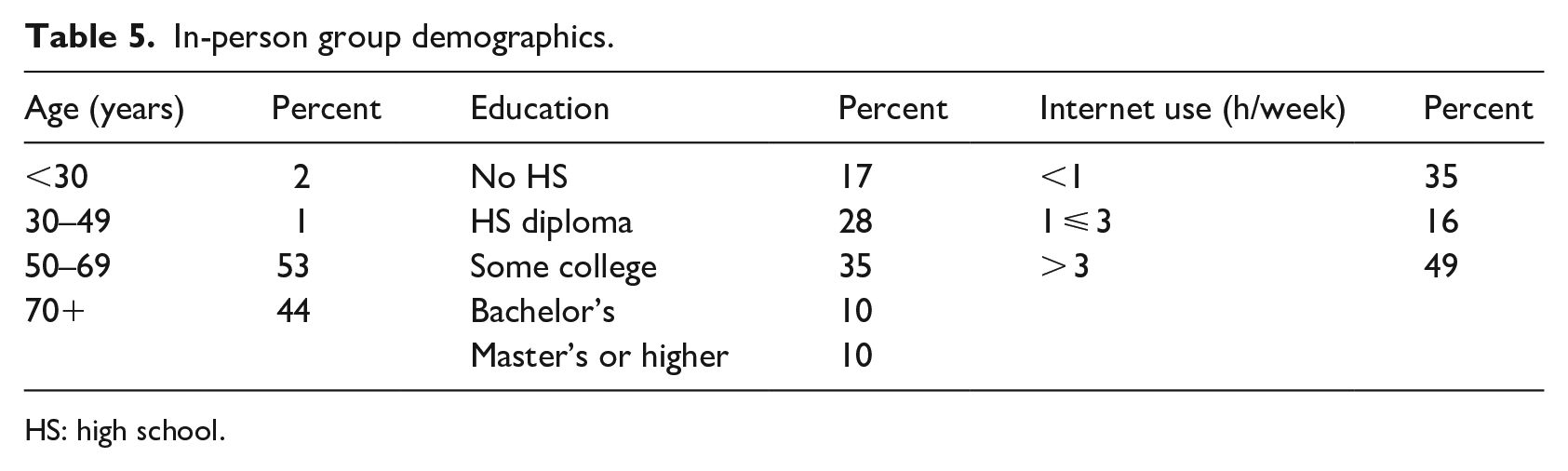
HS: high school.
Figure 8 demonstrates the PLS analysis of the model using this group’s data. Table 6 demonstrates the effect size of variables on BI, and Table 7 shows the cross-validated redundancy of the model variables. GOF of the model 44 is presented as formula (2)

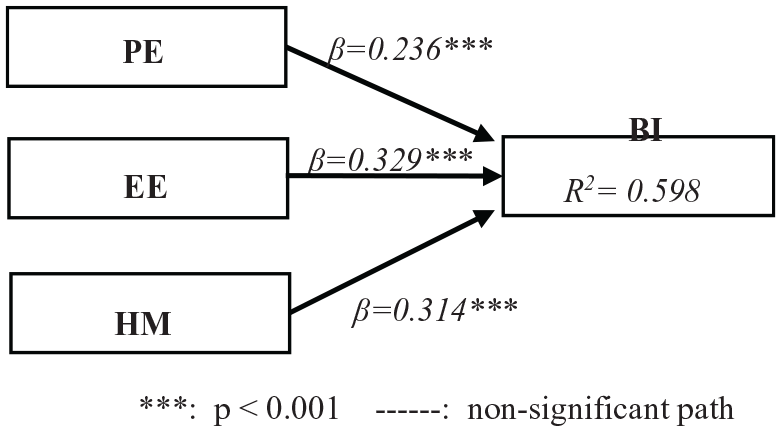
PLS results of the proposed model—in-person group.
f 2 (effect size) of the variables—in-person group
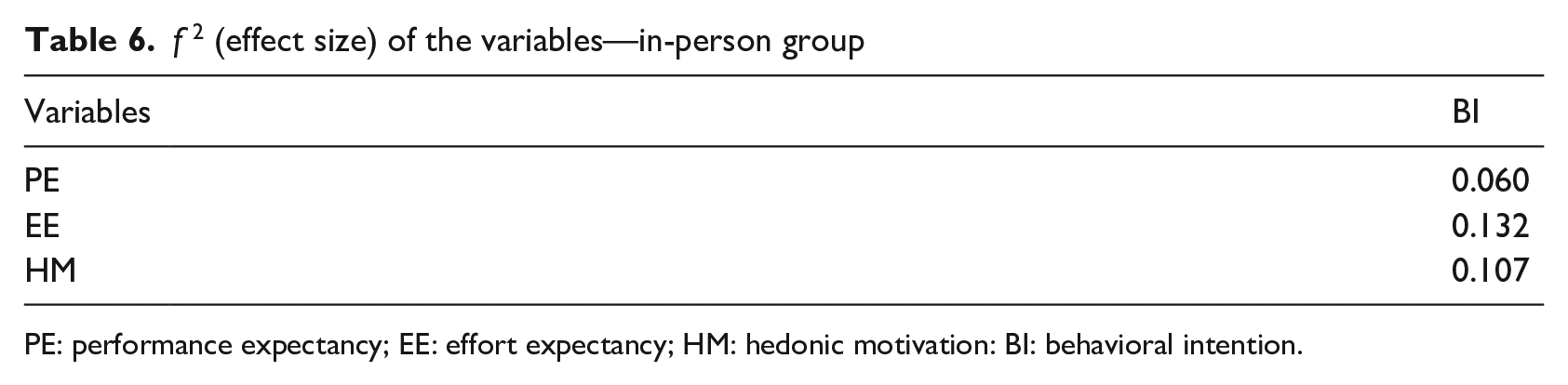
PE: performance expectancy; EE: effort expectancy; HM: hedonic motivation: BI: behavioral intention.
Predictive relevance of the model variables—in-person group.
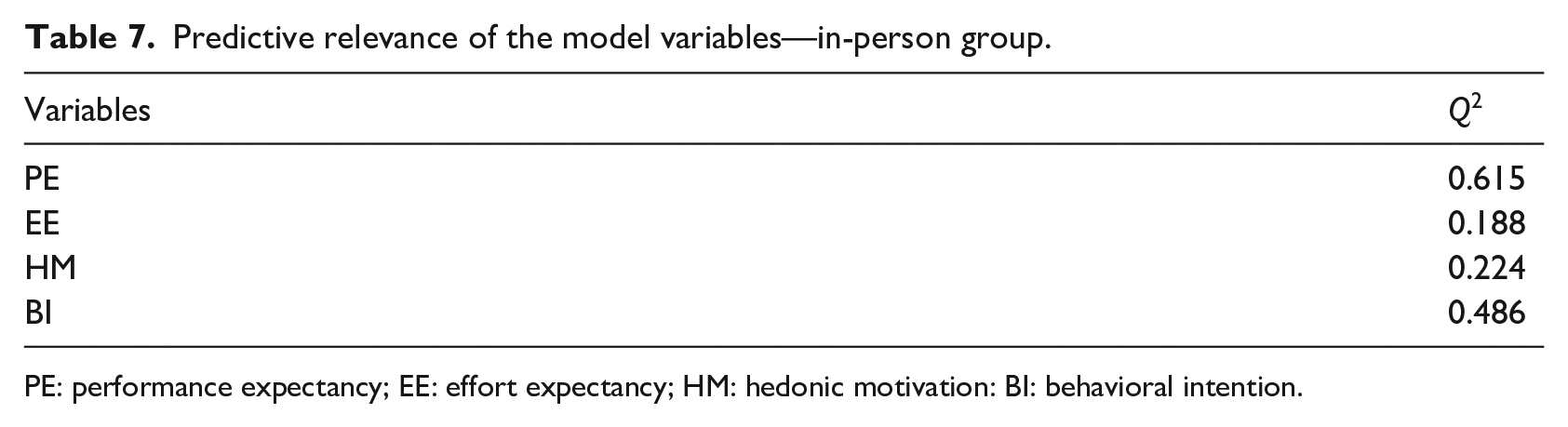
PE: performance expectancy; EE: effort expectancy; HM: hedonic motivation: BI: behavioral intention.
Discussion
The modified UTAUT2 model gave good results, shown by the high predictive relevance 43 of the model in both cases for all variables, the high R2 46 for BI of users in both groups, and high GOF 44 for both groups (model A = 0.743 and model B = 0.634). The average published values for R2 in UTAUT2 studies 9 are about 0.74. The R2 for both groups (Internet-panel: 0.711 and in-person: 0.598) are acceptable in comparison with other well-established studies in the field. 47 Predictive relevance for all endogenous variables for both groups is promising (Tables 4 and 7). These results reconfirm our choice of the UTAUT2 model for this study.
There were significant correlations between performance expectancy (PE), hedonic motivation (HM), and BI (PE → BI: β = 0.411, f2 = 0.242 and HM → BI: β = 0.515, f2 = 0.284) in the Internet-panel group, but there was no significant relationship between effort expectancy (EE) and BI (EE → BI). This is kind of unexpected according to other studies. 9 However, we did find the same relationship to be valid and significant in the in-person group (EE → BI: β = 0.329, f2 = 0.132). It seems that although both models explained the data, there is a difference between them in the sense of how EE affects BI (EE → BI). A plausible explanation for this is: Internet-panel participants were better educated on average than those in the in-person group (see Tables 2 and 5). The lack of a significant correlation between EE → BI (in Internet-panel) may be due to prior education and knowledge in the Internet group about working online. Thus, in their perception, using the system would be effortless. In the in-person group, on the contrary, there was less prior education and knowledge, so even though they saw the system as useful (PE → BI) just like the Internet-panel group, they might expect it to require significant effort (EE) to learn and use. Patient responses to the four open-ended questions also provide a solid ground for this explanation. Most the patients in the in-person group were concerned about how to learn the system, while in the Internet-panel group, less than half of the questions were about effort to use the system. Further studies may be required to confirm this theory.
In addition, we evaluated the moderators (age, gender, and experience) in both models. Experience was not a factor, since we intentionally chose and employed users (patients) without any prior experience with such systems. Gender also did not have any correlation with BI (or any other variable in the model). However, age has a negative relationship with a small effect size on BI in both models (Model A (Age→BI) : β = −0.215, f2 = 0.102, Model B (Age→BI): β = −0.219, f2 = 0.108). The results are consistent for both groups and indicate that the older patients exhibited less intention to adopt and use the system (BI). Having said that, the effect size is small, meaning that although age should be taken into consideration, it is not a deciding factor (due to its small effect size) and could be dealt with by strengthening other important factors in the model (i.e. PE, EE, and HM).
Conclusion
A large number of the Baby Boomer generation are retiring every year, and their health and medical needs put a huge burden on the healthcare system. 48 Moreover, retirement itself is a significant factor in developing depression or at least some psychosocial symptoms that patients are simply not equipped to deal with by themselves. 49 The availability of online health self-management will aid greatly in meeting the growing needs for cost-effective healthcare for this rapidly growing population. This can be accomplished at least partially through education and lifestyle change support to lessen the impact of chronic illnesses on these populations.
However, these changes depend very much on the physician–patient relationship. A recent longitudinal qualitative study 50 has shown that patients experience a high level of anxiety and vulnerability, when they want to start a new relationship with a “human” care provider due to a variety of factors such as uncertainty, embarrassment, lack of understanding, and fear of judgment. Providing the system with the described features in this study may help patients on many of those points. Having said that, we do not suggest that the support provided by an online system is enough by itself for patient health self-management, but it must complement and support care providers. This is specifically important since lifestyle change plays an important role in chronic disease management, particularly disease prevention, as a recent systematic review of chronic disease management showed. 51
Health self-management support must focus mainly on lifestyle change, with motivations it can provide for sustainability, through education, training, leisure activities, and social involvement. 52 The proposed system will provide an infrastructure that facilitates all the factors mentioned and will help to reduce the anxiety and sense of vulnerability of patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.