
Abstract
Despite large-scale adoption during COVID-19, patient perceptions on the benefits and potential risks with receiving care through digital technologies have remained largely unexplored. A quantitative content analysis of responses to a questionnaire (N = 6766) conducted at a multi-site acute trust in London (UK), was adopted to identify commonly reported benefits and concerns. Patients reported a range of promising benefits beyond immediate usage during COVID-19, including ease of access; support for disease and care management; improved timeliness of access and treatment; and better prioritisation of healthcare resources. However, in addition to known risks such as data security and inequity in access, our findings also illuminate some less studied concerns, including perceptions of compromised safety; negative impacts on patient-clinician relationships; and difficulties in interpreting health information provided through electronic health records and mHealth apps. Implications for future research and practice are discussed.
Introduction
The rapid shift to digital health care during the COVID-19 pandemic has removed some long-standing barriers to adoption. 1 Telemedicine; including remote consultations, personal health records, and mobile health apps, has been associated with several benefits in secondary care. These include shorter waiting times, 2 lower travel costs for patients, 3 and reduced need for face-to-face appointments for routine check-ups.4,5 Meanwhile, personal health records and some mobile health apps can support patient self-management, improving medication adherence,6,7 and chronic disease management.8–10
Although the past decades have seen a growing number of studies on clinicians’ views and experiences, the equivalent body of research on patient perspectives remains comparatively small, particularly in secondary care. The widescale implementation of digital services in secondary care during the pandemic offers opportunity to examine patients’ ‘real world’ experiences using these technologies at scale. Analysing responses to a questionnaire (N = 6766) from a large multi-site NHS Trust in London (UK), this study aimed to identify patient-perceived benefits and concerns with using digital health services during the COVID-19 pandemic.
Background literature
Amidst growing health system demands and limited resources, telemedicine’s promise to make healthcare more efficient, cost-effective, and accessible has led to widespread adoption. Digitization of secondary care was accelerated by the COVID-19 pandemic, resulting in a significant rise in the use of digital health technologies, such as remote consultations, wearable sensors, and virtual wards, across the United Kingdom.11–13 Despite this, evidence on effectiveness, efficacy and risks of telemedicine remains inconsistent. 14 For example, although some studies indicate that telephone consultations can reduce time to initial response, 2 time from referral to treatments, 4 and time-effectiveness of consultations, 15 others find that it may miss rare but serious conditions, and can result in higher rates of re-attendance.16–18
An emergent body of social scientific work is focussing on the social, cultural, and ethical effects of digital health technologies.19,20 This includes the impact of self-tracking and data surveillance on personal wellbeing, how digital health technologies redefine patient and provider roles and relationships, and the lived experiences of those using technologies. Oudshoorn et al have depicted the ‘invisible’ work and diagnostic competency required from patients to use a wearable heart monitoring system. 21 Greenhalgh et al have illuminated factors such as cognitive capability and fear of intrusion, that influence older adults’ usage of home-based assistive technologies. 22 Other qualitative research highlights the risks of technology undermining the patient-doctor relationship. 23 Collectively, these studies show the importance of considering patient perspectives when evaluating technology adoption.
The increased integration of health technologies into patients/public’ lives, has evoked ethical debates about surveillance, privacy, and equity. From electronic health record data to geolocation data collected through wearable sensors and fitness apps, digital health technologies have the propensity to generate a wealth of highly individualised data. This has introduced serious data privacy risks (e.g., data leaks and cyberattacks).24,25 These concerns highlight a larger ethical question regarding whether the benefits of technologies outweigh the risks, and the circumstances in which health data collection is considered acceptable by the public. Research exploring public attitudes towards data practices in health can offer insights to inform ethical practices in innovation, and support initiatives aimed at improving transparency, accountability, and public involvement in patient data use in health systems (e.g., UK’s ‘Understanding patient data’).
Another major area of work has focused on the ‘digital divide’ in access to health technologies and inequities in the design, purpose, and use of these applications across populations. Telemedicine has been presented as a solution to inequalities in healthcare caused by distance or disability status.26,27 Yet, it is becoming increasingly clear that telemedicine can also cause inequities in access, such as through due to limited availability of stable internet,28–30 language barriers,31,32 and poor digital literacy (in particular for older age groups).33,34 The introduction of data-driven healthcare technologies may further introduce risks for marginalised groups due to existing biases in historical data used to create these technologies, as exemplified by recent cases of underperformance and bias for minority groups.35,36 Hence, equitable access to technology does not necessarily result in an equal distribution of health outcomes. Due to a dearth of research examining the structural conditions and lived experiences that shape digital health use and subsequent outcomes, insight on this has remained limited.
Aim of this paper
Given the active role of patients and public in adopting digital health technologies, and the aim for digital health applications to support individuals to self-manage their health and care, there is an urgent need for research that examines patient experiences using these technologies. The shift in responsibility from health providers to ‘empowered patients’ means patient experiences are not only integral to the success of these technologies, but can also cast light on potentially harmful social, ethical, or cultural implications. This article utilizes data from a hospital questionnaire to identify benefits and concerns reported by patients who used a range of digital health services during the pandemic. Their insights can provide critical insight on major themes that require urgent attention in future research and policy.
Methods
Data collection
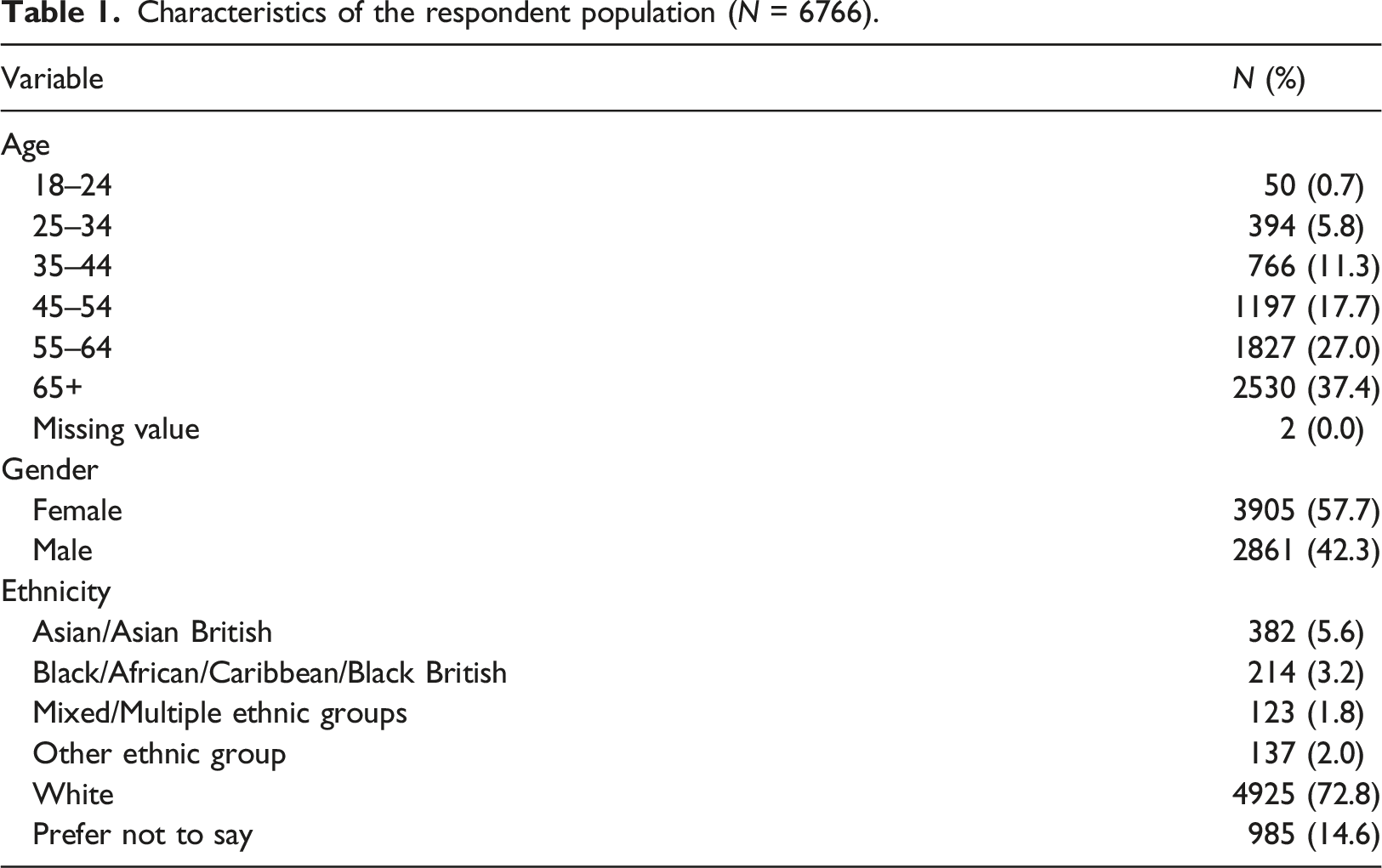
This study uses survey data from a larger questionnaire conducted as part of The Longitudinal Effects on Wellbeing of the COVID-19 Pandemic (LoC-19) project in August 2020. This questionnaire was hosted on Care Information Exchange (CIE): a web application provided by Patient Knows Best that gives on-line access to medical records for patients and their health professionals, and currently represents the largest patient-facing electronic health record system in the English NHS. An invitation to complete the questionnaire was shared with all CIE registrants at a large multi-site NHS Trust in North-West London who previously opted-in to receive weekly questionnaire invites for the LoC-19 project (N = 18,581). A total of 9359 of all 18,581 invited participants completed the survey (50.4%) of which 6766 (72.3%) provided answers to both or either of the two free-text questions and were included in this study.
The two open-ended questions in this survey queried perceived benefits and concerns with using digital health services during COVID-19. The survey also consisted of several multiple-choice questions regarding adoption rates. Survey items were tested with patient and carer representatives (N = 5) before inclusion. A full version of the original questionnaire can be found in Multimedia Appendix 1.
This work was conducted as part of a service evaluation (registration number 508) and therefore did not require ethical approval.
Data analysis
Three researchers ([JD], [CG], [NB]) analysed the free-text responses using the framework analysis method. 37 This method was considered appropriate due to its propensity to analyse large qualitative datasets in a systematic manner. 38 Framework analysis involves five stages: data familiarization, developing a thematic framework, indexing, charting, mapping, and interpretation. 38 Two researchers ([JD], [CG]) independently re-read a sub-set of the dataset (N = 2,000, 29.6%) to inductively develop a list of initial codes. A meeting was facilitated by a third researcher ([ALN]) to review, discuss, and revise initial codes towards an agreed set of codes which were then organized into overarching domains. This provided a working coding framework which was applied by two researchers ([JD], [AP]) who each coded half of the dataset. The coding framework was adjusted iteratively throughout the analysis stage to ensure no critical codes (e.g., frequently occurring or distinctive themes) were missed. Once finalized, a third researcher ([NB]) coded a randomised sub-set of 900 responses (13.3%) to test inter-rater reliability in applying the framework. Inter-rater reliability was tested using Gwet’s AC1,39,40 which corrects for category distribution.
Frequencies of reported themes across the respondent population were reported using descriptive statistics. Chi-square tests were conducted to test associations between reported themes and patient demographics (i.e., age group, gender, ethnicity). Verbatim responses of each theme were analysed descriptively and included in the results to illustrate the themes. Quantitative analyses were conducted in SPSS v26.0.
Results
Characteristics of the respondent population (N = 6766).
Patient-reported benefits with digital health services
Benefits reported by respondents, their respective frequency, and illustrative quotes are described below. A total of 211 respondents did not respond to this particular item (but did respond to the ‘concerns’ question). Of 6555 included responses, 202 (3.1%) respondents reported ‘no benefits’.
Ease of access (N = 2506; 38.2%)
Patients most frequently reported ease of access as a benefit of using digital health services, mostly reported by younger age groups (χ2 = 293.840, p < .001) (Multimedia Appendix 2). Beyond perceived benefits with regards to enhanced flexibility of accessing care (e.g. “access whenever and wherever”), patients often reported that the option of remote consultations had removed access barriers in their daily lives, such as needing to arrange childcare, fears for taking time off work, and costs for travel. Not having to travel reduces the cost significantly. Three members of my family are treated at [the hospital] for the same condition so the travel expenses are quite high. Also, I do not need to take a whole day off work to attend the appointment.
Others noted the difficulty of travelling to appointments with mobility issues or while feeling ill: “a benefit is not needing to have face to face consultations each time – this is especially helpful for disabled people like me who find travelling painful and difficult”.
Supports disease and care management (N = 1565; 23.9%)
Nearly a quarter of patients reported that the introduction of digital health services had allowed them to better manage their own health and care. Personal health records were often highlighted as supporting patients to manage their healthcare appointments, review test results and scans, and prepare questions for upcoming consultations. The pandemic forced the innovations in virtual care to happen, I had never before had access to Patient Knows Best or DrDr and it happened quickly due to the pandemic. Benefits are immense, allowing me to own my care and understand my clinical data and be part of my plan of care.
The use of mHealth apps for self-managing and improving health were also often reported as beneficial, including reports of feelings of empowerment and ability to have more control over one’s health: “[they] empower one to be proactive in with health and give them knowledge which can allay uncertainty and then allow for self-care”.
Timeliness of care (N = 1255; 19.1%)
Nearly one-fifth of patients reported that digital health services improved the timeliness of care with faster access to consultations over the telephone or video (compared to face-to-face) and quicker subsequent prescriptions and referrals. The introduction of these digital technologies during the pandemic has been great. It has allowed patients to access care quicker and faster. It has also allowed patients to contact their named consultant or medical healthcare professionals when they have felt it was necessary. It has also meant that patients have not had to wait too long for follow up/review appointments, like they normally would have before the pandemic.
Many also noted the benefit of being able to access immediate self-help information through on-line symptom checkers and health information websites, often stating this had relieved unnecessary concerns and enabled informed decision making.
Prioritisation of healthcare resources (N = 775; 11.8%)
Patients who discussed prioritisation of healthcare resources reported that digital health services could support improved prioritisation of patients based on urgency and nature of care needed, with digital triaging presenting a more resource-efficient alternative for minor issues and follow-up checks.
Freeing up the time of clinicians to see face to face those patients who really need to be seen as opposed to, for example, having to attend a clinic simply to talk about test results
This benefit often co-occurred with reports of ease of access in the context of minor outpatient appointments –patients felt that remote outpatient consultations could save time and resources for both patients (e.g. by minimising regular travel) and the hospital (e.g. by minimising resources spent on simple check-ups).
Care continuity amidst COVID-19 (N = 502; 7.7%)
Those reporting care continuity amidst COVID19 referred to the ability to continue care while staying at home; preventing transmission risks for oneself, peer patients, or healthcare workers. For many, the knowledge of being able to access the clinical team at any time had contributed to a general feeling of ‘being looked after’. COVID-19 brought feelings of isolation, fear of attending medical facilities etc. By using this tech, I still felt fully supported by the clinics I usually attended.
Patient-reported concerns with digital health services
Concerns reported by respondents, their respective frequency, and illustrative quotes are described below. A total of 322 respondents did not respond to this question (but did respond to the ‘benefits’ question). Of 6444 included responses, 1699 (26.4%) reported ‘no concerns’, in particular older age groups (χ2 = 13.474, p = .019) and White respondents (compared to respondents from any other minoritized ethnic group) (χ2 = 19.150, p < .001) (Multimedia Appendix 2).
Data security and privacy (N = 1182; 18.3%)
Data security and privacy was the most frequently reported concern, with respondents from minoritized ethnic groups reporting this significantly more often than White respondents (χ2 = 23.804, p < .001) (Multimedia Appendix 2). Patients reported not only perceived risks around cybersecurity breaches and commercial end-use, but also with data being shared with governmental bodies. Data hacks and government knowing too much about me. Also potential selling of this data - insurance companies would not provide cover if they knew you had pre-existing conditions and there should be no bias.
Compromised safety (N = 1150; 17.8%)
Concerns with compromised safety were often discussed in the context of remote consultations, where respondents perceived a heightened risk of a mis(sed) diagnosis due to the clinician’s inability to physically examine patients. The nagging doubt that the patient has not been seen “properly”. The clinician cannot use their sense of touch, for example. Or the clinician may notice something from the patient's appearance or manner. Or the opportunity is missed to take a blood-pressure or temperature reading.
The absence of non-verbal communication was often noted as problematic, with many believing that subtle cues (e.g. a patient’s body language) can provide clinicians with critical information to guide the consultation (e.g. knowing whether to probe; asking follow-up questions). Others mentioned they had found it difficult to verbally explain their symptoms in remote consultations, sometimes complicated by a lack of a privacy when undertaking telephone or video consultations. There is so much non-verbal communication that can be picked up on in person but not over the phone. There is also the issue of patients not being comfortable to talk freely about certain things if they live with someone else (my personal experience!).
Overall, 1140 (17.4%) provided insufficient information to codify or did not fit into the coding framework (e.g. coded as ‘unspecified or other’; e.g. “they are great”; “the way forward”).
Patient-doctor relationship (N = 807; 12.5%)
Patients further highlighted concern about the impact of digital health services on the patient-doctor relationship. Such reports referred to the lack of interpersonal reassurance, missing the human connection with clinicians and the wider care team, and a perceived reduction of holistic care (i.e. discussing not only the disease, but also one’s wider circumstances). There is no substitute for a face-to-face meeting with a doctor. A patient is more than just an ailment. They may feel alienated or unwanted by the health professional on the other end. The best experience a person can have is to have proper relationship with their doctor, GP practice or hospital personnel.
Inequity in access and use (N = 796; 12.4%)
A significant proportion of patients were concerned with inequity in access and use of digital health services. Some of these reported barriers relating to access to stable internet or digital devices. We often have a bad internet connection in our house, and mobile phone reception is practically non-existent.
Others highlighted language barriers, disabilities (e.g. hearing or vision impairments), and low digital literacy hindering access and use. It was often noted that more work could be done to better support older patients in accessing and using digital health technologies. From my experience I believe that older people may not have or understand the technology to access, for example, a video call. Not everyone understands how technology works. I have spoken to friends who are the same age as me and dismiss technology as they have never had the opportunity to learn or use.
Misunderstanding health information (N = 431; 6.7%)
A substantial number of patients reported low confidence in their ability to correctly interpret their health data on electronic health records or mHealth apps. For some, this had resulted in increased anxiety, and concern about incorrect self-diagnosis or taking inappropriate steps with regards to seeking care. Being able to access test results is right and proper in principle, but lack of own medical knowledge can mean either worrying about something which doesn't matter, or alternatively not realising the potential seriousness of a result.
Overall, 910 (14.1%) provided insufficient information to codify or did not fit into the coding framework (classified as ‘unspecified or other’; e.g. “not sure really”; “I am quite sure there are”). In such responses, it was often noted that digital health alternatives should remain a supplementary option, rather than a replacement (“no concerns as long as it is optional and without penalties”).
Discussion
Patients reported a range of benefits of receiving care through digital technologies beyond usage during COVID-19 (e.g., improved access, timeliness, and self-management of care). However, in addition to some well-known risks such as data security and inequity in access, patients also highlighted some novel areas of concern including perceived loss in social and relational aspects of care, and challenges in interpreting medical information provided by digital health technologies.
The most common patient concern referred to data security and privacy, echoing previous studies.42–44 Interestingly, in contrast to some previous studies that show these concerns primarily relate to cybersecurity breaches and commercial third party-use,44–46 our study finds that these concerns extend to governmental access to data. This shift in concern may be a consequence of COVID-19 related initiatives to track personal health data and enable data sharing between governmental bodies and the NHS.47,48 As digital health solutions become more widespread boundaries between health services and third-party organisations will need to be protected, with clear regulation around transparent and consensual data collection and retention.
Our findings provide novel insights into the social factors that shape digital health use – a critical gap in digital health research. In terms of benefits, digital health services improved access to care for a significant proportion of (mostly working age) respondents, who highlighted benefits in tackling social barriers to traditional care including travel expenses; arranging childcare; mobility issues; and repercussions for taking time off work. Meanwhile, barriers to access, such as digital literacy, internet access and usability (particularly in relation older and more vulnerable groups) were highlighted as a significant impediment to digital technology adoption; supporting existing research.28,29,34,49–52,
Safety risks were also raised, particularly relating to diagnostic error and compromised communication quality. 53 Studies in paediatrics have demonstrated comparative clinical outcomes using telemedicine approaches.54,55 Research has also shown that the perceived reduction in some clinical risks (such as contamination) 53 can drive uptake of teleconsultation solutions. However, other studies others have found that the use of telemedicine can miss rare but serious conditions, and can result in higher rates of clinical re-attendance.16–18 More research is required to assess the potential of missing relevant clinical signs and diagnoses across different patient groups.
Although personal health records and mobile apps may provide a greater sense of control over one’s health, our findings suggest they can also induce anxiety and inappropriate healthcare seeking behaviours when users do not have the confidence or skills required to interpret medical data. This finding illuminates the invisible work and health literacy requirements that influence the use of health technologies, and suggests the need for co-design efforts and patient education to ensure that patients can accurately interpret digital health information.
Our findings suggest that concerns about the use of digital technologies are not unrelated to wider determinants of health (e.g. age, socioeconomic status, educational level and language barriers)31,32 or particular health needs (e.g., cognitive impairment, visual or hearing impairment). This emphasises the need for wider evidence across patient groups, clinical conditions, and social context to understand if, when, and for whom digital care services are appropriate for use. This should focus not only on clinical, but also environmental, social and humanistic factors, such as relationship building and patient-clinician communication.
Study strengths and limitations
Strengths of this study include its large sample size, the use of the systematic framework analysis approach to codify a vast number of free-text responses, excellent inter-rater reliability between coders, and the novel exploration of patient experiences of technologies in secondary care.
This study was developed as rapid research to evaluate patients’ experiences using digital health services during COVID-19 – using data from a non-validated survey. The survey was distributed opportunistically to patients who accessed CIE and agreed to complete the survey. The sample was therefore not stratified or randomly selected. Whilst this approach ensured that respondents had first-hand experience with using digital health services, the views of those unable or unwilling to access digital health services are underrepresented. Further, of 9359 respondents to the original survey, 2593 (27.7%) did not respond to either open-ended question. Most of these (91.4%) moved on to complete the subsequent multiple-choice question, suggesting that non-response may be due to the relative burden of the open-ended items. 56 The broad nature of the questions included in this study also means that responses may have been shaped by the respondent’s respective experience with particular types of digital health services (e.g., remote consultations, medical records). We have therefore provided details on particular technologies typically referred to by respondents when discussing a particular theme to support the interpretation of the results. Finally, although the analysis of survey data provides insight on views held at a large-scale, it is limited in examining the context of these experiences. More in-depth qualitative research, such as interview studies and ethnographic research, is needed to provide a deeper, contextualised understanding of the themes identified in this study.
Conclusion
Our study adds to existing literature by demonstrating patients’ perceptions of the benefits and risks of digital health services deployed during the COVID-19 pandemic. Benefits include easier access, patient empowerment, and improved timeliness. Concerns include practical barriers linked to social determinants of health such as poor internet access and low digital literacy. Other risks include anxiety caused by interpreting medical information, the risk of reduced diagnostic accuracy, data security concerns and fear of degrading the patient-clinician relationship.
These findings demonstrate the importance of user-centred co-design and patient education to ensure that patients across the spectrum of digital and health literacy can easily use and interpret digital health technologies. This should be supported by clear regulation and public engagement around the use of healthcare data.
Limitations of this study include the use of a non-validated survey on a non-stratified, non-random sample. The views of those unable or unwilling to access digital health services are therefore underrepresented. Responses may also have been influenced by respondents’ personal experience with digital health services and this study is limited in examining the context of these experiences.
Further research including interview studies and ethnographic research is required to determine when, and for whom digital care services are appropriate for use. This should inform robust systems change processes for digital health technology implementation which promote equity and patient autonomy, offering non-digital alternatives where appropriate and ensuring no patient group is left behind.
Supplemental Material
Supplemental Material - Identifying benefits and concerns with using digital health services during COVID-19: Evidence from a hospital-based patient survey
Supplemental Material for Identifying benefits and concerns with using digital health services during COVID-19: Evidence from a hospital-based patient survey by Annabelle Painter, Jackie van Dael, Ana Luisa Neves, Patrik Bachtiger, Niki O’Brien, Clarissa Gardner, Jennifer Quint, Alexander Adamson, Nicholas Peters, Ara Darzi, Saira Ghafur in Health Informatics Journal
Supplemental Material
Supplemental Material - Identifying benefits and concerns with using digital health services during COVID-19: Evidence from a hospital-based patient survey
Supplemental Material for Identifying benefits and concerns with using digital health services during COVID-19: Evidence from a hospital-based patient survey by Annabelle Painter, Jackie van Dael, Ana Luisa Neves, Patrik Bachtiger, Niki O’Brien, Clarissa Gardner, Jennifer Quint, Alexander Adamson, Nicholas Peters, Ara Darzi, Saira Ghafur in Health Informatics Journal
Footnotes
Acknowledgements
The manuscript was written by [AP], [NO], [SG], and [JD], and reviewed and approved by all authors. [NO], [JD], [CG], and [ALN] contributed to the analysis. [PB] developed and launched the questionnaire on Care Information Exchange (CIE). We thank [ALN, JD and NP] for their contribution in reviewing a draft of the questionnaire.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Patient Safety Translational Research Centre.
The open access fee was paid from the Imperial College London Open Access Fund.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.