
Abstract
The use of Internet-enabled technology (information and communication technology such as smartphone applications) may enrich information exchange among providers and, consequently, improve health care delivery. The purpose of this systematic review was to gain a greater understanding of the role that Internet-enabled technology plays in enhancing communication among physicians. Studies were identified through a search in three electronic platforms: the Association for Computing Machinery Digital Library, ProQuest, and Web of Science. The search identified 5140 articles; of these, 21 met all inclusion criteria. In general, physicians were satisfied with Internet-enabled technology, but consensus was lacking regarding whether Internet-enabled technology improved efficiency or made a difference to clinical decision-making. Internet-enabled technology can play an important role in enhancing communication among physicians, but the extent of that benefit is influenced by (1) the impact of Internet-enabled technology on existing work practices, (2) the availability of adequate resources, and (3) the nature of institutional elements, such as privacy legislation.
Introduction
Governments routinely consider ways to improve health care systems such as increasing access to care, enhancing quality, and controlling costs. Communication among health care providers is one area that has received attention as research has demonstrated close links between better communication and service delivery improvements. For example, good communication has been shown to be crucial for advancing coordination of patient care, 1 ensuring patient safety,2,3 minimizing duplications in efforts across providers, and limiting inappropriate use of health care services. 4
In the current digital age, information and communication technology (ICT) has been widely promoted as a means of achieving health care system improvements.5–7 The general premise is that the resultant “electronic bridges”—which allow for interactions among multiple users either in real time or asynchronously—can help enrich information exchange among health care providers. 4 Some evidence suggests that enhanced communication through the use of ICT can improve health outcomes, health care provider performance, quality of care, coordination and efficiency of services, and patient engagement in care.8,9 However, evidence continues to be limited regarding the extent to which ICT improves communication among specific groups of health professionals.10,11
Rationale and purpose
Physician-to-physician communication by electronic means is not well understood.1,2,12 Most studies in this area have focused on one type of technology, such as e-mail or electronic health records.1,13 In addition, perspectives on newer forms of ICT for enhancing communication, such as social media and smartphone apps (i.e. Internet-enabled technology (IET)), are limited. Given their influence as frontline care providers, physicians can affect work processes (e.g. the implementation of clinical practice guidelines or setting the “climate/tone” of the health care environment). Furthermore, physicians can play an important role in the uptake of new technology as their behavior may shape that of other physicians and health care providers. 14 The purpose of this systematic review was to gain a greater understanding of the role that IET plays in enhancing communication among physicians—which may inform current practices and future research—by examining evidence in the scholarly literature.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), 15 and the guidelines for undertaking systematic reviews in health care from the Centre for Reviews and Dissemination, 16 were used as a model for conducting this literature review (the first author performed all the study procedures). Studies were identified through a search in three electronic platforms: the Association for Computing Machinery (ACM) Digital Library, ProQuest, and Web of Science. Across these platforms, 12 databases/indexes were examined (e.g. MEDLINE), which were selected based on the relevance of their subject content to the topic of study. Keywords/search terms related to IET (e.g. eHealth, digital), communication (e.g. correspondence, exchange), and physicians (e.g. clinician, medical practitioner) were used. Truncations of terms were searched within each database to capture all possible iterations of keywords in the literature (e.g. technolog*). The search identified articles with a combination of the specified keywords in—one or more of—the papers’ title, abstract, keywords, or full-text.
Study selection and eligibility criteria
To be eligible for inclusion in the study, articles needed to (1) be published in a peer-reviewed journal, (2) be accessible in English, (3) be published between 2005 and 2015, and (4) have IET for health care communication among physicians as the primary objective of the investigation. Non-primary research articles (e.g. editorials, study protocols) were excluded, with the exception of systematic reviews. The search was limited to the last 10 years to capture more recent forms of ICT (i.e. IET).
Following initial screening (titles and abstracts), the full-text of each remaining article was reviewed to determine if eligibility criteria were met. In addition, the references in the included articles were examined for other eligible studies. The first author of this study carried out the database searches.
Data screening and extraction
The following data were extracted from the articles that met eligibility criteria: article/study author(s) and year of publication, demographic(s), objective(s)/research question(s), study design/method, technology used, and main outcomes (Table 1).
Article summaries.
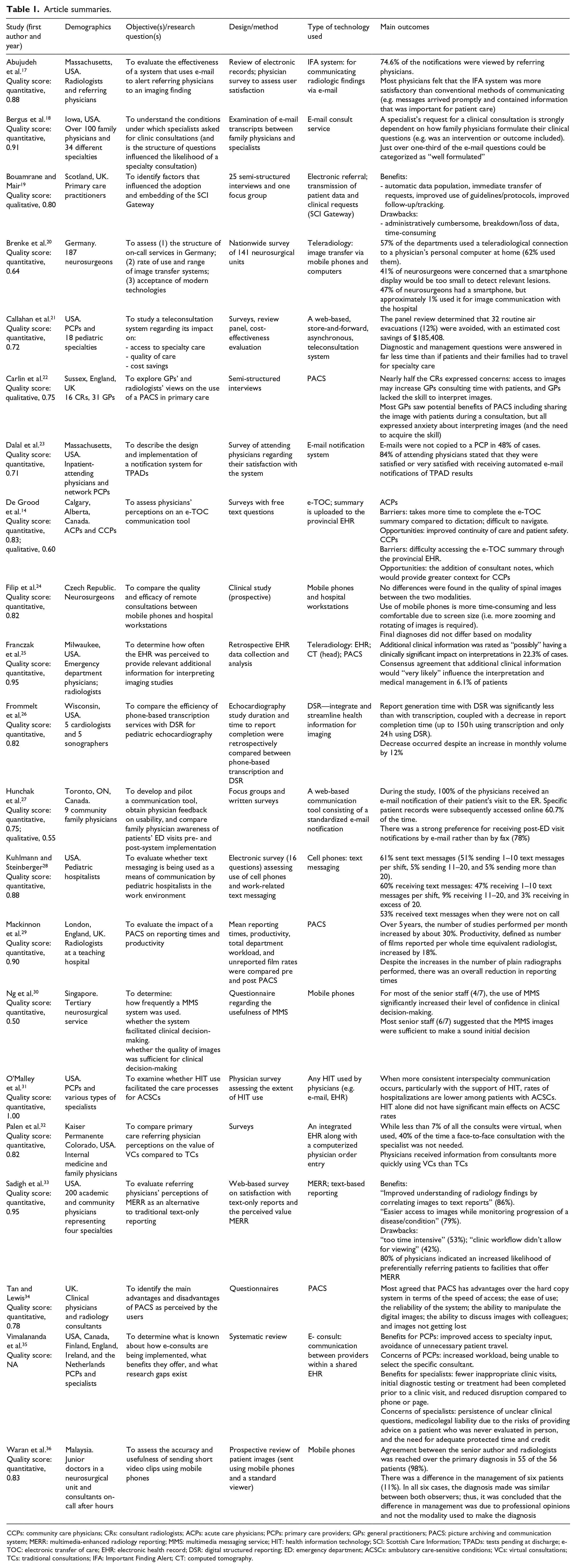
CCPs: community care physicians; CRs: consultant radiologists; ACPs: acute care physicians; PCPs: primary care providers; GPs: general practitioners; PACS: picture archiving and communication system; MERR: multimedia-enhanced radiology reporting; MMS: multimedia messaging service; HIT: health information technology; SCI: Scottish Care Information; TPADs: tests pending at discharge; e-TOC: electronic transfer of care; EHR: electronic health record; DSR: digital structured reporting; ED: emergency department; ACSCs: ambulatory care-sensitive conditions; VCs: virtual consultations; TCs: traditional consultations; IFA: Important Finding Alert; CT: computed tomography.
Quality assessment
Qualitative and/or quantitative data reported in the articles were assessed for methodological rigor using Kmet et al.’s 37 validated tool QualSyst. The tool consists of 14 items/questions for quantitative studies, 10 items/questions for qualitative studies, and a related scoring system (from 0 to 1; higher scores are indicative of greater quality). Items relate to components such as a clear description of the research question or objective; whether the sample was appropriate; a description of data collection/analysis; and tying the findings back to theory or the broader literature. While Kmet et al. do not assign specific values to the possible scores (e.g. 0.4 = “poor quality”), they discuss various cut-points for the overall scores (possible cut-off scores included <0.55, <0.60, <0.65, <0.70, and <0.75). Based on these cut-points, and for the purposes of this study, less than 0.55 was considered lower quality, 0.55–0.75 was considered moderate quality, and greater than 0.75 was considered higher quality. QualSyst has been used in other health-care-related systematic reviews,38,39 and is considered a key resource for appraising evidence in the literature. 40
Analytic approach/synthesis of findings
Findings were summarized and analyzed through a process of narrative synthesis. A preliminary synthesis consisted of grouping the included studies in a way that helped to describe and analyze the data. This involved looking for patterns within and across groups. 16 The identified groupings consisted of (1) the type of IET that was being used, such as mobile devices and web portals; and (2) the reason why IET was being used, such as consultation and notification. To explore relationships within and across studies idea webbing and conceptual mapping were used, which involved visual methods to aid in the development of groupings and associations. These techniques are used: “(i) to group findings that are empirically and/or conceptually similar and (ii) to identify (again on the basis of empirical evidence and/or conceptual/theoretical arguments) relationships between these groupings.” 16 The analysis consisted of identifying the recurrent and/or most prevalent themes across the studies.
Results
Search outcomes
The search identified 5140 articles (70 from the ACM Digital Library, 1609 from ProQuest, and 3461 from Web of Science). Of these, 5044 articles were excluded during initial screening (5042 through title and abstract review; two were duplicates across databases). Of the 96 remaining articles that underwent full-text review, 39 were excluded as IET for health care communication among physicians was not the primary objective of the investigation (i.e. other health care providers were included and the results could not be separated by profession); 16 were not focused on communication; seven did not include IET; and 21 were removed for not being primary research studies (e.g. they were commentaries or they described a protocol). Three systematic reviews were identified by the search, but only one was included. The other two were removed as either (1) the studies included in the review were older than 2005; or (2) the studies included in the review were already identified in the main search. The references in the 13 remaining articles were examined for additional studies. In all, 33 articles that met the inclusion criteria were identified and eight of these were included, bringing the final number of articles contained in the review to 21 (Figure 1).
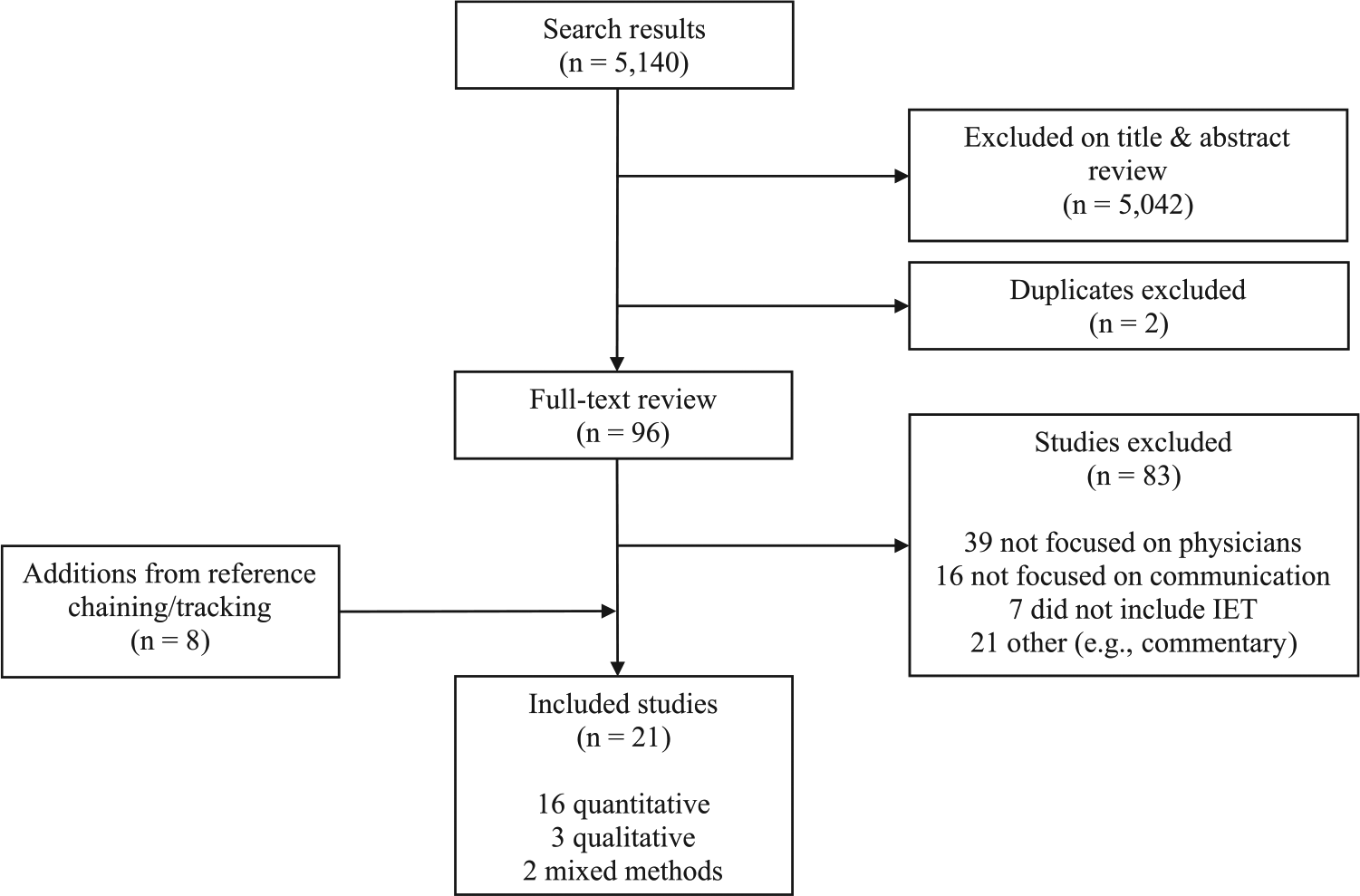
Flowchart of the search results.
Descriptive summary (study characteristics)
Of the 21 studies that were included for final analysis, 16 used quantitative methods consisting of questionnaires/surveys (n = 12), records/transcripts review (n = 6), and a cost-effectiveness evaluation (n = 1). Three studies used qualitative methods, consisting of interviews and/or focus groups (n = 2), and a narrative synthesis from a systematic review (n = 1). Two studies used mixed methods, consisting of focus groups and surveys.
The physicians participating in the 21 included studies were from a variety of medical specialties including cardiology, emergency, endocrinology, family/general practice, gerontology, intensive care, internal medicine, neurology, oncology (medical and radiation), psychiatry, pulmonology, radiology (breast, musculoskeletal, neurologic, thoracic, vascular), and surgery (general and neurologic). Most of the studies were conducted in the United States (n = 10), followed by the United Kingdom (n = 4), and Canada (n = 2); while one study was conducted in each of the Czech Republic, Germany, Malaysia, and Singapore. The included systematic review contained studies from Canada, Finland, England, Ireland, and the Netherlands. 35
Quality ratings
Of the 21 included studies, one was not suitable for evaluation as it was a systematic review and narrative synthesis. 35 Of the 20 studies that were assessed, 18 contained quantitative elements that were rated for quality; scores ranged from 0.50 to 1 (mean score = 0.82, high quality). Two of these studies used mixed methods and, thus, also had qualitative elements (scores = 0.60 and 0.55, respectively; mean score = 0.58, moderate quality).14,27 Two studies employed exclusively qualitative methods (scores = 0.80 and 0.75, respectively; mean score = 0.77, high quality).19,22
Quantitative components that were consistently well done across the studies included a sufficient description of the question or objective; selection of an appropriate design; provision of some variance estimates for the main results; detailed reporting of the results; and results supporting the conclusions. Items that were done less well and received lower scores included (one or more of) a description and appropriate method of subject selection; provision of participant characteristics; details regarding appropriateness of sample size; and controls for confounding.
Qualitative components that were consistently well done across the studies included a clear description of the research question or objective; selection of an appropriate design; clear context for the study; and connection to a theoretical framework or wider body of knowledge. Items that were done less well and received lower scores included (one or more of) description of a relevant and justified sampling strategy; a clear, complete, and systematic data collection method; use of verification procedures to establish credibility (e.g. member checks, inter-rater reliability); and reflexivity of the account (i.e. assessment of the researchers’ impact of their personal characteristics and the methods used on the data obtained). 37
Narrative synthesis
As previously stated, the initial grouping process consisted of categorizing (1) the type of IET that was being used across the included studies and (2) the reason why IET was being used. The types of IET consisted of electronic health records (EHRs; eight studies); mobile devices (five studies); e-mail (four studies); image transmission and storage/picture archiving and communication systems (PACS; four studies); and web portals (three studies). The reasons for IET use consisted of consultation and clinical decision-making (seven studies); image transmission (five studies); notifications (three studies); quality (two studies); reporting turnaround time/enhancements in efficiency (two studies); communication not otherwise specified (two studies); referral (one study); transfer of care summary (one study); access (one study); and cost (one study).
Using idea webbing and conceptual mapping (as discussed earlier, and based on the objectives of the included studies, the reasons for use, and the findings/results), three main groups/themes were identified. Namely, provider satisfaction with IET (the extent to which physicians perceived IET to be more or less satisfactory than traditional practices), efficiency of health information exchange (the extent to which communication using IET was more efficient), and the impact of IET on clinical decision-making (the extent to which information provided via IET made a difference to clinical decisions/diagnoses). Each of these classifications will be discussed in turn.
Provider satisfaction with IET
In all, 10 studies reported on physicians’ perceived satisfaction with IET use.14,17,19,20,23,27,32–35 These perceptions were related to different categories of IET, including e-mail notifications (n = 3), the transfer of images (n = 3), consultations via an EHR/web portal (n = 2), electronic referrals (n = 1), and the transfer of care summaries (n = 1). In general, physicians agreed that these various forms of IET were more satisfactory than conventional methods of communicating, such as e-mail compared to fax.14,17,19,23,27,33–35 The main reasons for greater satisfaction included ease of use/convenience, speed of access/turnaround time, improved information-sharing and clarity, increased awareness of the care that patients received, and improved continuity of care.14,17,19,27,33–35 However, some studies revealed dissatisfaction with certain elements of IET,14,19,34,35 or no difference in satisfaction compared to traditional methods. 32 The main reasons for dissatisfaction were concerns related to IET being slow, difficulties with access to information, and associated time-consumption.14,19,35
Efficiency of health information exchange
In all, 10 studies reported on the efficiency of information exchange among physicians and the associated implications, such as whether time or money could ultimately be saved.14,21,22,24,26,29,32–35 Across a variety of IET uses, physicians reported a reduction in response time for consults. In addition, questions related to diagnosis and management were answered in less time compared to traditional methods.21,22,26,32,35 These reductions occurred despite overall increases in consult requests.26,29 However, in some of the reviewed studies, while health-care-related information was transferred between physicians faster, it took longer to prepare and complete in digital form, raising questions of whether widespread IET use may waste resources.14,22
While the speed of access to information may be greater with IET,33–35 such access does not necessarily translate into actual use of the information that is received. The data available in such mediums may be seen as too time-consuming to review (i.e. physician workflow can act as a barrier to reviewing additional information provided by IET). 33 For example, downloading and evaluating images requires significantly more time using a mobile phone compared with a workstation, and viewing images on mobile devices is more time intensive due to the need for greater image manipulation because of the smaller screen size (e.g. zooming, rotating). 24
The impact of IET on clinical decision-making
Seven studies reported on aspects of consultation/clinical decision-making.18,21,24,25,30,35,36 There was a lack of consensus across the studies as to whether information exchanged among physicians via IET made a difference to clinical decision-making. In the case of mobile phones, the quality of shared images was often perceived to be similar to those via hospital “workstations”/PACS. One study suggested that multimedia messaging service (MMS) use (i.e. “texting” or “messaging”) obviated the need to view the original scans and increased levels of confidence in clinical decisions/diagnoses; 30 while three studies suggested that the final diagnosis made using a mobile device did not differ from traditional methods.24,30,36 However, the use of conventional systems (i.e. PACS) allows for additional functionality such as variation of contrast and magnification, which may capture smaller structural changes compared to images via MMS. 36 In the case of adding additional information from an EHR into PACS, or images to consults via a web portal, physicians felt that the extra information would be likely to impact diagnosis and/or medical management, but only in a small minority of cases.21,25
Discussion
This study examined evidence in the scholarly literature regarding the role that IET plays in enhancing communication among physicians. Three core themes were identified, namely, provider satisfaction with IET, efficiency of health information exchange, and the impact of IET on clinical decision-making. Here, we discuss some of the associated implications of these themes for practice and policy as well as recommendations for future research.
Implications for practice and policy
Workflow
Evidence from the studies included in this review revealed that physicians were generally more satisfied with IET than conventional methods of communicating. However, in some instances, communication by electronic means can disrupt workflow and productivity due to interruptions in traditional practices which, consequently, may decrease satisfaction and influence the use of new technology.14,33 For example, with the evolution of mobile devices, physicians may be more likely to have work-related communication outside of their regular working hours, which can negatively impact work/life balance. 28 Given the ease with which communication can be sent via IET, physicians may feel an obligation to reply to correspondence immediately, as opposed to managing such communication at set times throughout the day when not engaged in other activities. Tending to every message when it is received, regardless of clinical importance, can lead to alert fatigue (wherein some messages may be ignored), 41 which may have adverse consequences for patient care. A potential solution to this problem is establishing configurable rules or flexibility within existing systems,14,19 such as limiting communication to the most critical and time-sensitive information.23,33 Restrictions on the immediacy of the flow of information may reduce the frequency of information that physicians receive after-hours and, thus, provide adequate down-time.
Resource requirements
While IET has the potential to positively affect health care delivery through more efficient communication (e.g. facilitation of daily work processes, improvements in decision-making), such innovations require significant resources, which may be a considerable barrier to clinician acceptance. In particular, whether physicians use IET on a regular basis is dependent on financial compensation. Communication among medical specialties via IET is often poor, partly due to the fact that fee-for-service payment models lack incentives for information-sharing.25,31 Without suitable remuneration, physicians may opt for practices they deem most efficient. 21 Therefore, if the goal is to enhance electronically mediated communication among physicians, payment structures—such as salaries plus workload-based credits—will likely need to be in place to ensure the sustainability of these activities.32,35
Institutional structures
IET use is also influenced by institutional elements, such as regulatory processes, policies, and norms (rule-setting, monitoring, how things should be done). 42 As concerns regarding the security of health care data are persistent, 21 there is a need for safeguards, like data transmission with end-to-end encryption, to ensure compliance with local privacy legislation. Adequate devices and networks also need to be in place (those that have the requisite security features, data transmission speeds, etc.) to ensure that timely, protected, and quality data are available.20,24 These measures are particularly important when information is shared across jurisdictions or via short message service (SMS)/MMS (which are less secure forms of IET).28,32
Recommendations for future research
Following our review, several issues became apparent that warrant further consideration.
A small minority of the included studies used qualitative methods, such as interviews or focus groups. The emphasis on quantitative methods comes at the cost of not capturing important details or nuances related to how and why physicians are using certain types of IET for communication, along with the associated impacts (e.g. disruption of workflow).
Only one of the included studies incorporated theory. 19 The use of theory is important as it provides a means for explaining findings, and affords the opportunity to examine and test theoretical constructs, which help predict behavior.
Most studies focus on IET adoption, use, and gains in efficiency. Better metrics are needed for clinical outcomes, which have thus far been measured primarily by provider perceptions rather than objective criteria. 35
A small number of the included studies (n = 6) discussed the impact of maintaining the security of health information and/or the impact of privacy legislation on the use of IET. Research efforts to gain a greater understanding of how existing privacy legislation affects physician behavior are needed. Depending on the specifics of such legislation, laws may actually constrain the use of particular forms of IET.
Only one of the included studies explicitly discussed the management of physician-to-physician communication by administrative/support staff. It would be helpful to gain a better understanding of how often this form of staff-managed communication occurs, the reasons why it occurs (e.g. are physicians too busy to learn how to use the technology?), and the associated implications.
Limitations
While this review used a systematic approach following established guidelines, numerous types of physician specialties were included across a variety of settings, and exclusion of studies based on design were relatively few, some limitations warrant mention. First, given the heterogeneity of IET used in the included studies, and the diversity of contexts in which IET was used, it is challenging to arrive at a consensus as to whether IET enhances physician-to-physician communication (based on satisfaction, efficiency, and clinical decision-making). Second, the overarching search strategy consisted of peer-reviewed journals from three electronic platforms (12 databases/indexes). The inclusion of other sources of information, such as gray literature, may have revealed additional relevant information and resulted in a more comprehensive assessment (other sources were not included for practical reasons/feasibility). Finally, the studies included in this review did not examine clinical communication among physicians in urgent circumstances, which limits the scope of our findings. However, acute patient care constitutes more complex informational exchange than non-acute care and, as a result, may require different forms of communication, such as telephone conversations or in-person meetings (i.e. some technology can limit “meaningful interactions”). 43
Conclusion
Effective communication among physicians is important to the success of high performing health care systems. IET can help facilitate effective communication, but cannot ensure that it occurs. Failure of IET initiatives is often related to a focus on technology at the expense of social and organizational factors that will impact its use (e.g. attitudes, training time). 44 Therefore, as new technology is adopted, there is a need to understand and manage these domains. Depending on the context, IET use may lead to more but not necessarily better communication. 43
This review reveals that IET can play an important role in enhancing communication among physicians, but the extent of that benefit is influenced by (1) the impact of IET on existing work practices (e.g. if it disrupts normal processes), (2) the availability of adequate resources for IET implementation and use, and (3) the nature of institutional elements, such as privacy legislation. Inattention to these factors may result in less than optimal improvements in communication among physicians and, as a corollary, health care system performance.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.