
Abstract
Introduction
Video consultation (VC) became vital for improving healthcare access during COVID-19 pandemic and remains so. Despite evidence of effectiveness, concerns including technology literacy and inconsistencies in experience highlight the need for larger, patient-focused studies. While patients appreciate the convenience of VC, challenges during complex issues and patients’ preferences for in-person care persists. Synthesising qualitative studies offers insights into the fragmented understanding of patient experiences with VC. This review explores adult patients’ experiences of VC.
Methods
A systematic literature search was conducted for studies published between 2011 and 2024 and reported according to the PRISMA statement. Study quality was assessed using the CASP checklist, and data were analysed through thematic synthesis. Confidence in the findings was evaluated using GRADE-CERQual.
Results
In total, 3203 unique studies were retrieved; 13 were included in the final synthesis, resulting in four main themes: (1) suitable for less complex issues when technical problems can be solved; (2) feeling secure, relaxed, and having mutual focus in an equitable partnership; (3) limitations regarding personal needs and practical help; and (4) increased vulnerability and lack of emotional feedback.
Conclusion
VC is experienced as ideal for managing less complex issues but is challenging for emotional topics due to technical concerns. It empowers patients by providing a neutral place for focused conversations but can create vulnerability and distance that can challenge the patient–professional relationship. Success requires technological adaptation, sufficient time during VC, and emotional support. VC should complement – not replace – traditional care, with its use determined in dialogue with patients.
Introduction
Video consultation (VC) enables communication through real-time visual and audio connection. 1 Information and communication technologies such as VC are believed to be an essential factor in ensuring universal health coverage, 2 and provide opportunities to overcome geographical distances and ensure access to healthcare in areas where it is lacking. 3 During the COVID-19 outbreak, VC played an important role in providing continuous access to necessary health services, while keeping patients and healthcare professionals safe.4,5 A post-pandemic analysis of the use of telehealth, which includes VC, showed that between 2019 and 2023 there was a remarkable global effort to utilise telehealth. 6 The year 2020 might well be the turning point where digital technology became accepted as part of healthcare routines by the public as well as governments. 7 The effectiveness of telemedicine in healthcare has been the subject of investigation for several decades. A systematic review of reviews published in 2010 reported that 21 reviews concluded telemedicine to be effective. However, it also identified 22 reviews that found the evidence to be limited and inconsistent. This divergence underscored the need for more large-scale studies and a greater emphasis on incorporating patients’ perspectives into evaluations of telemedicine services. 8
Comparative reviews have demonstrated that both telephone and VC are as effective as face-to-face (FTF) consultations in improving clinical outcomes across primary care,9,10 psychotherapy, 11 and hospital-based settings. 12 Moreover, VC has been found to outperform telephone consultations in a variety of healthcare contexts, 13 offering enhanced effectiveness at significantly lower costs than traditional care. 12 Despite the extraordinary increase in use of VC, patients still prefer FTF consultations14–16 and VC with healthcare professionals that they have previously met in person.17–19 Besides that, VC is still found challenging concerning emotional and complex questions20,21; and have issues related to technology.18,22
Patient involvement in healthcare can enhance the relevance, quality, safety, and effectiveness of healthcare services globally, and there is a need for qualitative studies that explore patients’ experiences in depth. 23 Patient preferences are central to the delivery of high-quality care, and a paucity of research focusing on patients’ experiences of virtual care has been identified. 24 The patient perspective contributes with recognition of the most appropriate use of VC for different patient groups and clinical conditions, and can capture potential downsides.9,25 Patient experiences of VC suggest that patients are comfortable communicating through video, and that VC has become normalised 18 and is seen as a convenient tool19,20 that is appreciated by patients as well as by healthcare professionals.25,26 However, contradictions within patient experiences of VC suggest that this is a fragmented field of research, and that patients’ preferences should be better examined 25 in order to explore what works well for different patient groups and why. 27 Evaluation of satisfaction with VC is most often undertaken using questionnaires,26,28 and several studies report patient experiences based on healthcare professionals’ observations. 25 The lack of comparable results and qualitative studies focusing on patient perspectives regarding VC highlights the need to gather existing knowledge generated by qualitative studies.
Reviews from 2019 and 2020 state that experiences, such as satisfaction, of VC have rarely been systematically reviewed using robust methodology.14,26 The lack of qualitative systematic reviews on patient experiences of VCs still remains since PROSPERO, 29 an international systematic review registry, shows only two existing or ongoing reviews in this area, both focusing on a much broader field of digital healthcare solutions and telemedicine for conditions such as somatic diseases 30 and chronic disease management during COVID-19. 31
To enhance the delivery of digital health services such as VC, understanding the patient perspective is of unequivocal importance. While previous research has explored patients’ experiences of VC across various clinical specialisations, to our knowledge, no systematic review has yet examined the experiences between patients and healthcare professionals via VC without categorising participants by specific conditions or specialties. Despite the rapid expansion of research on VC in recent years, there remains a notable gap in studies that synthesise qualitative data to complement the insights derived from quantitative approaches. A systematic review focusing broadly on patient experiences of VC, investigated through qualitative methodologies, could offer critical insights for healthcare practitioners, telehealth system designers, and policymakers alike.
Aim
The aim of the study was to compile and synthesise the scientific literature on adult patients’ experiences of VC with healthcare professionals.
Methods
Search strategy
A systematic search was undertaken in PubMed, CINAHL, MEDLINE, PsycINFO and Web of Science to find articles on patient experiences of VC in the context of healthcare. This review is reported according to the PRISMA statement guidelines, 32 in line with the ‘Enhancing transparency in reporting the synthesis of qualitative research’ (ENTREQ) statement, 33 and is registered in the International prospective register of systematic reviews (PROSPERO; Registration ID: CRD42022330476). The search strategy was formulated using the SPICE Framework, suitable when assessing experiences. 34 The concepts were set as follows: Setting (S) − Healthcare; Population (P) − Patients; Intervention (I) − VC; Comparison (C) − not relevant to the review question; and Evaluation (E) − Experiences. Key terms related to the SPICE concepts was identified by test searches, a hand review of reference lists from relevant studies, and searches for synonyms and related terms using the Swedish MeSH database, 35 supplemented with appropriate terminology sourced from Merriam-Webster's online dictionary. 36 This approach ensured both linguistic and conceptual breadth in capturing relevant literature. As the thesaurus and subject headings used in PsycINFO differ from the more harmonised vocabularies found in Cinahl and PubMed, a separate search was conducted in PsycINFO to identify terms equivalent to those used in the search strings of the other databases. Some of the identified key terms were, telemedicine, remote consultation, mhealth, VC, audiovisual, videoconference, patient satisfaction, attitude, and perception. Further construction of the search strategy was then structured around conceptual blocks. Words categorised under the same block was combined using the Boolean operator “OR”, and blocks were combined using “AND”. The combination of the three blocks; #1 key terms related to telemedicine; #2 key terms related to VC; and #3 key terms related to patient experience, resulted in the most relevant hits and was kept for the final search. The search strategy employed a combination of controlled vocabulary terms (e.g. MeSH terms) and free-text keywords, structured using Boolean operators (AND, OR) and field-specific tags (e.g. [Mesh], [tiab], [All fields]). Truncation symbols (e.g. *) were used to capture variations of root words. Each database's specific indexing system was considered. For full details of the search strategy in the different databases, see Appendix 1, and for search strings, limitations set, and number of hits, see Appendix 2.
A significant effort was made to have a broad yet manageable search strategy. The strategy and terms were agreed upon with an information specialist.
Literature search and study characteristics
The initial search was conducted on 11 October 2021, and complemented with a second search on 29 January 2024. Duplicates were removed from the results of the initial search using the EndNote software, and from the results of the second search using Rayyan. 37 The remaining duplicates were identified and manually removed by the authors.
The authors co-operated on the process of study selection. Title, abstract and full-text screening was performed by two of the authors independently to include studies that fit the inclusion criteria (Table 1). Disagreement at all stages was solved through discussions between the authors; when needed, articles were reviewed by a third author.
Inclusion and exclusion criteria.

Quality assessment
The quality of the included studies was assessed by the authors, with two authors independently, using the Critical Appraisal Skills Programme (CASP) checklist. 38 During the process of quality assessment from the initial search, the authors decided to exclude studies that used mixed methods, since the reporting especially regarding the recruitment strategy, the qualitative data analysis, and result section was substandard. There was also lacking information about the different steps of the analysis; references to methods used; and citations to strengthen the results; which altogether made it impossible to assess the quality in all mixed-method studies that were evaluated. The proportion of mixed-method studies included in the quality assessment was 5.4% in the initial search, and during the second search, mixed-method studies were excluded during the title, abstract and full-text screening.
Data extraction
Data that aligned with the aim of this systematic review were extracted from the Results/Findings section of each of the studies; this included both quotations from patients, and analysis conducted by authors. To ensure a similar procedure between all the authors, all three authors extracted data from one of the studies and discussed the results to reach consensus. Data extraction was thereafter undertaken independently by the authors, and the data was imported into MAXQDA (Version: MAXQDA 2022 (Release 22.8.0)) and Excel (version 2407). The extracted data also included authors; year of publication; title; publication; country; study population; number of participants; data-collection method; data-analysis method; and research questions/aim. These are presented in Table 2.
The included studies.
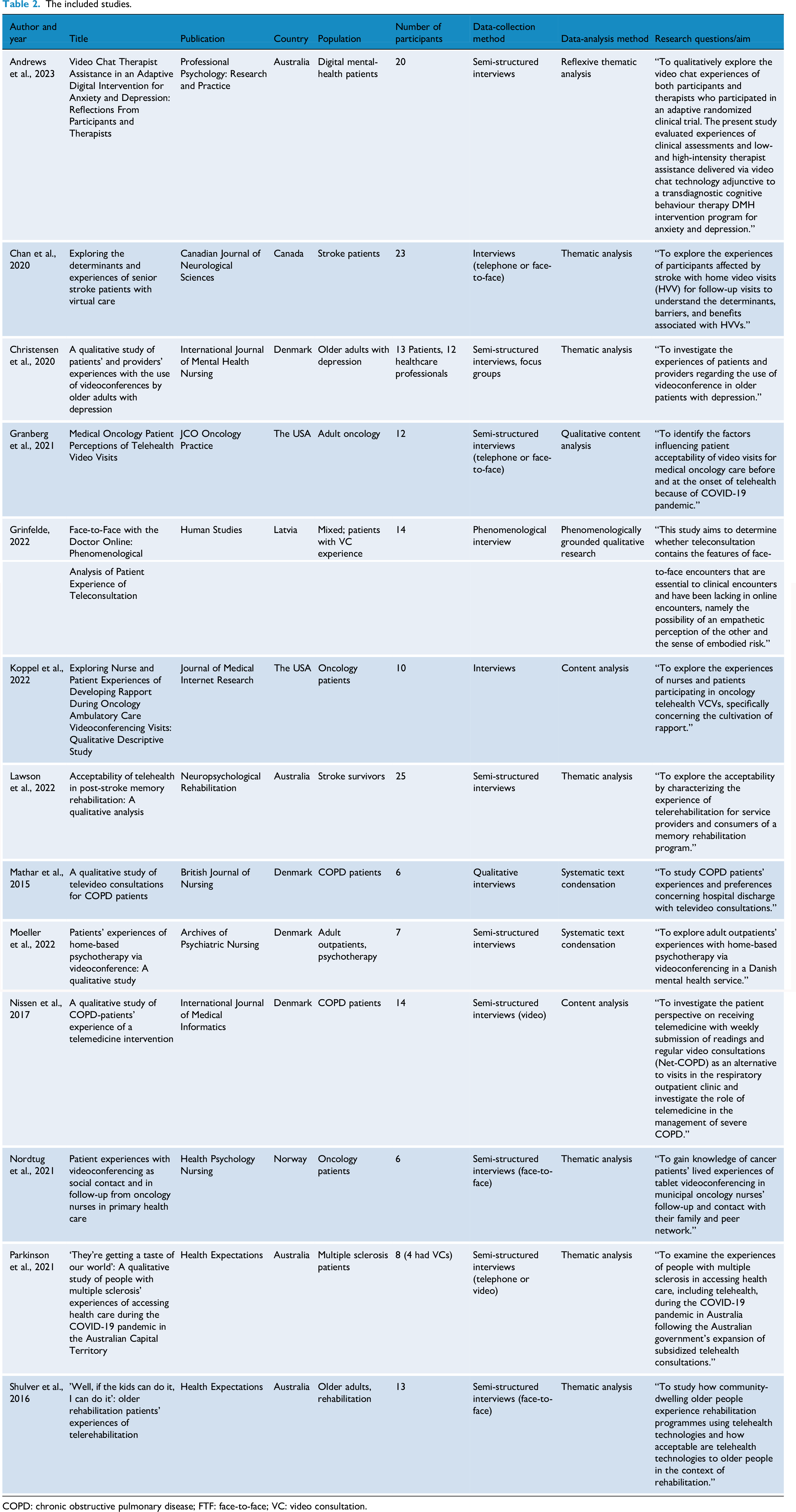
COPD: chronic obstructive pulmonary disease; FTF: face-to-face; VC: video consultation.
Data synthesis
The data were analysed using thematic synthesis, as formulated by Thomas and Harden 39 ; here, over the course of three stages, themes that reoccurred across the selected studies were identified. First, the extracted data were given a free line-by-line coding that summarised or described the text with a very low degree of interpretation, remaining close to the original findings. 39 To verify the method, all three authors independently coded one study and then discussed their results. After this, each of the remaining studies was coded by the first author. Second, similar codes were discussed by the authors, grouped into descriptive themes and kept close to the original findings. Third, a more abstract and analytical discussion between the authors was held to group, explain and describe the initial descriptive themes that emerged, forming the main analytical themes. 39
Quality appraisal
The assessment of confidence in the findings was guided by the GRADE-CERQual (Confidence in the Evidence from Reviews of Qualitative research) approach, 40 and performed using the iSoQ (interactive Summary of Qualitative Findings) – tool by all three authors jointly. The confidence in the evidence was based on four key components, that together contribute to an overall assessment: methodological limitations; coherence of the review findings; adequacy of the data contributing to the review findings; and relevance of the included studies to the research question of this study (Appendix 3).
Results
The search yielded 4252 publications; following the removal of duplicate citations, 3203 were studies to be screened. Following title and abstract screening, 133 were included in the full-text screening, and 33 of these were eligible for inclusion in the quality assessment. Of these, 20 studies were assessed to be poorly described, and therefore excluded; the remaining 13 studies were included in the synthesis (Figure 1).

Flow chart of included and excluded studies, along with reasons for exclusion.
Demographics of included studies
The 13 included studies were conducted in six countries (Canada, the USA, Norway, Denmark, Latvia and Australia), with publication dates from 2015 to 2023. Data were collected using interviews, and thematic and content analyses were used as predominant method of analysis. The number of participants ranged from 6 to 25; they were 20 to 92 years old and the only active party in the conversation during VCs with healthcare professionals due to stroke, depression, anxiety, chronic obstructive pulmonary disease (COPD), cancer, multiple sclerosis (MS), rehabilitation or psychotherapy.
Qualitative synthesis of findings
Thematic synthesis of adult patients’ experiences of VC with healthcare professionals identified four main themes, each with subthemes (Table 3). The synthesis did not identify any diagnostic or geographic context as dominant within the themes; however, all studies consistently supported two subthemes: ‘Less time, effort, and travel, and more accessible’ and ‘Challenges to the patient-healthcare professional relationship’.
Summary of the main themes and their subthemes, with contributing references.

FTF: face-to-face; VC: video consultation.
Main theme 1: Suitable for less complex issues when technical problems can be solved
The first main theme relates to patients seeing VC as saving both time and energy, if used in appropriate situations and under the right circumstances, and in line with patient's capacities and condition. A patient stated: “Now I – to get up in the morning and make the bed and get in the shower – I’m very slow. It's at least an hour and a half before I’m ready to come down… I felt that [VCs are] a way of saving me time and effort. Physical effort.”
41
Many studies noted the idea of
Patients described changing their attitudes to VC after trying it, and so
Main theme 2: Feeling secure, relaxed and having mutual focus in an equitable partnership
The second main theme relates to patients feeling that VC contributes to a sense of security and equity when the conditions are right, leading to fulfilment of needs and empowered patients. Authors in one study expressed: “This manifest[s] in that they were able to relax and felt more empowered to express themselves better from within [the] practical comfort and easy familiarity of their own home.”
42
Patients feel that VC offers
The result shows that many patients are satisfied with VC – that their
Main theme 3: Limitations regarding personal needs and practical help
The third main theme concerns VC restricting patients' ability to communicate effectively enough to obtain the help they need, whether that help is practical, physical or psychological, as one patient expressed it: “Well, it's a little bit more shorter and brief like just to make sure everything's going okay. When you’re in an office visit with the doctor, you’re more specific and asking specific questions and you’re there a little bit longer, I think, like you get more in detail.”
43
Some patients report that VC
Main theme 4: Increased vulnerability and lack of emotional feedback
The fourth main theme relates to patients experiencing relationships with healthcare professionals mediated solely by VC as being unsatisfactory and feeling increased personal vulnerability due to being at home with less emotional support and more responsibility. One patient described: “I would say that it is − in an odd way [video visits] kind of makes you a little more vulnerable to your provider because they see you in your home and sometimes in your pajamas, maybe they see − I don’t have children, but maybe they see your kids running around or they might be more attuned to parts of your personal life that you might keep confidential, whether − just in terms of making the relationship as − they probably want it to be professional or whatever. So I think that video does permit a level of vulnerability that an office visit would not.”
43
In 12 of the 13 included studies, the authors conclude that there exist
The results show that VC
Discussion
This study systematically reviewed 13 qualitative studies to synthesise their findings regarding adult patients’ experiences of VC with healthcare professionals. The synthesis resulted in four main themes: (1) suitable for less complex issues when technical problems can be solved; (2) feeling secure, relaxed, and having mutual focus in an equitable partnership; (3) limitations regarding personal needs and practical help and (4) increased vulnerability and lack of emotional feedback.
The results of this study are insights from qualitative research on the varying experiences of VC, which depend on the context, personal circumstances, and individual abilities of patients. Thus, the results state that VC is sometimes experienced as being as good as FTF, but FTF is still the best option for quality healthcare. Patient experience can, presumably, vary depending on practical factors such as having home visits compared to travel long distances. If you increase the risk of attracting a deadly virus when visiting the office your motivation to use VC will likely increase. This review presents patient experiences in various specialities and over a time-period including a pandemic, with widely differing circumstances and expectations. Interpreting the results must be done with consideration that these scenarios are represented in the original studies. Results published in 2023 show that the main reason patients did not want to continue using video consultations was a preference for FTF care, 15 regardless of disease or clinical scenario. 16 Usability concerns were less commonly cited. 15 When needing a prescription or receiving test results, a telephone consultations was preferred. 16
Overall, the results show that VC contributes to feelings of security and empowerment due to its accessibility, because the home is experienced as a private, and safe place where the patient is in charge. Being at home can contribute to patients performing actions with confidence 54 and facilitate empowered patient self-management. 55 For some, VC can increase patients’ privacy and prevent the sense of being on display in, for example, a waiting room. These empowering feelings depend on multiple circumstances, particularly the availability of home-based support and health conditions. The need of finding a quiet place at home to create a private, safe place for the VC, is sometimes challenging, which is in line with previous research.14,56 Another circumstance that is recognised as crucial for patients’ feelings of security is the ability to contact healthcare whenever needed. This is not a ‘built-in’ function of VC but certainly affects patients’ sense of control. Empowered patients are more likely to feel responsible, self-determined, and equal to healthcare professionals during VC, facilitating co-planning alongside healthcare professionals and self-confidence in overcoming initial technical problems and discomfort. It seems that VC creates a sense of equality in terms of dialogue during such circumstances. Research has highlighted a shift in power dynamics from hierarchical to collaborative in the physician–patient relationship, and the complexities of vulnerabilities when using digital tools. 57 The shifting of roles in healthcare due to the use of digital tools has for long been an area of interest emphasising the need to redesign the relational geography between actors in the healthcare process. 58 With empowered patients, research has shown a need for healthcare professionals to transition from a role of authority to one of guidance,57,59 and with a shift of power and roles comes a shift of responsibility between healthcare professionals.58,60,61
VC contributes to patients’ feelings that they are on the same level as healthcare professionals, but there are challenges with building relationships, especially when the two have never met before. Patients find it harder to talk, ask questions and discuss complex issues during VC. When concerned with potential technical problems, patients become reluctant to discuss emotional topics. Similarly, previous research describe that even though most patients experience a sense of being in the same room as the healthcare professionals during VC ‘the intimacy was experienced depending on the quality of the technical equipment’. 62 Unfortunately, technological difficulties relating to VC are still a challenge, even in highly developed countries. A systematic review in the Nordic countries found the technology uncertainties to be the dominant challenge present across all clinical specialisation studied, 22 making it difficult to guarantee optimal technical conditions for VC. This reduces trust in the ‘digital relationship’ between patients and healthcare professionals, and patients argue that VCs should only supplement FTF consultations, not replace them.
Another contribution to lost trust in the patient–professional relationship when it is conducted by VC is the absence of the physical room and context that is experienced when meeting FTF. VC is experienced as less personal with eye contact missing, which gives the ability to distance oneself. This distance can be positive when it feels like a protective space − helping the person avoid pressure or persuasion − and allowing for better focus without external distractions. However, distance can also be a negative barrier, creating a sense of alienation between the patient and the healthcare professional. 63 Similarly, our result show that distance can be negative when it makes things easier to dismiss and hinders a trusting relationship. When comparing differences in patient–doctor communication between FTF, and mainly VC (some telephone), a systematic review found that there is little significant difference between FTF and teleconsultation, with one exception, duration. FTF consultations were longer on average and there were fewer gaps to engage in small talk during teleconsultation. 64 Studies show that missing small talk during VC makes the relationship more challenging.21,65 The experience of VC as stressed and shorter could be related to the missed small talk in our result and challenge the building of relationship with unknown healthcare professionals.
As healthcare moves from offices to homes there is a shift in power that can empower, as stated earlier, but also bring a sense of vulnerability. Patients feel more vulnerable when healthcare professionals see their home environments. Their personal space has been described by healthcare professionals as the patients holiest place 66 that is almost sacred. 67 In addition, the personal preparedness seems to change, resulting in embarrassment over unbrushed hair, and alienation can be caused by seeing oneself on camera. This vulnerability, combined with less emotional support from healthcare, is a risk with VC that needs to be accounted for. Research on self-view during virtual meetings indicate the need to customise the technological features individually since it is associated with the users degree of public self-consciousness, 68 and has a negative impact on satisfaction while listening but can be neutral while speaking. 69
Importantly, the results suggest that healthcare professionals should be sensitive, and the organisation flexible enough to succeed in supporting patients, regardless of the communication tool used. VC in healthcare is a balancing act between empowerment and vulnerability, obligation and support, distance and relationship. To deliver high-quality healthcare using VC, patient involvement and co-operation are essential.
Future research could explore patient experiences of VC, taking differences in expectations and motivations into account. The perspective of healthcare professionals is important to add in future research for a deeper understanding of the challenges in patient–professional relationship, and how to decrease the risk of vulnerability in combination with less emotional support during VC. How individual customisation of technological features affects the patients’ and healthcare professionals’ experiences of VC needs to be evaluated. Knowledge on how to best support the shift of roles among stakeholders due to VC should be further compiled and implemented in the healthcare system.
Limitations
The limitations of this review relate to the quality of the included studies, not all of which reported on, for example, recruitment strategy and the relationships between researchers and participants. This is information that could have affected the results and has been accounted for in the assessment of confidence in the findings. Further, the included studies only report from middle- and high-income countries, the search was limited to English-language publications, and grey literature was excluded due to challenges in quality assessment and time constraints. Further, the exclusion of mixed-method studies in this review could have resulted in missed knowledge that would be important for the aim and transferability of the results. The included studies capture patient experiences of VC across a wide range of contexts, diagnoses, and healthcare professions, which enables a general conclusion across settings but limits the specificity. Transferability to age groups other than adults is limited.
Conclusions
Patients feel that VC provides accessible care that is best suited for less complex issues, and its use is preferred when patients already know the healthcare professional they will be meeting. Taking time for small talk during VC is important to more actively improve the patient–professional relationship and increase the feeling of being seen as a person. Patients avoid asking complex and emotional questions during VC because they fear interruptions due to technical problems. Making a back-up plan in co-operation with the patient is crucial to increase the feeling of safety. In addition to overcoming technical issues, a quiet place and home-based support is important, which healthcare professionals should emphasise when suggesting VC. VCs can offer a neutral, non-hierarchical arena, and contribute to patient empowerment through a more focused dialogue. The shift of roles and responsibilities between stakeholders is necessary to support in the development of future digital healthcare. During VC, some patients experience a distance that is challenging for the relationship between the patient and the healthcare professional, but this can also strengthen the feeling of security. Patients may feel more vulnerable when revealing private spaces via video and engaging in stressful VC conversations with less support and more responsibilities compared to FTF visits – a risk healthcare stakeholders should consider.
The findings of this review indicate that the mode of communication between patients and healthcare professionals should be determined collaboratively with patients and supports system designs that enable individually tailored VC, recognising that patient vulnerability spans diverse settings and conditions. For the time being, VC should be a complement to, and not a replacement for, FTF conversations in healthcare.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251404513 - Supplemental material for Patients’ experiences of video consultations: A qualitative systematic review
Supplemental material, sj-docx-1-dhj-10.1177_20552076251404513 for Patients’ experiences of video consultations: A qualitative systematic review by Lina Ärlebrant, Robyn Schimmer and Anette Edin-Liljegren in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251404513 - Supplemental material for Patients’ experiences of video consultations: A qualitative systematic review
Supplemental material, sj-docx-2-dhj-10.1177_20552076251404513 for Patients’ experiences of video consultations: A qualitative systematic review by Lina Ärlebrant, Robyn Schimmer and Anette Edin-Liljegren in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251404513 - Supplemental material for Patients’ experiences of video consultations: A qualitative systematic review
Supplemental material, sj-docx-3-dhj-10.1177_20552076251404513 for Patients’ experiences of video consultations: A qualitative systematic review by Lina Ärlebrant, Robyn Schimmer and Anette Edin-Liljegren in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076251404513 - Supplemental material for Patients’ experiences of video consultations: A qualitative systematic review
Supplemental material, sj-docx-4-dhj-10.1177_20552076251404513 for Patients’ experiences of video consultations: A qualitative systematic review by Lina Ärlebrant, Robyn Schimmer and Anette Edin-Liljegren in DIGITAL HEALTH
Supplemental Material
sj-docx-5-dhj-10.1177_20552076251404513 - Supplemental material for Patients’ experiences of video consultations: A qualitative systematic review
Supplemental material, sj-docx-5-dhj-10.1177_20552076251404513 for Patients’ experiences of video consultations: A qualitative systematic review by Lina Ärlebrant, Robyn Schimmer and Anette Edin-Liljegren in DIGITAL HEALTH
Footnotes
Acknowledgements
A special thanks to Information Specialist Mattias Lennartsson at Umeå University Library and PhD Åsa Holmner for their support and help during the initial phase of this systematic review. The authors would like to thank David J Boothroyd for proofreading the manuscript before submission.
Ethical considerations
All data included in this review were derived from publicly available sources, and no primary data collection involving human participants was conducted. Therefore, ethical approval was not required.
Consent to participate
Not applicable.
Consent for publication
All authors have agreed to the publication.
Contributorships
LÄ was involved in study design, search strategy, literature search, duplicates removal, study selection, quality assessment, data extraction, data synthesis, quality appraisal, and manuscript writing; and RS and AEL in duplicates removal, study selection, quality assessment, data extraction, data synthesis, quality appraisal, manuscript review, and comments.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Open access funding was provided by Umeå University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The authors declare that this review is reported according to the PRISMA statement guidelines for systematic reviews, and in line with the “Enhancing transparency in reporting the synthesis of qualitative research” (ENTREQ) statement. The protocol for this review was registered in the International prospective register of systematic reviews (PROSPERO; Registration ID: CRD42022330476). Details regarding the assessment of confidence are fully public at ![]() .
.
Supplemental material
Supplemental material for this article is available online.
Appendix 1. Search strategy

| PUBMED | CINAHL | PSYCHINFO | WEB OF SCIENCE | COCHRANE | |
|---|---|---|---|---|---|
| #1 | telecommunications [mesh] OR telemedicine [mesh] OR “health personnel” [mesh] OR health [mesh] OR teleconferenc* [tiab] OR telehealth* [tiab] OR health* [tiab] OR OR telerehabilitation* [tiab] OR telecommunication* [All fields] OR “remote consultation*” [All fields] OR telemedicine [All fields] OR teleconsultation* [All fields] OR “tele consultation*” [All fields] OR tele-consultation* [All fields] |
SU “health personnel” OR SU health OR teleconsultation* OR SU “tele consultation*” OR telerehabilitation* OR SU telehealth* OR TI teleconferenc* OR AB teleconferenc* OR TI health* OR AB health* OR TX telecommunication* OR TX “remote consultation*” OR TX telemedicine OR TX teleconsultation* OR TX “tele consultation*” OR TX tele-consultation* |
SU “telecommunication media*” OR SU “teleconsultation*” OR SU “tele consultation*” OR SU “telemedicine” OR SU “health personnel” OR SU Health OR SU “telepsychiatry” OR SU “telepsychology” OR SU “online therapy” OR SU telerehabilitation* OR SU telehealth* OR TI “teleconferenc*” OR AB “teleconferenc*” OR TI health* OR AB health* OR TX telecommunication* OR TX “remote consultation*” OR TX telemedicine OR TX teleconsultation* OR TX “tele consultation*” OR TX tele-consultation* |
ALL = (“teleconsultation*” OR “tele consultation*” OR tele-consultation* OR “health personnel” OR telemedicine OR telecommunication* OR “remote consultation*”) OR TI = (teleconferenc* OR telehealth* OR health* OR telerehabilitation*) OR AB = (teleconferenc* OR telehealth* OR health* OR telerehabilitation) |
[mh telecommunications] OR [mh telemedicine] OR [mh “health personnel”] OR [mh health] OR teleconferenc*:ti,ab OR telehealth*:ti,ab OR health*:ti,ab OR telerehabilitation*:ti,ab OR telecommunication* OR “remote consultation*” OR telemedicine OR teleconsultation* OR “tele consultation*” OR tele-consultation* |
| #2 | videoconferencing [mesh] OR “video-based intervention*” [All fields] OR “video teleconferenc*” [All fields] OR videoconferenc* [All fields] OR “video conferenc*” [All fields] OR "video communication*"[All fields] OR "video consultation*” [All fields] OR "video telehealth*” [All fields] OR "video visit*” [All fields] OR “live video” [All fields] OR “real-time video” [All fields] OR “real time video” [All fields] OR “video call*” [All fields] |
TX “video-based intervention*” OR TX “video teleconferenc*” OR TX videoconferenc* OR TX “video conferenc*” OR TX “video communication*” OR TX “video consultation*” OR TX “video telehealth*” OR TX “video visit*” OR TX “live video” OR TX “real-time video” OR TX “real time video” OR TX “video call*” |
SU “audiovisual communications media” OR TX “video-based intervention*” OR TX “video teleconferenc*” OR TX videoconferenc* OR TX “video conferenc*” OR TX “video communication*” OR TX “video consultation*” OR TX “video telehealth*” OR TX “video visit*” OR TX “live video” OR TX “real-time video” OR TX “real time video” OR TX “video call*” |
ALL = (videoconferenc* OR “video-based intervention*” OR “video teleconferenc*” OR videoconferenc* OR “video conferenc*” OR “video communication*” OR “video consultation*” OR “video telehealth*” OR “video visit*” OR “live video” OR “real-time video” OR “real time video” OR “video call*” | [mh videoconferencing] OR “video-based intervention*” OR video teleconferenc*” OR videoconferenc* OR “video conferenc*” OR videocommunication* OR “video consultation*” OR “video telehealth*” OR “video visit*” OR “live video” OR “real-time video” OR “real time video” OR “video call*” |
| #3 | “health care quality, access, and evaluation” [mesh] OR “professional-patient relations” [mesh] OR “nurse-patient relations” [mesh] OR “physician-patient relations” [mesh] OR “patient satisfaction” [mesh] OR “patient preference” [mesh] OR perception [mesh] OR “patient* experience*” [All fields] OR perception* [All fields] OR "professional-patient relation*” [All fields] OR “nurse-patient relation*” [All fields] OR “physician-patient relation*” [All fields] OR “patient* satisfaction*” [All fields] OR “patient* attitude*” [All fields] OR “patient* preference*” [All fields]) |
MH “quality of health care+” OR TX “health care quality, access, and evaluation” OR TX “patient* experience*” OR TX perception* OR TX “professional-patient relation*” OR TX “nurse-patient relation*” OR TX “physician-patient relation*” OR TX “patient* satisfaction*” OR TX “patient* attitude*” OR TX “patient* preference*” | SU “client attitude*” OR SU “client satisfaction” OR TX “health care quality, access, and evaluation” OR TX “patient* experience*” OR TX perception* OR TX “professional-patient relation*” OR TX “nurse-patient relation*” OR TX “physician-patient relation*” OR TX “patient* satisfaction*” OR TX “patient* attitude*” OR TX “patient* preference*” | ALL = (“health care quality, access, and evaluation” OR “patient* experience*” OR perception* OR “professional-patient relation*” OR “nurse-patient relation*” OR “physician-patient relation*” OR “patient* satisfaction*” OR “patient* attitude*” OR “patient* preference*”) OR TS = (“health care” NEAR/3 (quality OR access OR evaluation)) |
[mh “health care quality, access, and evaluation”] OR [mh “professional-patient relations”] OR [mh “nurse-patient relations”] OR [mh “physician-patient relations”] OR [mh “patient satisfaction”] OR [mh “patient preference”] OR [mh perception] OR “patient* experience*” OR perception* OR “professional-patient relation*” OR “nurse-patient relation*” OR “physician-patient relation*” OR “patient* satisfaction*” OR “patient* attitude*” OR “patient* preference*” |
Appendix 2. Search strings
Appendix 3. Level of confidence according to CERQual approach

| Summarised review finding | Confidence | Methodological limitations | Coherence | Adequacy | Relevance | Studies contributing to the review finding |
|---|---|---|---|---|---|---|
| Main theme 1: Suitable for less complex issues when technical problems can be solved | ||||||
| Theme 1. Less time, effort, and travel, and more accessible. Patients feel that VC saves time, effort, energy, and trouble. Worth a lot for the persons not feeling unwell. Easy access also led to feelings of security, control, less anxiety and stress. Not having to arrange for travels was associated with a lot of benefits | High confidence | No/very minor concerns regarding methodological limitations | No/very minor concerns regarding coherence | No/very minor concerns regarding adequacy | No/very minor concerns regarding relevance regarding relevance because the context in our review question is health care and the data supporting this theme is only from healthcare. Our population are patients, and we have only extracted data where we have been able to the identify the patient's perspective | Andrews et al., 2023; Chan et al., 2020; Christensen et al., 2020; Granberg et al., 2021; Grīnfelde, 2022; Koppel et al., 2022; Lawson et al., 2022; Mathar et al., 2015; Moeller et al., 2022; Nissen & Lindhardt, 2017; Nordtug et al., 2021; Parkinson et al., 2021; Shulver et al., 2016 |
| Theme 2. Shorter waiting times for booking appointments. Patients feel that VC was preferred because it meant less waiting when receiving bad or important news | Moderate confidence | Moderate concerns regarding methodological limitations because only 1 ref of 3 had high reliability. 2 had unclear recruitment strategies. Nothing written on relationship | Minor concerns regarding coherence because there are only a few codes supporting this and it's not clear why some patients had a feeling of less waiting with VC | Moderate concerns regarding adequacy due to the number of studies and the data is not rich in detail regarding circumstances and context | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable. 4 of 13 studies contribute to this theme, all from different healthcare contexts | Andrews et al., 2023; Chan et al., 2020; Granberg et al., 2021; Grīnfelde, 2022; Nordtug et al., 2021 |
| Theme 3. VC for shorter, less complicated issues. Patient experience VC as shorter which suits brief follow ups. It was meaningful time spent. VC is not a good option in acute situations or to assess complications, treatment decisions, or sensitive subjects | High confidence | Moderate concerns regarding methodological limitations because all studies have low or moderate reliability except one (Mathar). Recruitment strategy was unknown or performed by provider, researcher and relations towards participants was not stated | Minor concerns because many experience VC as more appropriate for follow-up and short visits, less for acute situations | No/very minor concerns regarding adequacy because most data support this theme | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable | Andrews et al., 2023; Chan et al., 2020; Christensen et al., 2020; Granberg et al., 2021; Grīnfelde, 2022; Koppel et al., 2022; Mathar et al., 2015; Moeller et al., 2022; Nordtug et al., 2021; Parkinson et al., 2021 |
| Theme 4. Overcoming technical problems and discomfort. Patients change their attitude after trying VC. Acceptance came with familiarity but for some, help and support was a must. Technical issues led to feelings of frustration, mistrust, incompetence and concerns | High confidence | Minor concerns regarding methodological limitations because of lacking details on recruitment and researcher-participant relations. This was however assessed as having only minor implications on this theme | No/very minor concerns regarding coherence. Important to remember the individuals’ different prerequisites, some learn and some needs help | No/very minor concerns regarding adequacy because most data support this theme and are rich in details | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable | Chan et al., 2020; Christensen et al., 2020; Granberg et al., 2021; Grīnfelde, 2022; Koppel et al., 2022; Lawson et al., 2022; Nordtug et al., 2021; Shulver et al., 2016 |
| Main theme 2: Feeling secure, relaxed, and having mutual focus in an equitable partnership | ||||||
| Theme 5. A sense of privacy and security at home. Patients feel that VC offers security and privacy in the comfort of home which is appreciated and contributes to feeling calm and empowered | High confidence | Minor concerns regarding methodological limitations because half of the studies had low or moderate reliability, and the other half high reliability | Minor concerns regarding coherence because a considerable amount data supports this theme. There is, however, also data suggesting that certain conditions must be in place for patients to feel secure with VC at home, e.g., support from family, possibility to contact at any time, the feeling of safety at home | No/very minor concerns regarding adequacy because most data support this theme | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable | Chan et al., 2020; Christensen et al., 2020; Granberg et al., 2021; Grīnfelde, 2022; Mathar et al., 2015; Nissen & Lindhardt, 2017; Nordtug et al., 2021; Shulver et al., 2016 |
| Theme 6. Having more time, relaxation, and focus. Patients feel relaxed in VC. Conversations are concentrated and focused | Moderate confidence | Moderate concerns regarding methodological limitations because of lacking details on recruitment and researcher-participant relations in most studies. 2 studies had high reliability | Minor concerns regarding coherence because most of the data support the theme. However, there is also data suggesting that VC meetings were experienced as shorter and with forced tempo. There is also contradictive data where patients felt relaxed and had more time available | Minor concerns regarding adequacy because of lack of supporting data. Suggests that time is context dependent | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable | Andrews et al., 2023; Christensen et al., 2020; Granberg et al., 2021; Grīnfelde, 2022; Koppel et al., 2022; Nordtug et al., 2021; Shulver et al., 2016 |
| Theme 7. Feeling on the same level. Patients feel self-determinate and responsible in their care while being more equal to the healthcare professionals and in co-planning | Moderate confidence | Minor concerns regarding methodological limitations because 2 of the studies have high reliability, one moderate and one low. Lacking details on recruitment and researcher–participant relations | No/very minor concerns regarding coherence | Moderate concerns regarding adequacy because few studies contribute with supporting data | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable. 4 studies contributed to this theme, all from different healthcare contexts | Andrews et al., 2023; Christensen et al., 2020; Granberg et al., 2021; Koppel et al., 2022; Nissen & Lindhardt, 2017 |
| Theme 8. Positive to be able to see healthcare professionals. Patients appreciate to see the healthcare professionals. It improves the communication and led to control and relational benefits | High confidence | Minor concerns regarding methodological limitations because some of the studies have low reliability and lack details on recruitment and researcher-participant relations. However, 10 of 13 studies contributed data for this theme | No/very minor concerns regarding coherence. Remember that some found it negative to see themselves on camera | No/very minor concerns regarding adequacy because most of the data supported this theme | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable | Andrews et al., 2023; Chan et al., 2020; Christensen et al., 2020; Granberg et al., 2021; Grīnfelde, 2022; Koppel et al., 2022; Lawson et al., 2022; Mathar et al., 2015; Moeller et al., 2022; Nissen & Lindhardt, 2017; Nordtug et al., 2021; Parkinson et al., 2021 |
| Theme 9. Needs are met similarly to FTF. Patients is satisfied with VC, would choose it again and recommend it, even to examine visual symptoms.VC is found personal and no different than FTF | Moderate confidence | Moderate concerns regarding methodological limitations because most of the studies were assessed as having moderate reliability | Minor concerns regarding coherence because a lot of data supports the theme, however, there are also contradictory data where patients expressed experiences pointing in opposite directions | No/very minor concerns regarding adequacy | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable | Andrews et al., 2023; Chan et al., 2020; Christensen et al., 2020; Granberg et al., 2021; Grīnfelde, 2022; Koppel et al., 2022; Lawson et al., 2022; Mathar et al., 2015; Moeller et al., 2022; Nissen & Lindhardt, 2017; Nordtug et al., 2021; Shulver et al., 2016 |
| Main theme 3: Limitations regarding personal needs and practical help | ||||||
| Theme 10. Does not add anything and is insufficient. VC is not enough and a disadvantage for complex needs | High confidence | Minor concerns regarding methodological limitations because the studies have high or moderate reliability but are only 5 | No/very minor concerns regarding coherence because this seem to be true for patients with a lot of knowledge about their own disease and when VC is booked ‘just because’ without a need for it | Minor concerns regarding adequacy because of the quantity of the data | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable | Christensen et al., 2020; Granberg et al., 2021; Mathar et al., 2015; Moeller et al., 2022; Parkinson et al., 2021; Shulver et al., 2016 |
| Theme 11. More difficult to talk and ask questions. It is difficult to go into complex issues, ask questions, and open up. Disturbing technical problems prevent emotional conversations. Not being able to call whenever needed is a drawback | High confidence | Minor concerns regarding methodological limitations because of the contributing studies to this theme, 3 studies have moderate reliability and 2 have high reliability | No/very minor concerns regarding coherence because this is true for some patient while others experience it as easier to talk over VC. There is a theme saying that VC is only suitable for shorter, less complicated issues which also strengthen this theme | Minor concerns regarding adequacy because although only a few studies support the theme, this is likely to be an experience that some patients have | No/very minor concerns regarding relevance | Andrews et al., 2023; Christensen et al., 2020; Granberg et al., 2021; Grīnfelde, 2022; Koppel et al., 2022; Moeller et al., 2022; Nissen & Lindhardt, 2017; Shulver et al., 2016 |
| Theme 12. Physical exam and practical help are limited. It is negative that physical exams and practical help with paperwork and information material is limited since it is important. To consult others and get translation service is not possible in VC | High confidence | Minor concerns regarding methodological limitations because of variations in quality. Half of the studies had high reliability, one moderate and one low. Lacking details on recruitment and researcher-participant relations | No/very minor concerns regarding coherence | Minor concerns regarding adequacy because of the large quantity of data. Concerns that this theme might be pruned to be diagnose specific | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable | Chan et al., 2020; Granberg et al., 2021; Grīnfelde, 2022; Lawson et al., 2022; Moeller et al., 2022; Nissen & Lindhardt, 2017; Shulver et al., 2016 |
| Main theme 4: Increased vulnerability and lack of emotional feedback | ||||||
| Theme 13. Challenges to the patient-healthcare professional relationship. It is beneficial to have an established relationship before VC and to meet first FTF. A relationship only on VC is not enough and patients prefer FTF consultations over VC | High confidence | Minor concerns regarding methodological limitations because only half of the studies have high reliability | No/very minor concerns regarding coherence because there is substantial data supporting the patient experience expressed in this theme | No/very minor concerns regarding adequacy | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable | Andrews et al., 2023; Chan et al., 2020; Christensen et al., 2020; Granberg et al., 2021; Grīnfelde, 2022; Koppel et al., 2022; Lawson et al., 2022; Mathar et al., 2015; Moeller et al., 2022; Nissen & Lindhardt, 2017; Nordtug et al., 2021; Parkinson et al., 2021; Shulver et al., 2016 |
| Theme 14. Patients are more vulnerable at home. A good support system, like family, is crucial and patients feel more vulnerable at home. Home is a private space, and some did not like to see themselves on camera | High confidence | Moderate concerns regarding methodological limitations because of variations in quality. Two studies were assessed as having low reliability, two with high reliability and the rest with moderate reliability | No/very minor concerns regarding coherence because the patients are more vulnerable at home, because it's revealing more about their personal life. But on the other hand, the security of being at home can also be experienced. This is two-folded | Minor concerns regarding adequacy because there is substantial data supporting this theme | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable | Andrews et al., 2023; Granberg et al., 2021; Koppel et al., 2022; Mathar et al., 2015; Moeller et al., 2022; Nordtug et al., 2021; Parkinson et al., 2021 |
| Theme 15. Less personal and provides less emotional support. VC is less personal, and some feel unimportant, rushed, just like the next person in line. To interpret reactions is difficult and to feel compassion, comfort, and reassurance. Patients feel insecure, distant, worried and anxious during VC | High confidence | Minor concerns regarding methodological limitations because of lacking details on recruitment and researcher-participant relations. Two studies with high reliability. Missing information on recruitment strategies was assessed as having low impact on this particular theme | No/very minor concerns regarding coherence | No/very minor concerns regarding adequacy because there is substantial data supporting this theme | No/very minor concerns regarding relevance because the supporting data origins from healthcare only. Data was only collected when patient perspectives were identifiable | Andrews et al., 2023; Chan et al., 2020; Christensen et al., 2020; Granberg et al., 2021; Koppel et al., 2022; Lawson et al., 2022; Moeller et al., 2022; Parkinson et al., 2021; Shulver et al., 2016 |
| Theme 16. Creates obligations and pressure. VC interfere with daily life which is disturbing and to feel stuck in front of the screen at home is an unwanted obligation and a tiresome customary routine | Moderate confidence | Minor concerns regarding methodological limitations because of variations in quality. 3 of the studies have high reliability | Minor concerns regarding coherence. Data shows the importance of VC supporting a specific purpose and it should not to be implemented without a reason or need. There is also contradictive data supporting the opposite, patients experiencing VC as relaxing | Minor concerns regarding adequacy because only a few studies support this data | No/very minor concerns regarding relevance | Andrews et al., 2023; Grīnfelde, 2022; Koppel et al., 2022; Mathar et al., 2015; Moeller et al., 2022; Shulver et al., 2016 |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.