
Abstract
This study tested a structural model examining the effects of perceived usefulness, perceived ease of use, attitude, subjective norm, perceived behavioral control, health consciousness, and application-specific self-efficacy on the acceptance (i.e. behavioral intention and actual usage) of a computer-based chronic disease self-monitoring system among patients with type 2 diabetes mellitus and/or hypertension. The model was tested using partial least squares structural equation modeling, with 119 observations that were obtained by pooling data across three time points over a 12-week period. The results indicate that all of the seven constructs examined had a significant total effect on behavioral intention and explained 74 percent of the variance. Also, application-specific self-efficacy and behavioral intention had a significant total effect on actual usage and explained 17 percent of the variance. This study demonstrates that technology acceptance is determined by patient characteristics, technology attributes, and social influences. Applying the findings may increase the likelihood of acceptance.
Keywords
Introduction
Type 2 diabetes mellitus and hypertension are two highly prevalent diseases, affecting hundreds of millions of people worldwide.1,2 Management of the diseases requires patients’ adherence to various self-care activities, including regular self-monitoring of blood glucose (SMBG) and self-monitoring of blood pressure (SMBP). However, SMBG and SMBP can be challenging without proper support and resources.
To motivate and empower patients to involve themselves in self-monitoring, various forms of health information technology (IT) have emerged that enable patients’ measurement, recording, and sharing of vital signs; behavioral change; communication with caregivers and peers; and decision-making about care.3–5 However, for a variety of reasons, patients may not accept and adopt the technologies, and as a result, they do not experience the benefits.
In this study, we set out to develop a patient health IT acceptance model and examine it in a longitudinal setting using a data pooling analysis to understand the factors that affect the acceptance of a computer-based disease self-monitoring system among patients with type 2 diabetes mellitus and/or hypertension. The remainder of this article proceeds as follows: first, a review of empirical research on patients’ acceptance of health IT, the research model and its theoretical background, and the study hypotheses are provided; second, the study methodology is described; and third, the results, a discussion of the findings, and conclusions are presented.
Theoretical development and research model
Many studies examining the determinants of patients’ acceptance of health IT in longitudinal contexts have been qualitative. In one study, 6 patients who used telehealth for heart failure management for 2 to 6 months were interviewed. The results indicated that usage of the technology was affected by its perceived usability and usefulness and the disease conditions and personalities of the patients. A pre- and post-intervention interview study 7 examined patients’ experiences using a mobile telehealth-based application in their management of chronic obstructive pulmonary disease over 6 months. The study found that patients’ use of the application was associated with an increased awareness of the variability of symptoms and a sense of reassurance. A more recent study 8 used semi-structured focus groups and individual interviews to explore factors influencing patients’ use of a telerehabilitation intervention over 2 years. The results revealed that patients’ perceived improvement in their health conditions, emotional safety, and independence in self-care were the factors determining acceptance.
Health IT acceptance has also been studied using quantitative analyses. However, many of the studies adopted cross-sectional designs that did not demonstrate acceptance over time. Moreover, many of the studies that used longitudinal designs focused largely on the effects of demographic factors, such as patients’ age, gender, and race, on health IT acceptance.9–12 Examinations of other factors that are grounded in established models and theories and may influence acceptance are scarce. To this end, in this study, we developed a research model based on the technology acceptance model (TAM) 13 and theory of planned behavior (TPB) 14 and tested it in a longitudinal setting to understand factors influencing the acceptance of a computer-based health IT among chronically ill patients over a period of 12 weeks.
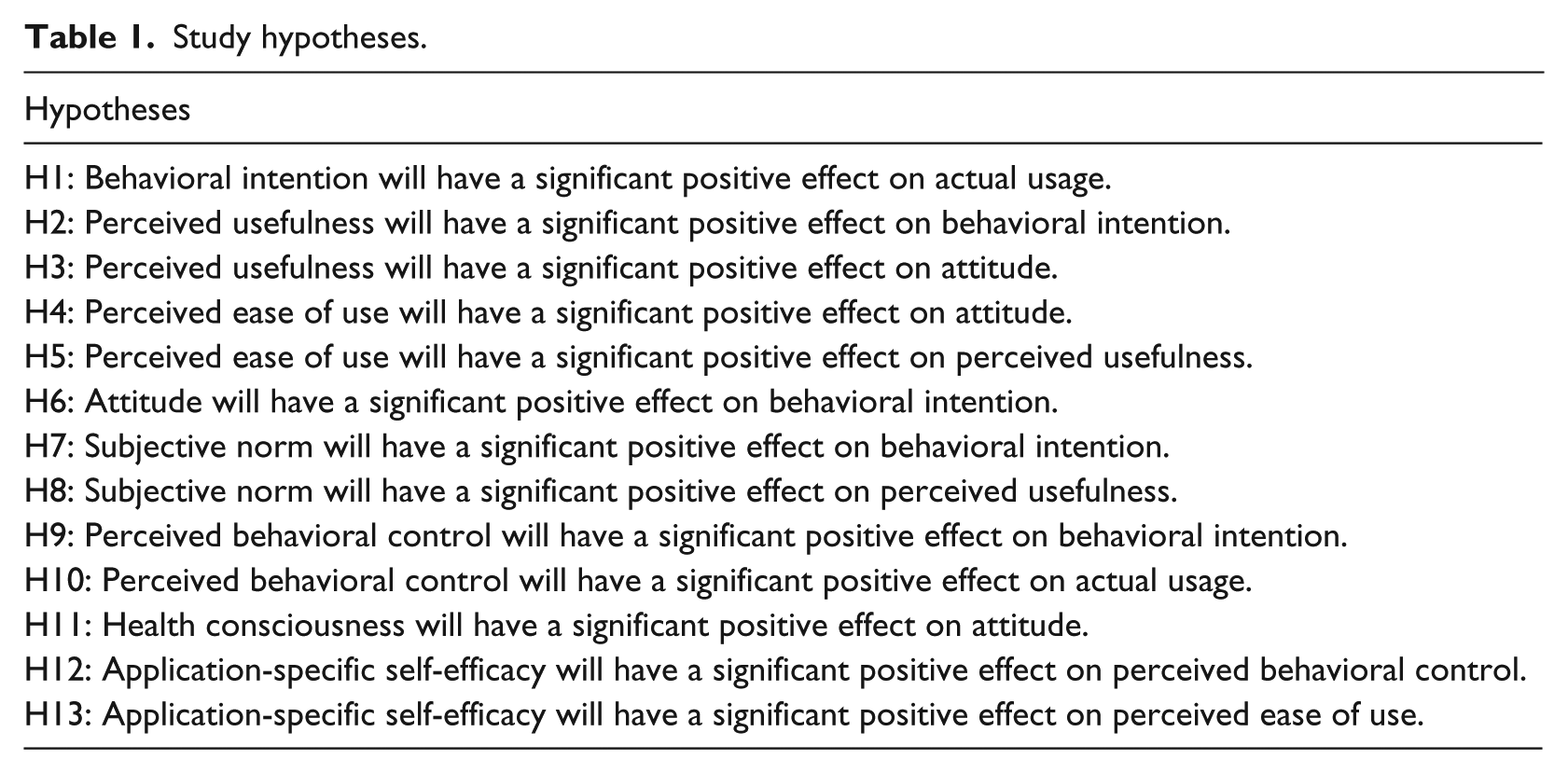
This study adopted the TAM and TPB as a theoretical basis for model development because they provide a credible foundation for examining individuals’ technology acceptance15,16 and health-related behaviors.17,18 The research model tested the effects of perceived usefulness, perceived ease of use, attitude, subjective norm, perceived behavioral control, health consciousness, and application-specific self-efficacy on acceptance, which was measured as both patients’ behavioral intention to use the technology and their actual usage behavior (see Figure 1). The specification of each of the constructs is presented below, and accordingly, 13 hypotheses were made and tested (see Table 1).
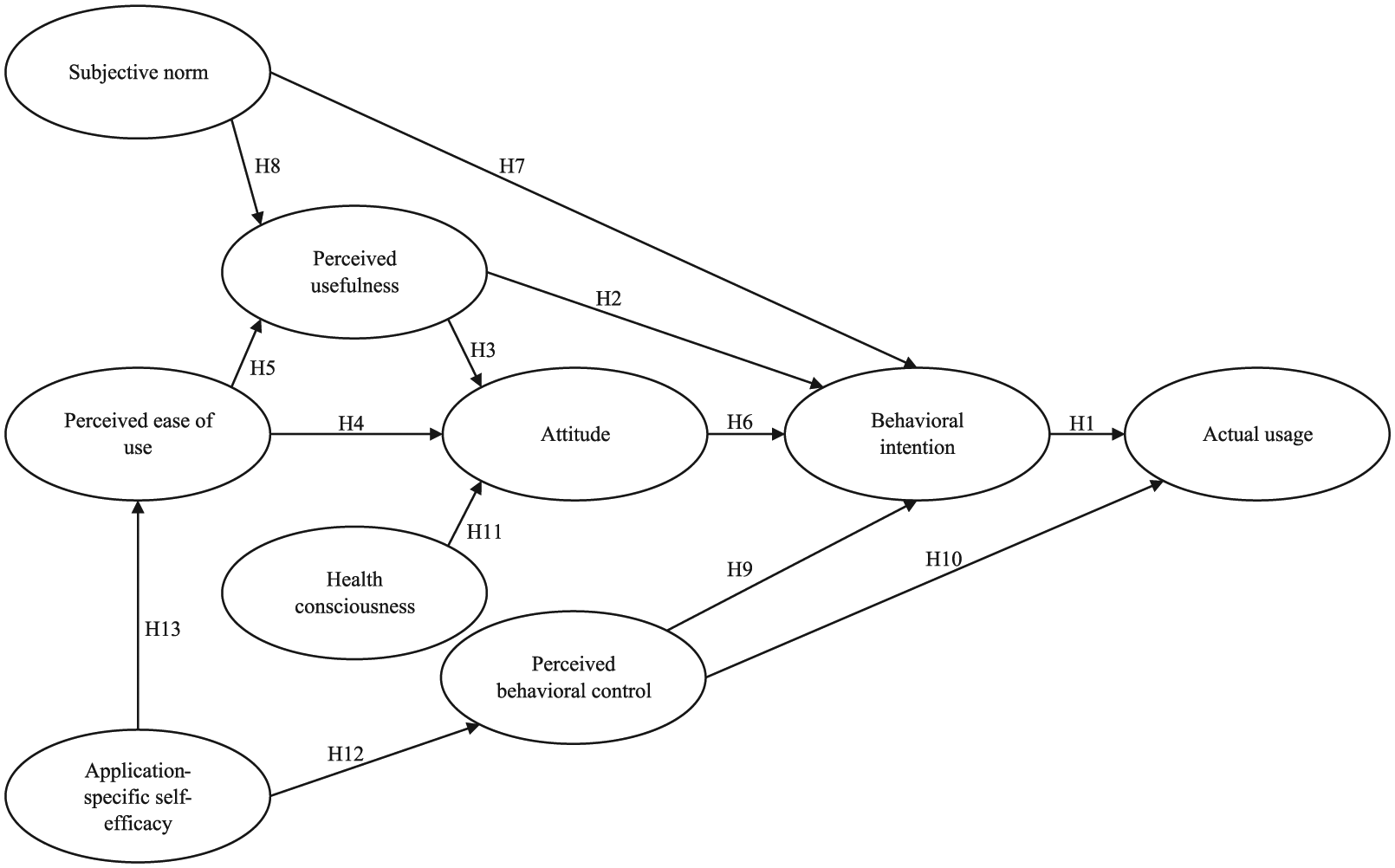
Research model.
Study hypotheses.
Behavioral intention and actual usage
In this study, behavioral intention, which refers to the strength of a patient’s intention to use health IT and is a measure that has been commonly used to indicate acceptance,19–21 was used to assess technology acceptance. In addition, patients’ actual usage of health IT was collected and used to assess the acceptance behavior. Based on the literature,14,22,23 we hypothesized that patients would be more likely to use health IT if they had the intention to use the technology (see H1).
Perceived usefulness
Perceived usefulness was drawn from the TAM, which in the context of this study refers to the degree to which a patient believes that using health IT will improve his/her ability and effectiveness in managing the disease. Healthcare research has shown this construct to be an important determinant of acceptance.24–26 It is believed that patients will have positive attitudes and intentions toward the use of health IT if they perceive the technology to be useful for their disease self-management (see H2 and H3).
Perceived ease of use
The TAM demonstrates that perceived ease of use significantly influences IT acceptance, mediated by perceived usefulness. This result has also been demonstrated in health IT studies.19,27 Moreover, perceived ease of use is associated with attitudes toward technology.28,29 In this study, perceived ease of use refers to the degree to which a patient believes that using health IT is free of effort. Based on the literature, it is believed that patients will be more likely to form positive attitudes toward the use of health IT and perceive the technology as useful if they feel it is easy to use (see H4 and H5).
Attitude
Attitude was drawn from both the TAM and the TPB to predict acceptance. In this study, the construct refers to a patient’s positive feelings about using health IT. Although the effect of attitude on acceptance is controversial outside the healthcare discipline, 30 literature studying acceptance among healthcare professionals has shown that attitude significantly influences behavioral intention.31–33 Therefore, it is believed that patients will be more likely to develop higher intentions toward using health IT if they have positive feelings about the technology (see H6).
Subjective norm
In this study, the concept of subjective norm was drawn from the TPB and refers to the degree to which a patient perceives that important others think he/she should use the health IT system. This construct was included in the research model because the opinions of important others may influence patients’ health-related behavior.34,35 A meta-analysis of IT acceptance found that subjective norm significantly influenced perceived usefulness and behavioral intention. 36 These findings are also seen in health IT acceptance research.19,37 Therefore, it is believed that patients will perceive the technology as useful and be more likely to have higher intentions toward using health IT if they perceive a positive social influence from important others (see H7 and H8).
Perceived behavioral control
Based on the TPB, perceived behavioral control in this study measured patients’ perceptions of the internal and external constraints of using health IT. Previous information systems research has shown this construct to be a significant determinant of intentions and behavior.23,38,39 However, studies examining perceived behavioral control in the context of health IT are relatively scarce. An exploration of its possible effect on patient health IT acceptance is needed (see H9 and H10).
Health consciousness
Health consciousness, which refers to the degree to which a patient focuses on or pays attention to his/her own health, was included in the research model because individuals’ health-related consciousness, beliefs, and activities are significantly correlated.40,41 Health ITs can be used by patients to facilitate disease self-management, which may increase the chances of staying healthy. It is therefore believed that health-conscious patients may be more likely to develop positive attitudes toward health ITs (see H11).
Application-specific self-efficacy
Based on social cognitive theories42,43 and other related studies,44,45 application-specific self-efficacy was integrated into the research model to examine patients’ beliefs in their operative capability to use health IT to accomplish a particular task. We are unaware of any studies that have examined this construct in the context of this study. However, previous information systems research suggests that self-efficacy is a significant antecedent of perceived ease of use45–47 and perceived behavioral control.38,48 This suggests that patients who believe they have the ability to use health IT may be more likely to perceive the technology as easy to use and exert better control over the technology (see H12 and H13).
Methods
Participants
The participants in the study were mainly recruited from three community health centers of a nonprofit health service network located in Hong Kong. Interested patients who knew about the study from other channels (e.g. introduced by friends) were also included in the screening for eligibility. Patients who met the following criteria were considered eligible for inclusion: (1) 18 years of age or older, (2) diagnosed with either hypertension or type 2 diabetes mellitus or both, (3) taking either antihypertensive medications or hypoglycemic medications or both for at least 3 months, (4) normal or corrected-to-normal eyesight, (5) able to learn and perform computer-based disease self-monitoring, (6) not physically or cognitively impaired, and (7) understood spoken and written Chinese. Patients who failed to meet the inclusion criteria or had life-threatening/unstable conditions were excluded.
Study intervention
The health IT system tested in this study was a computer-based chronic disease self-monitoring system. The system comprised a 10-inch touchscreen tablet computer, a two-in-one blood pressure and blood glucose meter, and a cable connecting the computer and the two-in-one device. A chronic disease self-monitoring application, which was developed based on a series of usability evaluations guided by human factors approaches, consultation with healthcare practitioners, and feedback from intended target users,49–51 was programmed to run on the tablet computer. The self-monitoring system could be used by patients to measure and keep track of their blood glucose, blood pressure, and heart rate. The system automatically fetched and stored the outcome readings after each measurement. Historical records were presented in structured tables and graphs in which normal values were shown in black and abnormal values were shown in orange or red based on the specific situations. Video-based educational materials about the causes of diabetes and hypertension and ways to manage the disease conditions were also provided in the system.
Procedure and outcome measures
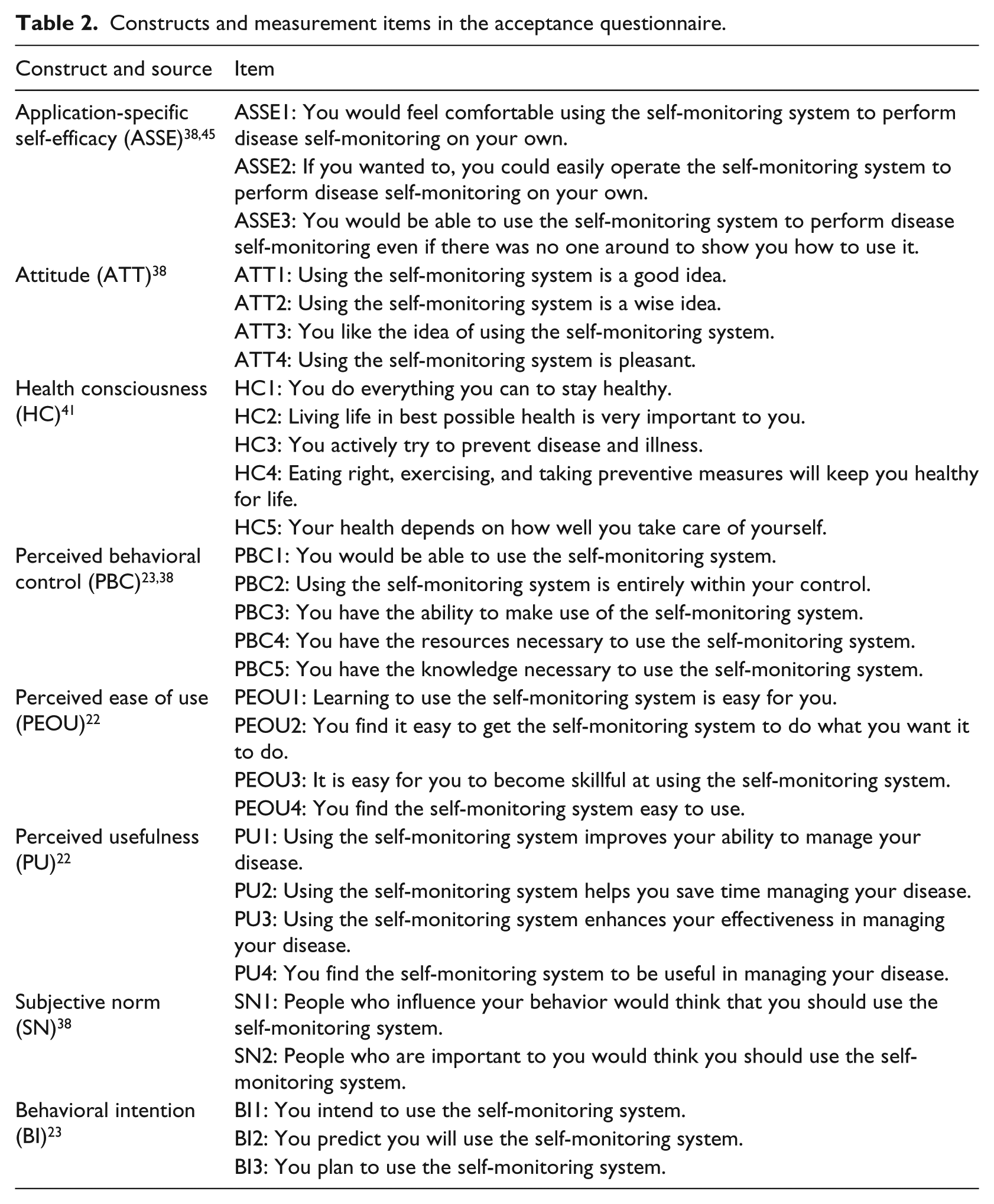
This study lasted for 12 weeks, during which participants were provided with the self-monitoring system, lancing devices, lancets, and blood glucose test strips at no cost. A technology acceptance questionnaire comprising the above-mentioned constructs was administered to participants during home visits conducted at baseline (BL), 4 weeks post-implementation (4W), and 8 weeks post-implementation (8W). The constructs were measured with items adapted from validated scales and adjusted to reflect the current context. Seven-point Likert-type scales, ranging from 1 (very strongly disagree) to 7 (very strongly agree), were used to rate the measurement items. Table 2 presents the constructs and items used in the questionnaire.
Constructs and measurement items in the acceptance questionnaire.
During the BL home visit, participants’ demographic information was collected, followed by a training to teach participants how to use the system. The actual usage of the technology was measured as the daily frequency of SMBP and/or SMBG conducted by participants using the system. Questionnaire data collected at each measurement time point were used to predict actual usage in the subsequent 4-week period. The system was withdrawn from participants after the 12 weeks’ intervention. Each participant received HK$200 upon completion of the study. Technical support was provided throughout the study period.
Ethics
The research team received institutional review board approval from the authors’ institution and obtained the written informed consent of the participants prior to data collection.
Data analysis
A power analysis was conducted using G*Power version 3.1 to determine the number of observations needed for model testing. Descriptive statistics of the measures including mean, standard deviation (SD), 95 percent confidence interval (CI), kurtosis, and skewness were calculated to determine the nature of the data. A partial least squares structural equation modeling (PLS-SEM) approach was used to test the research model using SmartPLS version 3. Pairwise deletion was used for handling missing data.
To increase the reliability of measurement 52 and the precision of parameter estimations,53,54 the observations collected at BL, 4W, and 8W were pooled across time. To examine the validity of pooling data across time, the assumption of independence in the pooled data was tested by examining the correlations among the error terms associated with the prediction of behavioral intention at the three measurement time points. This approach is consistent with previous research. 23
To assess the reliability and validity of the measures, the following criteria53,55 were used: Cronbach’s alpha and composite reliability of the constructs should be higher than 0.7, the average variance extracted (AVE) of the constructs should be higher than 0.5, the square root of the AVE of each construct should be higher than its correlations with any other constructs (Fornell–Larcker criterion), and a measurement item’s outer loading on its associated construct should be higher than 0.7 and greater than any of its cross loadings on other constructs. As actual usage was a single-item construct, these criteria were not applicable.
To test the research model, multicollinearity was first examined by computing the variance inflation factor (VIF) of the predictor constructs for each subpart of the model. VIF values of less than five were considered satisfactory in the context of PLS-SEM. 55 Path coefficients were estimated and their significance was determined by running 5000 bootstrap subsamples with observations randomly drawn from the pooled data. Coefficients of determination (i.e. R2 values) of the endogenous constructs were estimated to indicate the overall amount of variance that can be explained by the predictor constructs.
Results
Sample size and participant characteristics
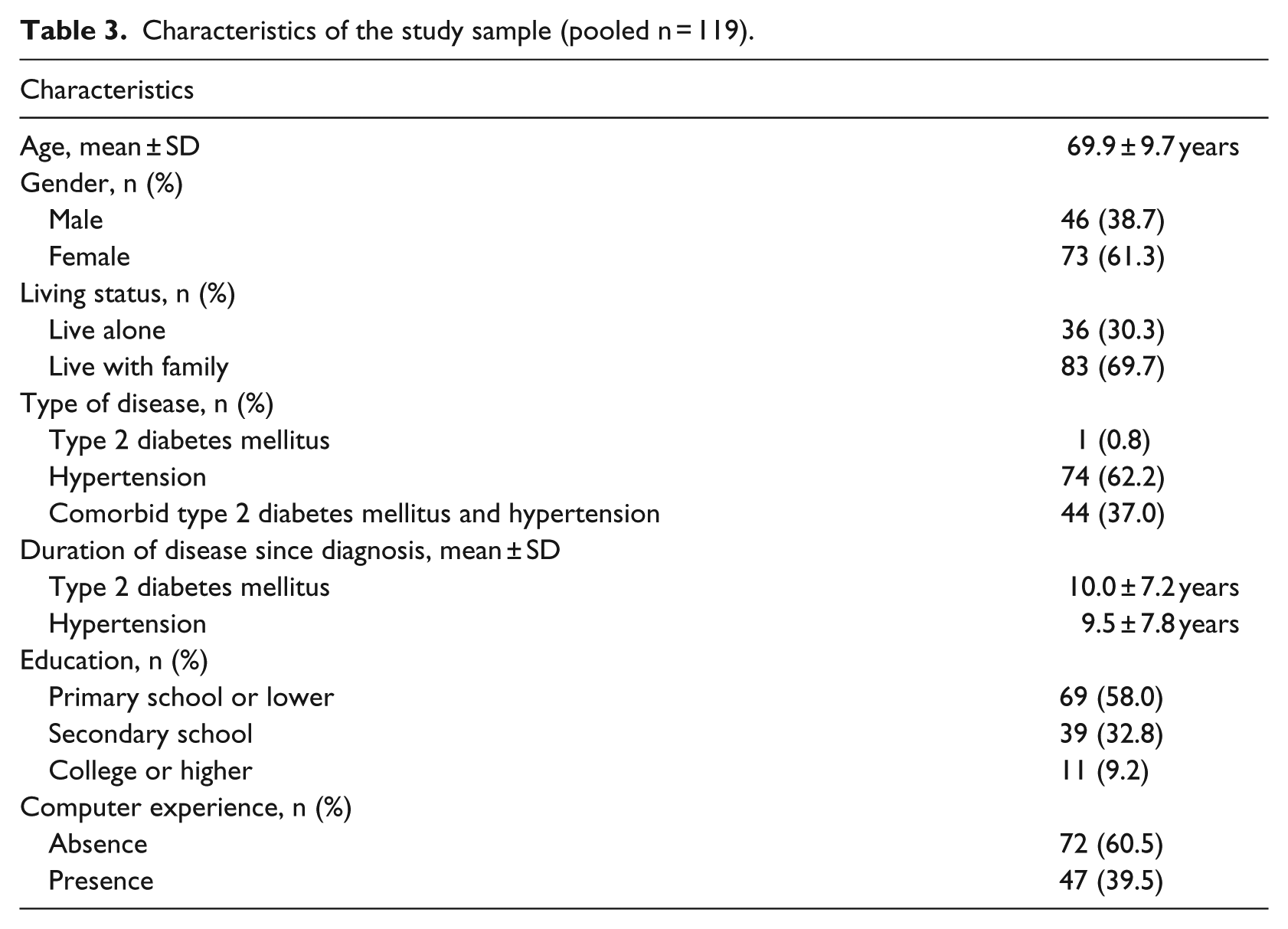
The power analysis indicated that 85 observations were needed to detect a medium effect size ƒ2 of 0.15 with an 80 percent statistical power at the 0.05 significance level for a two-tailed test. In this study, 42 patients were studied at BL. In total, 39 and 38 of the patients were studied at 4W and 8W, respectively. The reduced number of patients at 4W and 8W was due to patients lost to follow-up and study withdrawal. A total of 119 observations were generated by pooling data across time, which was believed to be sufficient for data analysis. Table 3 presents the demographic characteristics of the participants.
Characteristics of the study sample (pooled n = 119).
Descriptive statistics
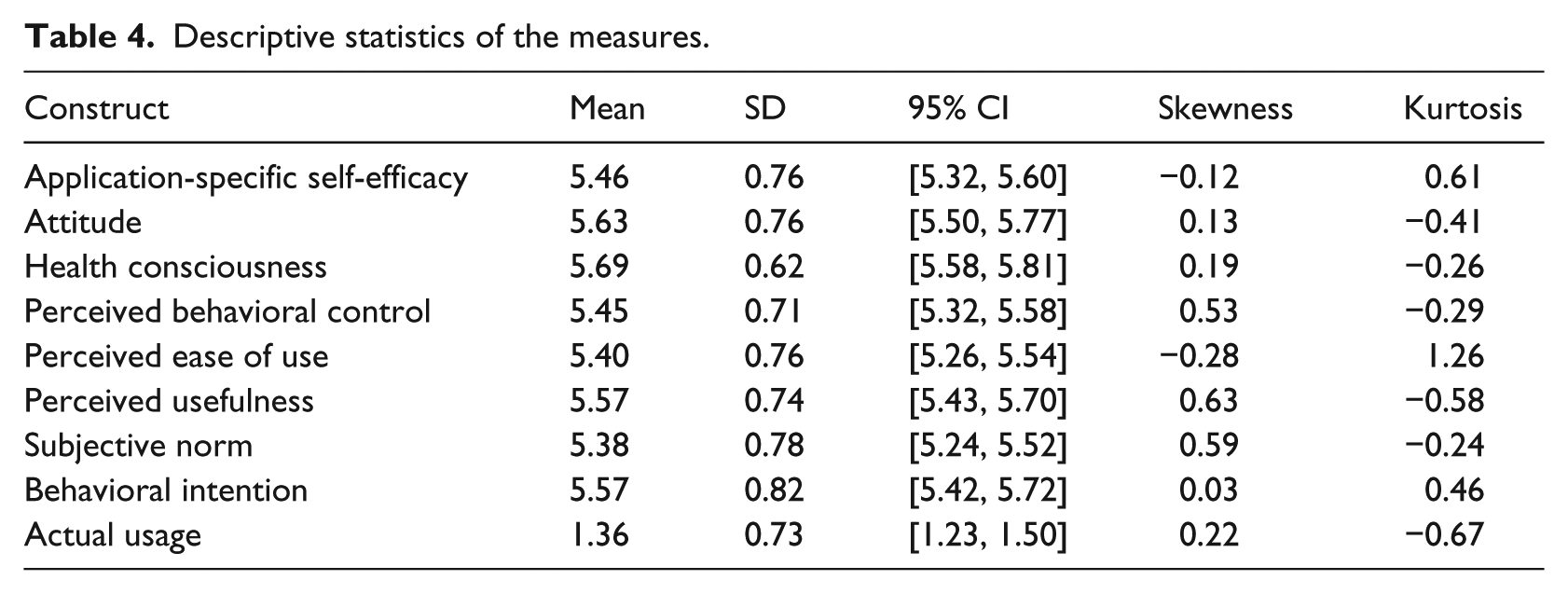
As shown in Table 4, on average, a patient used the system 1.36 (SD = 0.73) times each day during the study period. Patients’ average ratings for application-specific self-efficacy, attitude, health consciousness, perceived behavioral control, perceived ease of use, perceived usefulness, subjective norm, and behavioral intention ranged from 5.38 to 5.69; the lower bounds of the ratings were above five at the 95 percent confidence level. Except for perceived ease of use, the absolute values of skewness and kurtosis were less than 1, indicating normal distributions of the data.
Descriptive statistics of the measures.
Model testing
The results of the correlation analysis showed no significant relationships among the error terms associated with the prediction of behavioral intention at the three measurement time points (p-values ranged from 0.46 to 0.83). Therefore, the independence assumption in the pooled data was not violated.
As shown in Table 5, the values of Cronbach’s alpha and composite reliability for all constructs ranged from 0.74 to 0.97, indicating reasonable internal consistency of the measures. All AVE values were higher than 0.5, demonstrating satisfactory convergent validity. The discriminant validity of the measures was believed to be sufficient as all constructs fulfilled the Fornell–Larcker criterion, except that the square root of AVE for health consciousness was slightly lower than its correlation with attitude. The measurement items showed reasonable reliability and validity as all of the outer loadings of the items were higher than 0.7, except for the first item of health consciousness, and greater than their cross loadings (see Table 6).
Cronbach’s alpha, composite reliability, AVE, and the Fornell–Larcker test of the constructs.
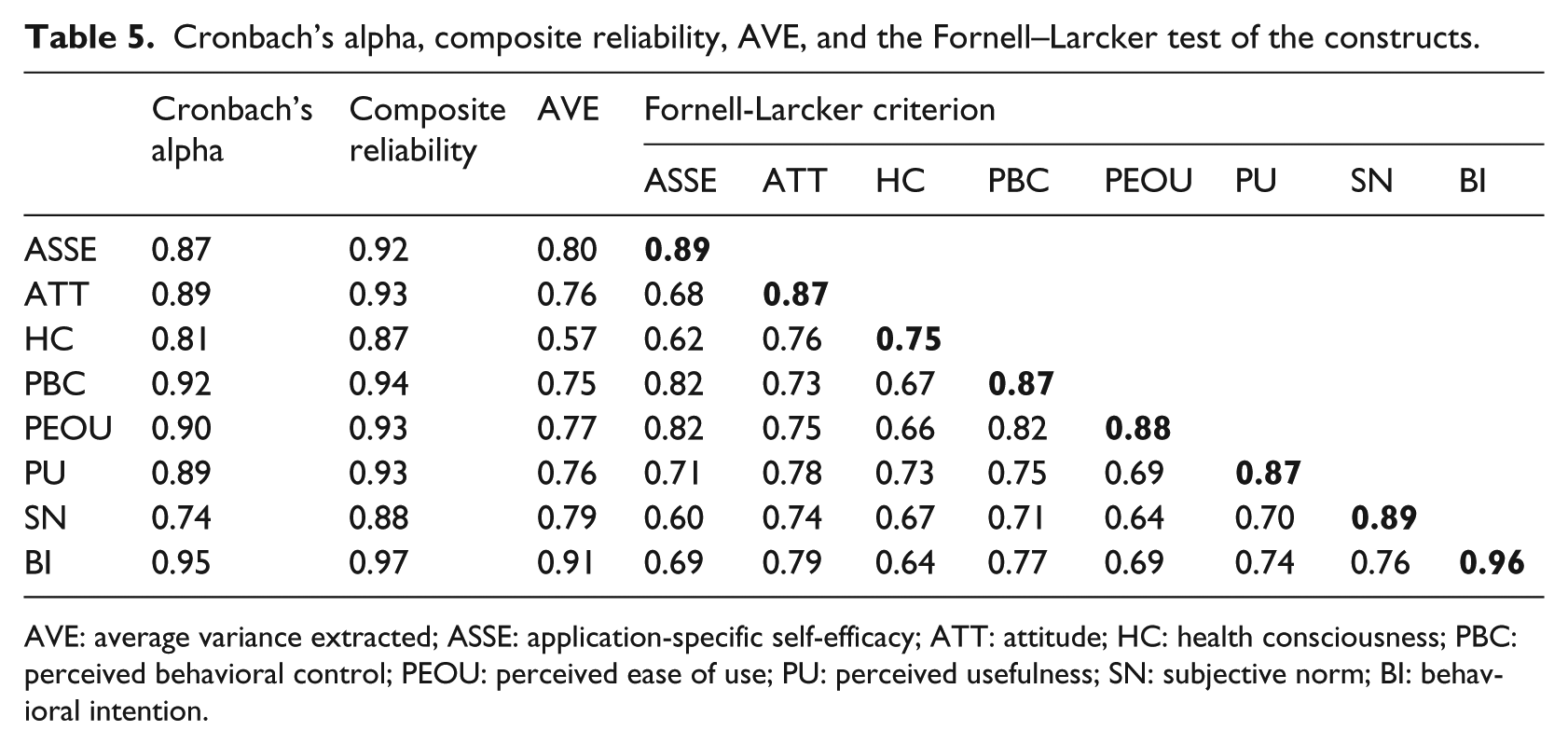
AVE: average variance extracted; ASSE: application-specific self-efficacy; ATT: attitude; HC: health consciousness; PBC: perceived behavioral control; PEOU: perceived ease of use; PU: perceived usefulness; SN: subjective norm; BI: behavioral intention.
Outer loadings and cross loadings for the measurement items.
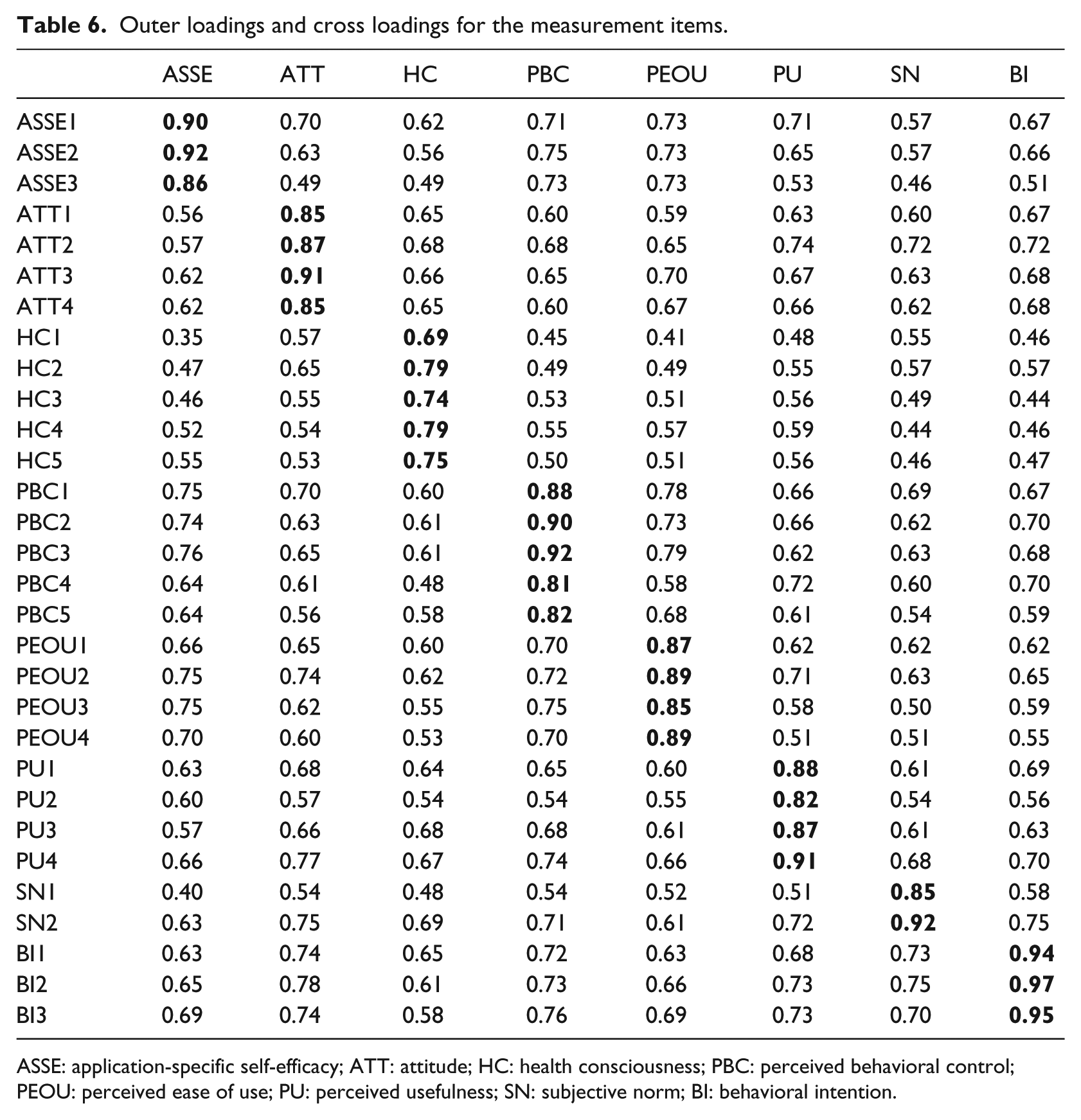
ASSE: application-specific self-efficacy; ATT: attitude; HC: health consciousness; PBC: perceived behavioral control; PEOU: perceived ease of use; PU: perceived usefulness; SN: subjective norm; BI: behavioral intention.
The results of the VIF calculation suggested the absence of multicollinearity issues. As shown in Table 7, 11 hypotheses were supported (H1, H3, H4, H5, H6, H7, H8, H9, H11, H12, and H13). In addition, the total effects of application-specific self-efficacy, health consciousness, perceived ease of use, and perceived usefulness on behavioral intention were significant, and the total effect of application-specific self-efficacy on actual usage was significant. Overall, the research model was able to explain 74 and 17 percent of the variance in behavioral intention and actual usage, respectively. The model testing results are illustrated in Figure 2.
Path coefficient estimation and bootstrapping results of the research model.
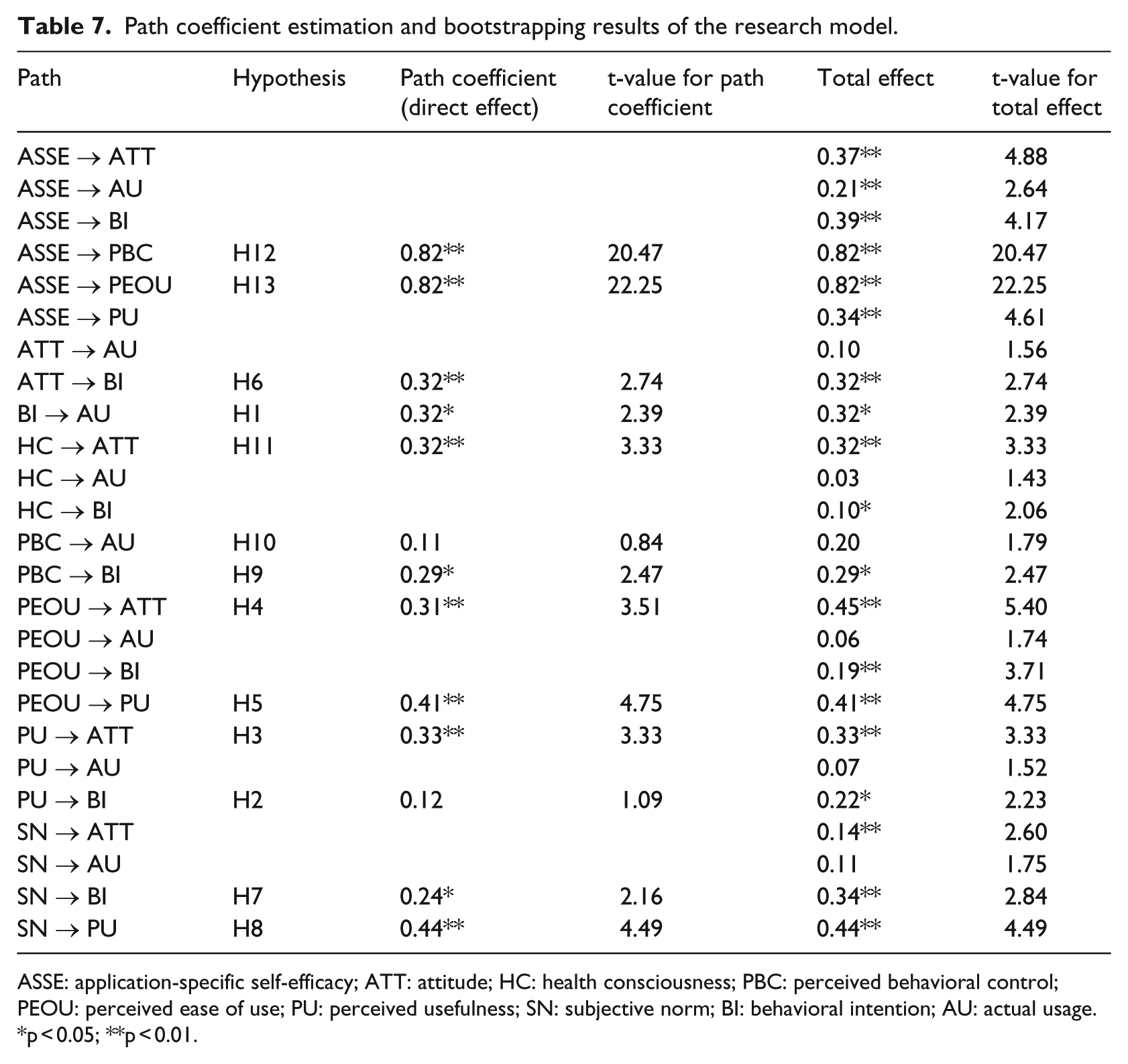
ASSE: application-specific self-efficacy; ATT: attitude; HC: health consciousness; PBC: perceived behavioral control; PEOU: perceived ease of use; PU: perceived usefulness; SN: subjective norm; BI: behavioral intention; AU: actual usage.
p < 0.05; **p < 0.01.
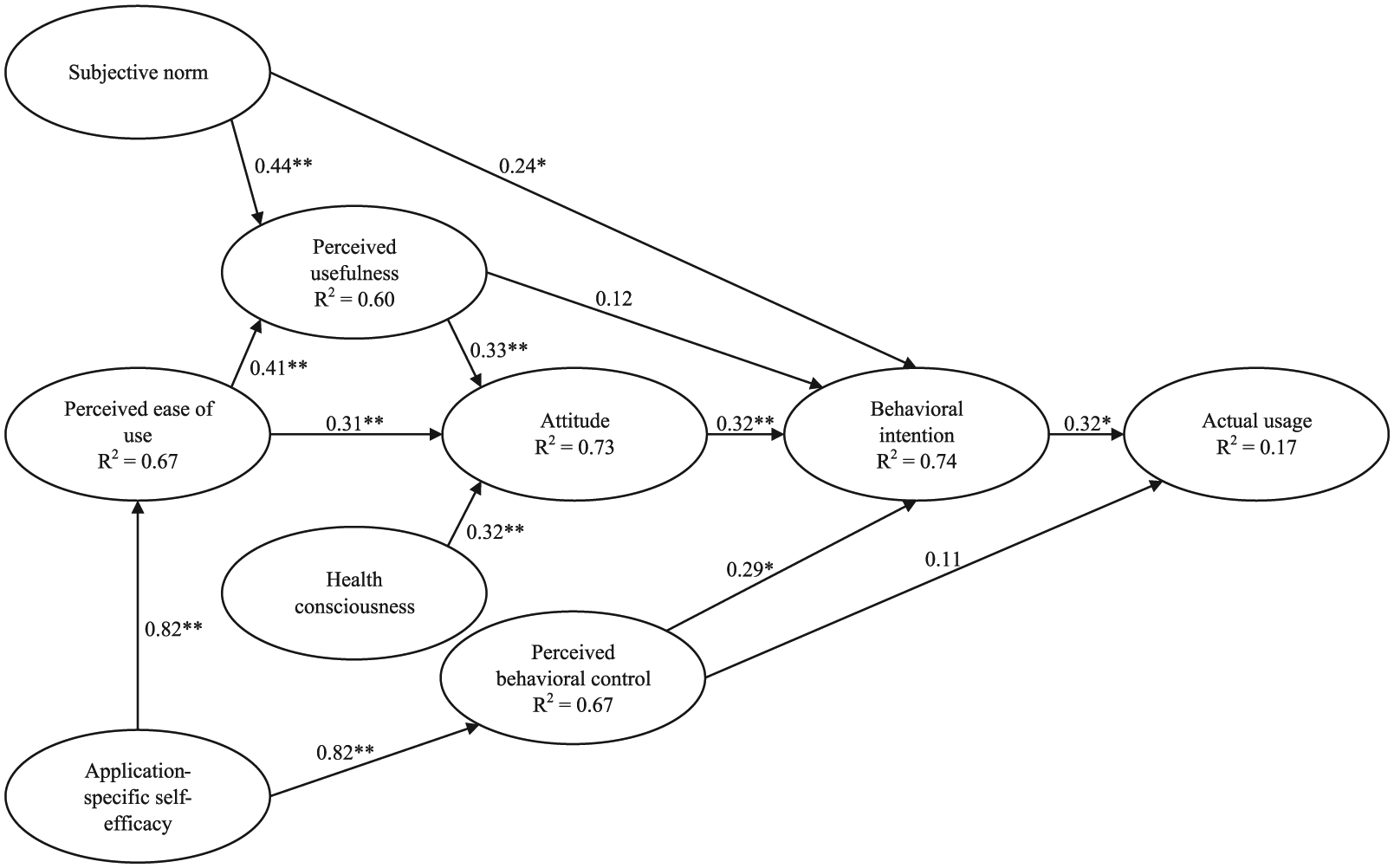
Model testing results from the PLS-SEM analysis (*p < 0.05; **p < 0.01).
Discussion
This study examined the acceptance of a computer-based chronic disease self-monitoring system among patients with type 2 diabetes mellitus and/or hypertension. The research model was developed by integrating context-specific constructs on the theoretical basis of the TAM and the TPB and tested using data collected over a 12-week period.
The research model tested in this study was able to explain 74 percent of the variance in behavioral intention, comparable to or outperforming previous models.20,56 Actual usage was significantly directly influenced by behavioral intention. However, the amount of variance in actual usage that was explained by behavioral intention was modest, which may be because the measures for actual usage were objective rather than self-reported.18,57 Although intentions to use health ITs may easily be formed, patients may not actually use the technologies in accordance with their intentions. An exploration of the unforeseen factors affecting actual usage is needed.
Contrary to what was expected, the direct effect of perceived usefulness on behavioral intention was insignificant. However, perceived usefulness exerted a significant total effect on behavioral intention, mediated by attitude (total effect = 0.218, p < 0.05), indicating that patients are more likely to form positive feelings and intentions toward the use of health ITs if they perceive the technologies as useful for their disease self-management. To promote usefulness, health ITs should be designed to improve patients’ ability to manage their diseases effectively and efficiently. Achieving this is likely to require careful studies of the intended target users’ needs, preferences, and expectations to provide information about what functions to incorporate in health ITs.
Perceived ease of use was found to significantly influence behavioral intention via perceived usefulness and attitude (total effect = 0.189, p < 0.01), underlining its importance in developing patients’ health IT acceptance. Therefore, we advocate not only focusing on the functions or features of the technology but also evaluating its usability to ensure that it is easy for the intended target users to use. Usability and user-centered design principles should be followed in the technology development process. 58 In particular, technology interventions with careful designs tailored for older adults are important because these patients are more likely to suffer from chronic conditions.59–61
Attitude significantly directly influenced behavioral intention and fully mediated the effects of perceived usefulness, perceived ease of use, and health consciousness on behavioral intention. This finding is different from previous studies outside the healthcare discipline, which overlooked the mediating effect of attitude on the causal relationships between beliefs and intentions.22,38 This implies that an individual’s attitude may play a relatively important role when it comes to the acceptance of health ITs. This study suggests the inclusion and further examination of attitude in future research works.
Consistent with previous research,36,37 subjective norm was shown to have a significant direct effect on perceived usefulness and behavioral intention, indicating that other people’s opinions may have an essential influence on patients’ perceptions of the usefulness of health ITs and the formation of patients’ behavioral intentions to use the technologies. Therefore, it is necessary that a positive social environment is cultivated to encourage and motivate patients in adopting health ITs. Patients’ important others, such as their family members, healthcare providers, and close friends, may want to express their positive attitudes toward patients’ use of health ITs by, for example, emphasizing the benefits of the technologies. It is also important that prompt help could be offered by these people when patients encounter difficulties in using the technologies.
The direct path from perceived behavioral control to actual usage was not supported in this study. However, behavioral intention was shown as a significant mediator between perceived behavioral control and actual usage. This suggests that when patients perceive themselves as able to control the health ITs, they are more likely to form positive intentions toward the use of the technologies, which in turn leads to a higher likelihood of actual usage; this might be especially the case for users who have prior experience with the technologies. 62 Therefore, adequate training before the technology is used might help patients become familiar with and gain experience using health ITs and consequently increase the chances of technology acceptance.
As expected, health consciousness and application-specific self-efficacy significantly influenced acceptance via multiple mediators, indicating that patients who actively try to prevent illness, maintain healthy lifestyles, and believe themselves capable of using health ITs to perform disease self-management would be more likely to accept the technologies. As patients are the principal users of health ITs, their proactive engagement in the interventions is especially important. Although the possession of health-related knowledge, awareness, and attitudes may vary across different individuals, there are ways to motivate and empower patients to assume more active roles in their disease self-management processes. For example, hospitals, nongovernmental organizations, and universities may take initiatives to offer more educational programs to enhance patients’ self-competence in self-care. In addition, an educational module integrated into health ITs that introduces knowledge such as nutrition intake, physical exercise, and emotion regulation may help to promote acceptance.
This study has several limitations. First, the effects of the constructs on technology acceptance may fluctuate over time as patients may have different focuses and concerns at different times.62–64 Although the data used in this study were collected at multiple time points, pooling data across time restricted us from testing such potential changes. Second, the number of constructs examined in this study was limited due to the small sample size. A research model examining a wider range of variables would be helpful to better understand patients’ acceptance of health ITs. Third, the study sample may not be representative of all patient populations. Most of the participants enrolled in this study were older adults with low educational levels and computer literacy, which may limit the generalizability of the findings. Moreover, the demographic factors, such as age, gender, and experience, can affect individuals’ acceptance and use of technologies. 23 Future research should be conducted to expand the model by exploring the potential impact of such factors on patients’ acceptance of health ITs.
Conclusion
The examination of the pooled data collected over the 12-week period supported most of the hypothesized paths in the research model, which explained a notable amount of variance in patients’ behavioral intention to use the disease self-monitoring system and their actual usage. Although the study may have provided useful insights into the research topic, the results await confirmation from future examinations with a larger sample size and longer duration. Hopefully, by applying the findings of this study in designing, developing, and implementing health IT, the chances of acceptance can be increased.
Footnotes
Author’s note
Mian Yan is now affiliated with “School of Electrical and Information Engineering, Jinan University (Zhuhai Campus), Zhuhai 519070, China” and “Institute of Physical Internet, Jinan University (Zhuhai Campus), Zhuhai 519070, China”.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was conducted with the support of the Theme-based Research Scheme of the Hong Kong Research Grants Council (grant no. T32-102/14-N).