
Abstract
Health Information Technology (HIT) systems are receiving increasing attention in recent years. Yet, individual adoption research in health care settings, especially in developing countries are quite limited. Moreover, large body of Information Systems research has focused on user perceptions to form intentions to use a particular technology. However, the antecedents and consequences of perceptions remained largely unanswered in existing research. This study aims to fill this gap by proposing and testing a research model based on a modified Technology Acceptance Model (m - TAM) which incorporates socio psychological and cognitive factors to assess the HIT’s adoption level of Turkish physicians. To do so, two different methods were used to collect data from head physicians, assistant head physicians, and physicians: face to face and online survey. Total 212 useful responses were returned. 174 of them were face-to-face surveys which were administrated to all the first level and some second and third level health organizations. The rest of the surveys were administrated to the second and third level healthcare organizations via online participation. Data were analyzed by Structural Equation Modelling via SmartPLS software program. Results present that commitment is a strong predictor of HIT usage, whereas neither motivation nor resistance has a significant impact on HIT usage.
Keywords
Introduction
Information and Communication Technologies (ICTs) have become a major internal part of any organization and represent significant amount of investment today. As ICTs have been employed largely in our organizations and incorporated into all organizational work roles and work processes, individuals’ technology adoption and use decision have become a critical issue in the assessment of success or failure of these systems. ICTs have been advancing more rapid rate than advancement of our understanding of them, 1 making it difficult to realize full potential of those technologies. Yet, utilization and continuing use of ICTs to full extend could enhance individual performance and organization competitiveness. 2 The real value of ICTs can only be realized, if they are fully utilized by their intended users to contribute strategic and operational goals of the organizations. 3
In our increasingly digital world and networked society, the volume of personal information captured and kept in electronic databases continue to grow at exponential rates 4 Health care is no exception. Health care industry have benefited recent technological advancements and established dependence on ICTs for maintaining patient records, scheduling, billing, accounting, materials management and management of clinical and administrative operations. 5 Health Information Technology (HIT) systems are a kind of ICT that allows health care providers to collect, store, retrieve and transfer clinical and administrative health information electronically. The widespread wisdom is that ICTs would transform the health care industry by containing costs, enabling consistently safer, high quality and more efficient medical care. 6 Health care organizations are trying to find ways to improve customer service and reduce health care providing costs by heavily utilizing ICTs and electronic patient databases. Health care professionals largely use Electronic Health Records (EHR) to manage health care delivery in today’s health care facilities. EHRs are the widely used version of HIT and enable to create, store and share individual data in electronic format. EHR Systems are the software platforms that physicians or hospitals use to create, store, share, update and manipulate EHRs for patients. 7 EHRs are so beneficial for health care providers that could reduce health care providing costs significantly 5 . EHRs can reduce record keeping time for health care professionals and enables historically related records to be accessed easily via integrated central computer system. 8
Although the health care organizations’ managers and academicians realize the importance of HITs, more specifically EHRs, the implementation and adoption of them remained limited throughout the health care industry. 6 As Burke and Menachemi 9 argued health care facilities lagged behind about 10–15 years in IT spending, when compared to other industries. This gap is still valid as Haried et al. 10 argued that adoption of HITs in health care has traditionally slow and many facilities have failed to adopt these technologies. Similarly, Ljubici et al. 11 also posited that there is lack of studies for IT acceptance within health care organizations. Possible reasons of this outcome could be limited health care professionals and organizations have adopted HITs to affect the entire health care system, misplaced enthusiasm among health care professionals and lack of appropriate conditions to achieve highest possible potential of HITs. 6 Health care systems do not necessarily reward and even often penalized organizations making HIT investments. If a provider also knows less about a patient, it can charge more for clinical processes such as tests and other diagnoses that could be another lack of enthusiasm by health care providers to rapidly adopt those systems.
Little is known about adoption and use of HITs among health care professionals, 12 besides HITs are accepted as a key enabler for improving the healthcare quality. 13 Although related studies receiving increasing attention from scholars in the recent years, individual adoption research in health care settings especially in developing countries are still quite limited. 14 This study aims to fill this gap by investigating the individual adoption levels of physicians towards Electronic Health Records (EHR), which is a specific type of HIT. We develop and empirically test Individual ICT Adoption Model of Turkish Health care professionals with a data collected via survey instrument. The original research model based on a modified Technology Acceptance Model (m - TAM) which incorporates socio - psychological and cognitive factors from IS literature, predicting human intentions and actual behaviors to use particular information technology. The proposed model also incorporates social influence tactics of hospital administrators to promote EHRs to physicians. The current study only covers physicians of health care providing organizations. Our focus is mainly individual adoption of EHRs. Yet, future studies shall include nurses as well as hospital administrators in order to provide a more complete view of the phenomenon.
Health information technology systems in Turkey
New technologies in Turkey have been found to create significant benefits for health care providers as well as patients. As health care providing costs continuously raise and patients have become more aware of their rights and demand better services, health care has become the main political issues and seems to stay that way in the future, investment in HITs is expected to increase even in the case of economic slowdown.
However, since payments to physicians and health care facilities are rewarded volume rather than quality of the service provided and Turkish health care system is fragmented with number of players providing services, the investment rate to HIT remained relatively low throughout Turkish health system. In addition, high cost of acquiring the systems because of low value of Turkish currency and uncertain return on investments in HIT further hinders the successful adoption of Turkish physicians of HITs. Implementing HIT could require skills that are not part of the medical practice. Especially in Turkish hospitals, physicians have to treat about 60–100 patients daily in average in public hospitals and frequently complain that they cannot spend any time to learn how to use new HITs. Doctors see HIT as intrusion in patient physician relationship. Therefore, a new position called physician’s secretary has been formed to use information systems and notes diagnoses and treatments when physicians dealing with patients. Yet, Turkey has been going through extensive transformation process in Turkish health care and has carried out important reforms in health care services in recent years. 15 Turkey has united its health care system in October 2008 and initiated extensive information technology investments in its health care system. By united, it does not mean exactly a single system that all level of health care providers as well as public and private hospitals adopt their own HIT and EHR systems. Yet, all the data from these systems have been collected and accumulated within Turkish Health Care Ministry servers and all those adopted and preferred systems shall adhere some specific standards in terms of integration and connectivity. Turkish Health care transformation program as a general name of these initiatives aimed to provide better quality information to hospital managers and public officers that would help to make better and sound health care system policies and administrative decisions. 15
Health information technology implementation and adoption pose different challenges in Turkish setting that Turkish Doctors practice significant autonomy and perceive their services superior than other professional practices and they highly regard their status role and expertise. In addition, among Turkish patients to argue or even assess doctors’ diagnosis and treatment plans are very much taboo. Hence Turkish doctors benefit from quite high power distance. Similarly, as Ilie et al. 12 argued one of the major reasons for physicians to resists new HITs is the time it takes to feed the systems with data that is very prohibitive considering already busy schedules and work routines of doctors. Other reasons are inflexible and unfriendly systems interfaces, incompatibility of HIT to how health care personnel would want to practice.
This research’s focus is Turkish health care since, there is still limited number of studies published in widely circulated international journals about Turkish health care staff’s EHR adoption characteristics. Moreover, Turkish health care would be a good example of how a health care system could be transformed in merely 15 years and become quite a success story in developing country context.
Theoretical foundation
Studies investigating individuals’ reactions to computing technology have been an important topic in Management Information Systems research. 16 After 1980s, the ICT adoption research has focused on identifying determinants of users’ intentions to adopt new technologies. Number of theories have been developed or used to explain and predict users’ attitudes and behaviors towards new ICTs, including Innovation Diffusion Theory (IDT) by Rogers, 17 Theory of Reasoned Action (TRA) by Fishbein and Ajzen (1975), 18 Theory of Planned Behavior (TPB) by Ajzen, 19 and Technology Acceptance Model (TAM) by Davis 20 along with its vast variety of extensions. Although there are significant differences among these theories, the common underlying assumption of them is that the individual beliefs and perceptions about specific technologies could shape our behavior of adoption of specific ICTs. All the mentioned theories argue that individuals perceive new technologies from their internal cognitive process and form beliefs on adopting or not adopting those new ICTs. 21 In MIS literature, there is extensive research pointing out the importance of beliefs in technology adoption process in explaining system usage and usage intentions 21 Yet in general, Information Systems research has focused on centrality of beliefs in forming attitudes and usage behavior, less emphasis has been given on how such beliefs are formed. 3 Moreover, large body of Information Systems research has focused on user perceptions to form intentions to use a particular technology. However, the antecedents and consequences of perceptions remained largely unanswered in existing research. 22 This study aims to fill this gap by proposing a research model based on a modified TAM which incorporates socio psychological and cognitive factors to assess the HIT’s, more specifically EHR’s, adoption level of Turkish health care physicians. Although the underlying theory of our research model drives from TAM, we have integrated some major constructs from motivational theories from psychology literature. Years of technology adoption research relying on intention-based theories revealed that perceived usefulness, perceived ease and intentions are strong determinants of individual technology acceptance and adoption behavior. We also support our theory by incorporating motivational and individual commitment as well as resistance-based variables.
Research model
Motivation could play an important role that depends on whether system use is hedonic or utilitarian.
23
If system use is hedonic, intrinsic motivation could play more important role than the system usage is utilitarian. Only intrinsic motivation, where we want to do something rather than someone else wants us to do something (extrinsic motivation) could create positive sustainable motivation.
24
Hence managers at health care organization should first try to enhance intrinsic motivation of their health care personnel to increase better utilization chances of HITs. However, in this study, we did not differentiate these two major types of motivation since it is strongly argued that both extinct and instinct motivation will have positive and significant effects on our intentions to perform a particular behavior or use a particular IS (Figure 1).
23
Thus, it is proposed: H1: Physicians’ motivations will influence positively and significantly to their behavioral intention to use.
With the commitment to use HIS, health care personnel agree to use the system and internalizes this behavior and belief set and demonstrates extensive effort to use the system.
25
The individual presents persistency and consistency to use the system as well.
26
Thus, it is proposed: H2: Physicians’ commitments will influence positively and significantly to their behavioral intention to use.
Resistance is seen as a barrier that needs to be removed or sometimes it is perceived as a mean to communicate users’ discomfort with the system developers. Markus.
27
posits that if a new system changes the balance of power and causes one party to lose power, that party would resist the system. If health care personnel perceive new HITs as challenge to their power and authority, he or she will eventually refuse and even argue for not to perform that particular behavior.
25
Even though resistance is seen as a critical factor in the adoption of new technologies ,
28
resisting to HITs by heath personnel have not much studied in the literature.
29
The main reason may stem from the fact that the outright refusal of using the system is very rare in health care context. Yet, it is observed that putting off the system use and frequent criticisms of the system itself are more common.
29
Thus, it is proposed: H3: Physicians’ resistance will influence negatively and significantly to their behavioral intention to use.
In the literature the sound relationship between intention to use a system and actual use is clearly proposed by number of scholars.20,30,31 In IS adoption literature this relationship is frequently proposed and empirically assessed. We have adopted intentions to use and actual use scales from
20
and.
31
Since these constructs are well studies and self-expletory, we prefer not to go in details with them. Hence, it is proposed: H4: Physicians’ intentions to use will positively and significantly affect their actual system usage behaviors.
Research methods
Research setting and participants
This study is conducted among Turkish hospitals’ health care personnel in two different cities namely Tekirdağ and Kocaeli. All the health care organizations in these two cities regardless of their types were reached. Permissions from Institutional Review Board namely Turkish Ministry of Health were obtained. No financial support was received for this study.
Before conducting the survey, the entire instrument has been translated from English to Turkish and back translated into English by two independent bilingual individuals to ensure equivalency and some discrepancies has been resolved by the translators. An Expert of four physicians, who have also administrative duties checked instrument finally in terms of accuracy, consistency and appropriateness. All participants were physicians employed for three different titles such as head physician, assistant head physician, physician. Sampling method was nonrandom convenient sampling method. Total 212 responses were returned. To treat missing values, we used mean value replacement option.
Two different methods were used to collect data: face to face and online survey. The survey was administered at the first level health organizations in Tekirdağ (n=135) by the Tekirdağ Branch of Health Ministry. Some second and third level health organizations in Tekirdağ (n=39) were visited personally by the first author. Response rate was 100% since data collection was carried out by Ministry of Health with their special permission and rest face to face interaction. Totally 174 responses were obtained.
To increase the number of the participants, an online survey link was also sent to the physicians performing in second and third level health organizations in a neighboring city, Kocaeli. Prior to sending the link, head physicians of the hospitals were called and the details of the study explained. A special permission and support letter from Turkish Ministry of Health was also mentioned. Totally 50 survey links were sent and 38 responses were returned. Response rate was high since authors gave a brief information about their study and also made sure the head physicians received the support letter of the Ministry.
Measures
Our research model consists of three second order constructs namely motivation, commitment, and resistance. Each of them is formed by first order constructs with their relative indicators. Brief information for each first order constructs can be found in Appendix 1.
Results
Descriptive statistics
Descriptive statistics.
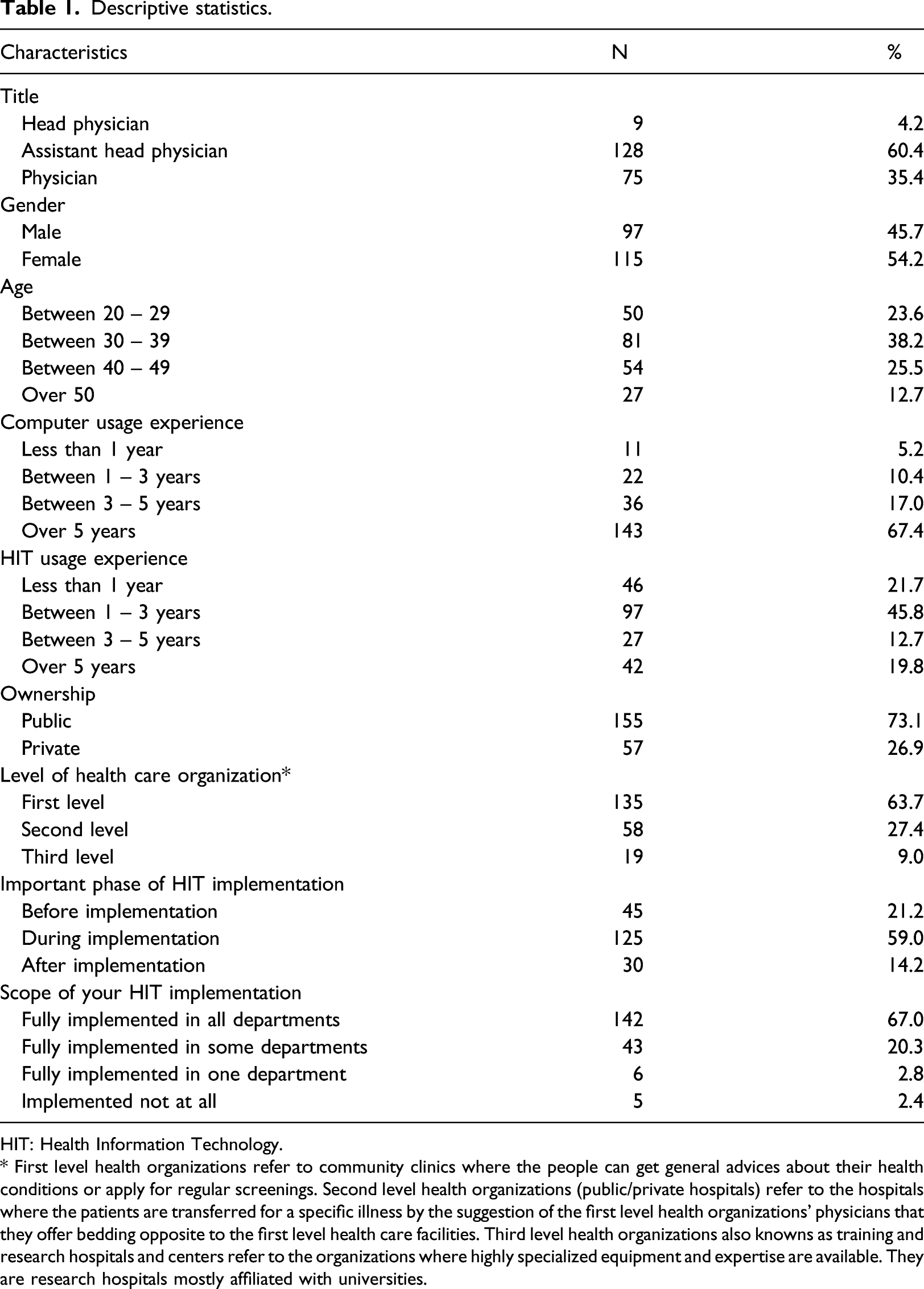
HIT: Health Information Technology.
* First level health organizations refer to community clinics where the people can get general advices about their health conditions or apply for regular screenings. Second level health organizations (public/private hospitals) refer to the hospitals where the patients are transferred for a specific illness by the suggestion of the first level health organizations’ physicians that they offer bedding opposite to the first level health care facilities. Third level health organizations also knowns as training and research hospitals and centers refer to the organizations where highly specialized equipment and expertise are available. They are research hospitals mostly affiliated with universities.
Most of the participants of our study is composed of assistant head physicians (60.4%) following physicians (35.4%). More than half of the participants are females (54.2%) in their middle ages between 30 and 50 years of age (63.7%). Overwhelmingly respondent has extended period of time computer usage experience (over 5 years–67.4%). Yet their experience with HIT is not so long mostly less than 3 years (67.5%). 59.0% of respondents expressed that the important phase of HIT implementation process is during the implementation. Around three quarter of all respondents (67.0%) indicated that in their health care organizations HITs are fully implemented in all departments already.
Analysis
Number of tests has been performed on the measurement model to assess its validity and reliability. Before performing Partial Least Squares Structural Equation Modeling (PLS-SEM), we conduct confirmatory factor analysis to assess the structural validity of our first-order constructs. The maximum likelihood approach was adopted for the CFA with the item covariance matrix as input data. The results are presented in Appendix 2.
Reliability and convergent validity measurements for reflective constructs.
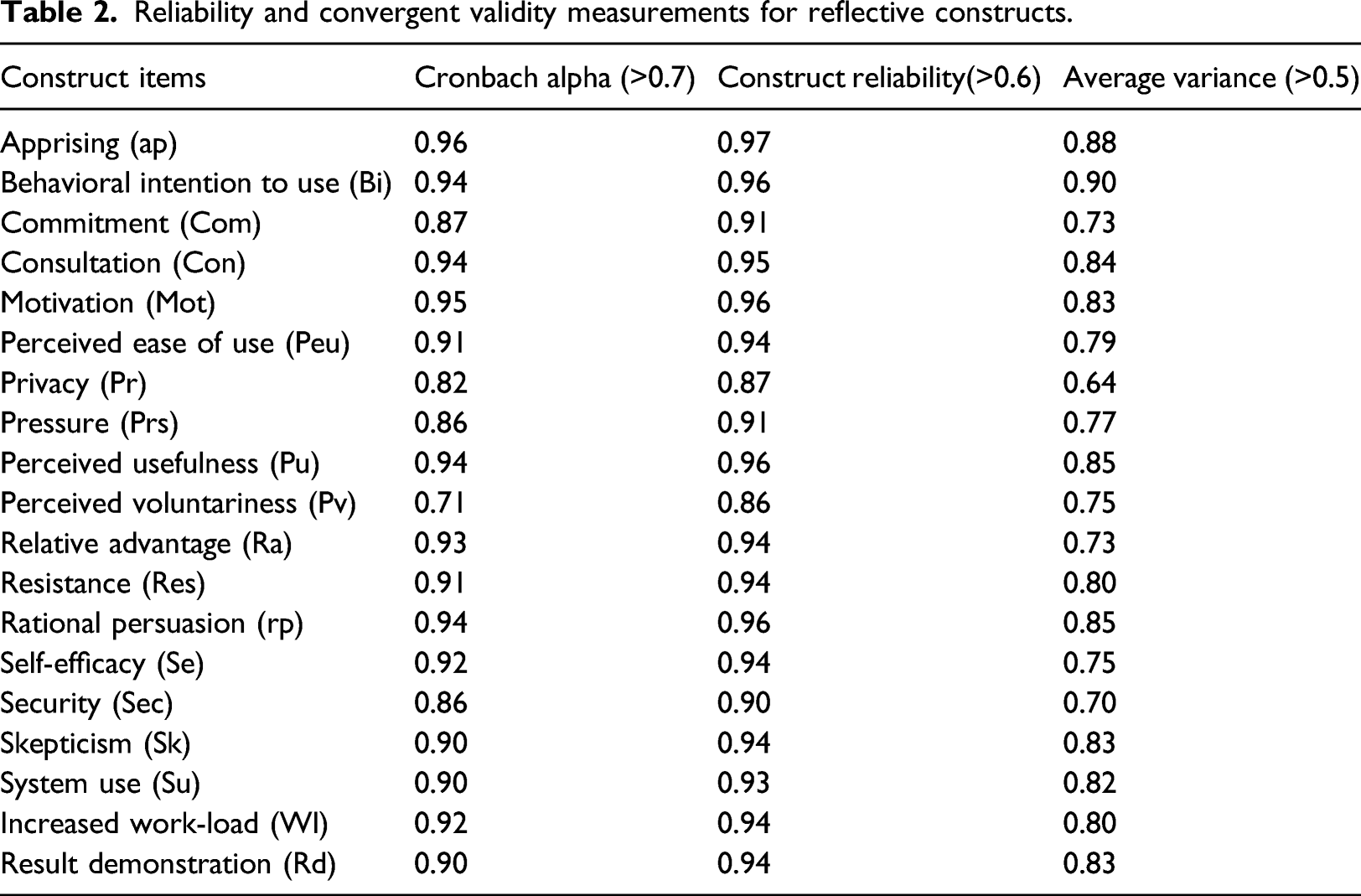
Based on the validity of reflective indicators, as Hair et al. 32 state that the outer loadings should be perfect if it is higher than 0.7, however outer loadings between 0.4 and 0.7 should be retained in the model if Cronbach Alpha and Average Variance (AVE) cannot change in case of deletion of the related item. Reflective items with lower than 0.4 outer loadings were eliminated from the model. Appendix 2 proves that most of the factor loadings of the items for each construct in the measurement model are over 0.70 as recommended. In addition to three items called Prs1, Pv3, and Rd4 which have been already excluded during CFA, Com5 was also deleted because of its low outer loadings.
The next step is evaluating the convergent validity which tests the correlation between related constructs via Average Variance (AVE) value. It should be noted there that, our model consists of three second order (Motivation, Commitment, and Resistance), and two first order (Behavioral Intention to Use and System Use) latent constructs with reflective indicators. To assess their convergent validity, AVE for each construct should be investigated separately. For a desirable measurement model, AVE values are expected to exceed 0.50 threshold 33 which is confirmed for our model.
Cronbach alpha and composite reliability (CR) is another important criterion for reflective constructs. According to 34 a Cronbach Alpha value with greater than 0.70 indicates a reliable measurement model. Similar to this, CR is expected to locate the threshold between 0.60 and 0.70. 35 In our measurement model, all CRs and Cronbach Alpha values well above recommended levels.
The last quality criteria for reflective items are discriminant validity which aims to detect the undesirable correlations between unrelated constructs. To do this, three different methods Fornell-Larcker Criterion , 33 HTMT approach, 36 and Cross Loading Criterion 37 can be used. Regardless of which technique is chosen, discriminant validity can be only used for first-order constructs. 38 We have used Fornell-Larcker Criterion 33 to establish discriminant validity, which admits that “the square root of the AVEs of each latent variable must be greater than its correlations with any other constructs.”. According to the results given in Appendix 4, all of our first-order constructs satisfied this criterion.
Structural model assessment
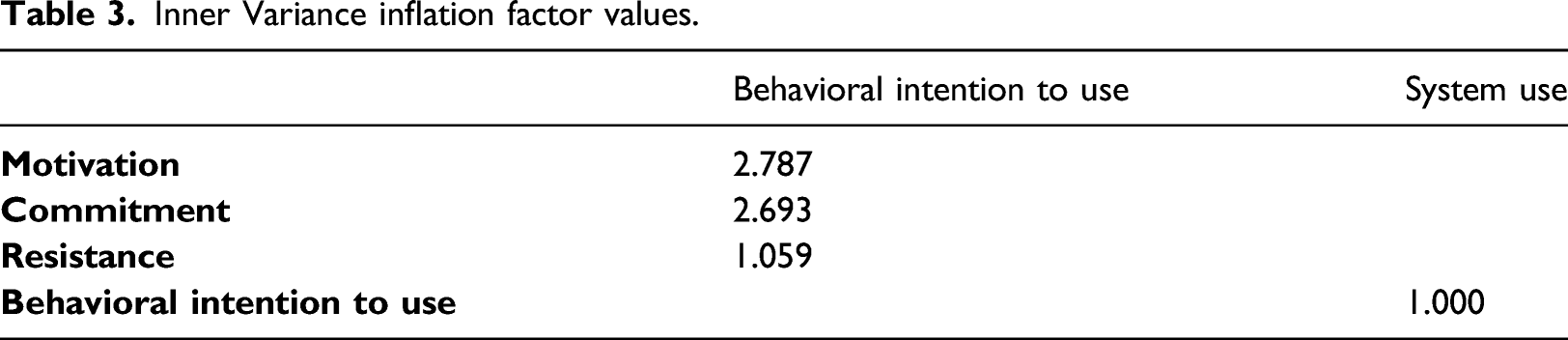
Inner Variance inflation factor values.
In addition, although PLS does not fully estimate goodness of fit due to its covariance matrix logic, SmartPLS offers some related indexes called SRMR, RMS_theta, NFI, d_ULS, d_G, and Chi2 to evaluate the model fit. Among them, standardized root mean square residual (SRMR) has the most common used
40
and should be less than 0.08. The SRMR for our final structural model was 0.053, which indicates sufficient model fit. The Research Model.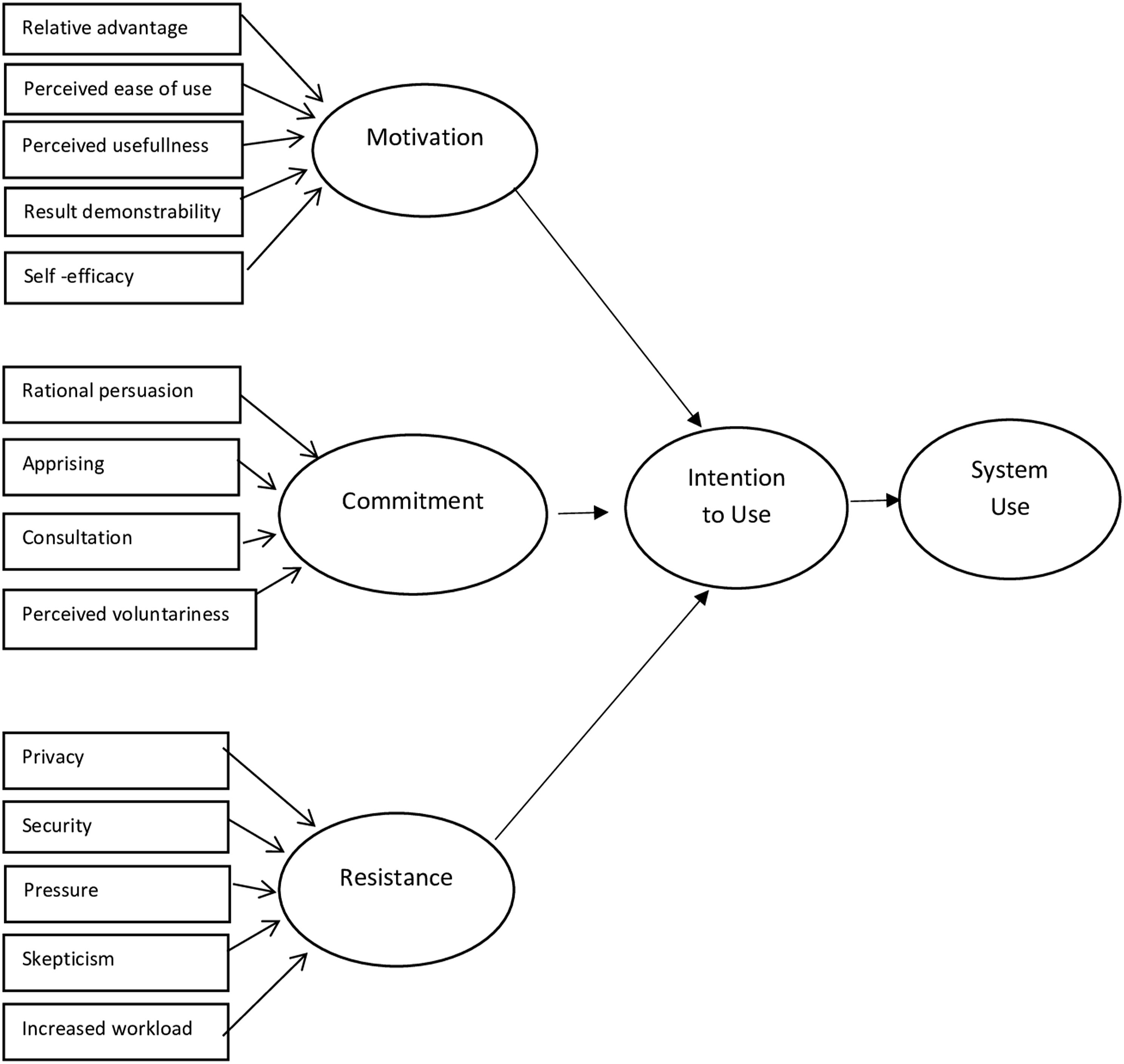
After initial checking was done, the next step is calculating the R2 which represents the explanatory power of the model explained by independent variables.
39
Power of the R2 depends on the context of the study. Therefore, different researchers propose different thresholds. Figure 2 shows the R2 values of two independent variables respectively as 0.313 and 0.032. This means that three latent variables (motivation, commitment, and resistance) together explain the 31.3% of the variance behavioral intention to use, whereas behavioral intention to use alone explains the 3.2% of the variance of system use. Structural Model Assessment.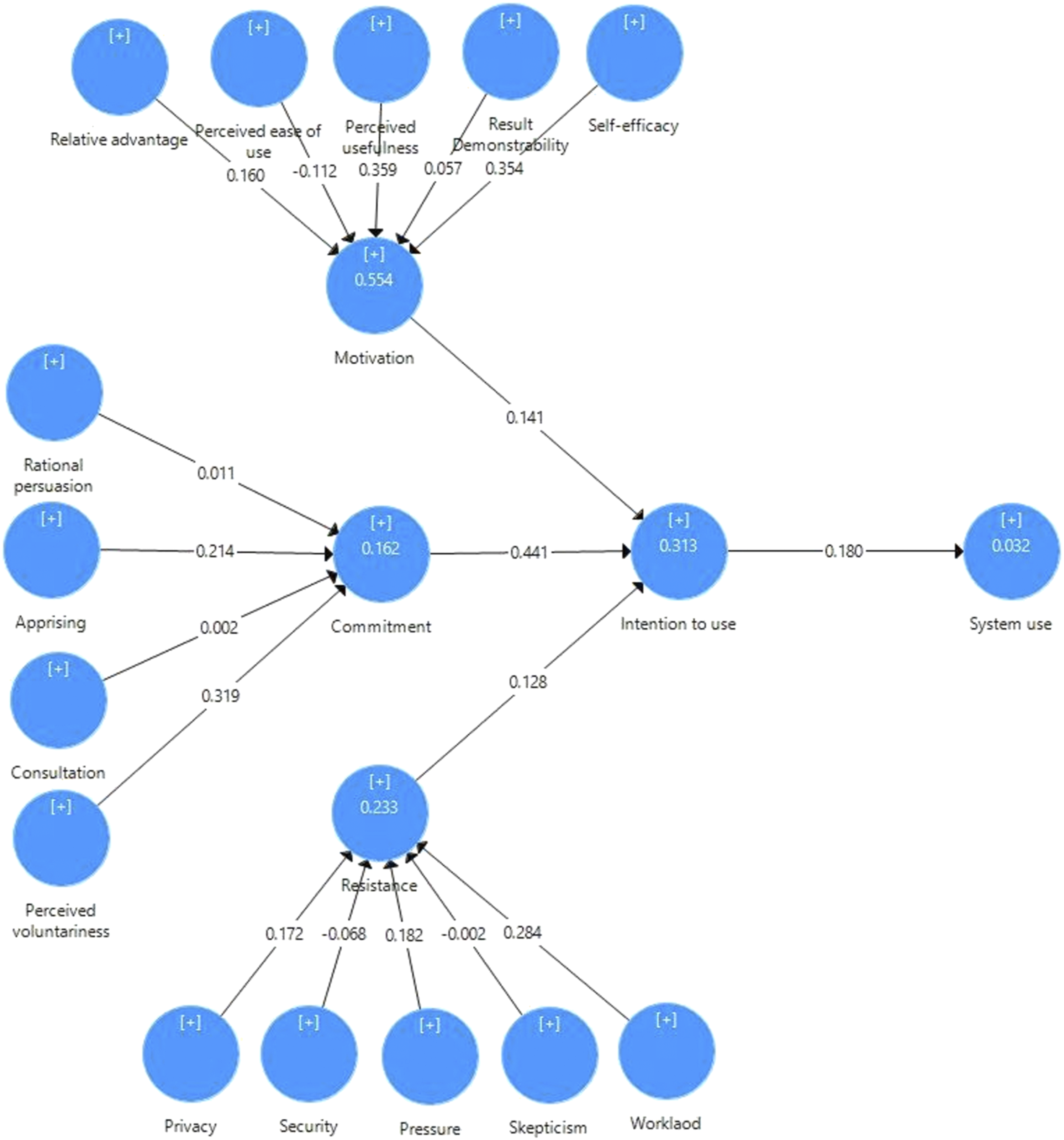
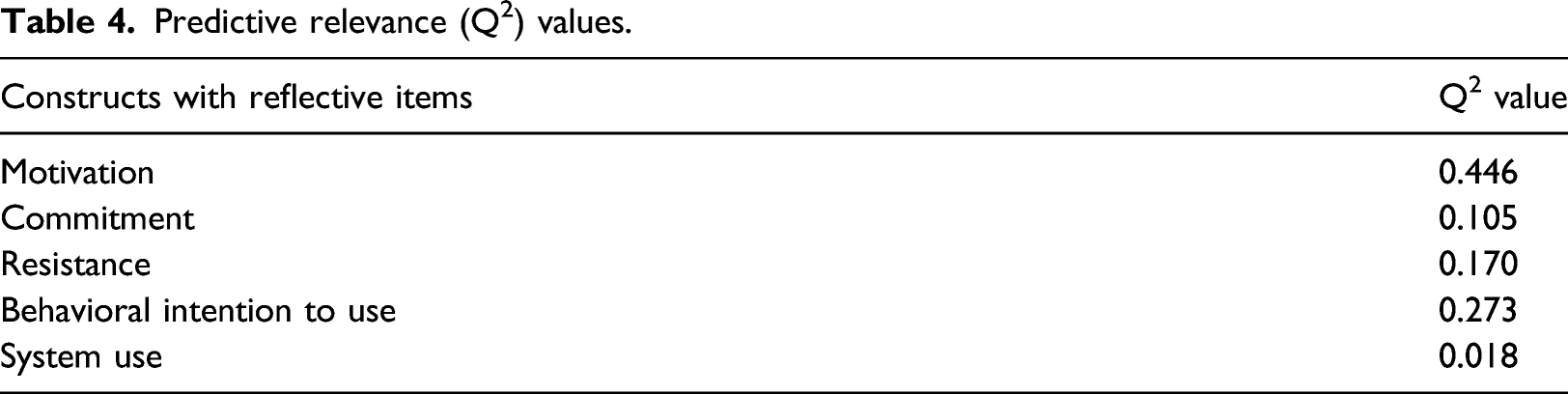
Predictive relevance (Q2) values.
Final causal model coefficients.
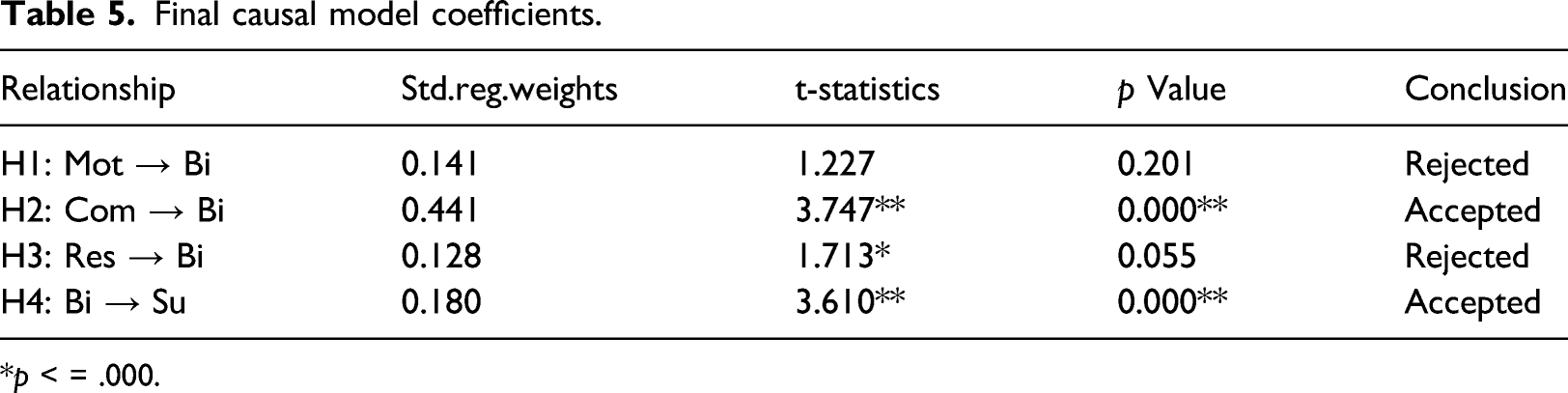
*p < = .000.
Conclusion
Investment in IT in health care requires more than successful installations of the systems. Successful HIT investments also require extensive training and cognitive and psychological support, commitment, motivation and readiness of the prospective users along with possible changes in work processes. Other than including subjective norm construct in studies, MIS research usually ignores the effects of social influence theories in technology adoption and in consequent usage behavior. Hence, this research contributes significantly in MIS research by including constructs from social influence theories such as relational persuasion, apprising, consultation and pressure. This research differs from traditional user acceptance research as well that our subjects i.e. physicians have largely previous knowledge and even experience with investigated using health care information systems. In addition, this research is an effort to respond the call made by Ketikidis et al., 44 where the authors noted that modified version of existing TAM models is needed to better understand the acceptance of HITs among the health care professionals.
Although after so many years of investing in ICTs in health care, expected results have not fully achieved yet. The potential benefits are widely accepted, all stakeholders in health care industry have continued to invest largely in ICTs. 6 We have empirically tested one of the most comprehensive research models that is rooted in intention-based theories and found partly empirical support to our hypothesis. Motivation and resistance have turned out to be not influential in Turkish doctors’ intentions to adopt HITs. Main reasons for this finding could be Turkish physicians high esteemed status quo and job security provided by government. Our data is collected mostly from public Turkish hospitals, where physicians are the king of the jungle with all job securities and professional privileges, in addition to respect provided them by just being a doctor.
On the other hand, commitment was found to be a significant predictor of behavioral intention, since still using EHRs are not compulsory largely for doctors and is not tied to their job performance and finally to their pay schedule, individual commitment and professional loyalty would seem to play mush role in adoption decisions and efficient use of HITs and EHRs by Turkish health professionals.
We have collected responses from all different types of Turkish Health care providing organizations that could enhance our generalizability to some extent. In addition, the core medical staff that are physicians were study subjects of this research. Other medical and administrative staff, who would have marginal effects on generalizability of our results were not included in the sample. Online survey further helped us to disseminate our questionnaire to a larger geographical area, which would also increase the generalizability of our results.
Limitations and recommendations
One of the major limitations of the study is that it does not consider some important constructs that would influence adoption process of IS, such as user participation and user involvement. 41 argued that user participation and involvement seem to have influence only for voluntary system use and system use is strongly influenced by intention to use the systems. Further studies might be useful to explore the effects of user participation and user involvement on the HIT adoption and use. Another limitation could be the data collected represent a snapshot of the ICTs adoption and usage phenomenon in organizations. Yet, a cross sectional study, in which adoption and usage could be measured with longitudinal data would provide more detailed information. Future studies could rely self-reported measures of ICT usage. Actual usage could have significantly weak linkages to self-reported usage; hence self-reported usage could not be an appropriate surrogate for actual usage all the time. 45
Future studies might be more interesting, if they include a comparison among different level of hospitals. As Shachak et al. 46 discussed HIT adoption models and theories have been mostly derived from TAM or UTAUT studies that have limited scope and perspective of HIT adoption in health care environments. In our paper, we adopted a large range of constructs originated from theories and models from sociology, psychology and MIS literature. Hence, we have tried to address existing complexity rising from health care context and human behavior as much as possible. We also have tried to address socio technical phenomenon of MIS nature in our research.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research model constructs.
Second-order constructs
First-order constructs’ characteristics
Name
Brief definition
Source
Example item
MOTIVATION(23) “the actual process of using Electronic Medical Record (EMR) is pleasant.”
Relative advantage
The extent a person perceives an innovation as an advantage over previous ways of doing the same task.
(47)
“Using EMR system at our hospital improves my productivity.”
Perceived ease of use
Users’ perceptions of the degree that the systems usage would be free of effort.
(20)
“I find our hospital’s EMR system easy to use.”
Perceived usefulness
Individuals’ expectation that using computers would results in improved job performance.
(20)
“I find EMR system useful in doing my hospital duties.”
Result demonstrability
The degree of a person can observe results of adopting or not adopting a particular technology.
(47)
“The results of using the EMR system at our hospital are apparent to me.”
Self-efficacy
Individual’s self-confidence on his or her ability to perform a particular behavior.
(16)
“I could learn the process of using computer and internet systems.”
COMMITMENT(55)
“I feel sense of ownership for the use of the EMR.”Relational persuasion
Something is trying to persuade users by using logical arguments and factual evidence to perform a particular behavior.
(48)
Our hospital management explains why adopting/using the EMR system would be practical and cost effective.
Apprising
The agent explains how carrying out a request or supporting a proposal will benefit the target personally or help to advance the target’s career.
(48)
“Our hospital management explains how adopting/using the EMR could help my career.”
Consultation
The agent asks the target person to suggest improvements or help plan a proposed activity or change for which the target person’s support is desired.
(48)
“Our hospital management consults with me to get my ideas about adoption/usage of the EMR system.”
Perceived voluntariness
The extent to which potential adopters perceive the adoption decision to be nonmandated.
(49)
“Our hospital administration is requiring me to adopt EMR system at this point.”
RESISTANCE (56)
“I oppose the change to the new way of working with EMR.”Privacy
Concerns include organization of complex information in standard database format, rapidly accessible key fields such as diagnoses, medications and diagnostics in legible for- mat and compact storage of multiple patient’s data.
(50)
“My patients’ health information should only be known to the patient and me.”
Security
Threats causes from interruption, interception, modification, and/or fabrication of the network infrastructure.
(8)
“I think EMR system in our hospital dependable/reliable.”
Pressure
The agent uses demands, threats, frequent checking, or persistent reminders to influence the target to do something.
(48)
“Our hospital management demands that I adopt/use the EMR system.”
Skepticism
The resistance towards new ICTs that would change work setting and professional relationships.
(51)
“I do not want EMR to change the way I practice my profession.”
Increased workload
Too much work and too little time has become a common complaint among employees.
(52)
“Right after we have adopted/used the EMR system, I seem to have too many things to do.”
Behavioral intention to use
The degree to which a person has formulated conscious plans to perform or not to perform some specified future behavior
(53)
“I plan to use the EMR system at our hospital in the future.”
System usage
The endpoint where people use the technology.
(54)
“Are you intensive user of the EMR system at your hospital?”
Results of the Confirmatory Factor Analysis for the first-order constructs (Prs1,Pv3,and Rd4 dropped).
Second order constructs
First order constructs
First order constructs’ items
Varimax-rotated loadings factor
1
2
3
4
5
Relative advantage
Ra1
0.813
Ra2
0.825
Ra3
0.761
Ra4
0.700
Ra5
0.467
Ra6
0.531
Perceived ease of use
Peu1
0.772
Peu2
0.820
Peu3
0.754
Peu4
0.605
Perceived usefulness
Pu1
0.590
Pu2
0.728
Pu3
0.713
Pu4
0.645
Result demonstrability
Rd1
0.695
Rd2
0.674
Rd3
0.765
Self-efficacy
Se1
0.503
Se2
0.548
Se3
0.553
Se4
0.819
Se5
0.670
Rational persuasion
Rp1
0.830
Rp2
0.870
Rp3
0.844
Rp4
0.814
Apprising
Ap1
0.771
Ap2
0.756
Ap3
0.698
Ap4
0.694
Consultation
Con1
0.713
Con2
0.828
Con3
0.841
Con4
0.853
Perceived voluntariness
Pv1
0.861
Pv2
0.850
RESISTANCE (p = .00; KMO = 0.781; 77.052% total variance explained)
Privacy
Pr1
0.558
Pr2
0.846
Pr3
0.821
Pr4
0.792
Security
Sec1
0.789
Sec2
0.882
Sec3
0.869
Sec4
0.810
Pressure
Prs2
0.887
Prs3
0.817
Prs4
0.905
Skepticism
Sk1
0.887
Sk2
0.929
Sk3
0.915
Increased work load
WI1
0.849
WI2
0.837
WI3
0.895
WI4
0.817
Descriptive statistics of each construct
Construct items
Mean
Standard deviation
Factor loadings (>0.7)
Apprising
3.00
1.19
Ap1
0.95
Ap2
0.95
Ap3
0.94
Ap4
0.92
Behavioral int.
3.44
1.00
Bi1
0.91
Bi2
0.97
Bi3
0.96
Commitment
3.26
0.71
Com1
0.86
Com2
0.87
Com3
0.81
Com4
0.86
Com5*
0.060
Consultation
2.96
1.17
Con1
0.89
Con2
0.90
Con3
0.93
Con4
0.94
Motivation
3.37
0.92
Mot1
0.86
Mot2
0.91
Mot3
0.93
Mot4
0.94
Mot5
0.91
Per. Ease of use
3.70
0.82
Peu1
0.88
Peu2
0.86
Peu3
0.94
Peu4
0.87
Privacy
3.37
0.88
Pr1
0.70
Pr2
0.81
Pr3
0.87
Pr4
0.82
Pressure
2.96
1.08
Prs2
0.90
Prs3
0.73
Prs4
0.94
Per. Usefulness
3.69
0.92
Pu1
0.93
Pu2
0.91
Pu3
0.92
Pu4
0.92
Per. Voluntariness
3.82
0.92
Pv1
0.77
Pv2
0.95
Rel. Advantage
3.82
0.87
Ra1
0.81
Ra2
0.86
Ra3
0.88
Ra4
0.83
Ra5
0.89
Ra6
0.89
Resistance
2.53
0.96
Res1
0.91
Res2
0.94
Res3
0.86
Res4
0.85
Rational persuasion
3.12
1.18
Rp1
0.90
Rp2
0.91
Rp3
0.94
Rp4
0.94
Self-efficacy
3.71
0.81
Se1
0.90
Se2
0.93
Se3
0.90
Se4
0.78
Se5
0.82
Security
3.52
0.78
Sec1
0.82
Sec2
0.87
Sec3
0.83
Sec4
0.82
Skepticism
3.63
1.02
Sk1
0.93
Sk2
0.89
Sk3
0.90
System use
8.08
2.48
Su1
0.97
Su2
0.97
Su3
0.76
Work-load
3.19
1.06
Wl1
0.88
Wl2
0.89
Wl3
0.93
Wl4
0.88
Result demons.
3.67
0.93
Rd1
0.95
Rd2
0.94
Rd3
0.83
Discriminant validity.
Ap
Bi
Com
Con
Wl
Mot
Peu
Pu
Pv
Prs
Pr
Rp
Ra
Res
Rd
Se
Se
Sk
Su
Ap
Bi
0.04
Com
0.23
0.53
Con
0.79
0.15
0.19
Wl
0.01
−0.19
−0.25
0.02
Mot
0.28
0.45
0.79
0.19
−0.30
Peu
0.20
0.39
0.58
0.19
−0.25
0.58
Pu
0.19
0.45
0.68
0.14
−0.25
0.70
0.71
Pv
0.09
0.21
0.33
0.04
−0.14
0.37
0.45
0.40
Prs
0.38
0.01
0.08
0.27
0.22
0.00
0.02
0.00
−0.05
Pr
0.02
0.02
−0.19
−0.01
0.48
−0.25
−0.13
−0.23
−0.04
0.19
Rp
0.68
0.06
0.19
0.62
−0.03
0.28
0.25
0.16
0.12
0.20
−0.08
Ra
0.16
0.36
0.62
0.10
−0.31
0.65
0.65
0.86
0.37
0.04
−0.25
0.17
Res
0.08
0.06
−0.07
0.10
0.41
−0.19
−0.15
−0.11
−0.26
0.26
0.36
−0.13
−0.18
Rd
0.19
0.32
0.59
0.11
−0.18
0.63
0.67
0.76
0.41
−0.02
−0.27
0.20
0.70
−0.19
Sec
0.30
0.13
0.52
0.22
−0.02
0.49
0.46
0.43
0.26
0.08
−0.22
0.36
0.39
−0.09
0.46
Se
0.23
0.38
0.60
0.20
−0.25
0.64
0.83
0.66
0.52
−0.01
−0.15
0.28
0.59
−0.22
0.71
0.45
Sk
0.08
0.07
0.03
0.09
0.16
0.05
0.16
0.10
0.21
−0.01
0.19
0.08
0.01
0.07
0.15
0.10
0.19
Su
0.02
0.19
0.18
0.01
0.06
0.18
0.28
0.16
0.35
0.01
0.10
0.05
0.15
−0.19
0.15
0.17
0.31
0.13