
Abstract
The adoption of e-healthcare services is critical for improving healthcare accessibility and efficiency, particularly in regions with diverse populations, such as Malaysia. Although e-healthcare services offer numerous advantages, their adoption is considerably low and requires a thorough understanding of the key factors that influence their use. This study investigated the determinants and dynamics of e-healthcare adoption among adults over 40 years by extending the unified theory of acceptance and use of technology. We employed a quantitative research approach, specifically a cross-sectional design. Data were collected from 393 Malaysian respondents through a structured survey questionnaire, using convenience sampling. They were analyzed using partial least-squares-structural equation modeling. The findings revealed that performance expectancy, effort expectancy, social influence, and perceived product value significantly influenced individuals’ intentions to use e-healthcare services. Meanwhile, perceived risk had an insignificant negative effect. Facilitating conditions significantly influenced individuals’ intentions and actual usage of e-healthcare services. Furthermore, individuals’ intentions to use e-healthcare services significantly affected their actual use of these services. Additionally, the intention to use e-healthcare services mediated the relationship between the factors and usage of e-healthcare services, except for perceived risk. Surprisingly, perceived service accuracy had no significant moderating effect on the relationship between individuals’ intention to use and their actual use of e-healthcare services. This study offers valuable insights for educators, practitioners, and policymakers, enriching the scholarly discourse in this field. For education, integrating e-healthcare topics into curricula can enhance digital health literacy. In practice, healthcare providers should focus on improving user experience and addressing barriers to technology adoption. For policy making, developing supportive policies, and infrastructure to facilitate e-healthcare adoption is crucial to enhancing public health outcomes.
Keywords
Introduction
The fusion of technological advancements and healthcare has ushered in a transformative era in healthcare worldwide. 1 One of the most striking developments is the emergence of e-healthcare, a multifaceted approach that utilizes digital technologies to enhance accessibility, efficiency, and overall patient outcomes in healthcare. 2 The benefits of e-healthcare services are extensive, encompassing the entire spectrum of healthcare delivery. E-health, which includes digital support and health informatics, has emerged as another important advancement. 2 The scope of e-health primarily includes telemedicine consultation, remote patient monitoring, digital health and medical histories, medical and chronic illness supervision applications, clinical decision-support systems, and e-prescription software. Meanwhile, e-healthcare services include the remote provision of physician consultation, surveillance, health screening, and other healthcare services. 3 E-health is currently viewed as a creative, dependable, and effective method of delivering healthcare because of its extensive range of services and solutions. The global e-health market is projected to exceed USD 206 billion by 2022. 4 However, e-Health market growth may be influenced by various drivers and challenges in government support and regulations, culture, economics, and technology.
The adoption of e-healthcare services is a multifaceted issue, influenced by various factors that determine its success and widespread utilization. While e-healthcare services offer convenience and accessibility, leading to increased popularity among consumers, 2 their adoption is not uniform across demographics and regions. For instance, despite the potential of mobile technologies to enhance healthcare delivery in low-income countries, user acceptance remains a critical challenge. 5 Moreover, healthcare digitization introduces significant security concerns that must be addressed to protect sensitive health data. 6 Additionally, specific demographic groups, such as senior citizens in Malaysia, show relatively low adoption rates, which may be influenced by factors such as information quality, privacy, security, trust, and health literacy.7,8 Furthermore, the IT revolution has transformed consumer behavior in healthcare, necessitating an understanding of the factors that drive behavioral intention to use and actual usage of e-healthcare services. 9
Malaysia is renowned for its technological advancements and dedication to healthcare improvements. Thus, the integration of e-healthcare services presents a promising opportunity to usher in a new era of excellence in healthcare. 10 Despite the benefits of e-healthcare services, an ongoing challenge is understanding which factors influence Malaysian adults’ intention and utilization of these services. For instance, Hayat et al. 8 highlighted that the actual adoption of e-health applications is not directly influenced by the intention to use them. This suggests a disconnect between positive attitudes toward eHealth and real-world application. Luai et al. 11 provide insights into the barriers specific to digitalizing oral health promotion, including the lack of supportive infrastructure, facilities, resources, and stable internet connections. Omar et al. 7 identified challenges such as information quality, privacy and security, trust, and health literacy as barriers to the adoption of digital healthcare services among senior citizens in Malaysia. While research explores the general acceptance of e-healthcare services, a comprehensive examination of the key factors, particularly within the cultural and societal context of Malaysia, is still lacking. 12 Furthermore, research has primarily focused on the design and implementation of these services from the service provider's perspective, with a limited understanding of how patients perceive technology usage and how it relates to behavioral aspects. The intersection of technology and healthcare introduces a complex interplay of factors spanning the technological, social, and individual dimensions, including concerns about privacy and potential consequences of the misuse of health-related information. 13 Gu et al. 14 claimed that few studies have expanded the original unified theory of acceptance and use of technology (UTAUT) model to include behavioral constructs in the context of healthcare delivery. Dhagarra et al. 13 found that most e-healthcare studies have explored the barriers and obstacles to technology adoption from a qualitative standpoint.
Healthcare technology adoption studies have employed various theories to comprehensively understand this phenomenon. For instance, Lu 15 studied online health community adoption using social exchange theory; Papa et al. 16 examined smart healthcare device adoption using the technology acceptance model (TAM); Ye et al. 17 explored mobile healthcare technology adoption by integrating stimulus-organism-response (SOR); and Arkorful et al. 18 researched mobile health technology adoption incorporating the theory of planned behavior and IoT adoption in e-healthcare. 19 Although behavioral intention, or intention to use, is a crucial element in technology adoption models that explain decision-making processes and precedes actual adoption, researchers are consistently discovering new perspectives on technology adoption. Wilson et al. 20 examined the enablers of and barriers to using e-healthcare among older adults. The authors concluded that scholars have not sufficiently emphasized factors influencing older adults’ decisions to use technology to access healthcare. Ross et al. 21 studied various factors related to organizational context, technology, and user acceptance, and recommended further exploring factors affecting successful e-health implementation. Endeshaw 9 recommended further in-depth investigation of factors which affect e-healthcare service quality. To address these research gaps, we aim to explore the behavioral and contextual factors in the context of e-healthcare usage among Malaysian adults, focusing on the UTAUT model. To enhance our understanding of the complex relationships within this framework, we introduced a critical moderating factor: perceived service accuracy.
We sought to address the following research questions (RQs):
To answer the abovementioned RQs, we developed a framework extending the UTAUT model to examine the factors influencing e-healthcare services adoption among Malaysian adults. The proposed model's applicability was empirically tested using data collected from 393 samples. The significance of this endeavor lies not only in advancing academic knowledge, but also in providing practical implications for healthcare stakeholders. The actionable insights for policymakers, healthcare providers, and technology developers can facilitate the development of targeted strategies that resonate with Malaysia's cultural and societal nuances.
Theoretical background and hypotheses development
The UTAUT model, developed by Venkatesh et al., 22 forms the theoretical foundation of this study. This model serves as a framework for understanding individuals’ behavioral intentions in technology adoption scenarios. In the e-healthcare literature, UTAUT has been utilized to grasp individuals’ intentions to adopt technology. Wang et al. 23 examined consumer willingness to use healthcare devices by considering performance expectations, ease of use, supportive conditions, social influence, and task-technology alignment. Arfi et al. 19 explored patient readiness to embrace IoT in e-health considering performance expectations, ease of use, social influence, supportive conditions, and credibility. Gu et al. 14 investigated patient intentions to adopt e-health technology by examining aspects such as performance expectations, ease of use, social influence, task technology fit, privacy, collision risk, and personal innovation in trustworthiness of information technology. Yang et al. 24 investigated consumer acceptance of m-health by analyzing health awareness, motivation, technological accuracy, critical mass, privacy protection, user-friendliness, and convenience as driving factors.
Next, in the context of e-healthcare services, users are always concerned about concealing information. Thus, understanding how perceived risk affects individuals’ intention to use and actual use of e-healthcare services is important. Sahoo et al. 25 examined the effect of perceived risk on performance expectancy and effort expectancy in the context of using an e-health consultation using the stimuli–organism–behavior–consequence model; however, the authors did not test the direct effect of perceived risk on intention. Zhang et al. 26 studied the effect of price value, as well as other factors, on patients’ intention to use online health communities. However, the authors did not assess product value. Interestingly, while perceived risk is acknowledged as a significant factor in technology adoption, its impact can vary. For instance, Yin et al. 27 indicated that perceived risk does not significantly influence behavioral intention in the context of wearable intelligent medical devices. This suggests that the integration of perceived risk into the UTAUT model may yield different implications, depending on the technology and context being studied.
Nonetheless, in the context of technology acceptance models, product and price values are distinct concepts. Product value generally refers to the perceived benefits or utility a user gains from using a technology, which can include aspects such as performance, efficiency, and effectiveness. Price value, on the other hand, is a construct specific to UTAUT2 that assesses the user's cognitive trade-off between the perceived benefits of the technology and the monetary cost of using it. 28 Interestingly, although price value is a key construct in UTAUT2, it has been adapted or replaced in some studies to better fit the context. For instance, in the study of e-government services, the price value was substituted with public value, reflecting the non-commercial nature of public services. 29 This indicates that, while price value is important in consumer contexts, its relevance may vary in different settings.
Thus, we integrate perceived risk and product value into the model and investigate their effects on e-healthcare services adoption intention. Incorporating the construct of perceived risk into the model aims to address issues related to e-healthcare services, including confidentiality, data security, and dependability of the system. Furthermore, we include perceived service accuracy as a moderator in the relationship between individuals’ intention to use e-healthcare services and their actual usage to gain a comprehensive understanding of the phenomenon. Introducing perceived service accuracy as a moderating construct in the context of e-healthcare services could be theoretically justified by the nature of these services. The importance of accuracy is implicit in healthcare contexts where the consequences of inaccurate information can be severe. 23 These services must provide accurate data that can be useful and trusted by the users. The perceived accuracy of the service provided could influence the relationship between core UTAUT constructs and user behavior. If users perceive the data provided by the services as accurate, they may be more likely to find the service useful (performance expectancy) and easier to use (effort expectancy), which could in turn increase their behavioral intention to use the device and their actual usage behavior. 27 Grounded in the theoretical frameworks of technology acceptance and trust, we posit that users’ confidence in the accuracy and reliability of e-healthcare services significantly influences their likelihood to act on their intention, particularly in the context of e-healthcare, where the accuracy of medical and health-related information is crucial.
Performance expectancy and intention to use e-healthcare services
Performance expectancy refers to a user's perception of the technology's effectiveness in enhancing performance.
22
Performance expectancy is the combination of two important dimensions, perceived usefulness and ease of use, which originate from the constructs of TAM.
25
Individuals who perceive e-healthcare services as useful (e.g., improving health outcomes and providing timely information) are more likely to have the intention to use them. Moreover, if individuals find e-healthcare services to be user friendly, they are more likely to adopt them. Studies show that using innovative technologies substantially impacts individuals’ intentions to use these technologies.
30
Zhang et al.
26
found a significant positive relationship between patients’ acceptance of online health communities in China and their behavioral intention to use these communities. Sahoo et al.
25
found a significantly positive impact of performance expectancy on adopting e-health consultation services. Thus, we propose the following hypothesis:
Effort expectancy and intention to use e-healthcare services
Effort expectancy centers on the perceived ease of use of technology.
22
The concept of ease of use is derived from both the DOI and TAM theories.
25
Studies show that effort expectancy significantly influences individuals’ intentions to adopt new technologies, even in the healthcare sector. Hossain et al.
30
studied the electronic health records in healthcare systems among Bangladeshi physicians and found that effort expectancy substantially influenced physicians’ decision-making in the adoption process. Gu et al. (2021) revealed that effort expectancy significantly influenced the intention to adopt e-health technology of patients in hospitals. Srivastava and Raina
31
explored e-pharmacy adoption in India and found a positive and significant correlation between effort expectancy and consumer adoption intention. Thus, we propose the following hypothesis:
Social influence and intention to use e-healthcare services
Social influence plays a pivotal role in technological acceptance.
22
This construct captures the impact of social interactions, norms, and influences on an individual's decision to adopt e-healthcare services. This encompasses the influences of family, peers, and healthcare professionals on the adoption process. Individuals who observe their family and friends using e-healthcare services for health-related activities and believe that they endorse the use of these services are expected to express positive intentions to use them.
32
Moreover, the inclination to use e-healthcare services because family and friends also engage in such activities results in an overall positive relationship, highlighting the impact of familial and peer behaviors on individual intentions.
33
The influence of significant others who hold sway over one's behavior and those who generally influence behavior further strengthens the positive relationship. Thus, individuals who perceive the endorsement and encouragement of significant others are more likely to express a positive intention to use e-healthcare services.
30
Gu et al.
14
and Arfi et al.
19
found a positive impact of social influence on the intention to use e-healthcare services. Thus, we propose the following hypothesis:
Perceived risk and intention to use e-healthcare services
Perceived risk refers to an individual's subjective evaluation and assessment of potential uncertainties, hazards, or negative consequences associated with a particular action, decision, or choice.
34
In the context of e-healthcare service adoption, perceived risk encompasses the concerns and uncertainties users may associate with using digital healthcare platforms. Individuals who express concerns, such as sharing their personal information without consent and perceptions of financial risks, are expected to have a negative intention to use these services.
35
Additionally, concerns about financial or payment fraud, uncertainty due to regulatory complexities, and an increased likelihood of receiving spam or spam SMS services after subscribing to e-healthcare services contribute to an overall negative relationship.
36
This underscores the impact of perceived risks, including privacy, financial security, regulatory uncertainties, and potential inconveniences such as spam, as barriers to the adoption of e-healthcare services within the Malaysian context. Lu et al.
37
and Upadhyay et al.
3
empirically demonstrated the negative impact of perceived risk on the behavioral intention to use smart healthcare services. Thus, we propose the following hypothesis:
Perceived product value and intention to use e-healthcare services
Perceived product value refers to an individual's subjective assessment of product quality and satisfaction derived from using a particular product or service compared to the perceived costs or efforts associated with its use.
17
According to Zhang et al.
26
perceived product value is a multidimensional concept that requires individual assessment of relevant determinants, including functional, symbolic, and experiential characteristics. However, few e-healthcare studies investigate the role of perceived product value in influencing users’ intention to adopt e-healthcare services. Immonen and Koivuniemi
38
studied the determinants of self-service technologies in the healthcare sector and the effect of perceived product value as a dimension of perceived benefits, finding a significant relationship between the two constructs. Researchers have revealed a substantial relationship between perceived product value and positive intention to adopt innovative technologies, particularly in the healthcare sector. When users have a positive perception of the value of e-healthcare services, they tend to adopt them very quickly.
39
Thus, we propose the following hypothesis:
Facilitating conditions, intention to use, and actual usage of e-healthcare services
Facilitating conditions are external factors that facilitate or hinder technology use.
22
Facilitating conditions include the adequacy of infrastructure, technical, and organizational capabilities while using any application or technology. Studies have shown that facilitating conditions significantly influence individuals’ intention to use innovative technologies in healthcare services. Gu et al.
14
found that favorable conditions for the e-health technology positively affected hospitalized patients’ willingness to adopt it. Sahoo et al.
25
discovered that the presence of adequate technological infrastructure played a crucial role in shaping users’ intentions to adopt e-health consultations. These supportive conditions encompass resource accessibility, technical assistance, and training opportunities, which not only shape users’ intentions, but also facilitate the effective utilization of e-healthcare services.
14
Thus, evaluating the impact of facilitating conditions on individuals’ intentions to utilize e-healthcare services and their subsequent actual usage are important. Accordingly, we hypothesized the following:
Intention to use and actual usage of e-healthcare services
Individuals expressing their intent to use e-healthcare services for health management, planning frequent usage, and predicting future usage may exhibit a positive correlation with the actual usage of e-healthcare services. This highlights the motivational aspect of intention in driving individuals’ active consideration and planning for the adoption of e-healthcare services.
40
Continued time investment, a desire for future health safety, plans for regular usage, and intention to continue using e-healthcare services contribute to the overall positive relationship.
41
Users who actively and consistently translate their intentions into tangible actions by using these services are more likely to engage with and adopt digital healthcare platforms. Yang et al.
24
also found a strong relationship between intention to use and actual adoption of new healthcare applications. Thus, we hypothesized the following:
Moderating role of perceived service accuracy
Here, we consider the concept of perceived service accuracy as an individual's belief that the e-healthcare services will function without any errors or issues. A product with higher perceived service accuracy should increase customer satisfaction and reliability, ultimately creating a competitive advantage for that product.
42
Most studies investigate perceived service accuracy as an independent variable and measure how it influences the adoption intention of a particular technology or service. Johnson and Woolridge
43
found that service accuracy substantially influences the adoption of mobile self-checkout systems. Singh et al.
44
investigated the determinants that influence the adoption of wearable healthcare technologies and found a significant association between service accuracy and adoption decisions. However, very few studies tested perceived service accuracy as a moderator, particularly in the field of e-healthcare services, which we consider here. Accordingly, we hypothesized the following:
Mediating role of intention to use e-healthcare services
We argue that the intention to use e-healthcare services significantly mediates the relationships between various determinants, including performance expectancy, effort expectancy, social influence, perceived risk, perceived product value, and facilitating conditions, and the actual usage of e-healthcare services among Malaysian adults. Individuals with higher performance expectations are more likely to engage in actual usage with positive intentions. Arfi et al.
19
found that belief in the benefits of using healthcare technology played a significant role in influencing individuals’ actions. Moreover, those who find e-healthcare services easy to use are more inclined to use them based on their positive intentions, as highlighted by Wang et al.
23
Additionally, individuals influenced by friends and family are more likely to use these services because of their intentions, as emphasized by Gu et al.
14
and Arfi et al.
19
Conversely, those who perceived risk are less likely to use these services.3,37 Meanwhile, individuals who perceive value in a product are more inclined to use it based on their positive intentions, as noted by Lee and Lee
45
and Yang et al.
46
Furthermore, people with access to resources and supportive environments are more likely to engage with these services due to their intentions, as demonstrated by Gu et al.
14
Therefore, we argue that users’ intentions serve as a bridge, translating the influence of these determinants into tangible actions and ultimately influencing their actual engagement with e-healthcare services. Accordingly, we propose the following hypotheses:
Accordingly, we propose the following research framework (Figure 1).
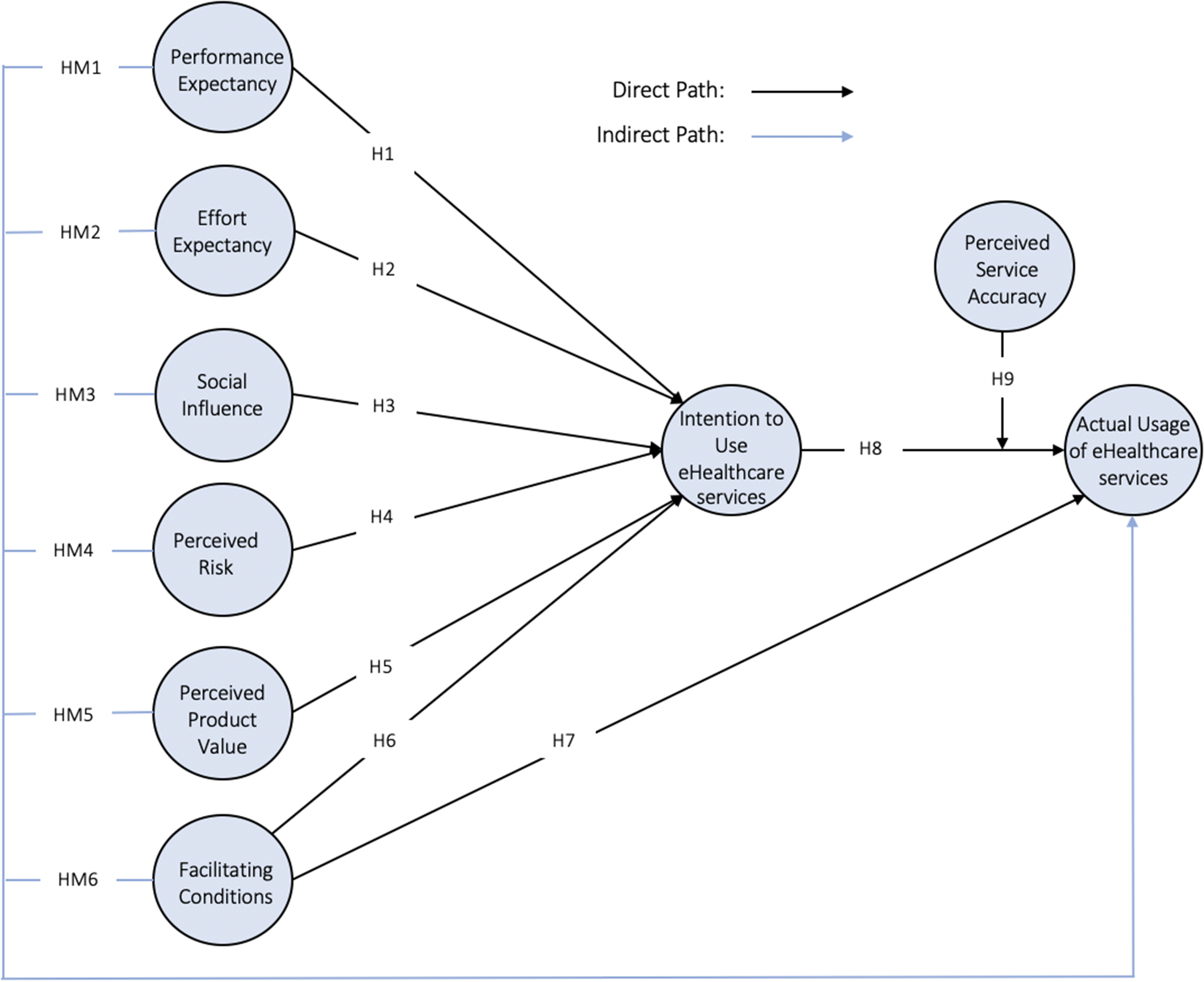
Research framework.
Research methodology
This study investigated individuals’ behavioral factors influencing their intention to use and usage of e-healthcare services. We adopted a quantitative research method using a cross-sectional research design for the collection of data at a single point in time that offered a snapshot of respondents’ attitudes, perceptions, and behaviors related to e-healthcare services. We used a structured survey questionnaire to collect data.
Population and sampling method
The sample population comprised Malaysians adults who were older than 40 years. Thus, individuals were the unit of analysis. Owing to shifts in lifestyles and the increasing prevalence of chronic diseases, this age group requires comprehensive, accessible, and technology-driven healthcare services. Thus, we collected data from this respondent population. We used convenience sampling for data collection because we selected respondents based on their accessibility and willingness to participate. The exploratory nature of this study also made it suitable for convenience sampling, as recommended by Andrade. 47
Survey instrument
The measurement items were adapted from existing literature and modified slightly to match the context of this study. However, we conducted a thorough review of relevant literature to ensure that the constructs and items included in the questionnaire were theoretically grounded and aligned with the objectives of our study. Additionally, we consulted with experts in the field to assess content validity and refine the questionnaire items based on their feedback. To establish reliability, we also conducted a pilot study by collecting data from 35 participants to assess the clarity, comprehensibility, and internal consistency of the items. We then performed statistical analyses, such as Cronbach's alpha coefficient, to assess the internal consistency reliability of the scales used in the questionnaire. We used a 5-point Likert scale to assess the variables, ranging from 1 = strongly disagree to 5 = strongly agree. The questionnaire comprised two sections. The first section included questions to obtain information about the respondents, such as gender, age, employment status, chronic illness, exercise frequency, monthly income, marital status, education, weight category, and physical fitness. The second section included questions on integrated variables. The details of the survey instrument are presented in Table 1 and Table S1 in the online supplemental materials.
Details of the survey instrument.

Note. PE: performance expectancy; EE: effort expectancy; SI: social influence; PR: perceived risk; PP: perceived product value; FC: facilitating conditions; PA: perceived service accuracy; IeH: intention to use e-healthcare services; AeH: actual usage of use e-healthcare services.
Sample size calculation and data collection process
We conducted a G*power test (version 4) to estimate the approximate sample size, as recommended by Hair et al. 53 We set the parameters of effect size (f2) as 0.15, power 1-β err Prob as .95, and number of predictors as 8. This yielded a G*power generated minimum sample size of 160. The respondents were recruited based on specific criteria. Only Malaysian residents aged 40 years or older were eligible to participate in the study. Additionally, individuals who had experience with or were potential users of e-healthcare services were included in the sample. We employed a self-administered survey questionnaire to gather data from the participants. The online survey questionnaire (Google Form) was disseminated over multiple online platforms and social media groups, such as Facebook and WhatsApp. We added a statement to the questionnaire that informed participants that they had the option to withdraw from the survey at any time and that their personal information would be safeguarded. A short explanation of e-healthcare services was also included to help participants understand the topic of the study. To foster participation, we regularly shared the online form and extended an offer to take part in the survey on a weekly basis from July to September 2023. To avoid potential complications, a total of 393 responses were collected versus a minimum sample size of 160. The STROBE Statement includes a checklist of items that can be found in Table S2 in the online supplemental materials.
Data analysis method
We used partial least-squares-structural equation modeling (PLS-SEM) to evaluate the data and test our proposed framework. This method is suggested when the nature of the study is exploratory with the aim of providing new theoretical insights or expanding existing theories. 54 PLS-SEM is also recommended for assessing complex frameworks with numerous variables and indicators. This method is appropriate for predicting a specific phenomenon by evaluating a proposed model. 55 Hence, we employed PLS-SEM to develop and explore a novel theoretical model that extended the UTAUT by including specific constructs with numerous indicators to predict individuals’ intentions to use e-healthcare services and their actual usage.
Demographic details
The demographic data (Table S3 in the online supplemental materials) display that 56.7% of the respondents were male, and 43.3% were female. The age distribution of the respondents showed that 53.7% were aged 51–60 years. Among them, 44.3% were employed full-time, while 27% were self-employed. Most of the respondents had a secondary school certificate (45.8%) or a diploma (35.4%). The marital status of the participants was primarily married (66.7%), followed by single (12.7%) and divorced (12.5%). More than two-thirds (65.1%) of the participants reported not having a chronic illness, while the remaining third (34.9%) reported having one. The majority of the respondents (84.7%) were physically fit, while 15.3% were physically unfit. In terms of weight, 60.1% reported having a healthy weight range, and 32.1% were slightly overweight. Regarding exercise, 49.1% of participants reported sometimes exercising, 26% reported often, 16.8% reported rarely, 3.8% reported never, and 4.3% reported always exercising.
Results
Common method bias
Common method bias (CMB) can occur when data are collected from a single source. 56 Hence, Harman's single-factor test was used to determine the presence of CMB. Specifically, the variance explained by a single source should be less than 50% of the total variance explained. The results revealed that the variance explained by a single factor was 22.892, which is lower than the recommended threshold. Moreover, we tested the presence of CMB by assessing the full collinearity of all constructs, as suggested by Kock. 56 Specifically, the variance inflation factor (VIF) of the constructs should be lower than three. Table 2 shows the results, which indicate that all values were lower than 3. Therefore, the data were free of CMB issues.
Full collinearity test.

Note. PE: performance expectancy; EE: effort expectancy; SI: social influence; PR: perceived risk; PP: perceived product value; FC: facilitating conditions; PA: perceived service accuracy; IeH: intention to use e-healthcare services; AeH: actual usage of e-healthcare services.
Multivariate normality
The Web Power online tool (https://webpower.psychstat.org/models/kurtosis/) was used to examine the multivariate normality. The Mardia skewness and kurtosis p-values were less than .05, confirming the non-normality of the data.
Measurement model
The measurement model was assessed by verifying the reliability, convergent validity, and discriminant validity of the constructs. Reliability was achieved with Cronbach's alpha values greater than .70. Convergent validity was achieved as composite reliability (CR) exceeded 0.70 and the average variance extracted (AVE) exceeded 0.5 (as shown in Table 3). Discriminant validity was assessed using the Fornell and Larcker criterion, heterotrait-monotrait (HTMT) ratio, and cross-loadings. According to the Fornell and Larcker criterion, the square root of the AVE of each construct should exceed its correlations with the other constructs. The results are presented in Table S4 in the online supplemental materials, which show that the square root of the AVE of each construct exceed its corresponding column and row. We then assessed the HTMT matrix. According to this criterion, the HTMT values should be lower than 0.90. The results are presented in Table S4 in the online supplemental materials, which show that all values were less than the recommended threshold. We also evaluated cross-loadings by checking whether the loadings of the intended construct exceeded those of other constructs. The results presented in Table S4 and Figure S1 in the online supplemental materials meet the stipulated criteria. Overall, this ensured the reliability and validity of the constructs used to create the measurement model.
Reliability and validity.

Note. PE: performance expectancy; EE: effort expectancy; SI: social influence; PR: perceived risk; PP: perceived product value; FC: facilitating conditions; PA: perceived service accuracy; IeH: intention to use e-healthcare services; AeH: actual usage of e-healthcare services; SD: standard deviation; CA: Cronbach's alpha; CR: composite reliability; AVE: average variance extracted; VIF: variance inflation factors.
Structural model
We evaluated the structural mode by examining the results of the direct and indirect effects, coefficients of determination, and effect sizes of the constructs.
Direct effects
The direct effect results are presented in Table 4 and Figure 2. These results enabled us to achieve RQ1, RQ2, and RQ3. Specifically, the relationships between performance expectancy and intention to use e-healthcare services (β = .163, p = .011), effort expectancy and intention to use e-healthcare services (β = .175, p = .002), and social influence and intention to use e-healthcare services are positive and significant (β = .138, p = .002). Hence, H1, H2, and H3 are supported. However, the relationship between perceived risk and intention to use e-healthcare services is negative and insignificant (β = –.064, p = .081); thus, H4 is rejected. Nevertheless, the relationships between perceived product value and intention to use e-healthcare services (β=.188, p = .009), facilitating conditions and intention to use e-healthcare services (β = .288, p = .001), actual usage of e-healthcare services (β = .191, p = .028), and intention to use e-healthcare services and actual usage of these services are positive and significant (β = .566, p = .000). Thus, H5, H6, H7, and H8 are supported.

Structural model with findings.
Hypothesis testing.

Note. PE: performance expectancy; EE: effort expectancy; SI: social influence; PR: perceived risk; PP: perceived product value; FC: facilitating conditions; PA: perceived service accuracy; IeH: intention to use e-healthcare services; AeH: actual usage of e-healthcare services; SE: standard error.
Indirect effects
The results of the indirect (mediating) effects are presented in Table 4, which support the achievement of RQ4. In particular, intention to use e-healthcare services has significant positive mediating effects on the relationships between performance expectancy and actual usage of e-healthcare services (β = .093, p = .014), effort expectancy and actual usage of e-healthcare services (β = 0.099, p = 0.007), and social influence and actual usage of e-healthcare services are positive and significant (β = .078, p = .002). Therefore, HM1, HM2, and HM3 are supported. However, intention to use e-healthcare services has a negative mediating effect on the relationship between perceived risk and actual usage of e-healthcare services (β = –.036, p = .084); therefore, HM4 is rejected. Nonetheless, the mediating effects of intention to use e-healthcare services on the relationships between perceived product value and actual usage of e-healthcare services (β = .106, p = .025), facilitating conditions and actual usage of e-healthcare services are positive and significant (β = .163, p = .000); therefore, HM5 and HM6 are supported.
Moderating effect
Table 4 presents the results of the moderating effect, enabling us to obtain RQ5. Perceived service accuracy had an insignificant effect (β = –.001, p = .495) on the relationship between the intention to use and actual usage of these services. Therefore, H9 is not supported.
Coefficient of determination (r2)
We evaluated the coefficient of determination (r2) to determine the degree of variance explained by the exogenous constructs among the endogenous constructs. Endogenous latent variables are typically classified as weak, moderate, or substantial based on their r2 values, which are .25, .50, or .75, respectively. Table 4 presents the results. The r2 value of intention to use e-healthcare services (.444) implies that performance expectancy, effort expectancy, social influence, perceived risk, perceived product value, and facilitating conditions explained 44.4% of the variance in intention to use e-healthcare services. Similarly, the r2 value of the actual usage of e-healthcare services (.484) signifies that facilitating conditions and intention to use e-healthcare services explain 48.4% of the variance in the actual usage of e-healthcare services.
Effect size (f2)
We assessed the effect size (f2) of the constructs to understand the functional influence of a particular exogenous variable on the endogenous variable, as suggested by Hair et al. 53 According to Cohen 57 f2 can be categorized as large (0.35), medium (0.15), or small (0.02). The results are presented in Table 4, which shows small effect sizes (f2) for most of the relationships. Specifically, PE → IeH, EE → IeH, SI → IeH, PR → IeH, PP → IeH, FC → AeH, and PA → AeH. However, the effect sizes (f2) for the relationships FC → IeH and IeH → AeH were medium and large, respectively.
Importance performance analysis
We also used importance–importance–performance map analysis (IPMA) to gain a deeper understanding of the perceptions and priorities of the participants concerning the main variables. This method, first introduced by Martilla and James 58 enabled us to assess the relative importance of each construct and evaluate its performance in enhancing the intentions and actual usage of e-healthcare services among Malaysians. The results of the IPMA are illustrated in Figure 3, where the vertical axis signifies the “importance” measure, which is the total effect, while the horizontal axis represents the “performance” measure, denoted by the index values. Clearly, facilitating conditions substantially influence the shaping of the intentions of adult Malaysians to use e-healthcare services, translating into the actual usage of those services. Additionally, perceived product value, effort expectancy, performance expectancy, and social influence showed higher levels of performance; however, they were moderately important in enhancing the intention to use e-healthcare services towards their actual usage among Malaysian people. However, perceived risk demonstrated less performance and importance.

Importance performance analysis.
Multi-group analysis
This study also conducted partial least-squares multigroup analysis (PLS–MGA). Before employing the PLS-MGA, we evaluated measurement invariance using the measurement invariance of composite models (MICOM) approach to determine the degree of homogeneity between the groups. The results of the MICOM analysis are presented in Table S5 in the online supplemental materials. The permutation p-values for several constructs exceeded the threshold of 0.05, confirming measurement invariance among the groups. Thus, we could perform PLS-MGA.
Table 5 presents the PLS-MGA results, which indicate no significant differences between the two age groups in terms of p-values (>.05) for all constructs. However, we observed p values lower than .05 (<.05) in the gender, chronic illness, and weight groups. The measurement invariance of the two gender groups (male and female) was also examined, revealing a significant difference in the relationship between facilitating conditions and the intention to use e-healthcare services, and the relationship between performance expectancy and actual usage of e-healthcare services among male and female respondents. Moreover, significant differences were observed in the relationships between social influence and intention to use e-healthcare services, and the relationship between effort expectancy and actual usage of e-healthcare services among respondents with and without chronic illness. Significant differences were also observed in the relationships between effort expectancy and intention to use e-healthcare services, facilitating conditions, and actual usage of e-healthcare services among respondents with healthy weight and those who were overweight.
Multi-group analysis results.
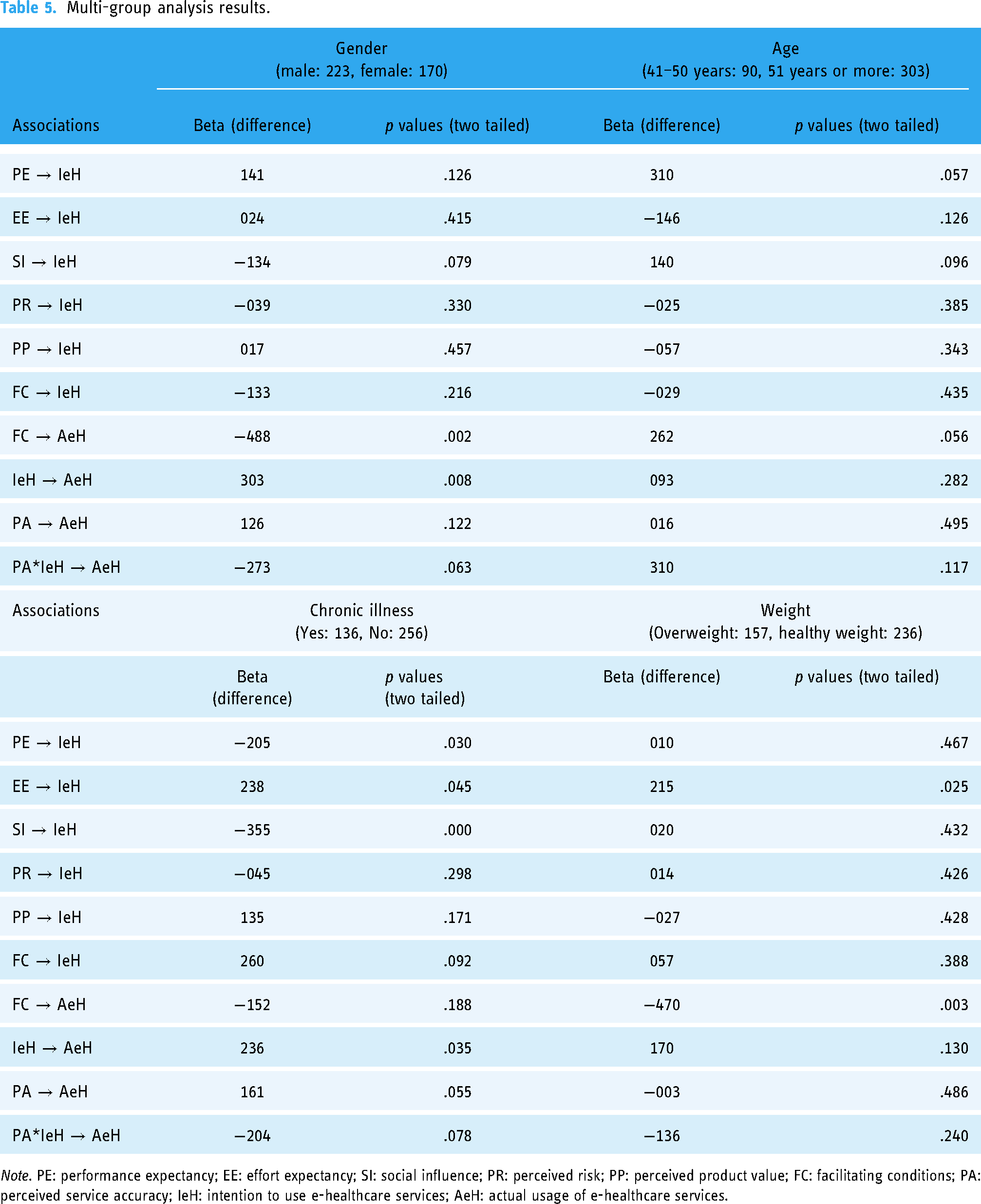
Note. PE: performance expectancy; EE: effort expectancy; SI: social influence; PR: perceived risk; PP: perceived product value; FC: facilitating conditions; PA: perceived service accuracy; IeH: intention to use e-healthcare services; AeH: actual usage of e-healthcare services.
Discussion
This study developed a model to understand individuals’ behavioral factors that influence their intention and actual behavior toward using e-healthcare services. We developed eight direct and six indirect hypotheses to test our model. The findings revealed that all proposed direct hypotheses were supported, except for the relationship between perceived risk and intention to use e-healthcare services. Additionally, all indirect hypotheses were supported, except for the indirect effect of intention to use e-healthcare services on the relationship between perceived risk and actual use of e-healthcare services. These findings are consistent with the existing literature and theoretical justifications.
Consistent with healthcare services research, we found that performance expectancy was significantly related with the intention to use e-healthcare services (H1). When individuals expect improved healthcare management and a better understanding of health issues from a service or technology, they are more likely to adopt and utilize it with greater intention. These findings are consistent with those of Zhang et al. 26 and Dash and Sahoo. 35 Next, effort expectancy and the intention to use e-healthcare services had a significant association (H2), consistent with the findings of Wu et al. 41 and Sahoo et al. 25 Thus, individuals who consider e-healthcare services to be user-friendly and simple to use are inclined to have a favorable intention to engage with digital health platforms. The observed positive correlation emphasizes the significance of the user experience and interface design in shaping individuals’ attitudes toward e-healthcare services.
Next, social influence and the intention to use e-healthcare services (H3) are significantly associated, consistent with Dash and Sahoo 35 and Sahoo et al. 25 Hence, the endorsement of e-healthcare platforms by family and friends substantially influences individuals’ decision to adopt these services. However, we found no negative association between perceived risk and the intention to use e-healthcare services (H4), thereby contradicting the findings of previous studies. Sahoo et al. 25 found that perceived risk negatively affects both effort expectancy and performance expectancy, which are key determinants of the intention to use e-health consultations. Zhang et al. 26 found that perceived risk was not significantly related to patients’ behavioral intentions, indicating that patients did not perceive online health communities as risky or uncertain. One plausible interpretation of the non-conforming results is that, in the specific demographics of Malaysian adults over 40 years of age, perceived risk may not be a dominant inhibiting factor in forming positive intentions toward e-healthcare services. Factors such as perceived benefits, trust in technology, and the influence of social networks may rather play a substantial role in shaping intentions, thereby mitigating the perceived risks associated with adopting digital health solutions. 26 Additionally, the discrepancy could be attributed to cultural nuances or specific characteristics of the study population, whereby perceived risk might be weighed differently in the decision-making process regarding e-healthcare adoption.
Nonetheless, the association between perceived product value and intention to use e-healthcare services (H5) was proven valid, consistent with Sahoo et al. 25 and Hayat et al. 59 According to the principles of consumer behavior, consumers commonly evaluate their purchases to assess whether they have met their desires or requirements, and subsequently, compare this assessment to the price they have paid. If an individual receives high value from a product or service, they become satisfied with that product or service, and intend to produce favorable intentions to adopt. Our study also validated the relationships between facilitating conditions and the intention to use e-healthcare services (H6) toward the actual usage of e-healthcare services (H7), in line with Gu et al. 14 Furthermore, our study confirms the relationship between facilitating conditions and actual usage of e-healthcare services, as demonstrated by Hossain et al. 30 Establishing favorable conditions, such as a conducive environment, adequate infrastructure, and seamless access to healthcare services, can foster individuals’ inclination to adopt these services. When individuals exhibit favorable intentions toward e-healthcare services, they are more likely to engage in concrete actions that promote their continuous use.
The findings also validated the substantial association between the intention to use e-healthcare services and the actual usage of these services (H8), consistent with Hayat et al. 59 Thus, individuals with positive intentions toward e-healthcare services are more likely to use these services continuously. In summary, the positive effects of the influential factors of e-healthcare services, including performance expectancy, effort expectancy, social influence, perceived product value, and facilitating conditions, produce favorable intentions among users, which subsequently lead to the actual usage of these services.
Next, we find that individuals’ intention to use e-healthcare services acts significantly and positively mediates the relationships between contextual factors and their actual use of e-healthcare services (HM1, HM2, HM3, HM5, and HM6). However, intention to use e-healthcare services negatively mediates the relationship between individuals’ perceived risk and their actual usage of e-healthcare services (HM4). Thus, individuals who perceive e-healthcare services positively in terms of enhanced performance outcomes and reasonable prices, and who have received positive recommendations from their social network are more likely to form favorable intentions toward using these services. These intentions are then translated into practical engagement with the services.
Implications
Theoretical contributions
Our study provides valuable insights that can be employed to enhance the UTAUT model and consumer behavioral actions. In the e-healthcare literature, UTAUT has been extensively utilized to examine individuals’ intentions to adopt technological innovations. For example, Yang et al. 24 delved into the adoption of m-health, Arfi et al. 19 explored the use of IoT in eHealth, Gu et al. 14 scrutinized e-Health Technology and Wang et al. 23 studied healthcare wearable devices; however, very few studies have focused on the critical factors that influence e-healthcare services adoption intention and actual usage among individuals. To address this knowledge gap, the present study investigates the behavioral and contextual factors that shape e-healthcare services adoption among users. Theoretically, this study makes a significant contribution to the field of technology adoption and consumer behavior, with a specific focus on the adoption of e-healthcare services.
Using the core constructs of UTAUT, including performance expectancy, effort expectancy, social influence, and facilitating conditions, we incorporated two additional constructs, perceived risk, and product value. These theoretical advancements contribute to the existing body of knowledge by extending the UTAUT model to include critical contextual variables that influence user behavior. The integration of perceived risk adds depth to our understanding of how user concerns can impact technology adoption, providing valuable insights for both researchers and practitioners. Additionally, the distinction between product and price value, along with the introduction of perceived service accuracy, further enriches the framework for analyzing technology adoption. These contributions not only enhance the explanatory power of the UTAUT model but also offer practical insights for practitioners aiming to improve user acceptance and satisfaction. We also empirically validated this robust theoretical framework to understand the intricacies of e-healthcare services. This integration aims to address the complex nature of user perceptions, and helps improve and modify existing theoretical models. Moreover, the literature on e-healthcare has mainly focused on exploring adoption intentions and actual usage of these services. The mediating effect of intention to use e-healthcare services has rarely been investigated. This study fills this gap, providing another noteworthy contribution to e-healthcare research.
We focus on Malaysia, which is undergoing a significant technological transformation. While studies have explored the general acceptance of e-healthcare services, no comprehensive examination of these factors has been conducted, particularly within the cultural and societal contexts of Malaysia. Our study fills an important gap in this context. Moreover, our focus on individuals aged 40 years or older represents a significant contribution, as this demographic requires extensive health support.
Moreover, this study employed IPMA and PLS–MGA, which have rarely been applied in e-healthcare studies. Thus, we provide a more nuanced understanding of the phenomena under investigation. The IPMA facilitated a comprehensive analysis of respondents’ perceptions and priorities regarding the key constructs in the framework. Furthermore, the application of PLS–MGA, a non-conventional method, provides valuable insights into the variations in relationships across different categorized groups. These innovative approaches significantly contribute to e-healthcare research.
Practical implications
This study offers noteworthy implications for managers and policymakers involved in strategic decision making for e-healthcare services, particularly in developing countries such as Malaysia. The findings on the performance and effort expectancy of e-healthcare services suggests that healthcare providers should focus on targeted communication and training programs which enable them to attract potential customers to adopt their services. Furthermore, healthcare providers should concentrate on demonstrating the advantages of e-healthcare services, including enhanced healthcare facilities with easy accessibility, which can foster positive behavioral intentions among individuals to avail these services. In Malaysia, many healthcare facilities, including hospitals, continue to rely on manual processes. Few have adopted a hybrid approach that combines manual and digital systems. Thus, to promote the adoption of e-healthcare services among adult Malaysians, e-healthcare providers should emphasize performance and effort expectancy. Recognizing the influential role of social influence, interventions should also leverage the support of family and friends to promote e-healthcare adoption. Healthcare providers should implement strategies to involve existing users as advocates, and highlight positive experiences and outcomes. Peer-driven initiatives and community engagement can contribute to building a supportive social environment that is conducive to e-healthcare adoption.
Our results emphasize the importance of safeguarding user data in e-healthcare services. Therefore, providers of such services should develop digital health systems that ensure the secure and encrypted storage of user data. They must address the potential risks associated with the use of e-healthcare services, and ensure that users’ data are fully protected and their privacy is completely respected. Service providers must also establish effective communication with users to maintain the necessary safety measures. Furthermore, governments should establish comprehensive data protection policies and strategies specifically for the e-healthcare sector.
A survey conducted by the Ministry of Health Malaysia indicated that Malaysian adults aged over 40 years require comprehensive, accessible, and technology-driven healthcare services because of demographic aging, increasing prevalence of chronic diseases, and lifestyle shifts to address diverse health needs and enhance their overall well-being. 60 Thus, interventions should be tailored to address their unique needs and concerns of this age group. Initiatives aimed at improving digital literacy, assisting technology adoption, and addressing potential age-related barriers can enhance the overall adoption experience.
Finally, government agencies and service providers should take initiatives to continuously monitor and evaluate user experiences. E-healthcare involves various dimensions, including technology adoption. Regular feedback mechanisms, user surveys, and usability assessments can provide valuable insights for future improvements. Healthcare providers should be responsive to user feedback, and adapt and evolve e-healthcare services to align with changing user needs and preferences.
Limitations and future recommendations
This study has several limitations. First, its cross-sectional design limits its ability to establish causal relationships; longitudinal studies are necessary to explore the dynamic processes involved in e-healthcare adoption over time. Second, our quantitative approach prevented us from obtaining a more comprehensive understanding through user interviews. A qualitative or mixed-methods approach can provide a richer understanding of users’ experiences, perceptions, and contextual factors that influence e-healthcare adoption. Third, the study only focused on Malaysian adults aged over 40 years, limiting the generalizability of the findings to other age groups and cultural contexts. Future research should explore diverse demographic groups to more comprehensively understand the dynamics of e-healthcare adoption. Fourth, this study did not consider cultural factors, despite Malaysia having diverse cultural influences. Future studies should delve deeper into the specific cultural factors influencing e-healthcare adoption, because understanding how cultural nuances interact with technology acceptance can inform culturally sensitive interventions. Fifth, although this study integrated additional constructs (perceived risk and product value) into the UTAUT model, it did not explore several other potential determinants that may influence e-healthcare adoption, which should be done in future works. Finally, the study employed a convenience sampling technique. Thus, the sample may suffer from bias, which can affect the generalizability of the findings. Future studies can use, say, cluster or stratified sampling to obtain more nuanced results.
Conclusions
This study investigated the factors and dynamics of e-healthcare adoption among adults aged over 40 years using the UTAUT model as a theoretical framework. The proposed model was empirically tested using data collected from 393 Malaysian respondents. The findings revealed that performance expectancy, effort expectancy, social influence, and perceived product value significantly influenced individuals’ intentions to use e-healthcare services, whereas perceived risk had a significantly negative effect. Additionally, facilitating conditions significantly influenced individuals’ intentions to use and actual usage of e-healthcare services. Furthermore, individuals’ intentions to use e-healthcare services significantly influenced their actual use of these services. Next, intention to use e-healthcare services mediated the relationship between the factors and usage of e-healthcare services, except for perceived risk. Surprisingly, perceived service accuracy had no significant moderating effect on the relationship between individuals’ intention to use and their actual use of e-healthcare services. Moreover, the IPMA findings revealed the substantial importance and performance of facilitating conditions in shaping individuals’ intentions toward the actual usage of e-healthcare services. Next, perceived product value, effort expectancy, performance expectancy, and social influence showed higher levels of performance, but moderate importance. Additionally, PLS-MGA revealed significant differences in e-healthcare adoption patterns among gender, chronic illness, and weight groups, whereas no differences were observed in the age group. This revealed the demographic variations in e-healthcare adoption patterns.
This study stands out because of its innovative expansion of the UTAUT framework by incorporating the constructs of perceived risk and product value, and validating the mediating effect of the intention to use e-healthcare services, thereby offering a more comprehensive understanding of the factors shaping e-healthcare service adoption behavior. Moreover, IPMA and PLS-MGA were used to uncover intricate contextual and demographic variations in e-healthcare adoption patterns. By focusing on the unique demographics of older adults, this study advances research by incorporating new dimensions into a theoretical framework and employing sophisticated analytical techniques. These novel perspectives and valuable insights into the complex dynamics of e-healthcare adoption enhance the academic discourse in this field.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241272577 - Supplemental material for Ageing well with tech: Exploring the determinants of e-healthcare services adoption in an emerging economy
Supplemental material, sj-docx-1-dhj-10.1177_20552076241272577 for Ageing well with tech: Exploring the determinants of e-healthcare services adoption in an emerging economy by Chinnasamy Agamudai Nambi Malarvizhi, Abdullah Al Mamun, Mohammad Nurul Hassan Reza and Muhammad Mehedi Masud in DIGITAL HEALTH
Supplemental Material
sj-csv-2-dhj-10.1177_20552076241272577 - Supplemental material for Ageing well with tech: Exploring the determinants of e-healthcare services adoption in an emerging economy
Supplemental material, sj-csv-2-dhj-10.1177_20552076241272577 for Ageing well with tech: Exploring the determinants of e-healthcare services adoption in an emerging economy by Chinnasamy Agamudai Nambi Malarvizhi, Abdullah Al Mamun, Mohammad Nurul Hassan Reza and Muhammad Mehedi Masud in DIGITAL HEALTH
Footnotes
Author note
Mohammad Nurul Hassan Reza, Faculty of Business and Management, UCSI University, Kuala Lumpur, Malaysia.
Contributorship
CANM and MMM contributed to conceptualization, methodology and writing–original draft. MNHR and AAM contributed to conceptualization, methodology, and writing–review and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
UKM Research Ethics Committee of Universiti Kebangsaan Malaysia approved this study (UKM/PPI/111/8/JEP-2023-466). This study has been performed in accordance with the Declaration of Helsinki. Written informed consent for participation was obtained from respondents who participated in the survey. No data were collected from anyone under 18 years of age.
Funding
This research received funding from Ministry of Higher Education, Malaysia (FRGS/1/2019/SS03/MMU/02/8).
Guarantor
Abdullah Al Mamun.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.