
Abstract
This study sought to determine how the proportion of physicians using electronic prescribing in nine US states was associated with the hospitalization rate for adverse drug events among older adult patients. A discharge-level analysis of the relationship between county electronic prescribing and adverse drug event hospitalization rates was conducted. Data from the 2011 State Inpatient Databases, the Office of the National Coordinator Health IT Dashboard, and the Area Health Resource File were obtained for nine US states. The analysis examined the odds that a discharge for older adults would have been adverse drug event associated, versus other causes, using multivariable logistic regression models. After adjusting for patient, provider, health infrastructure, and community factors, the lowest county electronic prescribing rate quartile was associated with significantly greater odds of an adverse drug event hospitalization (odds ratio: 1.10; 95% confidence interval: 1.02–1.19). Early results indicate greater odds of adverse drug event hospitalizations among older adults living in counties with low electronic prescribing rates when compared to those in high electronic prescribing counties.
Keywords
Introduction
Patient safety and quality of care have received increased attention from the healthcare industry since the release of the 1999 Institute of Medicine report, To Err is Human. 1 This heightened attention has continued as tools to identify adverse drug events (ADEs) and reactions are becoming widely available. ADEs, defined as injuries that are the result of medication, are of particular public health importance because of the increasingly high number of Americans taking prescription drugs, particularly older Americans. Across 2007–2010, approximately 40 percent of Americans aged 65 years and over used five or more prescription drugs in the past 30 days. 2 Occurrences of ADEs are also seen in older adults nearly seven times more often than among adults younger than 65 years, making ADEs an important indicator of patient safety. 3
ADEs that occur prior to hospital admissions are of particular interest because they are three times more common than ADEs that originate during a hospital stay. 4 Of all hospital stays, it is estimated that between 2.4 and 9.0 percent are caused by ADEs that are present at hospital admission.5–8 Von Laue et al. 8 determined that over half of ADEs were preventable. With the high risk and cost of ADEs in the older patient population, it is essential to ensure that effective and appropriate ambulatory prescribing habits are followed and ADEs that result in hospitalization are prevented.9,10
Kaushal et al. 11 describe the potential of health information technology (HIT) to improve patient safety in the outpatient setting. Additionally, Bates and Gawande 12 argue that electronic prescribing (e-prescribing) provides a method to reduce errors by preventing errors and adverse events. E-prescribing provides a tool to overcome the common risk factors of ADEs, including the lack of communication among concurrent prescribers.13–15
In an effort to increase the adoption of e-prescribing, federal legislation and incentive programs have been established. These programs include the Medicare Prescription Drug, Improvement, and Modernization Act of 2003; 16 the e-prescribing incentive program as part of the Medicare Improvements for Patients and Providers Act of 2008; 17 and most recently the electronic health record incentive program through the Health Information Technology for Economic and Clinical Health Act of the American Recovery and Reinvestment Act of 2009. 18 The combination of incentives has resulted in an increase in e-prescribing adoption from approximately 7 percent in December 2008 to 70 percent in April 2014. 19 However, whether the increase in HITs has resulted in meaningful population health improvements is undetermined.
Previous studies examining the impact of HIT on ADEs have been limited to a hospital setting and determining the rate of ADEs occurring within a hospital stay.20–32 No studies were found that examined the impact of HIT use in ambulatory settings on ADE hospitalizations. This study examines the odds of an older adult having an ADE hospitalization due to prescriptions provided outside a hospital setting, given the rate of e-prescribing in their county of residence.
Methodology
Theoretical model
An ecological modification of the Ancker et al. 33 Triangle Model was used as a theoretical framework for this analysis. While the Triangle Model lends itself to evaluating the impact of HIT within an organization, we utilized the framework at a systems/community level. The four main constructs of the Triangle Model (technology, provider, organization, and patient) were modified to technology, adopter/provider, healthcare infrastructure, community, and patient.
Data sources
Data were drawn from three datasets: 2011 Healthcare Cost and Utilization Project (HCUP) State Inpatient Databases (SID), 34 the ONC Health IT Dashboard—Health IT Adoption and Use dataset, 35 and the Health Resources and Services Administration (HRSA) Area Health Resource File (AHRF). 36 Datasets were merged using state and county Federal Information Processing Standards (FIPS) codes. 37 Key data elements for this study from HCUP SID include patient demographics, such as sex, age, race, number of chronic conditions using HCUP’s Chronic Condition Indicator for the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), and length of stay; principal diagnosis; and whether the diagnosis was present on admission (POA). 34 The POA indicator, commonly collected to provide documentation to Centers for Medicare and Medicaid Services, allows for the identification of ADEs that occurred in the community and are likely to be associated with outpatient provider prescriptions, rather than during a hospital stay. This study was exempted by the University of South Carolina Institutional Review Board.
Study sample
Due to budgetary constraints and per-state costs for HCUP SID files, this analysis used data from nine states: Arizona, Arkansas, Florida, Maryland, Michigan, Mississippi, New Jersey, Vermont, and Washington. States were chosen due to the availability of patient residence and POA indicator data elements while also allowing for the representation of at least one state from each of the four major US Census regions.
To ensure that our analysis did not inaccurately estimate the association between e-prescribing and ADE hospitalizations, several criteria were used to exclude discharges, hospitals, and counties from the county- and discharge-level analyses. Counties with missing e-prescribing rates were excluded (n = 16). Mirroring the analysis conducted by Weiss et al., 4 hospitals that reported all diagnoses as POA and hospitals with over 20 percent of discharges with missing POA indicators for non-missing diagnoses were excluded. The number of hospitals represented was reduced from 1099 to 899 after hospital exclusion criteria were applied. We also excluded discharges with missing age or age less than 65 years, missing POA information for non-missing diagnoses, and missing county of residence. Finally, discharges for out-of-state patients were excluded. The final study population consisted of 2,725,378 discharges across 404 counties.
Dependent variable
Following the algorithm utilized by Encinosa and Bae, 38 we modified the Lucado et al. 3 method to flag ADEs. To only identify ADEs that occurred within the community and outside of a hospitalization, our modification defines ADE hospitalizations as hospital discharges that had (1) a POA indicator and (2) an ICD-9-CM diagnosis code for an ADE. Both criteria were used to ensure that ADEs were acquired prior to hospitalization. The Lucado et al. 3 list of ICD-9 codes and external cause of injury codes were used to determine ICD-9 codes for ADEs. Discharges with ICD-9 codes that pertain to accidental poisonings, self-inflicted poisonings, and/or assault were not flagged as ADEs. The analysis utilized a dichotomous indicator of having an ADE hospitalization.
Independent variable
The ONC Health IT Dashboard—Health IT Adoption and Use dataset was utilized to determine the independent variable, the percentage of physicians e-prescribing in each county. The ONC Health IT Dashboard is an open government project that provides percentage of e-prescribers on the country’s largest e-prescribing network, Surescripts, by county.35,39 The adoption rate of counties was categorized as either high/low when compared to the median rate (35%).
Control variables
Multivariable analyses controlled for potential confounders at two levels: patient and county. Patient demographics controlled for patient sex, age group (65–74, 75–84, and 85+ years), race/ethnicity (White, African American, Hispanic, and Other), number of chronic conditions (0–20), and length of hospital stay in days. The HRSA AHRF was the source for control variables. Adopters/providers were determined through the AHRF by including the number of primary care physicians per 1000 population in the county (expressed in quartiles). Healthcare infrastructure was represented by including the number of hospital beds per 1000 population in the county (expressed in quartiles), whether the county had a hospital, and whether a county was designated as a Health Professional Shortage Area (HPSA; whole, partial, and none). Last, the community variables utilized included whether a county was rural (defined by the 2003 Urban Influence Code 40 of greater than 3), the percentage of the population living in poverty (expressed in quartiles), and the percentage of the population with less than a high school education (expressed in quartiles).
Analytic approach
A discharge-level analysis was used to determine whether the odds of a hospitalization being attributable to ADE were associated with county e-prescribing rates. Discharges were assigned to counties based on the patient county of residence. Differences across county e-prescribing adoption rates were assessed using Wald chi-square tests (α = 0.05). Multivariable logistic regression was utilized to identify patient and county characteristics that were associated with having an ADE hospitalization. Five logistic regression models were conducted to determine the impact of each major construct of the theoretical framework: technology, patient, adopters/providers, healthcare infrastructure, and community.
Results
Table 1 displays the characteristics of hospital discharges in the study population, by the county e-prescribing rate. Discharges for patients who resided in the highest e-prescribing counties were more likely female, between the ages of 65 and 74 years, White, and had a shorter length of hospital stay. The counties in which these patients reside have fewer primary care physicians, fewer hospital beds per population, are more likely to be whole county HPSA, are more likely to be rural, and have close to median levels of poverty and high school education levels.
Characteristics of hospital discharges among older adults, by electronic prescribing (e-prescribing) rates, 2011.
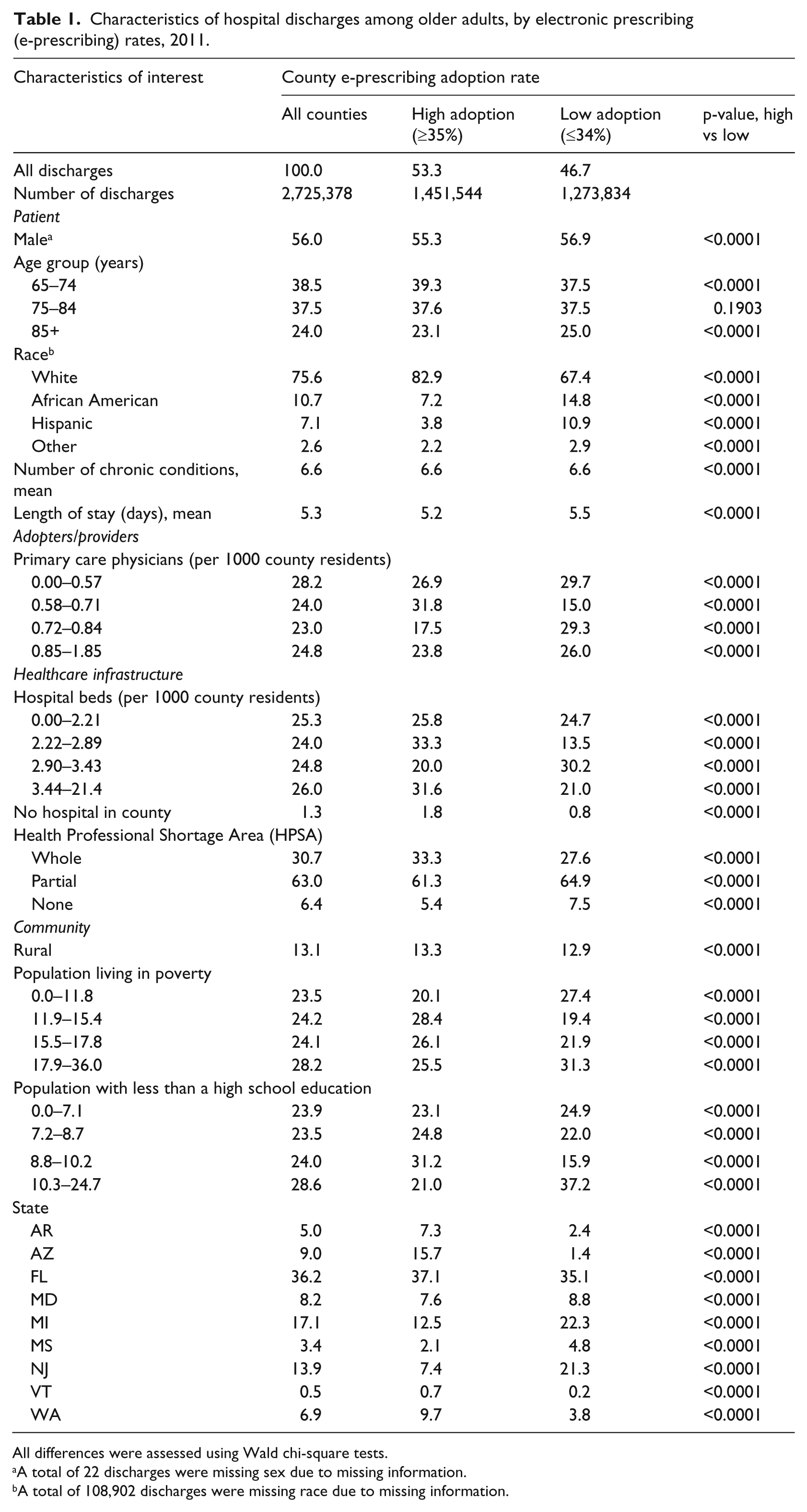
All differences were assessed using Wald chi-square tests.
A total of 22 discharges were missing sex due to missing information.
A total of 108,902 discharges were missing race due to missing information.
A total of 6400 of 2,725,378 (0.23%) discharges were due to ADEs that occurred in the community. The unadjusted proportion of all hospitalizations among persons 65 and older that included a community ADE was higher for counties with high e-prescribing adoption rates (0.25 versus 0.22; see Table 2). Other factors that were associated with proportionately more ADE hospitalizations included being female, between the ages of 65 and 74 years, White, living in a county with one or more hospitals, living in a HPSA or urban county, and residing in Washington, Arizona, or Florida.
Percent of older adult discharges that included a community ADE, by electronic prescribing (e-prescribing) rates, 2011.
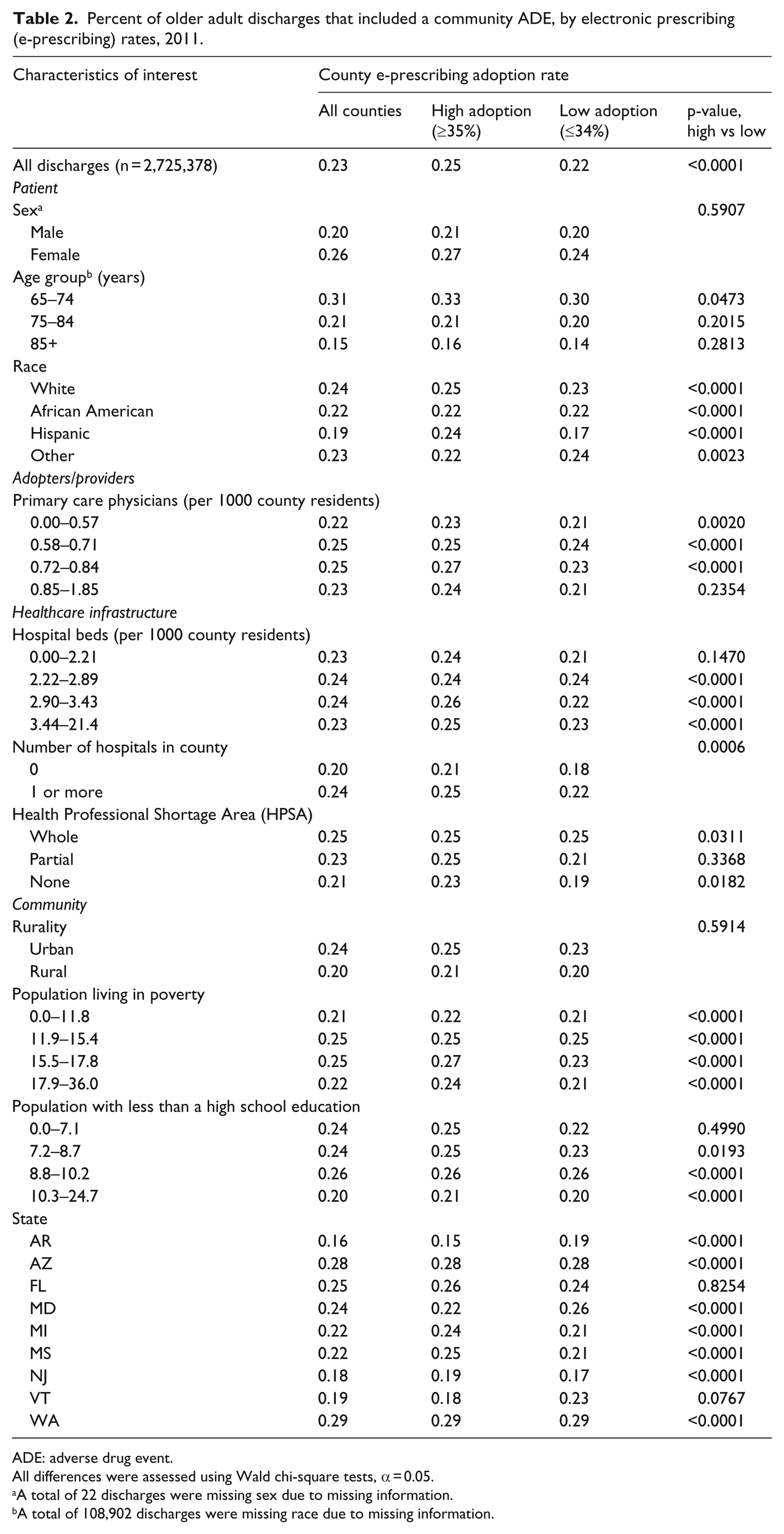
ADE: adverse drug event.
All differences were assessed using Wald chi-square tests, α = 0.05.
A total of 22 discharges were missing sex due to missing information.
A total of 108,902 discharges were missing race due to missing information.
The multivariate logistic model (see Table 3) estimated the odds of having an ADE hospitalization versus other diagnoses. Because this approach is based on all hospitalizations rather than all persons, our model controls for potential differences in the likelihood of hospitalization associated with regional variation in practice patterns. The first model included only the county e-prescribing rate. It found that residents of a county with a 30- to 34-percent adoption rate had lower odds of having an ADE hospitalization when compared to residents living in counties with an adoption rate of over 48 percent. When patient demographic information was added into the model (model 2), the odds of an ADE hospitalization for residents of a county with a 30- to 34-percent adoption rate were no longer significant. Other factors that were associated with having higher odds of an ADE hospitalization, when taking patient demographics into account, included being female and having additional chronic conditions. When adding the number of primary care physicians per 1000 population into the model (model 3), being female, having additional chronic conditions, and living in a county that have 0.72–0.84 primary care physicians per 1000 population were significantly associated with increased odds of ADE hospitalizations. Model 4 took healthcare infrastructure into account and there were no changes in significant factors. The final model (model 5) included all the previous variables and community factors. Model 5 indicates that the county e-prescribing rates that were in the lowest quartile (0%–29%) resulted in greater odds of an older adult having an ADE hospitalization when compared to counties in the highest quartiles of e-prescribing rates (⩾42%; odds ratio (OR): 1.10 (1.02–1.19)). Additionally, the model indicates that the odds of an ADE hospitalization are higher for females, individuals having more chronic conditions, individuals living in counties with 8.8–10.2 percent of the population having less than a high school education, and individuals living in Florida or Washington.
Adjusted odds of having an adverse drug event hospitalization among older adults, 2011.
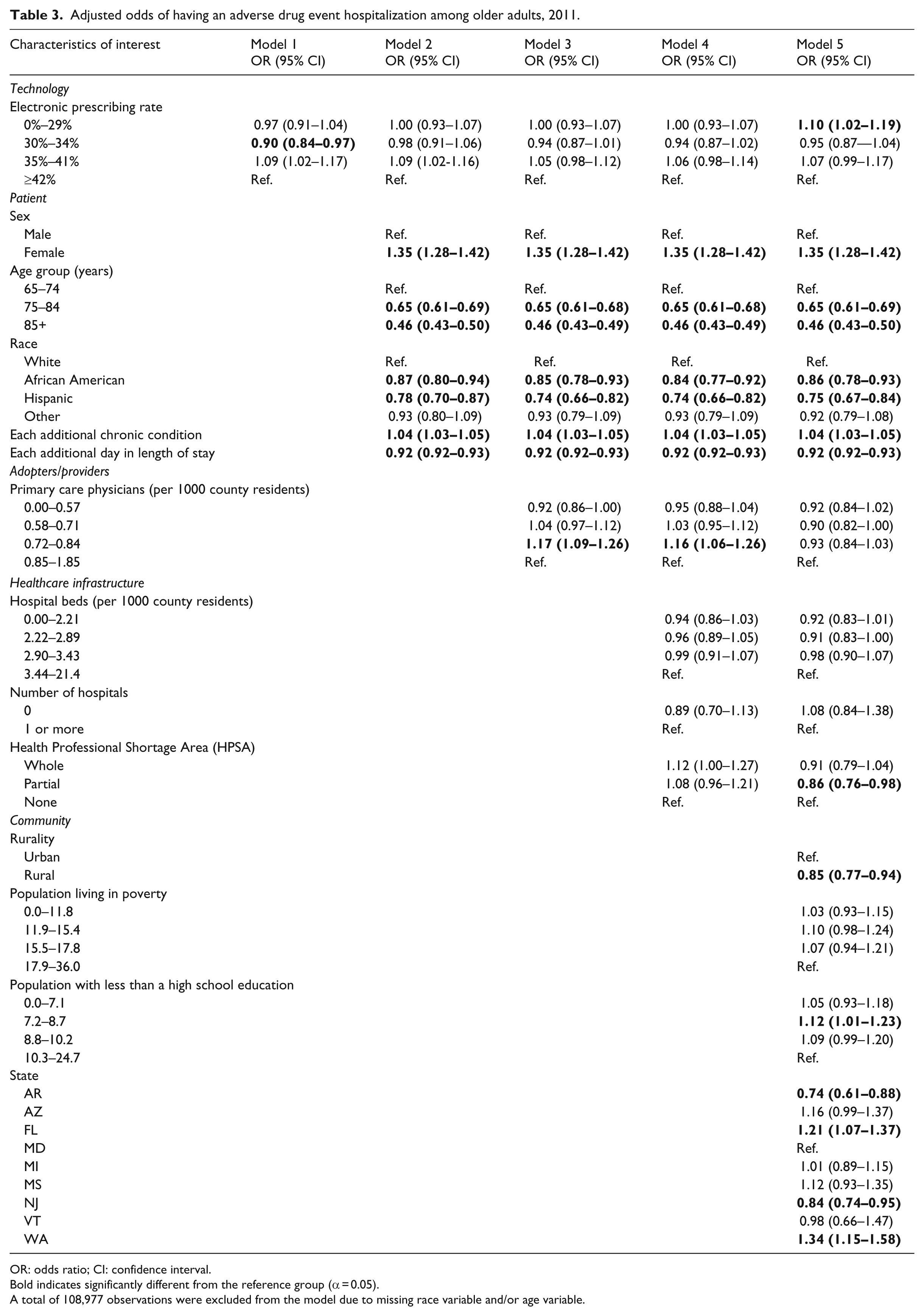
OR: odds ratio; CI: confidence interval.
Bold indicates significantly different from the reference group (α = 0.05).
A total of 108,977 observations were excluded from the model due to missing race variable and/or age variable.
Discussion
The analysis found e-prescribing rates at the county-level to be significantly associated with community-occurring ADE hospitalizations, but not in a simple manner. In unadjusted analysis, higher county-level e-prescribing was associated with a higher proportion of ADE admissions. However, in analysis adjusted for patient characteristics, the odds that an admission would be attributable to a community-occurring ADE were higher in counties with the lowest e-prescribing rate than among those in the highest category. Previous research in inpatient settings, including pediatric hospitals and intensive care units, have found no direct effect on ADEs.27,31,32,41 Research in other settings, such as a primary care clinic and long-term care facility, have demonstrated improved adherence to best-practice guidelines, but have been unable to demonstrate a reduction in ADE rates.26,30
Patient characteristics associated with increased odds of ADE hospitalization included being female and having a greater number of chronic conditions, while being older than 75 years, living in partial HPSA or rural areas, being African American or Hispanic, and having longer hospital stays were associated with reduced odds of ADE hospitalizations.
ADE admission rates varied across states, from 0.16 percent in Arkansas to 0.29 percent in Washington. Some differences persisted after adjusting for patient characteristics, with residents of Arkansas and New Jersey being less likely than residents of the referent state (Maryland) to experience an ADE admission, while Florida and Washington states remained elevated. The state variation in odds of an ADE hospitalization cannot be explained by variations in e-prescribing rates or POA reporting experience. In 2011, the states studied varied in e-prescribing rates from lowest to highest in the following order: New Jersey (31%), Mississippi (32%), Maryland (33%), Michigan (36%), Florida (37%), Arizona (42%), Washington (44%), Arkansas (45%), and Vermont (51%). 35 Additionally in 2011, Vermont had just begun reporting POA data to HCUP, Mississippi had reported for 2 years, Arizona, Arkansas, Michigan, New Jersey, and Washington had been reporting for 3 years, and Florida and Maryland had been reporting HCUP POA data for 4 years.
Although our findings detected a significant association between e-prescribing and community-occurring ADEs, the results should be interpreted with caution. Rogers’ Diffusion of Innovation theory suggests that the rate of innovation adoption gains momentum after 20 percent and continues to increase at an accelerated rate. 42 The national rate of e-prescribing increased from 7 percent in December 2008 to 70 percent in April 2014. 19 The mean e-prescribing rate for studied counties in 2011 was 37.9 percent, similar to the national mean of 41.4 percent. Rogers’ theory categorizes adopters during this stage as the “early majority.” Thus, our study potentially included counties comprising only early adopters. In addition, it is possible that e-prescribing rates need to be markedly higher than those observed to have consistent and sizeable effects on ADE occurrence.
Westphal and Shortell 43 found that early adopters of total quality management practices were more likely to adapt technologies to improve efficiencies within their organizations, while late adopters were more likely to conform to norms by adopting well-established programs. Studies also demonstrate that the true value of technology is how it is utilized by individuals and organizations.44,45 These studies demonstrate the need to address organizational and human factor changes to avoid unintended consequences.46–49 Further studies are necessary to determine whether gains in patient safety indicators continue to be seen with increasing adoption rates in a short- and long-term setting.
Limitations
This analysis may underestimate ADE hospitalization due to the underreporting of ADEs in administrative datasets.50,51 However, studies have noted the utility of using administrative data in detecting adverse events.51–54 This analysis was also restricted to nine states, which limits the generalizability of its findings.
We limited this analysis to ADE hospitalizations because they provide insight into the safety of ambulatory prescribing. 10 However, the definition utilized in this study was broad. Future analysis should indicate whether ADE hospitalizations are considered preventable, potential, or non-preventable. This distinction will allow for a better understanding of the performance of technologies such as e-prescribing. Previous studies have found decreases in preventable and potential ADEs.20,55 In addition, we only examined one HIT, e-prescribing; other technologies have also shown potential in decreasing ADEs and increasing patient safety. Given that e-prescribing can be viewed as an entry-level system when compared to more comprehensive HITs, this study provides a stepping stone to determine the impact HIT adoption is having throughout our nation. 56 We were also unable to determine the number of medications taken by an individual patient, patient medication adherence rates, and the underlying conditions of the patient in this analysis. However, data indicate that 89.7 percent of older adults have taken one or more prescription medications in the past 30 days. 57 Finally, we used an ecological measure for e-prescribing rates. This limited our ability to determine whether a patient with an ADE hospitalization was seen at a practice with e-prescribing capabilities.
Conclusion
Our results suggest that residents of low e-prescribing counties have greater odds of experiencing an ADE hospitalization, when compared to residents of high e-prescribing counties. Further research and monitoring that utilizes clinical, prescription, and other administrative datasets is necessary to determine the potential impact of e-prescribing and other health information technologies on patient safety indicators.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was partially supported by a Graduate Research Grant from the Office of the Vice President for Research at the University of South Carolina.