
Abstract
This article analyzes the range of system optimization activities taking place over an extended period following the implementation of computerized physician order entry and clinical decision support systems. We undertook 207 qualitative semi-structured interviews, 24 rounds of non-participant observations of meetings and system use, and collected 17 organizational documents in five hospitals over three time periods between 2011 and 2016. We developed a systematic analysis of system optimization activities with eight sub-categories grouped into three main categories. This delineates the range of system optimization activities including resolving misalignments between technology and clinical practices, enhancing the adopted system, and improving user capabilities to utilize/further optimize systems. This study highlights the optimization efforts by user organizations adopting multi-user, organization-spanning information technologies. Hospitals must continue to attend to change management for an extended period (up to 5 years post-implementation) and develop a strategy for long-term system optimization including sustained user engagement, training, and broader capability development to ensure smoother and quicker realization of benefits.
Background/context
Many countries are adopting health information technology (HIT) in an attempt to improve the quality and safety of care, while also reducing healthcare expenditure.1–4 In secondary care, this effort has tended to focus on electronic health records and associated computerized physician order entry (CPOE) and clinical decision support (CDS) systems. This technology is promoted with promises to improve patient safety and work flow, increase efficiency, and advance standardization of clinical practices. 5 These claims have been supported by historical studies of successful, home-grown, extensively customized CPOE/CDS deployments. 6 However, recent attempts to implement commercial CPOE/CDS systems have struggled to replicate these benefits and have in some cases yielded unintended consequences where, for example, commercial off-the-shelf (COTS) packaged solutions that were not well-aligned with clinical practices undermined improvements and threatened patient safety.7–9 This disparity in implementation outcomes underlines that the procurement of a system is a necessary, but not sufficient condition for successful adoption. Rather, the outcome of an implementation can be contingent on technical, social, and organizational factors.10–13 These factors vary across hospitals and can produce different outcomes when implementing the same system.13,14
We can most effectively account for the variability of implementation outcomes by considering system implementation as an extended mutual learning process where the fit between a technology and organizational setting is actively produced.15,16 Users adopting a new technology require time to acquire knowledge about its characteristics, which may only be fully realized through a prolonged period of use. 17 How this learning process unfolds across various professions, clinical settings, and local practices over time determines the prospects for effective adoption and use of new technologies in hospitals in the long run. 18 Health service change managers are beginning to explicitly address these issues as part of their strategies and policy guidelines for “benefit realization.” 19 The influential “Wachter Report” (Making IT Work: Harnessing the Power of Health IT to Improve Care in England, 2016 UK Department of Health) 4 drew attention to, and called for better understanding of, protracted system optimization activities following “go-live.” We thus analyze optimization as an ongoing process of interactive learning and adjustment that includes technical maintenance and development of the system, evaluation and improvement of clinical practices, and the exploration of opportunities offered by advanced or new functionalities. 20 However, as widespread implementation of commercial CPOE/CDS systems is only a recent development, little longitudinal research is available about how hospitals engage with the current generation of packaged software solutions. 21
Our study aims to shed light on the period after go-live of CPOE/CDS systems for electronic prescribing (ePrescribing) and to explore the various system optimization activities that users have undertaken to improve the fit between the technology and the practices and requirements of health professionals in particular clinical settings in English hospitals. We have gleaned insights from an extensive longitudinal qualitative study to develop a systematic analysis of system optimization activities, to present lessons learned, and to highlight the wide range of activities that users in hospitals may embark upon in the process of improving the clinical and administrative utility of CPOE/CDS systems.
Methods
This large-scale, multi-site, longitudinal evaluation of CPOE/CDS systems in English hospitals enabled the collection of a substantial body of information on the implementation and use of these systems. In this study (and the wider ePrescribing investigation), we applied a sensitizing perspective that attended to the long-term but intricate processes involved in HIT development, implementation, and use.
To examine optimization processes over time, we applied research design principles developed through the Biography of Artefacts and Practices (BoAP) perspective to address the evolution of technology systems and infrastructures over extended cycles of implementation and use.22–24 This analytical perspective captures the emergence and evolution of a technology and the configuration of its technical components with local practices as it moves across multiple sites over extended periods of time. In this perspective, an information system is conceived as part of an information infrastructure: a “system of systems” that is not built in one go as discrete solutions, but that grows iteratively over multiple cycles of development and use. 24 The BoAP provides methodological templates for examining the prolonged implementation and adoption processes of a CPOE/CDS system by extending enquiry across multiple sites and longitudinally given the prolonged timeframes of technology development and use. 24 Accordingly, this study follows various instances of CPOE/CDS system implementation and examines how learning processes played out over time as these systems were embedded in clinical practices in different wards and departments, and used by various professional groups including doctors, nurses, pharmacists, administrators, and other health care professionals.
Sampling
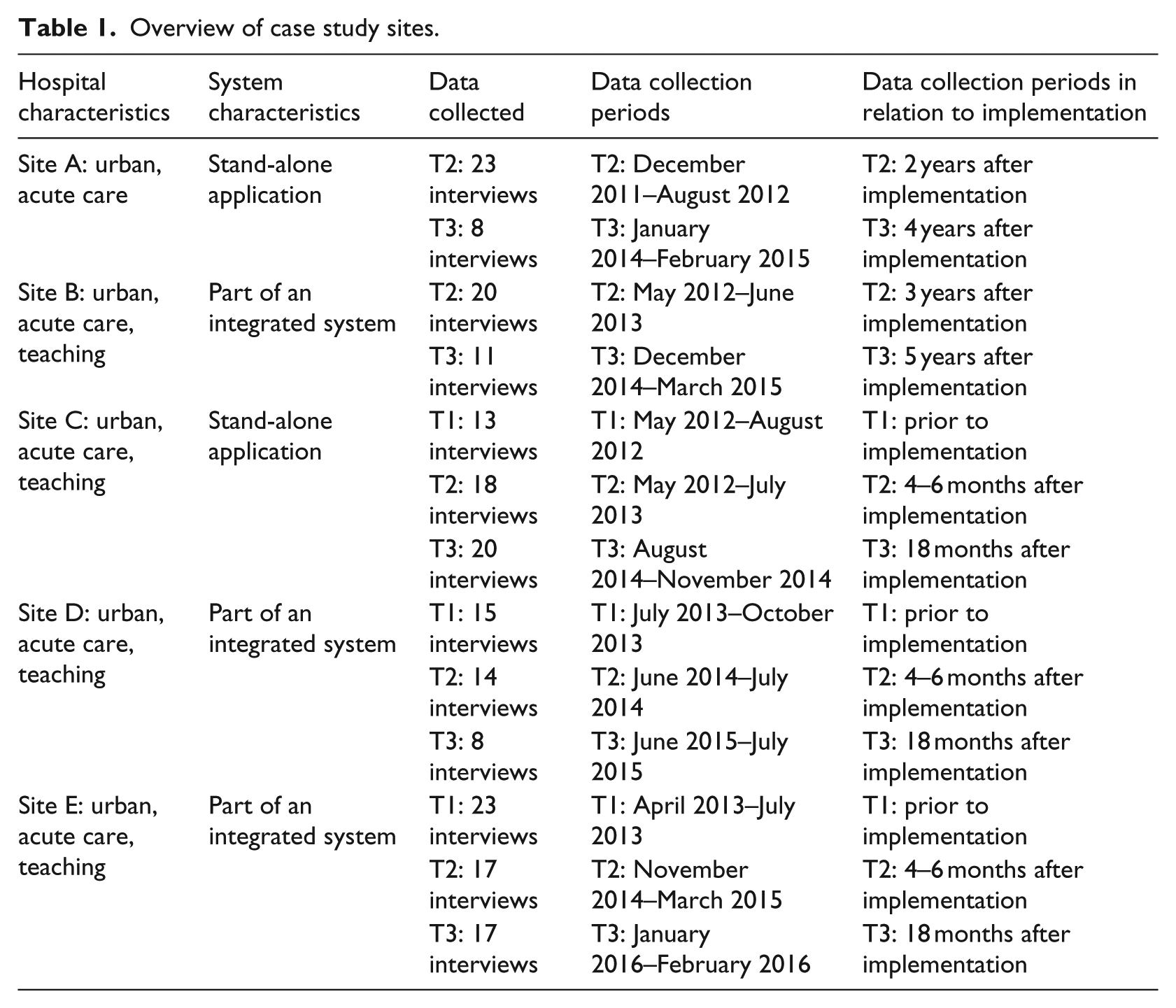
We used a purposive sampling strategy.25,26 Five urban hospitals were selected that had been carrying out or had plans to implement a packaged CPOE/CDS system during the course of the 5 year ePrescribing investigation (see Table 1). These were the (US and UK) solutions that had been most widely adopted across English hospitals. Three hospitals installed hospital-wide multi-modular integrated US systems of which CPOE/CDS was one component. These are split into multiple modules to serve different purposes, but which all run on a single, integrated database. The other two hospitals chose dedicated stand-alone applications (developed in the United Kingdom) to enable CPOE/CDS functionality. Initially, directors of pharmacy and other senior managers were contacted, who then subsequently identified relevant colleagues including doctors, nurses, pharmacists, allied health professionals, pharmacy technicians, and IT/implementation teams enabling a snowball sampling approach. Interviews were conducted at three time points (T1: prior to implementation, T2: 3–6 months after implementation, and T3: 1 year or more after implementation). There were no T1 data for sites A and B, which had already implemented systems before the study was launched. In consequence, in these cases, the T3 fieldwork covered later periods—4 to 5 years—after implementation. This allowed us to extend the timeframes of the analysis. All participants signed written informed consent forms to participate in the study. All identifiable data were anonymized at the point of transcription.
Overview of case study sites.
Data collection
As part of the large-scale, multi-site ePrescribing investigation, we (K.C., H.M., L.L., and A.K.) collected qualitative data including 207 semi-structured interviews with decision-makers and managers, clinical staff, and implementation teams; 24 rounds of non-participant observations of strategic meetings and system use; and 17 documents from hospitals and vendors. By pulling together data from different sources, our ethnographic inquiry highlighted contextual influences enabling us to produce rich accounts to understand the meanings of activities and the rationale of actions of individuals.27,28 Semi-structured interviews with healthcare professionals, implementers, and other healthcare staff involved in the implementation and use of the CPOE/CDS systems provided insights into the range and rationale of optimization activities taking place. A total of 24 rounds of non-participant observations of meetings and work routines contributed to deepening our understanding about how the implemented systems were embedded in clinical work practices. The collection of documents, including strategy papers, business cases, roll-out plans, and so on, provided further details and strengthened analytical validity by allowing for the triangulation of the mixture of data collected. 26 The data collection in hospitals was conducted at three different moments in time: shortly before (T1) and after (T2) the implementation of the CPOE/CDS systems, and at least a year thereafter (T3). As sites A and B had implemented their systems before the start of the project, no T1 data were collected. All interviews were audio-recorded and professionally transcribed.
Data analysis
Data analysis was carried out in two stages. The first stage involved inductive analysis. Multiple researchers (A.K., H.M., K.C., L.L., V.W., and Z.M.) reviewed the rich body of ethnographic materials to identify recurring themes across sites.29,30 Optimization emerged as a recurrent feature, explicitly flagged by many respondents, predominantly in T2 and T3. Optimization-related interview data were extracted by V.W. for sites D and E and by other colleagues for sites A–C. For the second stage of data analysis, the optimization theme was revisited in more detail by a single researcher (V.W.). Qualitative data coding in this stage was carried out with the aid of NVivo (version 10). In this stage, we followed a deductive approach, informed by our analysis of CPOE/CDS systems as new components that are being embedded into existing hospital information infrastructures. 24 Applying a grounded theoretical approach, 31 open-ended coding of the combined data set distinguished diverse efforts pursued in hospitals to improve the commencement and use of CPOE/CDS systems following initial implementation. In the second step, relationships between these open-ended codes were discussed, and codes were grouped into emerging categories. Throughout this process, discussions within the research team explored convergences and differentiations in the categorization process. Feedback from non-academic members of the team, including healthcare professionals and patient representatives, also contributed to iteratively shaping the systematic analysis.
The analysis was informed by a review of literature on IT maintenance taxonomies and customization of organization-spanning information systems in other sectors.32–35 However, the relevance of this literature was limited by its narrow focus on technical aspects of maintenance32,34 and/or on the managerial concerns of IT departments.33,35 These limitations stem from study designs restricted in range and duration, revolving largely around interviews in IT departments immediately following implementation and database records of change requests which only indirectly address users. In contrast, guided by our BoAP perspective, our longitudinal qualitative study of those directly involved in using CPOE/CDS systems had captured a substantial body of evidence about rather different kinds of optimization activity. This comprises the wide range of activities undertaken by users to get the CPOE/CDS systems to work and to support the efficiency and effectiveness of everyday clinical practices. 36 This use of the term optimization appears to have derived from studies which identified similar kinds of activities around the implementation and use of packaged enterprise resource planning solutions.12,22,34,37,38
Results
We developed a systematic analysis of system optimization activities (see Table 2). We note that categories are not mutually exclusive. An optimization activity can contain components that fit in more than one category.
Systematic analysis of system optimization.
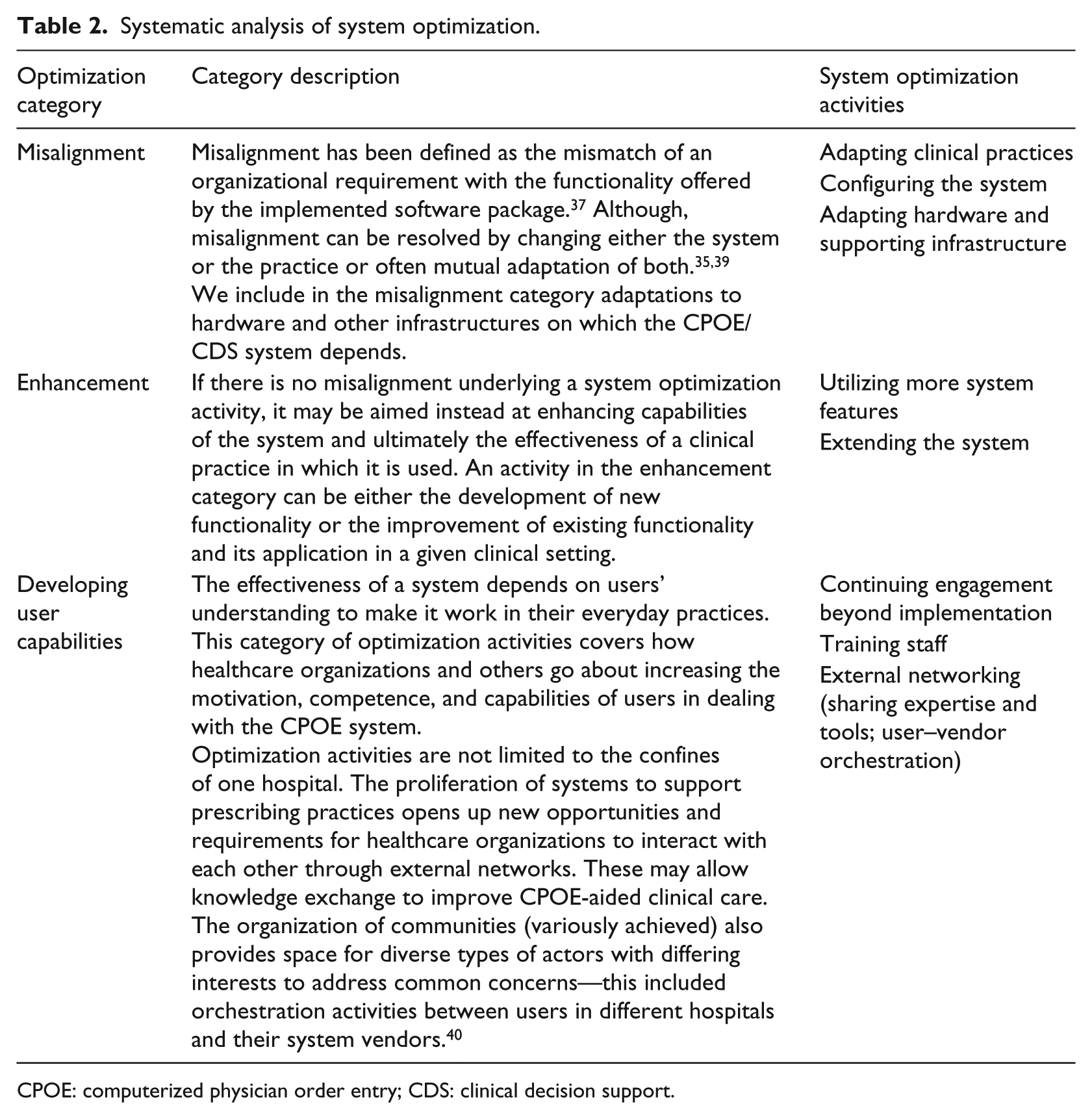
CPOE: computerized physician order entry; CDS: clinical decision support.
Table 3 includes quotes from respondents illustrating these issues. These are cited in the text as quotes 1–12.
Interview quotes from study participants.
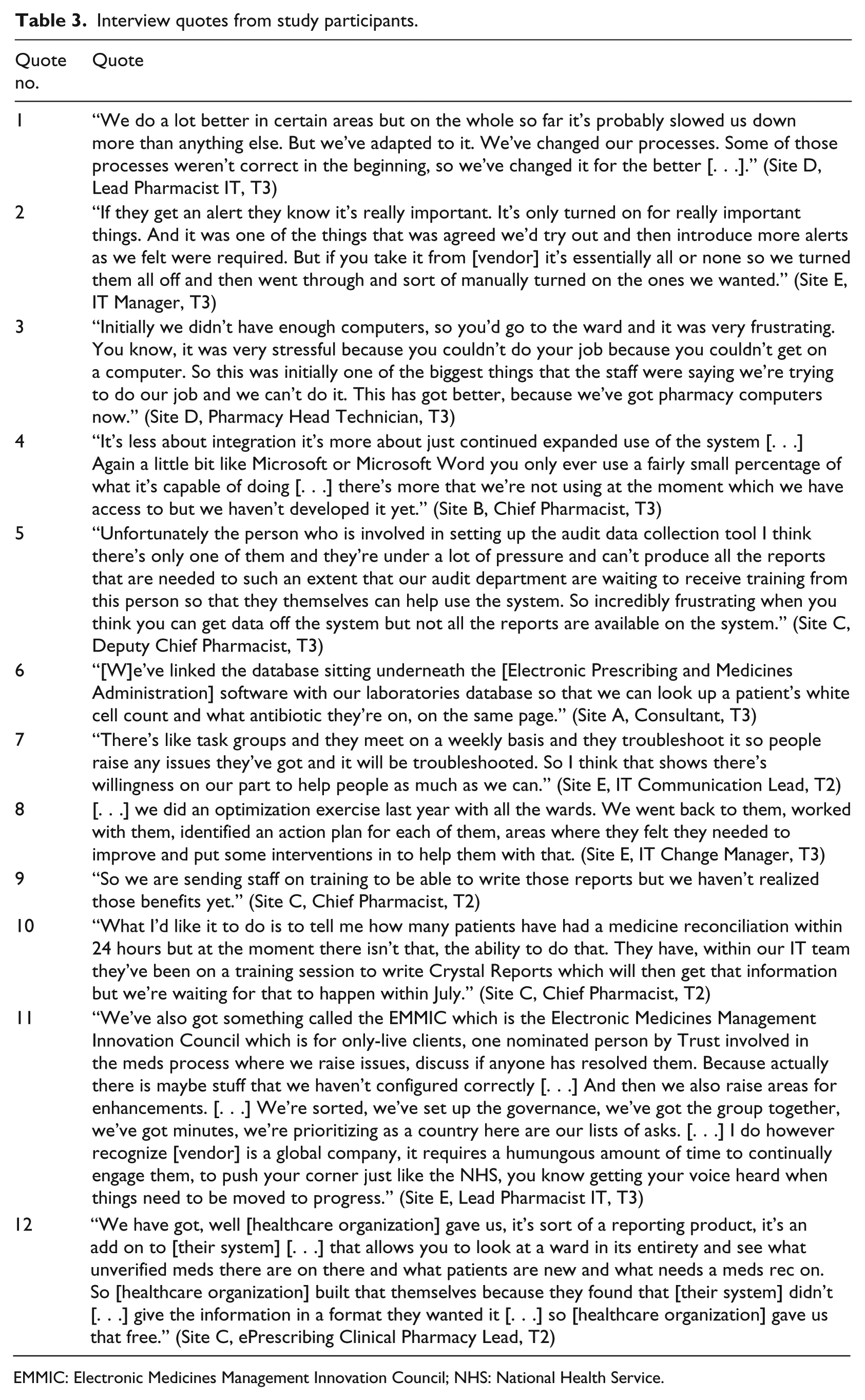
EMMIC: Electronic Medicines Management Innovation Council; NHS: National Health Service.
Misalignment
Adapting clinical practices
Adaptations and improvement to work practices are often deliberate goals of technology implementations. 40 Implementing new systems may prompt organizations to reflect upon taken-for-granted practices. Some adopters of a CPOE/CDS system took the deployment as an opportunity to optimize their clinical processes (see quote 1). This adaptation is seen as an ongoing process (post-implementation) as new features are turned-on or implemented.
Configuring the system
Instead of adjusting clinical practices, users can choose to (re)configure components of an installed system to meet local needs. Generic vendor solutions may cater for a range of industry practices through libraries of common processes. These can be made available to the user organization in the package configuration process without needing to adapt code. 41 Solutions may also include user-configurable components including, for example, the clinical decision support embedded in advanced CPOE systems. Decision support can take the form of alerts that pop-up in the course of an interaction of a prescriber with the system. Although a CPOE system comes with a default set of alerts and rules defining their behavior, pop-up alerts and rules can be configured freely by users at various points of time (see quote 2). We have observed many cases in which alerts were gradually configured and activated post-implementation.
Configurability of given functionality enables users to find various ways to address a problem. Pop-up alerts are designed to prohibit undesired prescription decisions. However, one hospital diverged from strict implementation of alert rules: some alerts were activated for a limited period for educational goals and to counter the phenomenon of alert fatigue. However, as current products offer only limited configurability, users will continue to rely on ongoing support from suppliers to increase the extent of system configurability over time.
Adapting hardware and supporting infrastructure
Although careful requirements analysis and procurement may reduce practical misalignments, these occur frequently as requirements are more effectively discovered and may evolve in the course of system use. Another issue that often proved difficult to anticipate concerned the need to upgrade the hardware and related supporting infrastructure (e.g. Wi-Fi connections). The insufficient number of available computers in particular can become a bottleneck when initial estimates of computer use are too conservative (see quote 3).
Inadequate physical infrastructure including lack of computers or Wi-Fi connectivity was an important factor hampering early uses of these systems. Some issues are relatively easy to resolve, whereas others, for example, structural changes to operating theaters, could require substantial financial commitments or incur unacceptable disruption to clinical operations.
Enhancement
Utilizing more system functionality
Some functionality may remain deactivated or underutilized following implementation. Reasons can be varied, including, for instance, the need for prior organizational adaptations, the lack of capacity or knowledge to support the function, and internal policy. In general, activation of further functionality is a gradual learning process (throughout and post-implementation) as this comparison with a common word processor illustrates (see quote 4).
Discussion of utilization frequently revolved around secondary use of data and the production of reports (the most frequent topic arising, accounting for about a quarter of all observations). The large amounts of transactional data generated by CPOE/CDS systems provide valuable opportunities for further analysis. 42 However, limited configurability, especially in stand-alone solutions, and lack of staff with expertise/training in analyzing data and generating reports (see also sub-category “Training staff”) remain obstacles to realizing anticipated benefits (see quote 5).
Extending the system
Current generic CPOE systems are limited in their ability to cater for the diversity of information requirements a hospital might have. 12 Code upgrades from suppliers may occasionally extend existing functionality or introduce new features. However, health professionals may call for special data or functions that are not built into a generic system. In these cases, hospitals may seek to extend the system themselves (where this is supported by the package), for example, by developing new input forms, amending existing ones, or linking up their systems with other applications via interfaces (see quote 6). Such system extensions are common months and years after go-live.
Developing user capabilities
Continuing engagement beyond implementation
Implementing healthcare organizations continue to actively engage with user concerns beyond the initial implementation stage. 21 This may arise through the reactive responsiveness of support staff in the IT department or pharmacy to problems raised by users in the wards (see quote 7). In other instances, more proactive initiatives focused on multiple wards can be helpful to sort out issues that accumulated over time (see quote 8).
External organizations also continue to engage with hospitals after implementation. Besides code upgrades, which can involve major changes to underlying data structures, vendors offer updates or patches to improve or correct errors in the installed software. Other organizations supplying drug and other databases may also provide regular updates to react to changing circumstances including changing demands or regulations.
Training staff
Although staff were trained in using the software ahead of implementation, some functionality required specialist knowledge and capabilities not covered in initial training. Some skills shortages emerge only post-implementation when proficiency in the use of the system increases. 17 For instance, the reporting function—key to the secondary use of data and one of the most anticipated benefits of CPOE/CDS systems from a managerial view point—turned out to require additional, often missing expertise to produce desired reports (see quote 9). One system required training in the use of third-party software to access and prepare data for further analysis (see quote 10).
External networking organizations sought to benefit from the experiences of other users. In the United Kingdom, hospitals operate in a non-competitive environment and, thus, are not constrained, for example, by commercial secrecy from sharing knowledge and tools with other hospitals to improve the quality of clinical health services nationwide (see quote 12). As a result, many forms of collaboration and knowledge sharing are formed during implementation and use of digital applications. Various fora emerged allowing adopters to discuss developmental issues and co-ordinate joint strategies to leverage their demands in dealings with the vendor 43 (see quote 11). Unifying the user voice could equally help the vendor steer product development by reducing divergences among change requests among their diverse customers.
Temporal distribution of optimization activities
Our methodology, of extracting references to optimization activity from a corpus of ethnographic material, provides some indirect evidence about the temporal distribution of this activity (though as the volume of ethnographic material and the granularity of extraction are not constant between phases, they cannot be statistically analyzed and patterns can only be seen as indicative). References to optimization grew from 12 in the pre-implementation phase (T1), to 61 in the 4–6 months after implementation (T2), to 95 in 18 months or more after implementation (T3) (see Table 4). Optimization processes thus reach their peak well after implementation. One consequence of the protracted challenges involved in implementing these complex systems and getting them to work21,39 is that optimization efforts are still continuing even as late as 4–5 years after go-live (observed in sites A and B, respectively). This points to an ongoing effort to better utilize the functionality offered by these extremely complex packages. The ways in which such packages may be productively applied within particular organizational settings and to a wide range of healthcare activities are not fully apparent a priori but are clarified in practice. Salient improvement activities in T3 included enhancement activities (e.g. implementation of complex prescribing and decision support, as well as developments in work practices). Indeed, the single most frequent activity observed (in T3 and throughout) involved developing reporting/the secondary use of data (44 from a total of 168 activities identified). There were a further 12 references to acquiring the skills/training needed to undertake such secondary use of data. Ongoing efforts to develop user organization capability to exploit systems were salient. In some sites this involved external knowledge networking activities with other sites and with vendors.
Temporal distribution of references to optimization activities.

Discussion
All hospitals were found to engage in a variety of ongoing system optimization activities to improve clinical care using CPOE/CDS systems. These findings confirm the notion that the implementation of a new CPOE/CDS system is a protracted learning journey that calls for change management activity and strategy to be extended well beyond the immediate post-implementation period and immediate concerns therein. As well as attempts to enhance systems and align them with organization practices, we also identified efforts to improve the organizations’ capacity to deal with these activities, notably through training and external networking.
Strengths and limitations
The longitudinal, qualitative approach, as guided by the BoAP perspective, 24 enabled systematic in-depth investigation of the hitherto underexplored post-implementation system optimization activities of CPOE/CDS systems. Our analysis of system optimization activities can be helpful in informing long-term-oriented HIT strategy processes within and beyond the field of CPOE/CDS systems. Implementers of other HIT with similar qualities in scope and scale to these multi-user, modular, organization-spanning systems can draw on our findings to inform their implementation strategies.
Our fieldwork addressed implementation processes across multiple sites over an extended period. The 207 interviews undertaken only represent a minute (and potentially un-representative) sample of the thousands employed in the five participating hospitals. The study therefore did not allow us to follow-up and track the development of particular changes in software and work practices in particular contexts over time. The relatively small number of CPOE/CDS implementations studied limited the range of observable system optimization activities. However, retrospective examination of a large corpus of collected ethnographic material provided a rich pool of insights into questions that had not been posed at the outset of the National Institute for Health Research (NIHR) investigation. Systematic secondary analysis of large-scale ethnographic resources can thus provide an evidence base for analytical generalizations that may have wider applicability. 44 As supplier offerings mature43,45 and other applications enter the market,12,16 the foci of optimization activities may shift from adapting systems to existing practices toward addressing new challenges. As well as further development of systems and work practices, this may take the form of developing user organization capabilities (e.g. through training and participating in knowledge networks).
Interpretation of findings in the context of the wider literature
The literature indicates that post-go-live system optimization activities are common and even necessary to maximize benefit realization.15,20,21,43,46,36 Our study sheds light on the wide range and extended duration (up to 5 years) post-implementation of optimization activities in hospitals. Implementation is only the beginning of a learning journey in which users learn about and adapt to the system as they discover its characteristics in use. 17 With greater experience of CPOE/CDS and similar systems, health professionals will improve their capability and confidence to overcome shortcomings, optimize or enhance existing technical capabilities. User and system behaviors are thus expected to evolve over time, and this needs to be captured in management strategy.
Previously, deviations from anticipated implementation outcomes came as a surprise to adopters, and the main strategies suggested for dealing with unintended consequences were either to avoid or to accept them.47,48 This is in line with a traditional, episodic understanding of systems implementation which emphasizes taking preventive measures prior to or during the implementation. 21 However, such strategies fail to explore the scope for long-term proactive strategies to contribute to shaping the further evolution of systems and practices. 49 In contrast, our results support an evolutionary understanding of technologies in which CPOE/CDS systems are regarded as new components in evolving hospital information infrastructures. 21 Accordingly, system optimization must be anticipated and can be planned for—as new components need to be actively fitted into a hospital’s idiosyncratic assemblage of historically specific local practices, organizational cultures, and technological infrastructures.
Previous systematic studies of post-implementation activities have mainly emphasized technical aspects or a managerial perspective.32–35 In contrast, our study of HIT takes a user point of view and stresses the variety of optimization activities that are important for those directly involved with the new technology. We found supporting evidence for established taxonomical categories. We also identified efforts to improve optimization capabilities (knowledge sharing and networking beyond the hospital) as an emerging category. Although this kind of knowledge sharing between user organizations may also occur in the commercial sector, it may be facilitated (and perhaps may also be more readily observed) in the non-competitive healthcare sector.
Implications for policy, practice, and research
Implementation strategies should be long-term-oriented and incorporate considerations for system optimization to address on-going and emerging concerns over a much longer timeframe than anticipated by existing episodic perspectives. 9 The short-term duration of many investments in this field has come into conflict with the long-term development of use and optimization activities, well beyond initial implementation. We therefore stress the need to allocate on-going financial resources and managerial effort to the post-implementation phase, coupled with the need to extend engagement 21 and sustain implementation support team structures to retain and re-use the internal experience and expertise acquired by team members in the course of the implementation journey. These can serve as facilitators for continued system optimization activities and points of contact for other users. Research suggests that taking into account long-term considerations may allow for an overall smoother and quicker implementation and acceptance process. 21
Governments and relevant regulatory bodies may need to take a stronger role in guiding further development of national standards and providing central resources. Policies should move beyond focusing narrowly on procuring novel HIT solutions and instead engage with long-term considerations of how to most effectively exploit these systems to optimize care delivery processes. In this regard, our findings reinforce recent proposals for a long-term deployment strategy for HIT suggested for National Health Service (NHS) Scotland, which has recently decided to roll out CPOE/CDS systems. 50 A similarly phased approach has been proposed to NHS England by the Wachter Review. 4 These include the suggestion to enhance information and experience exchange, for example, by pairing early and later adopter hospitals to ensure that learning from experience carries over to other hospitals, reducing time needed to realize benefits and enhance safety. In contexts where there is no central body, healthcare organizations should foster the creation of such shared spaces themselves. This might involve planned knowledge transfer activities (such as the learning networks currently being established by NHS England) and informal networks emerging among specialist communities, facilitated by social media. Vendors and users are also getting involved in initiatives to create and expand “user groups” through virtual and face-to-face meeting. We anticipate the emergence of multiple webs of relationships between different entities to exchange the knowledge and resources needed to optimize processes.
Conclusion
The deployment and adoption of CPOE/CDS systems is a protracted learning process. Hospitals engage in a wide range of activities to optimize the fit between the implemented system and its clinical setting. Our systematic analysis has highlighted the range of system optimization activities in the post-implementation period including resolving misalignments, enhancing the implemented system, as well as various efforts to develop user capability for further optimization. Here, our analysis flags growing secondary use of data (which called for training in generating reports) and also points to the formation of wider knowledge networks. System optimization is thus a continuation of the learning process that starts during implementation and in which responsibility shifts largely to the adopter organization to ensure sustained, efficient use of the system and to gradually increase benefit realization over time. Our results indicate that short-term HIT implementation strategies and related policies are unlikely to realize the full benefits promised by CPOE/CDS systems. Long-term strategies are required, including provision of sufficient support and resources, to allow for successful optimization.
Footnotes
Acknowledgements
We gratefully acknowledge the input from our Independent Programme Steering Committee, which is chaired by Prof. Denis Protti and has Prof. Sir Munir Pirmohamed, Prof. Bryony Dean Franklin, Ms Eva Leach, Ms Rosemary Humphreys, and Ms Ailsa Donnelly as members. We also gratefully acknowledge the input of Rosemary Porteous, who transcribed the interviews. We are very grateful to former research associates, Dr Lisa Lee and Dr Zoe Morrison, whose earlier fieldwork added to the corpus of empirical evidence. Members of the Programme Team are as follows: Dr Ann Robertson, Prof. Jill Schofield, Dr Jamie Coleman, Ms Ann Slee, Prof. David Bates, Dr Zoe Morrison, Mr Alan Girling, Mr Antony Chuter, Dr Laurence Blake, Prof. Anthony Avery, Prof. Richard Lilford, Dr Sarah Slight, Dr Behnaz Schofield, Ms Sonal Shah, Ms Ndeshi Salema, Mr Sam Watson, and Dr Lucy McCloughan.
Author contributions
A.S. and R.W. conceived this work. V.W., H.M., A.K., and K.C. collected data for this study. V.W. initiated and led data analysis and drafting of the manuscript with inputs from H.M. and R.W. All authors have commented on various versions of this manuscript and contributed to the analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article has drawn on a program of independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-1209-10099). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health. K.C. was supported by a Chief Scientist Office of the Scottish Government Postdoctoral Fellowship.