
Abstract
In this article, we examine three cases of e-health solutions for patients in Norway. For the analysis of the three cases, we focused on friction forces that come into play when different established arrangements need to change to accommodate novelty. We argue that the design of new technologies was shaped by friction related to institutionalised practices, regulatory regimes and entrenched patient roles. These friction forces connect the past with the present, come into action when aiming for novelty and result to the perpetuation of constituents of the past during change processes. Specifically, the e-health solutions under study were strongly influenced by established healthcare provision logics. All three initiatives expanded the healthcare information infrastructure towards the patients with as little disruption to established arrangements as possible.
Introduction
In current e-health research, there is considerable discussion on leveraging information systems to shift healthcare towards patient-centredness. In the medical domain, patient-centredness is a model of care that entails keeping patients informed, involving them in decisions and self-care management activities, and acknowledging their experience of illness and psychosocial context.1–4 Accordingly, patient-centred care indicates a shift towards seeing the patient as an integral part of the care team, giving responsibilities of self-care and monitoring to patients and ensuring personalisation of care treatment and care paths.
However, when it comes to putting in place e-health solutions for patient-centredness, there is no clear model for the functionality to offer. As a principle, designing e-health solutions for patient-centredness entails providing information and communication tools for both patients (that need to be enabled to contribute meaningfully in decision-taking) and providers (that need to get better insight on patient circumstances). Hence, solutions related to communications, information sharing and distributed data management are needed in order to facilitate a redistribution of tasks and new types of collaboration and coordination between actors. 5 These novel solutions are transforming the current healthcare information infrastructure that was historically shaped by established logics based on the communication and information needs of health providers.
In this perspective, the introduction of patient-centred e-health solutions can be seen as an attempt to shift current healthcare information infrastructures, from being provider-oriented and institution-centric, towards a balance between the information and communication needs of patients and those of healthcare professionals, supporting care provision that is respectful of patient preferences, needs and values. 6 This shift entails questioning and changing the ways in which patients, healthcare providers and health technologies co-constitute each other. 7 In addition, it entails intervening into how health information infrastructures support the practices of diverse communities that accrete around them. 8 Such interventions are complex, challenging and can lead to unexpected outcomes. Specifically, in this article, we examine how the relational nature of infrastructures shapes the process of putting in place e-health solutions for patient-centredness.
In the following sections, we analyse three different cases with the aim to advance our understanding of infrastructure interventions for patient-centredness. For our examination, we build upon prior research on change as a continuous process that addresses the relation between past and present in innovation.9,10 To understand change processes, this prior research proposed the concept of friction as an alternative to the concept of inertia. While inertia is linked to inaction and connotes an indisposition to motion or change, friction shifts attention to forces created through the interaction of different established arrangements that need to change in relation to each other. This relational focus is in line with the information infrastructure perspective. Accordingly, our aim is to understand how infrastructure interventions for patient-centredness take place and what is the role of friction forces. Therefore, we formulate the following research question ‘how are e-health initiatives that aim for patient-centredness being shaped by friction forces?’.
Based on the analysis of three case studies, our findings show that designing e-health around patient needs is shaped by friction forces leading to processes of negotiations and trade-offs between past arrangements and novelty. Furthermore, our findings also show that friction forces lead to the perpetuation of constituents of the past during change processes. In the cases considered in this study, the resulting solutions bring as little disruption to established arrangements as possible as established logics endure during infrastructure transformation. Overall, by bringing friction forces in focus, our study contributes to insights into how e-health solutions for patient-centredness find a fine balance between (a) introducing new orientations in care and (b) reproducing established healthcare arrangements.
The remainder of the article is structured as follows: first, we describe the theoretical background and the concept of friction. We then present the background of the cases studied and the method used to collect empirical data, subsequently, we present our findings, and finally, we conclude by discussing insights from our findings and relations to prior research.
Theoretical background
In general, the term infrastructure implies a focus on underlying structural supports which enable action, create connections and have durability. 11 Infrastructures are relational because they ‘work in between’ meaning different things to different groups that share infrastructures in their everyday practices. Infrastructures are also ecological because they are part of, made of and inseparable from actions, tools and their environment. 12 Accordingly, infrastructures are always a social and political matter as much as a technical one. However, the everyday experience of infrastructures is not about ongoing deliberations, but rather about boring background arrangements operating smoothly unless breakdowns happen. Studying the work of infrastructuring means attending to issues of maintenance and repair, and approaching infrastructures not as stabilised interlinked structures, but rather as continuous processes. Such a process view exposes how an information infrastructure comes into existence in relation to organised ‘technical, material and knowledge interventions’ and through ‘infrastructural work’. 8 This view implies shifting the emphasis from changes in infrastructural components to changes in infrastructural relations by unfolding the political, ethical and social choices made throughout infrastructure development. 13
In their inquiry into why and how technological systems are so often difficult to change, Håkansson and Waluszewski observed how different established arrangements often seem to be ‘cemented’ upon each other impeding alterations and novelty, and yet, these cemented arrangements do transform through interaction. 9 They conceptualise friction as an ‘active force’ of interaction, causing changes in existing arrangements, with a strong tendency to favour existing (i.e. historical) values due to their accumulated weight – or ‘economic heaviness’.9,10 Hence, friction is a peculiar relational force that can appear both as a stabiliser and a de-stabiliser during change processes. 9 We investigated the shaping of e-health initiatives for patient-centredness by viewing them as infrastructuring processes shaped by friction.
Cases background and method
We conducted three qualitative case studies (Table 1) of design and implementation activities for three separate e-health initiatives in Norway throughout the 2012–2015 period. The case studies are part of a large research project on the interplay between new information technologies and existing systems and modes of organising. For all three cases, data collection was confined to the design activities. We did not have access to use data after solutions’ launch.
Overview of the three case studies.
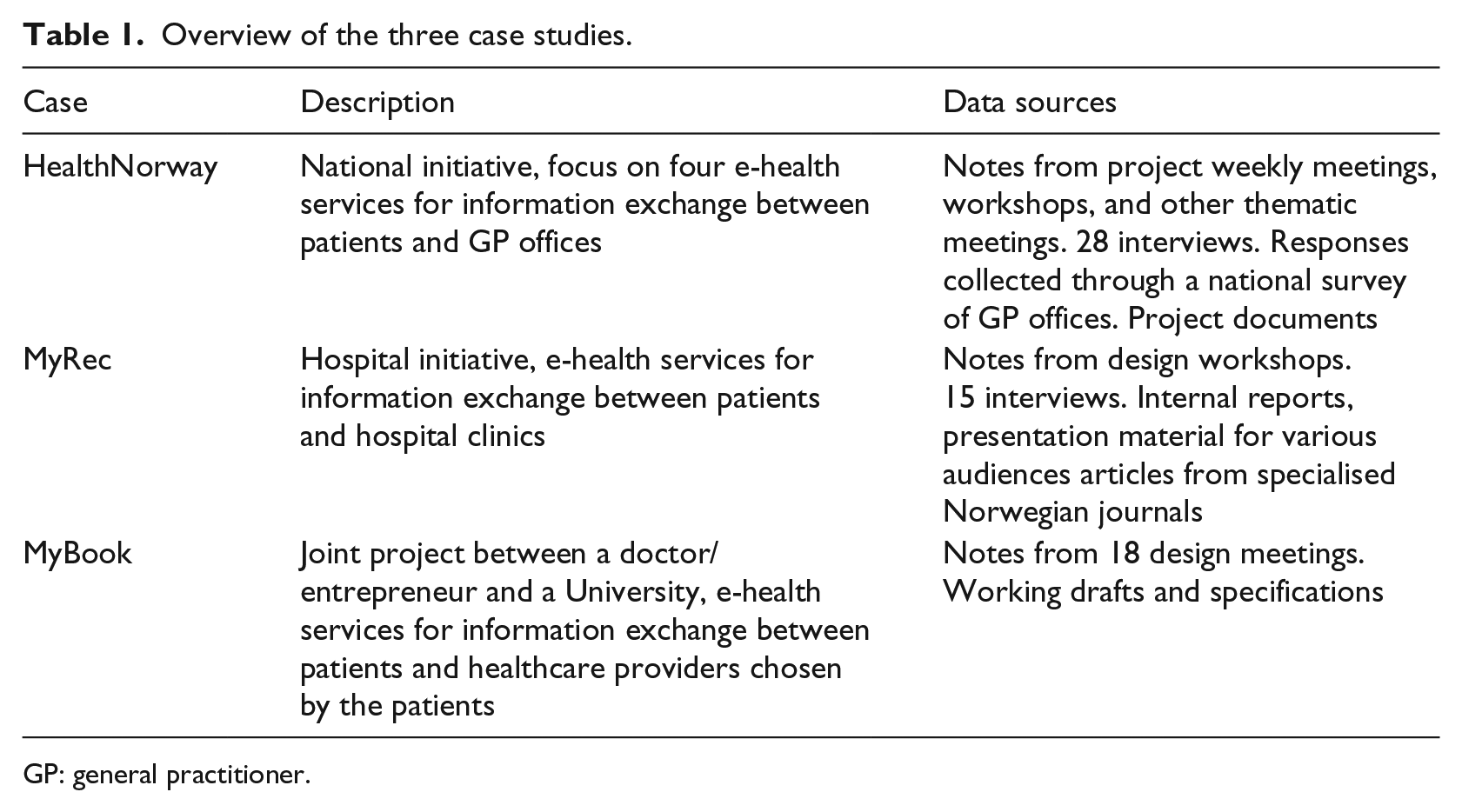
GP: general practitioner.
The first case concerns the design of novel services upon the national e-health platform, which citizens can access over the Internet (HealthNorway). A key aim for this initiative was to facilitate patients to assume a more active role in their own healthcare by providing more expedient means for interacting with healthcare providers. The platform was launched in June 2011 by offering quality assured information on medical conditions, treatments and healthy living. Then, in August 2013, a service for accessing personalised information (such as vaccination and e-prescription information) was launched. Since 2013, four key patient-oriented interactive electronic services are being designed and developed (in early 2017 about to transition from pilot to roll-out status). These four services support information sharing between patients and general practitioners’ (GPs) offices and are the focus of this article. The four services are booking of appointments, renewal of prescriptions, electronic contact for administrative purposes and e-consultation. While collecting data on the case, we attended project weekly meetings, workshops and other thematic meetings where we took detailed notes. We also conducted interviews (28 in total) with members of the project team. Additionally, we analysed the replies collected through a national survey of GP offices. Finally, we reviewed meeting documents, presentation slides and project reports as we have been granted access to project documents.
The second case concerns a hospital-based, patient-oriented web portal named MyRec. The first functionality within MyRec was launched in 2006 and the portal has since been under continuous development and expansion. It offers general functionalities such as secure email with clinical personnel, access to selected Electronic Patient Record (EPR) documents (e.g. discharge letters) and tailored functionalities for specific departments and patient groups including a functionality for notifying hospital clinics for the need to change an appointment and functionalities for data exchange between chronic patients and clinics. Hence, the users of MyRec are both patients and healthcare practitioners. Data collection for this case entailed interviews with hospital personnel (15 interviews in total), observation sessions during design workshops and document analysis (internal reports, presentation material for various audiences, policy documents, laws and articles from specialised press).
The third case concerns a small local project named MyBook. This was initiated by a doctor who identified the opportunity to create a solution for information sharing between patients and healthcare providers. MyBook allows patients to assume a central role in information management for their own health and provides a solution to a practical problem. The practical problem relates to the slowness of existing mechanisms for communication among healthcare providers in Norway. If a patient is discharged from a hospital on one day and has to consult a GP the next day, the discharge report will not have reached the GP. Furthermore, the mechanism is too restrictive: reports are sent only to the doctor who referred the patient; other relevant care providers do not receive them. The solution conceptualised was named MyBook. MyBook is an e-health application that supports patients to create digital copies of documents received after a care event and upload them in a central database from where healthcare professionals could access them. The information-handling approach proposed by MyBook brings the patients in the process and relies on their work to collect and share information. A joint project (between the University and the doctor/entrepreneur) was defined with the aim to deliver a prototype. We followed this project collecting data from 18 design meetings and reviewing documents including working drafts and specifications.
Our research is within the interpretive tradition in information systems research14,15 and we have taken a process approach to examine how ‘things change over time’. 16 In particular, our analysis was focused on taking stock of how functionality was influenced by friction forces between different established arrangements. The three cases allowed us to follow design processes of patient-centred solutions and to investigate the sequence of events that led to the specific functionalities offered. Our interest was focused on the friction forces that came into play when the features of the solutions were being decided. The cases studied relate to initiatives that stem from different levels within the same healthcare system (a national initiative, a hospital initiative, an initiative that was started by a practitioner) and illuminate different types of frictions. Hence, the cross-analysis of the three cases can provide insights on how e-health initiatives that aim for patient-centredness are being shaped by friction forces at different levels.
Findings
Frictions related to GP office established arrangements
The HealthNorway team in charge of the design of the four national electronic services distributed a questionnaire to all GP offices in Norway at the end of 2013 (completed questionnaires received by February 2014). Among other questions, doctors and secretaries working in the GP offices were asked to articulate (in free text format) perceived benefits and disadvantages/issues of web-enabled interaction with patients. There were 369 relevant answers (on benefits and disadvantages/issues) received from 230 distinct GP offices (approximately 15% of the total GP offices in Norway). Out of the 369 completed answers, 219 were submitted by doctors while the remaining were submitted by secretarial staff.
More than 80 per cent of both doctors and secretaries noted potential benefits. These benefits are linked mostly to the effects of introducing asynchronous modes of communication with patients. 17 Specifically, the expected benefits relate to both improvements for work organisation within GP offices (freeing time from answering/returning phone calls, less stressed secretarial personnel, less traffic due to less patients coming to the office to book appointments, improved documentation of patients’ contacts) and improvements of service quality (doctors being more accessible, service not linked to opening hours, less frustrated patients).
Although there were no significant differences between doctors and secretaries on the expected benefits, their perceptions differed on potential disadvantages/issues (Table 2). Secretaries were less inclined towards writing about issues than doctors (51% of Secretarial Personnel noted issues vs 71% of GPs). Secretarial personnel mostly worry about the need for lots of ‘back and forth’ due to insufficient information. Doctors mostly worry about the increase of demand.
Perceived issues in electronic information exchange between patients and healthcare providers.
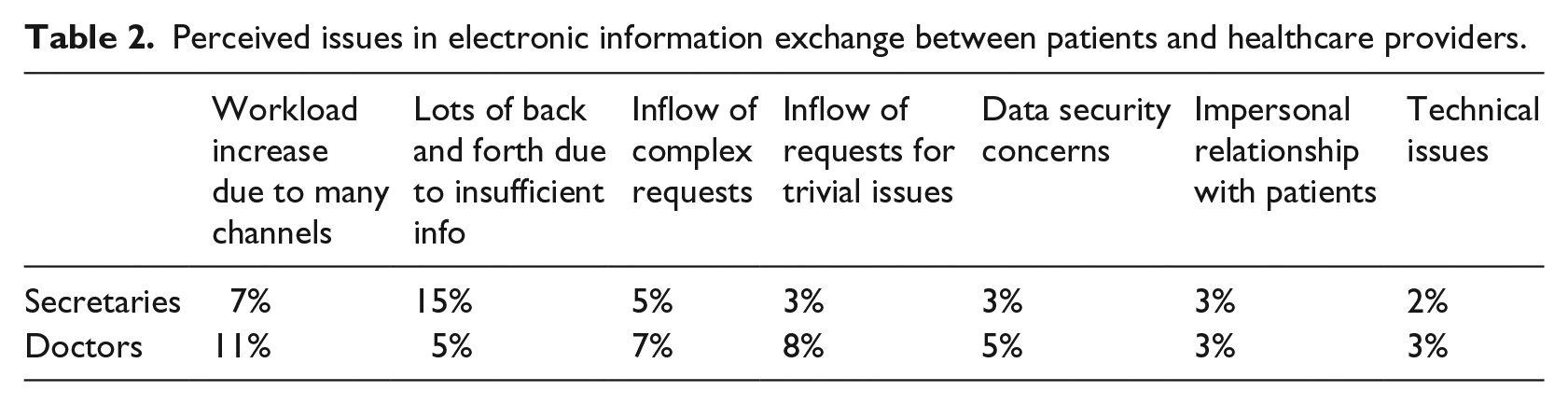
GPs and secretarial personnel seem to worry about specific types of potential patient behaviour. In the free text replies, we found references to specific types that we classified under three categories. The ‘demanding patient’ may expect immediate replies or ask trivial questions on things that can be found out without healthcare providers’ involvement. The ‘difficult patient’ may write very long and very frequent messages or may ask ‘too often’ for an appointment. The ‘non-competent patient’ may not be able to formulate requests in a concrete way or may not be able to provide information about current health status and medications used.
The responses to the survey illustrate how the introduction of e-health services seems unchartered territory for professionals. They are overall positively disposed but they also have concerns related to the impact of the new services to the existing work practices. Their concerns created friction with the overall intentions of the design team to offer patients more ‘control’ similarly to other domains (e.g. booking hotels and flights). The four e-health services designed and developed aim to be widely adopted by GP offices around the country so there was a clear need to configure them in a way that would not alienate professionals while pursuing enough novelty to set the ground for future advancements. In other words, the novel functionalities were shaped by the aim to minimise disruptions while maximising the perceived benefits of institutional actors.
For instance, the technological solution developed made it possible to offer a view into the GP’s calendar so that the patients could see the availability of slots and directly select and book one of the empty slots. However, this was not offered as standard functionality. It was up to the individual GP office to decide whether they wished to offer their patients this kind of access. The implemented solution can support both an interaction model close to the current one (with GP offices having full control over the calendar) and a model which is closer to the self-service paradigm (from banking and the travel industry) and requires significant changes in GP office practices.
Frictions related to regulatory arrangements
The design and development for the e-health initiative examined as a second case (MyRec) started within the IT department of a major Norwegian hospital. 18 As the initiative started from within the hospital, the MyRec team members had good access to clinicians and patient representatives and started working closely with them both to elicit requirements and to stimulate their interest. Starting from general ideas, the design team sketched out and experimented with multiple possibilities. In the initial version of the solution, on the main screen a right and a left set of icons used to appear. The icons on the left side were related to a set of services for which the hospital would be responsible (as for example access to information from clinical systems). The icons on the right were related to another set of services for which patients would be responsible (as for example a personally maintained medication list and a personal diary).
Some services proved to be very successful. A service that quickly took off offered functionality for online appointments change. This service solved the problem of lengthy waiting times for patients calling the hospital during peak hours. Also, services aiming to support patient groups living with chronic conditions were well received. In such cases, patients need to report information on a regular basis over long periods, monitoring their own health status and informing clinicians. Nevertheless, eventually some of the initially conceptualised services had to be abandoned. For instance, a functionality that allowed patients to keep a personal diary online had to be removed. This was because the envisioned patient ownership of the information collided with the regulations that stipulate that all personal health data treatment in hospital systems has to be closely monitored by the hospital’s privacy ombudsman.
Overall, e-health services that could enable patients to register their own private information without necessarily sharing it with healthcare professionals collided with regulations about hospital systems. As MyRec kept evolving, the categorisation of services in two distinct groups (left and right sides of the screen indicating hospital vs patient responsibility) was eventually abandoned. Since MyRec is a hospital-based system, the responsibility for the whole of it lies with the hospital so the two sides could be confusing. Although the health strategy documents instruct hospitals to include patients more actively, this created frictions with the existing regulations related to health-related data repositories that are not always congruent with such a vision. Hence, it was tricky to accommodate in a hospital-based system novel e-health services inspired by Web 2.0 such as keeping personal health diaries and engaging with patient groups without the intermediation of healthcare personnel.
Frictions related to reconciling patient needs to medical practices
In the early stages of the MyBook joint project (between the University and the doctor/entrepreneur), a design and development team worked closely with the doctor who initiated it to further elaborate the idea and develop concrete functionalities. The functionalities developed support patients to (a) digitise and tag paper copies from their records received after a care event (by scanning or photographing), (b) upload in a central database and (c) manage access rights to a personal data ‘folder’ in the central database. According to the doctor’s idea the documents uploaded would be categorised in five fixed document categories: record extracts, blood tests, medical images, medication and ‘other’.
After the functionality was defined, a demo was presented in a workshop with patients where the desirability for such a solution was discussed together with functionality options and opinions regarding security and privacy. The patients expressed wishes for specific additional functionalities such for note keeping (on health events or questions for the next appointment with a doctor). Also, they wanted to be able to register data and display them in a graph. Additionally, they expressed the wish to selectively share single documents rather than opening up access to the whole folder which includes everything uploaded.
The doctor/entrepreneur, for whom simplicity was an overall design goal, maintained that a minimal functionality should be pursued. A persona often mobilised by the doctor in the discussions was ‘Aunt Olga’. She was 80 years old and had several conditions that made her need health services from different providers frequently. She was not very into technology, she was expected to have a mobile phone with which she could call, take pictures and access the Internet. The doctor used this persona and made clear that this was the type of patient to be supported by the new solution. A functional prototype for iOS (iPhone) and a web interface to a secure database were developed. The prototype included only the functionality initially specified with the fixed five document categories (that could not be altered by patients) and no additional support for personal notes or graphics. Thus, the potential for the solution to deliver support both for doctors (that needed access to documentation produced after care events) and for patients (that needed a way to complement the information generated from within the healthcare system with their own notes and other data) was downplayed. The role of MyBook was confined to being a remedial addition to the existing healthcare information infrastructure: new means to carry information between health providers but without enriching this information. The patient, however, could decide for how long the ‘book’ was to be shared and with which healthcare provider and was in control of generating and distributing the access code required. In addition, the patient could see whether the provider actually had used the access right granted or not and could revoke or renew (extend) the access.
Following this case, we find that the new solution rendered patients as mere ‘carriers’ of information rather than full ‘owners’ with discretion over content and structure. Nevertheless, it should be noted that even the carrier role is novel, since patients in Norway are not responsible to carry their health data between providers. The concept of the new e-health solution circumnavigated the legal and interoperability issues that health records applications commonly face. However, it revealed numerous aspects around which there are different views between patients and healthcare personnel. This included which information types should be stored, how this information should be organised, what one should be able to do with the information (e.g. analysis functionality) and the granularity of access control. In this case, we witnessed how the e-health solution has been shaped by frictions between patient needs and established healthcare practices.
In practice, the technical realisation of the prototype left open possibilities for unintended usage and exertion of patient autonomy. For instance, initially, only image file types (jpg) are supported and no editing or annotation functionality is provided. Still, this data format is so generic that it is possible for patients to write notes or draw graphs on a paper sheet, photograph or scan this sheet and upload it. Actually, it would also be possible to photograph anything – for example, a patient could upload a photo of medication boxes rather than a textual medication list. The decision to rely on patients to upload information and the decision to use generic image files led to the development of an application that allows patients to deviate from the intended use although what is actually inscribed in functionality follows a specific healthcare provider’s view.
Discussion
Our cases show attempts to shift healthcare towards patient-centredness by designing and developing e-health solutions. Our aim is to understand how infrastructuring for patient-centredness takes place and what the role of friction forces is. Towards this aim we examined three cases at different levels within the Norwegian healthcare system (a national initiative, a hospital initiative and an initiative that was started by a GP practitioner). The concept of friction from innovation studies9,10 was used as an analytical lens orienting our attention to the confrontations between different established arrangements that need to change in relation to each other. Friction is a relational force with both stabilising and de-stabilising impact on change processes, with a strong tendency to favour existing (i.e. historical) values.
We applied the concept of friction and answered our research question by exposing how established logics endure and have a strong influence on the design of the new e-health solutions for patient-centredness. In the case of the national solution, GP office arrangements were in friction with the overall intentions of the design team to offer patients more ‘control’ (e.g. similarly to booking hotels and flights). The national solution aspires to be widely adopted by GP offices around the country so there was a clear need to configure it in a way that would not alienate practitioners while pursuing enough novelty to set the ground for future advancements. In the case of MyRec, friction emerged from the existing regulations that are aligned with a provider-centric care model. Although the national health strategy documents instruct hospitals to include patients, the regulations related to health-related data repositories are not always congruent with such a vision. Finally, in the case of MyBook, the medical logic associated with the doctor’s initial idea shaped the design process and rendered patients as mere ‘carriers’ of information rather than full ‘owners’. The healthcare providers’ views were privileged when deciding which information types should be stored, how this information should be organised and what kind of analytical functionality should be included.
Although in all three cases we observed the strong influence of established provider-centric arrangements on the new e-health solutions, we also found that the resulting functionality was indeed a step towards a more active patient role. The national solution for patient–GP office communications gives patients and citizens more control over their interaction with healthcare providers (e.g. they can use the new electronic channels at times that are convenient for them without fitting their agendas to GP office contact hours). Similarly, the hospital solution is a new entryway to the hospital and also a common space between patients and healthcare providers that supports information exchange. In the case of MyBook, patients were not only provided with new means for sharing information with health providers but also with decision rights on how long information will be shared and with which health provider.
The idea of shifting healthcare towards patient-centredness is present in policy documents but it is not detailed or specific. The shift is linked to multiple rationales (e.g. to improve the efficiency, or the quality, or the inclusiveness of health services). Furthermore, there are multiple possible modes of orienting services to the patients (viewing them as recipients/customers, co-creators or full owners of service). 19 Patient-oriented e-health initiatives are seen as opportunities to pursue innovation in healthcare services by strengthening the patients’ role. An underlying assumption in the arguments about the pivotal role of e-health initiatives for patient-centred care is that technology can be used to induce change and to disrupt the existing configuration of healthcare. Essentially, an agenda for ‘IT-led transformation’ is interweaved in the discourse about patient-centredness 20 feeding expectations for the accomplishment of swift and momentous changes. The assumption of technology accelerated change needs to be viewed in the light of our case findings: technology is not an independent factor that comes in to catalyse change processes, but rather, as technological artefacts are outcomes of design processes influenced by established logics, technology has to be studied as an interdependent part of these processes. In a sense, even when aiming to shift towards new visions and care models, we are always ‘amending’ in some way. There are always underlying arrangements that enable care work that need to be incorporated, adapted or migrated into a different way of doing things. As Huy and Mintzberg 21 point out, ‘change has to be managed with a profound appreciation of stability’.
Our findings make two contributions: first we show that infrastructuring for patient-centredness is an ongoing process of negotiations and trade-offs and that novelty in infrastructures is always a social and political matter as much as a technical one. These findings raise issues on how patients should relate to technology and health expertise. 22 Designing e-health around patient needs as proposed by advocates of patient-centred health technology 23 is not straightforward because friction forces emerge when attempting to change different established arrangements in relation to each other.
Second, our findings show that friction forces connect the past with the present, and result in the perpetuation of constituents of the past during change processes. Specifically, the e-health solutions under study were strongly influenced by established healthcare provision logics. All three initiatives resulted in expanding the healthcare information infrastructure towards the patients with as little disruption to established arrangements as possible. Hence, the e-health solutions are coming out of ‘mindful deviations’, 24 cautious steps that break away from established healthcare arrangements in a limited way. Such initiatives may not radically depart from existing healthcare models but can still be viewed as seeds for change. 25
In the cases we studied, we find actors that balance between persistence (keeping the electronic service initiatives going) and desistance and this reflects the exploratory and learning character of designing for patient-oriented services with the strategic aim of reshaping established relationships. Our three cases align with prior research on the need to reconcile the needs of clinicians with those of patients for patient-oriented e-health 26 but also, bring to surface the role of time as a resource and the need for stepwise strategies as the transformation of a complex and diverse sector such as healthcare, takes time. 20
Our article has a specific focus on infrastructures for patient-centredness facilitating patient–provider interactions. This is a relatively new domain for health informatics. Prior research on healthcare information infrastructures has mostly focused on infrastructures oriented solely to health practitioners. For instance, past research investigated hospital infrastructuring and pointed to unexpected side effects due to reflexive processes generated by complexity and to inertia caused by existing practices and technologies.27,28 Expanding research to infrastructures that need to work ‘in between’ patients and providers is critical for addressing the ongoing transformations of patient-healthcare provider relations in healthcare. 29 Our article contributes to building a body of knowledge specifically for these new types of infrastructural expansion and complements earlier research on new care models that does not cover technology aspects (e.g. research on patient-professional partnerships for chronic conditions, 30 research on patients’ information seeking behaviour 31 ).
Future research may proceed in two directions. The first direction is towards the analysis of other e-health initiatives for patient–provider communications to explore whether similar friction forces apply. This direction can lead to analytical generalisation by the comparative examination of multiple cases. A second future research direction is related to extending our research by following the three specific e-health cases in the future aiming to collect data on actual use. Our study has a focus on the design activities and we have not been able to cover use. By collecting and analysing data on use patterns and actual users’ perspectives (both patients’ and healthcare providers’), it will be possible to follow emergent and unanticipated change through actual use32,33 and examine how friction forces play out in the long run. Future transformations could be an effect of the potentialities that are opened up and that can be (but do not have to be) realised.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Norwegian Research Council (project no. 213143 and project no. 237766). We are grateful to the members of the HealthNorway, MyRec and MyBook teams who participated in the study. We would like to thank the Special Issue Editors and the anonymous reviewers for providing us with comments and suggestions that helped us improve the quality of the manuscript.