
Abstract
Objective and purpose
The purpose of this scoping review was to examine the breadth and scope of the existing literature on eHealth in older adults, with a particular focus on access, uptake, usability, and outcomes related to eHealth technologies. The review aims to map the existing evidence, identify research gaps, and from these, analyze the factors that influence eHealth literacy in older people and inform future research and interventions aimed at increasing eHealth engagement in the older population.
Methodology
A scoping review was conducted using Arksey and O’Malley's framework. Relevant peer-reviewed articles published over 10 years between 2015 and 2024 were screened from multiple electronic databases. Studies were selected based on predetermined inclusion and exclusion criteria, with a focus on older adults and their interactions with eHealth technologies.
Results
A scoping review of literature from PubMed, Web of Science, SCOPUS, and EBSCO identified 2247 studies, with 25 full-text articles published in the past 10 years. Findings reveal that e-health literacy decreases with age and lower education levels. External factors such as social support, technology access, and healthcare policies fluctuate with economic conditions, while internal factors like cognition, attitudes, and motivation are influenced by age and life experiences.
Conclusion
eHealth literacy holds promise for enhancing healthcare access and outcomes among older adults. However, significant barriers remain, particularly regarding usability, accessibility, and digital literacy. Future research should focus on targeted education and longitudinal evaluation to better understand and support older adults’ engagement with eHealth technologies.
Introduction
Background
Population aging is becoming one of the major social challenges of the 21st century. 1 The United Nations reported that 1 in 11 people was aged 65 or older in 2019 2 ; by 2050, the ratio is expected to be 1 in 6. With this demographic shift, the prevalence of chronic diseases among older adults is expected to increase dramatically. Available data emphasize the importance of health literacy for reducing comorbidities as well as enhancing the prevention and management of chronic diseases. 3 Traditionally measured at the individual level, health literacy refers to individual cognitive abilities that facilitate accessing, understanding, and utilizing health information for informed decision-making and the successful management of health. 4 Sørensen et al. expanded this concept by identifying three domains of health literacy: healthcare, disease prevention, and health promotion. 5 These domains illustrate the multi-dimensionality of health literacy and the necessity of addressing them, considering the challenges that an aging population presents.
The rapid advancement of technology has transformed the Internet into a primary source of health information due to its accessibility and immediacy. During the COVID-19 pandemic, internet usage for health information surged significantly. According to the Internet World Statistics report, global internet users surpassed 5.35 billion at the start of 2024, accounting for 69.4% of the world's population. 6 While online health information-seeking behavior is often associated with younger generations, an increasing number of older adults are also adopting this practice. 7 Despite challenges in learning and utilizing digital tools, the adoption rate among older adults has shown remarkable growth. For example, a 2023 report revealed that approximately 3.66 million Chinese individuals aged 60 and above accessed healthcare services via mobile internet, contributing to the total of 414 million healthcare users in the country. 8 The competence to obtain, understand and apply health information through electronic resources to improve health outcomes is designated as eHealth literacy or digital literacy and was originally conceptualized as e-health literacy by proposing the Lily Model, which consists of six components: traditional literacy, information literacy, media literacy, computer literacy, health literacy and science literacy. 9 However, this model has predominantly been explored in theoretical discussions, with limited empirical validation.
With a significant change in the availability and application of the power of health information, access to health knowledge from digital information not only opens more convenient and diversified channels for older adults to implement health management 10 but also empowers their self-care ability 11 to a certain extent. However, studies show that older adults from different geographical, cultural, and socio-economic backgrounds have been found to have very different levels of digital health literacy. This review synthesizes the research on eHealth literacy and older adults’ health outcomes in the past decade. It discusses how older adults use electronic devices to obtain health information today, as well as the different factors influencing this behavior. The results are helpful to understand the state of digital health in the aging population and showcase how eHealth literacy can meet the special health needs that older adults face.
Objectives and aim
The review aims: (a) to analyze and synthesize the key characteristics of the scientific literature on eHealth literacy published over the past decade, including research methodologies, tools for assessment, sample demographics, fields of study, and publication sources; (b) to explore how individual and societal level factors influence the effectiveness of eHealth education. The main research question can be further divided into the following questions.
What methodologies (including tools or approaches) have been used to evaluate the eHealth literacy of older adults? What internal and external factors, including but not limited to socioeconomic status, technology acceptance, education level, cultural differences, and social support, significantly influence older adults’ ability to utilize digital platforms for accessing health information?
Methods
Scoping studies have become an increasingly popular approach to synthesizing results from health research, particularly when the objective is to explore broad research areas or identify key concepts and knowledge gaps. 12 eHealth literacy and its associated factors represent a relatively nascent and interdisciplinary area of research, intersecting health sciences, information technology, and gerontology. Unlike systematic reviews, which are typically designed to answer narrowly defined questions or assess the effectiveness of interventions, scoping reviews are particularly useful for exploring broader research topics. This flexibility allows researchers to map existing knowledge, identify research trends, and highlight knowledge gaps in fields where definitions and frameworks are still evolving. Given the complexity and breadth of eHealth literacy, the scoping review method is well-suited to capture its multifaceted nature and synthesize the diverse findings reported in the literature. In addition, scoping reviews have a particular advantage in integrating conclusions drawn from different methodologies without excluding studies based on a rigorous quality assessment. 13 By accommodating both quantitative and qualitative data, the scoping review method allows for a richer understanding of how older adults engage with digital health information.
Methodological framework
Based on Arksey and O’Malley's 2005 publication of the first methodological framework 14 for conducting scoping studies serves, as a methodological framework for examining this article. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) acted as a foundation for this scoping review methodology. 15 Descriptive summaries and inductive analysis are utilized in scoping reviews to synthesize and summarize research findings. Unlike systematic reviews and meta-analyses, by not demand an evaluation of the listed research's methodological quality. 16 By using this approach, the study provides a comprehensive overview of eHealth literacy research while offering insights into the diverse factors that influence its development and application among older adults. This methodological choice not only aligns with the research objectives but also ensures that the review captures the complexity and breadth of the topic effectively.
Search strategy
To guide the search strategy, this study followed the Population, Intervention, Comparison, Outcome, and Study Design (PICOS) framework, as adapted for scoping reviews. 17
The main research question centers on eHealth education's impact on older adults’ health literacy. Specifically:
Population: Adults aged 55 years and older, Intervention: eHealth education, Comparison: Different levels of digital access, education, or health literacy Outcome: Measured levels of eHealth literacy or general health literacy
While the United Nations defines older persons as those aged 65 years and above, 18 this study adopted a broader age range to ensure inclusivity and comprehensiveness. Many previous studies have defined older adults using alternative age thresholds, such as 60+ or 55+. Therefore, to expand the scope of this review, we included individuals aged 55 years and older. The term “older adults” and its synonyms were incorporated into the search strategy, including: “>55 years old,” “Senior citizen,” “Elderly people,” “Older adults,” “Retirement age,” and “Mature adult,” “Advanced age.” For this study, eHealth education refers to the use of smartphones or other digital devices (e.g. smartwatches, human–computer interactions) to access health information. To ensure a comprehensive search, additional terms were included as synonyms for eHealth education, such as: “Digital Health literacy,” “Online Health,” “Telehealth Education,” “Web-based Health Education,” “Internet Health Education,” and “Health Informatics Education.” In line with the scope of the study, health literacy was conceptualized broadly to include varying levels of health knowledge and health education. To capture all relevant studies, the following terms were used: “Health Literacy,” “Health Knowledge Level,” “Health Education Level,” and “Health Information Literacy.” The search strategy was implemented across four major databases: Web of Science, SCOPUS, PubMed, and EBSCO. The search included studies published between 2015 and 2024, restricted to English-language articles with available abstracts. Table 1 demonstrates the list of search phrases specific to a certain database. The references were managed and deduplicated using EndNote 20, facilitating data extraction and organization.
Wednesday, March 27, 2024, with key terms: all terms.

Source: Authors’ own work.
Eligibility criteria
To be eligible for inclusion in this review, studies needed to meet the following criteria: involving older people (generally over 55 years of age); studies examining the access, use, usability, or impact of ehealth tools or interventions; published in English between January 2015 and 2024; and studies using qualitative, and quantitative, or mixed methods.
Exclusion criteria included studies that did not focus on e-health (e.g. information and communication technologies in general or non-health-related technologies); articles that were not specific to older people or were not analyzed separately for older people; to maintain a focus on high-quality literature, non-peer-reviewed sources were excluded, including opinion articles, editorials, systematic reviews, meta-analyses, letters to the editor, conference abstracts, and unpublished materials; non-English-language publications; and studies that were not available in full text.
Study selection
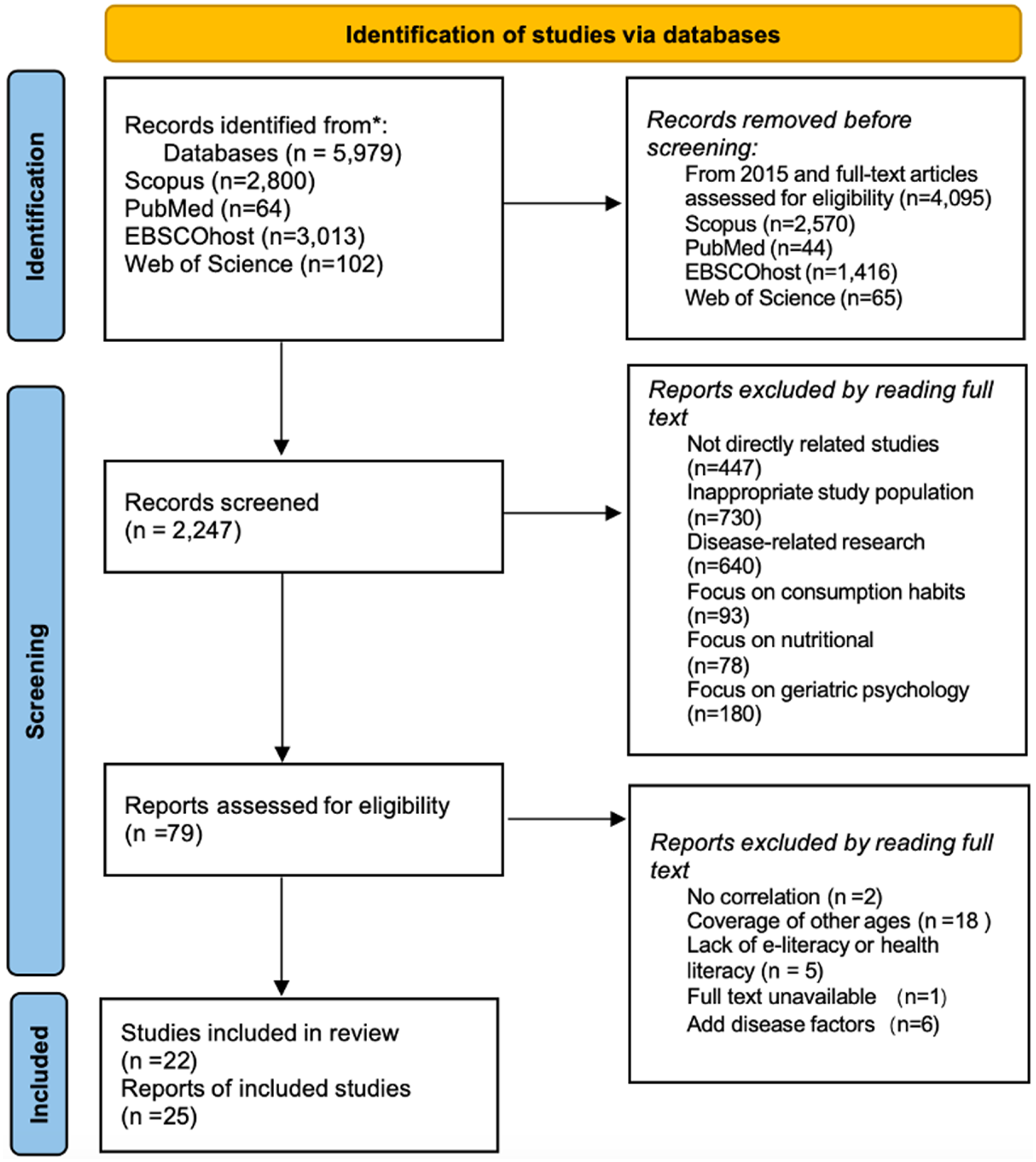
Following the completion of the literature search using the keywords outlined in Table 1, all references were imported into the literature management system (EndNote 20). The search yielded a total of 4095 studies (Scopus: 2570; PubMed: 44; EBSCOhost: 1416; Web of Science: 65) published between 2015 and 2024. After removing 1848 duplicates, 2247 unique papers remained for further screening. Using predefined eligibility criteria, two independent reviewers (YJ, SL) screened the titles and abstracts of the studies. This process was conducted in parallel, with any discrepancies resolved through discussion to reach a consensus, ensuring consistency and minimizing bias. After this stage, 79 studies were retained for full-text review. Subsequently, the full-text review was performed independently by both reviewers. During this process: 22 studies categorized as literature reviews were excluded; 18 studies focused on populations outside the target age group (55 years and older) and did not analyze or discuss the relevant population; 5 studies lacked specific references to e-health literacy or general health literacy: 3 studies focused solely on Internet use without addressing e-health literacy and 2 studies were unrelated to health literacy or health topics in general; 1 study lacked a full-text version accessible for analysis; 6 studies focused primarily on the impact of e-health literacy on geriatric illnesses, which, while informative, were considered better suited for discussion purposes rather than inclusion in the primary analysis.
This literature review process ultimately yielded 25 studies that met all inclusion criteria and aligned with the research objectives. These studies form the foundation of the analysis. Figure 1 presents an overview of the study selection process using the PRISMA flowchart.
Search procedure. Source: Authors’ own work.
Analysis
From the final set of 25 studies, key characteristics were extracted, including author(s), year of publication, study design, assessment tools, and population details (e.g. age distribution, mean age, and recruitment region). These attributes are visually summarized in Figures 2 and 3. The data extraction process was conducted independently by two reviewers (YJ, SL), who cross-validated the extracted information. Any disagreements were resolved through discussion to reach a consensus. This approach ensured reproducibility and minimized potential bias in data collection.

Summary of publication years. Source: Authors’ own work.
Scale summary. Source: Authors’ own work.
The studies were evaluated using the DigComp framework, 19 which was selected due to its robust structure for assessing digital competence. This framework allowed for a systematic analysis of critical elements, including digital health knowledge among older adults, the interaction between e-health literacy and general health literacy, the scope of e-literacy (e.g. use of smartphones, internet platforms, and e-coaching tools), and factors influencing e-health literacy. These evaluations focused on identifying both pertinent components and scales that could further inform the study's objectives. Where information was ambiguous or insufficiently reported, descriptive and statistical methods were applied to extract additional data, ensuring the completeness and accuracy of the findings. Table 2 provides a comprehensive summary of the studies, presenting a clear overview of their methodologies, outcomes, and focus areas.
Overview of included studies.

Result
Study characteristics
The sample consisted of 25 studies with publication years ranging from 2014 to 2024, having the greatest quantity of published studies in 2022 and the highest quantity of research in Asia (see Figure 2). Most research used a cross-sectional design (23/25), including 3 mixed studies, 2 qualitative studies, and 17 quantitative studies, while few employed longitudinal (1/25) and retrospective studies (1/25). Most of the studies used raw data, and in only two cases were the database data used for extraction.
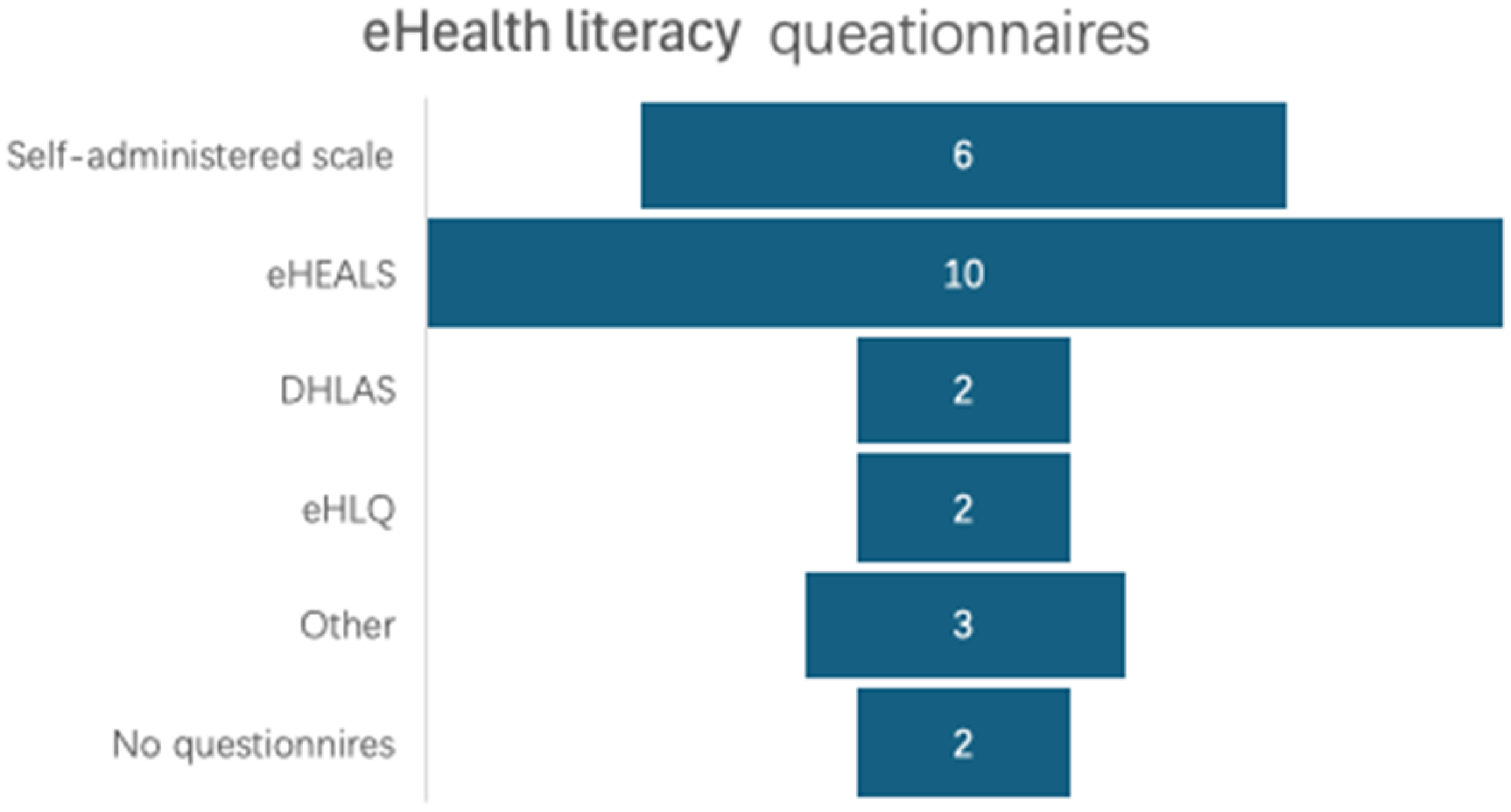
Comparison of scales used
Of the 23 articles containing full items of questionnaires, eHEALS (eHealth literacy scale), originally developed by Norman and Skinner, 44 was the most adopted, with eHEALS, DHLAS (digital health literacy assessment scale) and eHLQ (eHealth literacy questionnaire) being validated. Figure 3 shows using the scale of eHealth literacy for older people from the 25 articles; of these, eHEALS was used most for the eHealth Literacy Measurement Scale.
In this review, 13 studies employed sample sizes exceeding 100 participants, while others had smaller sample sizes. Notably, 4 studies included participants older than 60 years, 8 studies included participants over 65 years, and 2 studies focused on individuals aged 55 years and older. However, limited information was available regarding the residential areas of participants, with most studies being concentrated in metropolitan regions. Regarding the assessment tools, 10 studies utilized translated versions of eHealth literacy questionnaires, including 7 translations into Chinese Mandarin. Of these, one translation followed a strict translation process and was validated, while another used a previously translated version. Additionally, two studies employed a Korean translation, 45 and one study used a Spanish translation. 42 The remaining four studies relied on translated versions that had been previously validated in other studies.
In the development and validation of the remaining scales, each was constructed and validated independently, ensuring both robustness and relevance. Among these, two scales were derived from big data. One scale was based on the modification of a scale developed by Lim. 46 Additionally, six scales were self-created and subsequently verified. Table 3 provides a summary of the eHealth literacy questionnaires.
e-Health literacy questionnaire

eHEALS: eHealth Literacy Scale.
eHEALS-E: eHealth Literacy Dimensions.
DHLAs: Digital Health Literacy Assessment Scale.
eHLQ: eHealth literacy Questionnaire.
N/A: Not Applicable.
Source: Authors’ own work.
Associated factors
The factors influencing obtain to health information via the Web to improve health literacy were addressed to some extent in all 25 of the sample literature. Both internal and external factors were included. Internal factors include sociological factors, perceived behaviors, attitudes, etc., while external factors include social support, availability of equipment, and other related factors. Most studies have used sociological factors as dependent or control variables to investigate how eHealth literacy and health literacy are related and have found that they are mainly related to age, and education. Specifically, it shows that the older the age, the poorer the level of education, the more incidence of chronic ailments, and the greater the level of single-person residence in rural areas, the e-health literacy level is deficient. The impact of gender on it is not uniform, but most of the effects were higher for men than for women. One of them focuses on the heterogeneity of race in the United States with respect to searching for health behaviors via the Internet. Whereas positive behavioral effects, self-efficacy, and perceived reliability act as mediators to influence this eHealth literacy to health literacy-related relationship. And for external factors, social support is indispensable. Figure 4 summarizes the factors.

Influencing factors.
Discussion
Our review identified 25 studies that examined eHealth literacy in older adults, including 20 quantitative studies. Two qualitative studies, three mixed-methods studies. Additionally, an overview study provided broader insights into the topic. For each study, we listed the objectives, impact variables, and key findings. For quantitative studies, we specifically extracted data on eHealth literacy questionnaires and the factors influencing eHealth literacy. This review holds critical significance for public health and digital inclusion in the context of the global trend of population aging. As the proportion of older adults continues to grow worldwide, enhancing eHealth literacy is increasingly recognized as a vital pathway to improving overall health literacy and influencing health outcomes. Understanding the factors that contribute to or hinder eHealth literacy among older adults is not only important for advancing health education strategies but also for addressing broader public health challenges associated with an aging population. By systematically analyzing these studies, this review highlights the pressing need for targeted interventions and policy efforts to bridge the digital divide among older adults. It underscores the role of tailored eHealth education programs in empowering older adults to engage effectively with digital health tools and resources, thereby improving their access to healthcare information and promoting better health management.
Our review revealed that the overall level of eHealth literacy among older adults remains relatively inadequate. This insufficiency was consistently associated with internal factors such as aging-related physiological and cognitive decline, limited formal education, and socioeconomic factors. In reviewing the article, 21 studies reported a negative association between age and eHealth literacy, while 23 studies identified a strong positive link between higher education and eHealth literacy performance.
Socioeconomic factors, such as marital status and socioeconomic level, also exert a notable influence on eHealth literacy. Gender differences, however, present mixed findings across studies: Several studies report20,47,48 that men demonstrate higher awareness of eHealth literacy compared to women. This disparity is often attributed to patriarchal societal structures in certain regions, where males have greater access to educational opportunities, while others found women exhibit higher levels of eHealth literacy, likely due to their caregiving roles within families,49,50 which heighten their engagement with health-related information and preventive measures. Some studies argue that gender differences in eHealth literacy are negligible, 21 highlighting the need for further exploration of this relationship in diverse contexts.
Self-efficacy emerged as a crucial psychological factor influencing eHealth literacy among older adults. Several studies24,51,52 included in this review highlighted that individuals with higher self-efficacy were more confident in navigating digital platforms and more proactive in seeking health information online. These individuals were also more likely to translate digital engagement into positive health behaviors, including preventive care and chronic disease management. Moreover, self-efficacy mediated the relationship between social support and eHealth literacy, 1 indicating that individuals with stronger social networks may develop greater confidence in using technology through encouragement and guided experience. These findings underscore the need for interventions that build digital skills and strengthen users’ belief in their capacity to succeed. On the other hand, external factors, particularly social relationships and support networks, play a critical role in shaping older adults’ digital health engagement. Our review found that family involvement, companionship, and intergenerational support significantly contributed to older adults’ confidence in using eHealth tools. 53 For example, familial care and encouragement can mitigate psychological barriers, fostering a sense of competence and autonomy among older individuals in engaging with digital health technologies. 54 Understanding the interplay between these internal and external factors is essential for designing effective interventions aimed at improving eHealth literacy among older adults. A comprehensive approach that integrates both personal attributes and social contexts can inform tailored strategies to address the unique needs and challenges faced by this demographic. By addressing these multifaceted barriers, interventions can more effectively empower older individuals, enhancing their ability to access and utilize digital health resources to improve overall well-being.
eHealth literacy plays a pivotal role in shaping health literacy, particularly through the facilitation provided by Internet technologies. The widespread adoption of the Internet has dramatically simplified access to health information, enabling individuals to explore diverse health resources and educational content. This expanded accessibility not only broadens knowledge but also equips users with the tools to make informed health decisions. Norman and Skinner's eHealth literacy model 9 underscores the critical role of information assessment skills, highlighting that individuals with high eHealth literacy are more adept at evaluating the credibility and reliability of online health information. This ability reduces the likelihood of being influenced by misleading content and fosters the adoption of evidence-based health practices. Consequently, these individuals can make more rational and scientifically informed decisions regarding their health. Beyond information assessment, enhanced e-health literacy also empowers individuals to leverage digital technologies for self-health management. This proficiency is particularly crucial in managing chronic diseases, where regular monitoring and self-care practices are essential. Studies have demonstrated that the integration of e-health tools into chronic disease management significantly improves health outcomes. 55 By utilizing these tools, patients can better monitor their conditions, adhere to treatment plans, and engage in preventive measures, ultimately improving their quality of life. Understanding the connection between e-health literacy, health literacy, and chronic disease management underscores the importance of promoting digital health skills. This focus is critical not only for improving individual health outcomes but also for addressing the broader challenges associated with managing chronic conditions in aging populations.
Studies utilizing qualitative research methods, particularly those employing interviews to examine older adults’ subjective experiences with e-technology in health management, reveal a distinctly individualized approach to its use within this demographic. These studies underscore the diverse ways older adults engage with e-technology, shaped by their unique circumstances, preferences, and prior experiences. A consistent theme in the findings is the complexity and rapid evolution of e-technology, which often elicits feelings of anxiety, frustration, or apprehension among older users. 22 These emotional responses frequently lead to resistance or, in some cases, outright rejection of e-technology. Factors such as unfamiliarity with interfaces, fear of making errors, and the perception of e-technology as overly complicated further contribute to this hesitation. These findings highlight the pressing need for more accessible and user-friendly eHealth solutions tailored to the specific needs and concerns of older populations. Addressing these challenges requires not only simplified designs but also targeted training and support systems that build confidence and competency in e-technology use among older adults. Such interventions are essential to ensure that this demographic can fully benefit from the transformative potential of eHealth technologies, enhancing both health literacy and self-management capabilities.
In the initial stages of our review, we identified numerous studies examining eHealth literacy within the framework of specific chronic illnesses such as diabetes mellitus, malignancies, coronary heart disease, and spondylitis. This focus reflects the growing need for digital support in the management of these conditions. These findings underscore the critical need to address eHealth literacy as an integral component of chronic disease management for this demographic. For instance, a study conducted in the United States found a significant correlation between higher cancer fatalism belief scores and reduced utilization of health information technology. 56 This suggests that psychological factors like fatalism may hinder the adoption of eHealth tools, potentially limiting access to vital health information. Another American study focusing on older adults with chronic obstructive pulmonary disease (COPD) reported that increased disease severity was significantly associated with higher eHealth literacy levels. 57 This finding indicates that as health challenges become more pronounced, individuals may develop a greater need and motivation to engage with digital health resources. Given the high prevalence of multiple chronic conditions among older populations, understanding the relationship between e-health literacy and the self-management of these diseases is essential. The intricate relationship between disease-specific outcomes and ehealth literacy highlights the need for specialized interventions. 10 It follows that e-health literacy among older adults is influenced by a dual mechanism: psychological resistance may hinder participation, while perceived health needs promote digital adoption.
Our review also highlights the heterogeneity within the older people's population, reflecting differing aging processes and socio-cultural contexts. 58 Several studies set the threshold for older adults at 65 years and above,22–25 while others focus on those aged 60 and above.1,26–28 Additionally, a few studies adopt a broader definition, considering individuals aged 55 years and above.29–31 However, it is important to recognize that there are substantial variations in the use of electronic devices for health-related purposes within these age cohorts. The existing literature on e-health literacy often treats older adults as a homogeneous group, overlooking the significant heterogeneity within this population. A study by Győrffy et al. demonstrated significant behavioral differences within the group, with 65- to 75-year-olds showing higher rates of eHealth use than those over 75. 32 The study further projected that in the next decade, as younger cohorts age, their prior exposure to technology may reduce the generational gap in eHealth literacy. Future research and interventions should therefore avoid treating older people as a homogenous group and instead adopt an age-stratified or experience-based approach to digital health support. By applying the DigComp framework, we identified some imbalances in focus—review articles focused more on information and data literacy and problem-solving at the expense of digital collaboration, security, and content creation. However, problem-solving in the context of digital health remains a challenge for older people. The pressures of technological uncertainty and perceived security risks often hinder their ability to confidently use digital platforms, leading to lower e-health literacy,20,21 but few studies provide effective strategies to address these challenges. The lack of targeted interventions to build digital confidence and reduce perceived risk highlights a key gap in current research and practice. Integrating digital safety education and emotional support into eHealth literacy programs is essential to building a more inclusive and empowering digital health environment for older adults.
Limitations
This review has several limitations that should be acknowledged. Firstly, the exclusion of non-English publications may have resulted in the omission of relevant research published in other languages, potentially introducing a cultural bias. Secondly, while the inclusion criteria aimed to capture a broad range of studies, the use of wide search parameters may have inadvertently overlooked research focusing on more specific and nuanced aspects of e-health literacy. Furthermore, although the review adhered to the PRISMA-ScR guidelines, it is important to note that the protocol was not formally registered, which could impact the transparency and reproducibility of the review process. Finally, during the initial stages of screening, when titles and abstracts were reviewed, some articles that focused on disease-specific factors affecting e-health literacy, such as those on coronary heart disease or myelitis, were excluded. A more targeted focus on studies addressing how e-health literacy varies with specific physical conditions in older adults could have provided more comprehensive insights into the factors influencing e-health literacy in this population.
Conclusion
Over the past decade, particularly in the wake of the COVID-19 pandemic, the global focus on the utilization of electronic health information has intensified, leading to a rise in the number of older adults engaging with e-health tools. During the literature review process, it was noted that most studies continue to employ quantitative methods, primarily using specific questionnaires to assess the level of eHealth literacy among older populations. Despite global variations in demographic characteristics due to differences in economic development and national conditions, the overall e-health literacy among older adults remains relatively low. E-health literacy plays a pivotal role in influencing health behaviors among older individuals. Higher levels of e-health literacy are associated with more proactive and informed health decisions. Moreover, improved e-health literacy contributes to the enhancement of overall health literacy in older adults, which is increasingly important in today's digital healthcare environment. As access to accurate and timely health information becomes more dependent on digital platforms, empowering older adults with the skills to effectively use these resources can help bridge the gap between health information access and health outcomes. Ultimately, fostering higher levels of e-health literacy will contribute to a more health-literate and engaged older population, supporting their well-being in an increasingly digital world.
Footnotes
Acknowledgments
The authors would like to thank to Prof. Dr Yanti Rosil, Songlin Tang, Dr Nur Zakiah Mohd Saat, Prof. Dr Ruzita Abd Talib for their invaluable assistance and support in the completion of this project.
Ethics statement
This review does not involve any original studies with human participants or animals performed by the authors. All the reviewed studies were conducted in compliance with the respective ethical standards as reported by the original authors.
Contributorship
This study was supported by UKM, which provided the necessary research resources and academic environment; this study was guided by the PhD supervisors in the CORE group of the FSK college, which was pleased to complete this article.
All authors reviewed and approved the final version of the manuscript before submission.
Funding
The Article Processing Charge (APC) were supported by Faculty of Health Sciences, Universiti Kebangsaan Malaysia.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
YJ is the guarantor of this work and accepts full responsibility for the integrity of the content and data accuracy. The corresponding author, Prof Dr Yanti, serves as the guarantor of this work, ensuring its scientific integrity and overall quality.