
Abstract
Background
Leadership has emerged as a critical determinant of the performance and indeed the digital transformation of the healthcare system, especially in developing countries. The Health Sector Transformation Plan II and the Information Revolution Roadmap in the government of Ethiopia has emphasized leadership, governance, and digitalization; however, there has been little empirical evidence about leadership style.
Methods
This scoping study was conducted following PRISMA-ScR guidelines. Electronic databases and gray literature sources were searched for studies published between 2015 and 2024. Eleven empirical studies (2015–2024) on leadership and digital transformation of health in public health service in Ethiopia were identified for included. Study synthesis was carried out using the Full Range Leadership Model. Adaptive leadership and e-leadership were established as cross-cutting concepts for this study. Study quality was assessed through the Mixed Methods Appraisal Tool and Newcastle-Ottawa Scale.
Results
Among the different leadership styles studied, transformational leadership was found to be the dominant style, and it was the one that was highly and consistently linked to the three variables: health workforce motivation, accountability, and service delivery performance. The transactional leadership style was moderately utilized to achieve short-term compliance by performance monitoring. Passive and laissez-faire leadership strategies were rarely used, although they were always associated with negative results. Adaptive leadership behaviors were an integral part of transformational and transactional leadership styles, especially when the leadership decentralization was practiced.
Conclusion
Hybrid leadership models that are dominated by transformational leadership with digital leadership still emerging and having very limited capacity characterize Ethiopia's public health system. The institutionalization of adaptive and digital leadership is a must for the governance and leadership development frameworks to achieve a resilient, equitable, and digitally enabled primary healthcare in Ethiopia and other low- and middle-income countries.
Keywords
Key messages
A policy lever in leadership: Leadership, being transformational and adaptive, is a part of Ethiopia's Health Sector Transformation Plan II and will be an accelerator of progress toward universal health coverage by raising the level of health workforce motivation, accountability, and quality of the services.
Governance of digital investments in digital literacy, data systems, and infrastructure (frequent power shortages, insufficient internet connectivity in rural areas, and limited availability of hardware and digital devices) for expanding electronic leadership (e-leadership) capacity should be a priority according to the Information Revolution Roadmap.
Action for reform: National strategies should incorporate hybrid leadership models within the current Leadership, Management, and Governance programs to bring about a systemic change and not just isolated training programs.
Introduction
Leadership plays a critical role in the promotion of universal health coverage (UHC), particularly as health systems make greater use of digital technologies to increase access, quality, and integration. Global institutions such as the World Health Organization (WHO), the World Bank, and United Nations Development Program (UNDP) emphasize that achieving UHC requires leaders who can navigate complex digital health ecosystems, reconcile technology with policy, and manage sociotechnical change. Importantly, leadership in this context is not merely an administrative function but a relational and governance-driven process shaping how digital technologies are adopted, used, and sustained within health systems. In resource-constrained low- and middle-income countries (LMICs), such leadership is therefore a vital determinant of equity, resilience, and adaptive health system performance.1,2
On a global scale, digital health is expanding rapidly; however, leadership in digital transformation remains under-theorized and weakly operationalized, particularly in LMICs.3,4 Existing research has primarily focused on technology, infrastructure, and system functionality, while understating the role of leadership in digital governance, data use, accountability, and workforce engagement. This imbalance has limited understanding of why similar digital tools produce divergent outcomes across settings. Emerging evidence shows that digital technologies improve systems only when leaders are directly involved in shaping organizational culture, incentives, and decision-making processes.5,6
Evidence from sub-Saharan Africa illustrates this dynamic clearly: while Rwanda's digitally enabled performance management systems benefited from strong political and administrative leadership, experiences from countries such as Ghana and Uganda show that hierarchical or passive leadership can limit data use and slow reform despite the availability of digital platforms.7–9 These contrasts suggest that leadership style, rather than technology alone, mediates the effectiveness of digital health investments.
In Ethiopia, ambitious reforms under the Health Sector Transformation Plan II (HSTP-II) and the Information Revolution Roadmap explicitly position digitalization as a catalyst for UHC, service quality improvement, and equity. Despite growing investments in digital health infrastructure, there is limited synthesized evidence on how leadership styles influence the adoption, use, and equity outcomes of digital health systems within Ethiopia's primary healthcare (PHC) context. Moreover, existing studies remain fragmented, methodologically heterogeneous, and rarely analyzed through integrated leadership and sociotechnical frameworks, limiting their explanatory and comparative value.10,11
However, implementation evidence suggests that leadership capacity has lagged behind digital health expansion. Hierarchical management, politicized appointments, gender inequities, limited district autonomy, and insufficient digital leadership skills constrain effective integration of digital tools into governance and decision making.7,12 As a result, digital systems are often used primarily for upward reporting, rather than enabling strategic leadership, adaptive learning, or enhanced accountability across health systems.
Although Ethiopia has prioritized digital health through platforms such as District Health Information Software 2 (DHIS2), Electronic Medical Records (EMRs), and mobile health applications, implementation outcomes remain uneven across PHC settings, suggesting gaps beyond technological availability. Leadership in Ethiopia's digital health transformation represents a critical but insufficiently theorized domain. In particular, e-leadership (the process of leading individuals, teams, and organizations through digital technologies, emphasising virtual communication, technology-enabled decision-making, and remote team management) remains under-defined and under-assessed.13,14 Operationalizing e-leadership allows the study to examine how leaders guide digital teams, shape technology adoption, and facilitate digitally enabled accountability, bridging the gap between leadership theory and digital health practice.
To address this imbalance, this scoping review deliberately shifts its focus from leadership in general to leadership for digital health transformation. While transformational leadership remains a key theoretical foundation, it is examined specifically in terms of how it enables or constrains digital governance, data use, accountability, and organizational learning. Rather than proposing a new leadership theory, this study advances conceptual clarity by integrating the Full Range Leadership Model with Adaptive Leadership and e-leadership as cross-cutting capabilities relevant to decentralized, resource-constrained health systems. Ethiopia is treated as an analytically informative case, offering insights with relevance for other LMICs undergoing similar digital health reforms.
Methods
This study employed a scoping review methodology, guided by the Arksey and O’Malley framework and further refined by Levac et al., to map and synthesize existing evidence on leadership styles influencing digital health transformation in Ethiopia's PHC system.15,16 To ensure transparency, reporting adhered to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) checklist. 17
A completed PRISMA-ScR checklist is included as Supplemental 1. The review was structured using the PCC (Population, Concept, and Context) model, with analysis informed by the Full Range Leadership Model (FRLM), Adaptive Leadership, and e-leadership frameworks.
The guiding question was: “How do transformational, adaptive, and e-leadership styles influence organizational performance, accountability, and digital health transformation within Ethiopia's primary healthcare system between 2015 and 2024?”
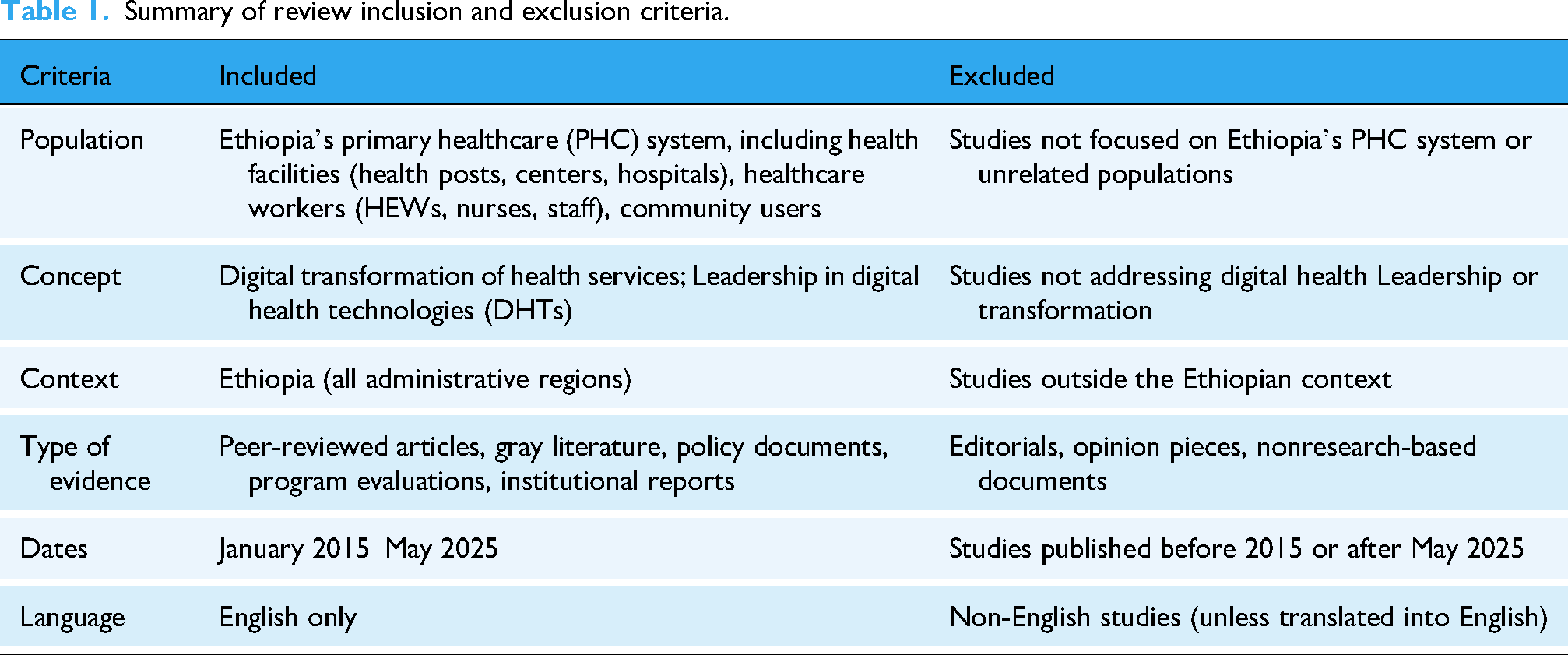
Inclusion and exclusion criteria
The literature search covered the period from 2015 to 2024. This time frame was deliberately selected to align with Ethiopia's major health system and digital transformation milestones, beginning with the launch of the first Health Sector Transformation Plan (HSTP-I in 2015) and including the subsequent HSTP-II (adopted/starting in 2020/21) and the national Information Revolution agenda and Strategic Plan (initiated around 2016–2018).
Digital health initiatives and leadership reforms prior to 2015 were limited in scale and policy relevance, whereas the post-2015 period reflects accelerated digitalization, decentralization, and governance reforms. Restricting the review to this period therefore ensured policy relevance, comparability, and alignment with contemporary leadership and digital governance frameworks (Table 1).
Summary of review inclusion and exclusion criteria.
A comprehensive search was conducted across PubMed/MEDLINE, Scopus, Web of Science, and Google Scholar, supplemented by targeted searches of institutional and policy-oriented sources.
These databases were selected to balance biomedical, health systems, leadership, and interdisciplinary scholarship, ensuring coverage of both peer-reviewed public health literature and applied governance research.
Google Scholar was included to capture context-specific and LMIC-focused studies that may not be indexed in conventional biomedical databases, particularly those addressing leadership, governance, and health system management.
In addition, reference lists of included articles were manually screened to identify relevant studies not captured through database searching. This approach strengthened retrieval of Ethiopia-focused and regionally published studies.
Search terms combined leadership concepts (“transformational leadership,” “transactional leadership,” “laissez-faire,” “adaptive leadership,” “digital leadership”, “hybrid leadership”), context-specific terms (“Ethiopia,” “primary healthcare,” “health system,” “digital health”), and performance metrics (“organizational performance,” “governance,” “health workforce”). Boolean operators and search filters were applied to refine results and ensure relevance. 18
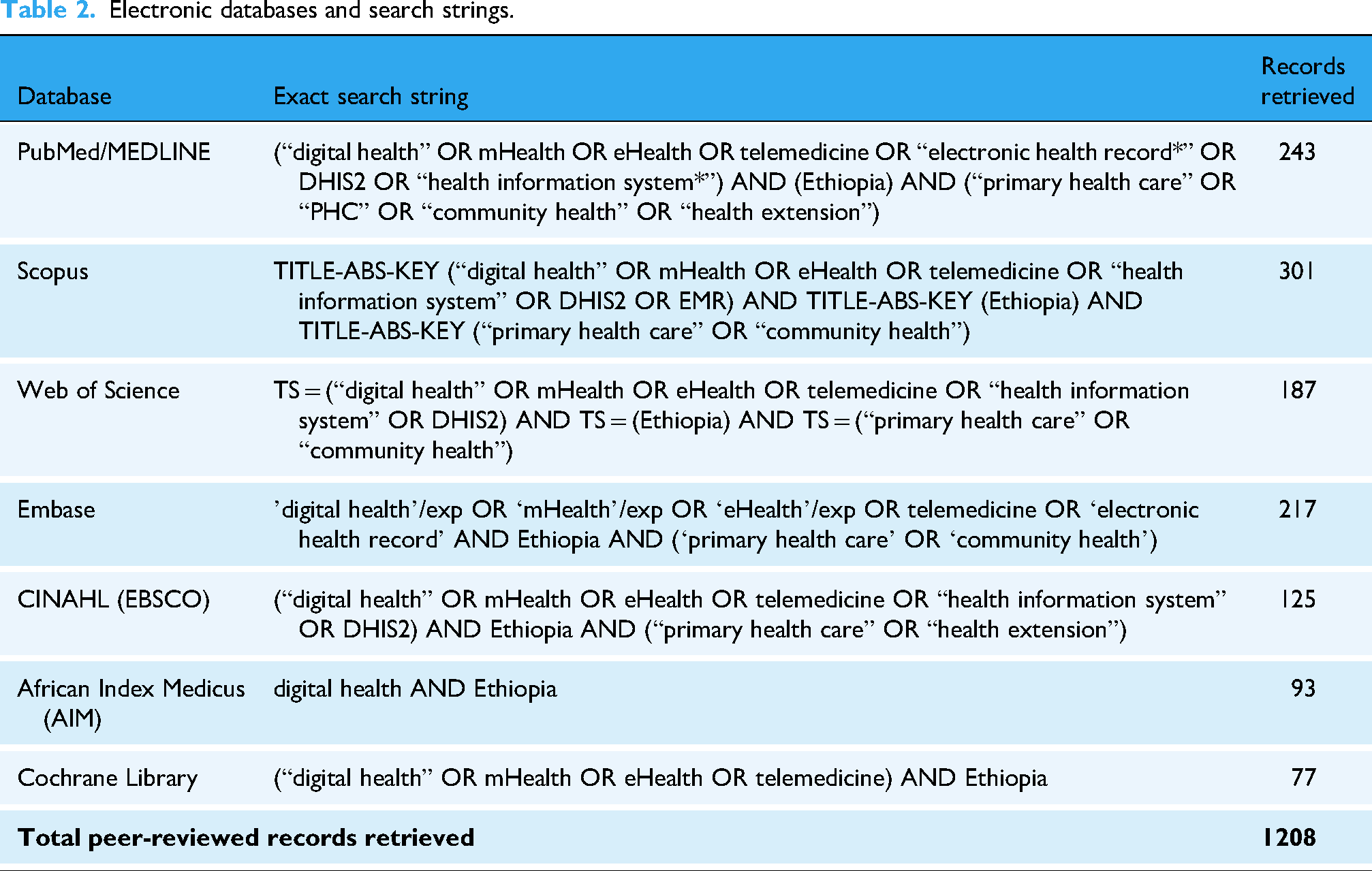
Electronic databases and search strings
We used controlled vocabulary (e.g. MeSH), Boolean operators and truncation adapted to each database. The search focused on digital health interventions in Ethiopia's PHC context (Table 2).
Electronic databases and search strings.
Gray literature retrieval
To capture unpublished and policy-relevant sources, we conducted a systematic gray literature search. This included national strategy documents, program evaluations, reports by international organizations and university theses (Table 3).
Gray literature retrieval.

All the records were managed in EndNote and duplicates were removed. Two reviewers (IM and RD) independently screened the titles and abstracts. The full texts of potentially relevant articles were assessed independently, with disagreements resolved by a reviewer (IM and RD).
A PRISMA-ScR flow diagram summarizes the search and selection process. A total of 1421 records were identified through database and gray literature searches. After the duplicate removal (n = 285), 1136 records remained. The title and abstract screening excluded 1024 records based on predefined inclusion criteria. The full-text review was conducted for 101 articles, of which 11 were eligible for final synthesis (Figure 1).

PRISMA diagram on digital transformation in the primary healthcare (PHC) system, Ethiopia, 2025.
All records were deduplicated in EndNote. Two reviewers independently screened titles and abstracts, followed by full-text assessment against predefined eligibility criteria. Disagreements were resolved through consensus, with consultation of a third reviewer when necessary. The study selection process is presented in the PRISMA-ScR flow diagram.
A standardized extraction tool captured study characteristics (author/year, setting, design, sample, leadership style, and outcomes). Beyond outcomes (e.g. staff motivation, organizational effectiveness, and digital integration), studies were also appraised for policy relevance, whether findings had implications for Ethiopia's governance structures, decentralization reforms, or alignment with national strategies (HSTP-II, Information Revolution Roadmap).
The FRLM, the Adaptive Leadership framework, and emerging constructs from e-leadership were used to guide data analysis and interpretation.19,20 Quantitative data were descriptively summarized, while qualitative findings were thematically analyzed using six-phase reflexive thematic analysis approach. 21 This dual analytic strategy ensured a robust synthesis across different methodological designs.
All 11 studies published between 2015 and 2024 met the minimum methodological quality thresholds required for inclusion in this review. Methodological appraisal was conducted using the Mixed Methods Appraisal Tool (MMAT, 2018 version) and the Newcastle–Ottawa Scale (NOS) for nonrandomized studies, consistent with established guidance.22,23 Collectively, these tools confirmed that the included evidence base was sufficiently robust to support an integrated synthesis of leadership styles and digital health outcomes within the Ethiopian PHC context.
Specifically, the MMAT was applied across its five methodological domains according to study design category, including qualitative, quantitative, and mixed-methods studies. For mixed-methods research, assessment explicitly addressed the rationale for mixed-methods use, integration of qualitative and quantitative components, interpretation of integrated findings, management of inconsistencies, and overall methodological coherence. In line with MMAT recommendations, no composite numerical scores were calculated; instead, domain-level judgments were reported to avoid inappropriate quantification and preserve methodological nuance.
In parallel, quantitative observational studies were assessed using the Newcastle–Ottawa Scale, focusing on selection, comparability, and outcome or exposure domains. Star-allocation criteria were clearly specified, and studies were categorized as low, moderate, or high quality based on established thresholds. These procedures are now described narratively in the Methods section and summarized in Table 4, thereby enhancing transparency and reproducibility.
Leadership models, study characteristics, and key findings from empirical studies conducted in Ethiopia's health system (2015–2024), 2025.

DHIS2: District Health Information Software 2; LMG: Leadership, Management, and Governance; MBE-A: Management-by-Exception (Active); MBE-P: Management-by-Exception (Passive).
Regarding study designs, cross-sectional surveys predominated, most commonly employing the Multifactor Leadership Questionnaire (MLQ) with high internal reliability (Cronbach's α ≥ 0.90).24,26,34 Larger samples, such as Teame et al., 27 (n = 844) and Woldu and Rao, 34 (n = 568), enhanced statistical power. Smaller-scale mixed-methods studies, 32 n ≈ 350 offered deeper contextual insights, especially regarding leadership challenges in rural or under-resourced settings.
Although limitations such as self-reported measures, social desirability bias, and limited longitudinal evidence were observed, the overall methodological quality was adequate. Importantly, the consistent use of validated tools, reasonable sample sizes, and increasing attention to adaptive and e-leadership capacities justify the integrated application of the FRLM, Adaptive Leadership, and e-leadership frameworks, reinforcing the credibility of this emerging evidence base within Ethiopia's digital health reform agenda. 10
In line with Arksey and O’Malley's recommended sixth stage, preliminary findings were discussed with two Ethiopian health policy experts during manuscript drafting. Their feedback was used to strengthen the interpretation of leadership implications for governance reform and UHC progress.
Theoretical integration
The review was guided by an integrated conceptual approach combining leadership theories (FRLM, Adaptive Leadership, and e-leadership). A synthesis of 11 Ethiopian studies using the FRLM was used to analyze leadership styles in Ethiopia's healthcare system. FRLM was selected because it comprehensively captures transformational, transactional, and laissez-faire leadership it alone does not fully address the dynamic, technology-driven, and complex challenges of digital health in LMIC settings.
Integration with adaptive leadership is required to enable leaders to respond flexibly to unpredictable challenges and system-level changes, while e-leadership integration ensures leaders can effectively guide digitally enabled teams and manage technology-driven processes. This combined model approach strengthens the applicability of FRLM in analyzing leadership in digital health transformation and our study objectives. 30
Adaptive Leadership features prominently in interventions like the Leadership, Management, and Governance (LMG) program, which focuses on problem-solving, team learning, and coaching, reflecting Heifetz and Linsky's core concepts such as managing distress and fostering productive conflict. 30 These adaptive practices effectively address complex technical and systemic challenges, especially amid resource constraints.31,32
E-leadership aspects are emerging through the adoption of digital tools like DHIS2 and electronic Health Management Information System (eHMIS) for data-driven decision making and performance monitoring.24,31 Yet, virtual collaboration and cyber-leadership remain limited, indicating a gap in digital leadership skills among Ethiopian health leaders.
Studies also link leadership to innovation agility, with managers employing quality improvement tools that encourage intellectual stimulation and adaptive change.26,28 Conversely, passive leadership is less explicitly evidenced. For example, studies report associations between passive leadership styles and staff disengagement, weakened supervision, and diminished accountability mechanisms, 25 yet they do not consistently provide disaggregated data linking passive leadership to measurable declines in service quality or performance outcomes in specific regions or facilities.
This review positions leadership as a central policy lever shaping governance effectiveness and digital health transformation in Ethiopia's PHC system. It presents an Integrated Leadership Framework designed to guide Ethiopia's digital health transformation within its PHC system (Figure 2).

Integrated leadership framework for digital health transformation in Ethiopia's primary healthcare system, 2025.
Results
Characteristics of sources of evidence
This scoping review comprises 11 empirical studies conducted within the Ethiopian public health sector between 2015 and 2024. The included studies consist of eight quantitative studies, two mixed-methods studies, and one qualitative study. The quantitative studies mostly used facility-based or system-level survey designs comprising structured questionnaires examining leadership styles and organizational practices. 29
Quantitative facility-based research included study samples from n = 212 to n = 844 participants, while system-level research included data from n = 76 to n = 284 districts. 35 Mixed-methods studies combined survey data with interviews, collecting additional data from 14 public health institutions or 844 healthcare managers. In the qualitative study, data were collected from 41 PHC managers. 33
Across the sources, participants represented a broad spectrum of the health system, including nurses and frontline workers, medical staff, facility managers and supervisors, and district health officials. Facility-level quantitative studies primarily focused on nurses and frontline staff in public hospitals and PHC facilities, with sample sizes typically ranging from 300 to 568 participants. 29 Other studies focused on facility-, district-, and regional-level leadership, with qualitative investigations examining the leadership backgrounds and experiences of facility and mid-level managers. 33
All studies were conducted in public health organizations across Addis Ababa, Oromia, Amhara, Tigray, and SNNPR regions. Collectively, these studies provide contextual insight into leadership dynamics shaping governance and service delivery within Ethiopia's decentralized public health system.
Distribution of leadership styles
Across the reviewed studies, transformational leadership emerged as the most frequently reported and consistently high-scoring leadership style, reflecting leaders’ role modeling, inspirational motivation, and intellectual stimulation. 29
In addition, adaptive leadership practices were commonly embedded within transformational and transactional behaviors, particularly in decentralized or resource-constrained settings. For example, district health offices in Ethiopia utilized adaptive leadership through mentoring, coaching, and participatory problem-solving sessions, enabling leaders to distinguish technical from adaptive challenges, foster staff engagement, and strengthen system resilience under decentralized governance. Meanwhile, transactional leadership demonstrated moderate and variable application, primarily through contingent rewards and active supervision.
Conversely, passive and laissez-faire leadership styles were consistently least observed, often correlating with limited oversight and reduced staff engagement. 33 Furthermore, e-leadership as a core enabler of health system transformation appeared recently and unevenly across digitally supported settings; however, they remained largely tool-focused and under-institutionalized, reflecting the early stage of digital leadership adoption in Ethiopia's health system (Table 4).
Transformational leadership
Transformational leadership emerged as the most prevalent and consistently practiced leadership style across facility, district, and regional levels. 29 Quantitative scores generally ranged from 2.2 to 2.8, indicating behaviors were practiced “sometimes” to “fairly often.” Across studies, transformational leadership was associated with higher staff engagement, organizational commitment, and improved service delivery performance.
Idealized influence
Idealized influence, both attributed and behavioral, manifested through leaders’ role modeling, ethical conduct, and visible commitment to organizational goals. Strong expressions were observed in district-level reforms and leadership initiatives emphasizing quality standards and accountability. 35 However, political appointments and limited merit-based selection mechanisms weakened the consistency of idealized influence in some contexts. 33
Inspirational motivation
Inspirational motivation was particularly prominent in facility- and district-level studies, with leaders emphasizing shared vision, mission alignment, and collective goal-setting. These behaviors were linked to higher staff morale, engagement, and progress toward priority service delivery targets, including maternal and child health indicators.
Intellectual stimulation
Intellectual stimulation involved problem-solving initiatives, quality improvement projects, and structured learning platforms. Health workers were encouraged to question routines, use data for decision making, and experiment with locally appropriate solutions. Externally supported quality-improvement programs institutionalized iterative learning and adaptive experimentation.
Individualized consideration
Individualized consideration was less consistently reported but included coaching, mentoring, and tailored staff development support. Constraints such as workforce shortages, leadership turnover, and high managerial workload limited its implementation in some settings. 29 Where present, individualized consideration enhanced staff readiness for change and morale.
Transactional leadership
Transactional leadership operates along a control–compliance continuum, primarily through contingent reward and management-by-exception (active).36,37 In Ethiopia, transactional leadership was moderately practiced, most visibly in donor-supported or performance-based initiatives where indicators, targets, and reporting structures were clearly defined. 35
Digital health systems increasingly mediated these transactional practices. Tools such as DHIS2, eHMIS, and electronic supervision platforms operationalized management-by-exception (active) by enabling routine performance monitoring, deviation detection, and corrective feedback. These findings demonstrate a digitally enabled transactional layer within the FRLM, where technology amplifies managerial oversight but does not independently generate motivation or learning.
Consistent with WHO and World Bank guidance, transactional leadership, whether digitized or manual, proved effective for short-term accountability but insufficient for adaptive system change.1,2 Without complementary transformational and adaptive leadership, digitally mediated controls risk reinforcing compliance-driven performance rather than sustained quality improvement.
Passive and laissez-faire leadership
Management-by-exception (passive) (MBE-P) and laissez-faire leadership represent the lowest-effectiveness leadership spectrum. Ethiopian evidence shows that MBE-P behaviors were reactive and delayed, often triggered only after performance failures became visible. 33
Importantly, digital systems did not compensate for passive leadership. Although routine data were available, passive leaders rarely interpreted or acted on information proactively, rendering digital platforms administrative reporting tools rather than leadership instruments. This aligns with LMIC evidence that digital infrastructure cannot substitute for leadership capacity.
Laissez-faire leadership consistently reflected leadership absence rather than intentional delegation, undermining accountability, coordination, and trust. From an FRLM perspective, this style negates both transactional control and transformational influence, posing particular risks in digitally governed systems that require active stewardship and ethical data use.
FRLM-aligned adaptive leadership practices
Adaptive leadership was rarely measured explicitly; however, its practices were embedded within transformational and transactional leadership approaches. Leaders distinguished technical from adaptive challenges while addressing governance gaps, organizational culture, and health workforce motivation, thereby supporting system-level responsiveness.
Moreover, adaptive leadership addressed organizational distress through coaching and mentoring, enabling health workers to manage uncertainty during reform. Responsibility was devolved to frontline teams through participatory planning and self-assessment, strengthening ownership, shared accountability, and context-responsive problem-solving. 29
Notably, adaptive leadership capacity was evident in practice but lacked formal operationalization or validated measurement across studies, highlighting a methodological gap in the Ethiopian leadership literature.
FRLM-aligned e-leadership practices
E-leadership in Ethiopia emerged indirectly, primarily embedded within transformational leadership rather than operating as a distinct leadership style. It enabled data-informed visioning and intellectual stimulation by leveraging routine service data and facilitated boundary-spanning coordination across facilities, districts, and communities.
Within transactional leadership, e-leadership manifested through digital performance monitoring systems, including DHIS2, eHMIS, and electronic supervision tools, which supported technology-enabled feedback loops and timely corrective action.
Nevertheless, advanced e-leadership competencies, such as virtual collaboration, digital trust, cybersecurity awareness, and strategic digital change management, were rarely assessed. Consequently, digital leadership remained tool-focused, under-institutionalized, and unevenly distributed across the health system.
Overall, the Results indicate a leadership profile dominated by moderate transformational leadership, supported by functional but limited transactional mechanisms, minimal laissez-faire leadership, and implicitly embedded adaptive and digital practices. These findings describe observed leadership behaviors without normative interpretation, which is addressed in the Discussion section.
Discussion
Overview and contribution to knowledge
This scoping review synthesizes evidence on leadership styles shaping Ethiopia's public health system between 2015 and 2024 and contributes to the literature by bridging leadership theory with digital health governance in an LMIC PHC context. The findings demonstrate that transformational leadership, often interwoven with adaptive practices, dominates leadership behavior across facility, district, and regional levels.
Transactional leadership plays a complementary role through performance monitoring and accountability mechanisms, while passive and laissez-faire leadership styles are consistently associated with weaker organizational outcomes. E-leadership emerges as an enabling but under-institutionalized capability, primarily embedded within existing leadership styles rather than functioning as a distinct domain.1,38,39
By explicitly mapping empirical findings to the FRLM and extending it through adaptive and digital leadership lenses, this review advances conceptual clarity on how leadership styles interact as a hybrid system rather than as isolated typologies. This integrated framing responds to global calls from WHO, World Bank, African Union, and UNICEF to better understand leadership as a sociotechnical governance process operating at the intersection of workforce capacity, accountability, and digital infrastructure.
Transformational leadership as a system stabilizer
Transformational leadership emerged as the most prevalent and consistently practiced style across Ethiopian public health facilities. Rather than being interpreted as a universally optimal model, transformational leadership in this review functions primarily as a system stabilizer, maintaining motivation, legitimacy, and organizational coherence in a resource-constrained and reform-intensive environment. This pattern aligns closely with the WHO's leadership and governance framework, which identifies transformational leadership as a cornerstone of resilient health systems and progress toward UHC. 1
Similarly, World Bank and AU governance analyses emphasize leadership that builds trust, legitimacy, and institutional commitment as essential for public sector effectiveness. 38 Evidence from Ethiopia mirrors experiences in other LMICs. In Rwanda, transformational leadership integrated with performance monitoring and community engagement has contributed to sustained gains in maternal and child health outcomes. In India, district-level transformational leadership has supported quality improvement in PHC when aligned with frontline empowerment and strategic visioning.
Comparative evidence from Rwanda and India reinforces this interpretation, demonstrating that transformational leadership supports digital health gains when aligned with governance reform, frontline empowerment, and accountability mechanisms.40–42 However, the Ethiopian case also illustrates the limits of transformational leadership when structural constraints, such as politicized appointments and weak meritocratic pipelines, remain unaddressed, underscoring the need for complementary adaptive and digital leadership capacities.
Similar barriers have been documented across LMIC health systems, where bureaucratic inertia limits the translation of visionary leadership into sustained organizational reform.42–44 Thus, transformational leadership in Ethiopia functions as a stabilizing force, but its reform potential remains contingent on governance reform and institutional support.
Adaptive leadership and distributed problem-solving
Adaptive leadership practices were rarely measured explicitly but were consistently embedded within transformational and transactional behaviors, as demonstrated in the results. Ethiopian leader distinguished technical from adaptive challenges, promoted participatory planning, and supported staff through mentoring and coaching, key elements of adaptive leadership theory. These findings align with WHO's adaptive governance principles, which emphasize learning, flexibility, and decentralized problem-solving in complex health reforms. 45
United Nations Children's Fund similarly demonstrates adaptive leadership as critical for empowering frontline workers and improving maternal, newborn, and child health outcomes, particularly in fragile and decentralized systems. 39 Comparative evidence from Uganda and Kenya suggests that adaptive leadership can mobilize local resources and foster iterative learning; however, its effectiveness is often constrained by weak accountability systems and infrastructure gaps.
World Bank and AU policy analyses reinforce this pattern, noting that while adaptive leadership enhances complexity management, it must be anchored within formal governance structures to avoid ambiguity and role diffusion. In Ethiopia, adaptive leadership appears necessary for navigating reform complexity but remains insufficiently institutionalized, echoing broader LMIC challenges in translating adaptive capacity into durable system change.
Transactional leadership and passive leadership
Transactional leadership was moderately practiced in Ethiopia, primarily through contingent rewards, supervision, and performance monitoring mechanisms. As shown in the Results section, transactional tools such as scorecards, audits, and review meetings supported short-term compliance and accountability, particularly within structured reform initiatives. This aligns with LMIC reform evidence indicating that transactional mechanisms are most effective when embedded within hybrid leadership arrangements that include transformational and adaptive elements.
Conversely, passive and laissez-faire leadership styles were consistently associated with reduced staff engagement, weak accountability, and poorer service delivery outcomes. This finding aligns with global leadership literature demonstrating that passive leadership undermines governance, morale, and workforce retention. AU and World Bank analyses similarly identify passive leadership as a critical barrier in systems lacking professionalized leadership pipelines and enforcement mechanisms. 46
Importantly, the Ethiopian evidence suggests that eliminating passive leadership requires systemic reform rather than individual behavior change, including merit-based appointments, leadership accountability frameworks, and sustained management capacity-building.
Digital e-leadership: Emerging but under-institutionalized
E-leadership in Ethiopia emerged indirectly, embedded within transformational and transactional leadership practices rather than operating as a distinct domain. Consistent with the Results, transformational e-leadership enabled data-informed visioning and boundary-spanning coordination, while transactional e-leadership relied on DHIS2, eHMIS, and electronic supervision tools to strengthen monitoring and feedback loops.
The widespread adoption of DHIS2 across more than 70 LMICs underscores the growing centrality of digital platforms in health governance. However, this review confirms that advanced digital leadership competencies, such as strategic digital change management, virtual collaboration, cybersecurity awareness, and digital trust, remain largely absent. As a result, digital leadership in Ethiopia remains tool-focused, fragmented, and unevenly distributed.
Contemporary digital leadership scholarship conceptualizes digital leadership as a sociotechnical influence process, requiring digital literacy, strategic foresight, and organizational change management capabilities. Empirical studies published reinforce this view, showing that health professionals increasingly expect leaders to manage digital workload, support competence development, and ensure accountability for digital service outcomes. These findings align with WHO's Digital Health Strategy, which identifies leadership and governance as core enablers of digital health ecosystems. 47
While Ethiopia's Information Revolution Roadmap and Digital Ethiopia 2030 strategy articulate these priorities, the Results indicate a gap between digital tool deployment and leadership capability development, placing Ethiopia in a transitional phase of digital leadership maturity.
Governance, equity, and LMIC considerations
Leadership effectiveness in Ethiopia is deeply shaped by governance arrangements, political dynamics, and equity considerations. Despite women comprising the majority of the health workforce, they remain underrepresented in leadership positions, a pattern observed across many LMICs. WHO, AU, and UNICEF frameworks consistently emphasize gender equity and inclusive leadership as prerequisites for legitimate and sustainable health governance.7,48
LMIC digital health research further highlights leadership capacity as a decisive determinant of digital adoption and outcomes. Frameworks developed for low-resource settings identify leadership alignment with regulatory and interoperability standards as critical enablers amidst persistent infrastructure and workforce constraints. 49 Evidence from Uganda demonstrates how leadership support for enterprise architecture and interoperability can standardize digital health interventions, offering transferable lessons for Ethiopia. 50
Comparative insights and transferability
The regional leadership landscape highlights how different styles shape health system outcomes in sub-Saharan Africa. Rwanda demonstrates the value of transformational leadership when combined with community engagement and digital innovation, contributing to sustained gains in maternal and child health. 51
Specifically, Rwanda's digital leadership training mechanisms and participatory governance approaches can inform Ethiopia by strengthening data-driven decision making, fostering local ownership, and improving district- and facility-level management. Similarly, Nigeria's Abiye project illustrates how political will, aligned with local leadership and digital referral systems, can drive systemic change. Adapting these practices, Ethiopia can integrate digital competencies with community participation to enhance accountability, innovation, and equity in its health system.
In contrast, Kenya and Uganda exemplify the limitations of transactional and hierarchical approaches. Although performance monitoring systems improved administrative compliance, they often failed to inspire frontline health workers or foster a culture of innovation. Likewise, Ghana and South Africa show that passive leadership at the facility level undermined otherwise strong governance frameworks, weakening accountability and contributing to staff attrition.52,53
The Tanzania–Malawi–Mozambique corridor highlights adaptive and e-leadership practices, including district coaching, governance councils, and mobile health platforms, which produced measurable improvements. Yet progress remained uneven, constrained by weak infrastructure and persistent gender inequities.54,55
Taken together, these cases demonstrate that leadership is a decisive lever for system performance. For Ethiopia, lessons from Rwanda and Nigeria suggest that hybrid models, combining transformational, adaptive, and digital leadership approaches, can accelerate UHC and digital health integration, while ensuring equity, innovation, and accountability. Countries relying primarily on transactional or passive leadership models, in contrast, struggled to achieve sustainable system improvements.56,57 The lesson for Ethiopia's Ministry of Health is clear: achieving UHC and digital transformation will depend on consolidating hybrid, equity-oriented leadership models that foster accountability, innovation, and inclusive governance (Figure 3).

Comparative analysis of leadership styles and health system effectiveness in selected African countries, 2025.
Toward hybrid and digitally ready leadership models
Collectively, the evidence supports the adoption of hybrid, digitally ready leadership models that integrate transformational, adaptive, transactional, and digital competencies. Such models are particularly suited to decentralized health systems facing simultaneous governance, equity, and digital transformation challenges.
Based on the Results and Discussion sections, key policy implications include:
Strengthening transformational and adaptive leadership competencies through formal training. Institutionalizing digital leadership within national leadership development programs. Embedding digital leadership within governance and accountability frameworks. Using transactional tools selectively to reinforce performance and learning. Eliminating passive leadership through professionalization and oversight. Mainstreaming gender equity and intersectionality within leadership pipelines.
These strategies align with Ethiopia's HSTP-II, Information Revolution Roadmap, and WHO Digital Health Blueprint, offering a coherent pathway for sustainable and equitable health system transformation. Future research should prioritize longitudinal and mixed-methods designs to assess the system-level effects of hybrid and digital leadership interventions in LMIC contexts (Table 5).
Integration of AL and EL in Ethiopia's health sector.

AL: Adaptive leadership; ANC: Antenatal Care; DHIS2: District Health Information Software 2; EHCRIG: Ethiopian Health Center Reform Implementation Guidelines; eHMIS: electronic Health Management Information System; EL: E-leadership; EPI: Expanded Programme on Immunization; FP: Family Planning; ICT: Information and Communication Technology; LMG: Leadership, Management, and Governance; OALF: Outpatient Antenatal and Labor Follow-up.
Policy and practice implications
This review positions leadership as a central policy lever shaping governance effectiveness and digital health transformation in Ethiopia's PHC system. The predominance of transformational leadership, complemented by adaptive and transactional practices, supports the institutionalization of hybrid leadership models within national strategies such as HSTP-II and the Information Revolution Roadmap. Leadership expectations should be operationalized through competency frameworks, performance indicators, and enforceable accountability mechanisms.
Leadership development should transition from fragmented training initiatives to professionalized pathways embedded in pre-service education, career progression, and accreditation systems, integrating transformational, adaptive, and e-leadership competencies. Despite widespread implementation of DHIS2 and eHMIS, limited digital leadership constrains the use of data for learning, accountability, and strategic decision making. Addressing passive leadership, strengthening merit-based appointments, and advancing gender-equitable leadership pipelines are essential for building resilient, inclusive, and digitally enabled health systems in Ethiopia and comparable LMICs.
Strengthening the link to planning and policy frameworks
Strategic leadership in Ethiopia's health sector shapes resource allocation, decentralization, and digital policy design. Transformational, adaptive, and e-leadership practices enable fairer distribution of resources, strengthen local decision making, and accelerate digital health adoption. Lessons extend beyond Ethiopia, offering cross-country relevance for low-resource systems seeking effective governance and sustainable reforms.
Resource allocation
Transformational leadership can institutionalize evidence-based priority-setting, ensuring resources are directed toward primary care and equity-focused programs rather than fragmented projects.
By motivating staff and fostering trust, it increases efficiency in budget utilization, aligning with Ethiopia's HSTP-II financing reforms.
Decentralization
Adaptive leadership empowers district health offices to make context-specific decisions, critical for Ethiopia's decentralized health governance.
This reduces bottlenecks from central ministries and supports more responsive, accountable service delivery, a core principle in WHO's health systems strengthening agenda.
Digital policy design
E-leadership enables policymakers to integrate digital dashboards (DHIS2 and eHMIS) into routine governance, shifting policy from reactive to data-driven.
By mainstreaming digital literacy into leadership training, Ethiopia can operationalize its Information Revolution Roadmap, moving beyond pilot projects to system-wide adoption.
Cross-country relevance
Rwanda's digital leadership training and equity-driven planning can guide Ethiopia in strengthening data-informed resource allocation for UHC. Nigeria's community-led leadership illustrates participatory governance, enabling local ownership and context-sensitive policy. Adapting these practices, Ethiopia can integrate digital competencies with community engagement to enhance system responsiveness, equity, and leadership effectiveness.
Conclusion
This scoping review synthesizes evidence on leadership styles shaping Ethiopia's public health system between 2015 and 2024 and demonstrates that transformational leadership, often integrated with adaptive practices, remains the most influential and stabilizing approach. It contributes to improved health workforce motivation, accountability, and service quality, while transactional leadership plays a supportive role through performance monitoring and compliance mechanisms. In contrast, passive leadership is consistently associated with weak governance, low staff engagement, and suboptimal service delivery.
These patterns align closely with guidance from the WHO, World Bank, African Union, and UNICEF, which emphasize that effective leadership is inseparable from governance capacity, equity, and system-wide coherence. The findings reinforce global and LMIC evidence that leadership effectiveness depends not only on individual competencies but also on institutional support, accountability mechanisms, and inclusive decision making structures within decentralized health systems.
Importantly, the review identifies e-leadership as an emerging but under-institutionalized domain. Although digital systems such as DHIS2 and eHMIS are widely deployed, leadership capacities for strategic digital transformation remain limited. The evidence supports a transition toward hybrid, digitally ready leadership models that integrate transformational, adaptive, transactional, and digital competencies. Institutionalizing these models within national leadership development frameworks is critical for building resilient, equitable, and digitally enabled PHC systems in Ethiopia and comparable LMIC contexts.
Strengthen and limitations of the study
Strengths
Comprehensive evidence synthesis: The study systematically reviews Ethiopian public health research from 2015 to 2024, providing a detailed, up-to-date mapping of leadership in digital health.
Theoretical integration: By applying the FRLM alongside adaptive and e-leadership constructs, the study offers a robust conceptual lens rarely used in LMIC contexts.
Policy relevance: Findings directly inform Ethiopia's digital health reform agenda, highlighting leadership as a critical enabler of UHC and system resilience.
Focus on governance and equity: The review emphasizes how leadership shapes accountability, data use, and decentralized decision making, bridging gaps between technology, management, and sociotechnical change.
Limitations
Evidence constraints and scope of available studies
The review relies on published and accessible gray literature, which may underrepresent informal, unpublished, or practice-based leadership initiatives and digital health interventions. In addition, the final number of included studies (n = 11) is relatively small, reflecting the limited availability of empirical research explicitly linking leadership styles with digital health transformation in Ethiopia's PHC system. This constrained evidence base should be interpreted as an important research gap rather than a methodological weakness of the review.
Context specificity and rural underrepresentation
Findings are largely Ethiopia-specific and may have limited generalizability to other LMIC settings with different health system structures and governance arrangements. Moreover, rural PHC contexts are underrepresented in the included studies, despite rural populations constituting the majority of health service users in Ethiopia. While some district- and system-level studies indirectly captured rural facilities, there remains a lack of explicit empirical evidence examining leadership practices in rural and remote PHC settings, highlighting a critical equity and research gap.
Variable study quality and analytical depth
Included studies vary in methodological rigor, and many provide descriptive rather than analytical insights, limiting causal inference. The predominance of cross-sectional designs and self-reported data further constrains the ability to assess leadership effects longitudinally or to establish robust causal pathways between leadership styles and digital health outcomes.
Limited measurement of adaptive and e-leadership
Empirical evaluation of adaptive leadership and electronic (E-) leadership competencies remains sparse, potentially underestimating their influence on digital health outcomes. This limitation reflects broader conceptual and measurement challenges within the digital health leadership literature, particularly in LMIC PHC settings.
Policy recommendations
Implementation logic
To move from policy aspiration to execution, leadership reform for digital health should be implemented in sequenced stages and differentiated across system levels. Ethiopia's decentralized PHC system and uneven digital maturity require phased actions that align national stewardship with regional adaptation, district execution, and facility-level practice.
Short-term actions
National level (MoH):
Define and endorse a national digital leadership competency framework, embedded within existing leadership and governance guidelines (not as a parallel structure). Integrate adaptive and digital leadership modules into ongoing national leadership programs linked to HSTP-II and the Information Revolution Roadmap. Issue policy directives requiring routine use of DHIS2 and eHMIS data in management and performance review processes, shifting digital systems from reporting tools to leadership instruments.
Regional and district levels:
Provide targeted in-service training for managers on data interpretation, adaptive problem-solving, and digital supervision. Strengthen review meetings and supportive supervision by explicitly linking decisions to digital evidence.
Facility level:
Promote distributed leadership practices, including mentoring, coaching, and team-based problem solving around digital workflows. Use transactional tools selectively (dashboards and scorecards) to reinforce learning and accountability rather than compliance alone.
Medium-term actions (3–5 years): Institutionalization and scaling
National level:
Institutionalize digital leadership within pre-service and in-service curricula for public health, health management, and clinical leadership training. Align leadership appraisal, promotion, and retention criteria with demonstrated competencies in adaptive leadership, equity, and digital governance. Strengthen national stewardship roles for interoperability, cybersecurity, and digital trust, ensuring leadership accountability beyond system deployment.
Regional and district levels:
Establish district-level leadership learning hubs for peer learning, coaching, and iterative problem-solving. Increase managerial decision space by decentralizing selected operational and data-use authorities.
Facility level:
Designate digital leadership focal persons within management teams to support data quality, feedback loops, and staff engagement. Strengthen gender-responsive leadership pipelines, addressing structural barriers faced by women and underrepresented groups.
Long-term actions (5 + years): System maturity and sustainability
National and system-wide:
Professionalize health leadership cadres through merit-based appointments, certification pathways, and continuous professional development. Embed digital leadership and equity indicators into national M&E frameworks, explicitly linked to UHC performance. Eliminate passive leadership practices through strengthened accountability, performance contracts, and oversight mechanisms. Promote learning-oriented governance cultures, where digital systems enable innovation, adaptation, and trust.
Policy relevance and alignment
These staged and multilevel recommendations align with HSTP-II, the Information Revolution Roadmap, Digital Ethiopia 2030, and WHO and World Bank guidance. By sequencing reforms and clarifying responsibilities at each system level, the recommendations move beyond descriptive guidance toward implementable policy action.
Implications for future research
Measurement of leadership competencies
Future studies should develop, validate, and apply standardized tools to measure adaptive and e-leadership competencies within LMIC digital health contexts. Such tools should be context-sensitive, linked to governance functions, and capable of capturing leadership behaviors across system levels.
Longitudinal and intervention research
Longitudinal and quasi-experimental studies are needed to establish causal relationships between leadership practices and digital health outcomes over time. Leadership training, coaching, or governance interventions should be evaluated using before–after or comparison designs to inform policy scale-up.
Contextual and comparative analyses
Comparative research across Ethiopian regions and peer LMICs should examine how sociopolitical, cultural, and infrastructural contexts shape digital health leadership effectiveness. Such analyses can identify transferable strategies while respecting contextual specificity.
Integration with health system performance metrics
Future research should explicitly link leadership behaviors to system-level outcomes, including data use for decision making, accountability mechanisms, equity indicators, service quality, and UHC progress. This linkage is essential for translating leadership research into performance-oriented policy.
Informal and networked leadership
Studies should explore informal, distributed, and networked leadership dynamics, including community-level and frontline leadership, which often shape digital health adoption and sustainability but remain under-documented.
Interdisciplinary and sociotechnical approaches
Combining health systems research, implementation science, and sociotechnical frameworks will strengthen understanding of leadership in complex digital transformations and support theory-informed, practice-relevant evidence generation.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261427507 - Supplemental material for Advancing leadership capacities in Ethiopia's digital health transformation: A scoping review using the integrated leadership model
Supplemental material, sj-docx-1-dhj-10.1177_20552076261427507 for Advancing leadership capacities in Ethiopia's digital health transformation: A scoping review using the integrated leadership model by Ibsa Mussa and Rabelani Dagada in DIGITAL HEALTH
Footnotes
Abbreviations
Acknowledgements
The authors would like to acknowledge the University of South Africa (UNISA) for providing the necessary resources and institutional support that enabled the preparation of this report and the compilation of the manuscript. The authors also acknowledge the use of ChatGPT (OpenAI, GPT-5), which assisted with grammar editing.
Ethical approval
All sources were secondary, and ethical clearance was not required under UNISA Policy on Research Ethics (2024, Sec. 7.5).
Consent for publication
Not applicable.
Author contributions
All authors contributed to the conception and design of the study, including the development of the proof outline. IM and RD co-authored the initial draft of the policy brief. All authors reviewed the findings, and participated in revising the policy brief. IM supervised the overall study process. All authors read and approved the final version of the policy brief for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability Statement
The original contributions presented in the study are included in the article/supplementary files, further inquiries can be directed to the corresponding author. All extracted data and study-level coding are available in Supplemental File 1/OSF DOI.
Reflexivity statement
The authors of this article are based in Ethiopia and bring interdisciplinary expertise in public health, digital transformation, and equity-focused health systems research. The lead author is a male public health specialist and early-career researcher based in Ethiopia with extensive experience in digital health policy and equity analysis. The co-author is a senior male scholar specializing in digital transformation and systems leadership in Southern Africa. While both authors identify as male and are based at African institutions, the research emphasizes inclusivity through its methodological focus on marginalized populations (e.g. rural women, persons with disabilities, and pastoralist communities). Future collaborations will seek to strengthen gender and geographic diversity in research teams to better reflect the populations studied.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.