
Abstract
Connected Health is an emerging and rapidly developing field which has the potential to transform healthcare service systems by increasing its safety, quality and overall efficiency. From a healthcare perspective, process improvement models have mainly focused on the static workflow viewpoint. The objective of this article is to study and model the dynamic nature of healthcare delivery, allowing us to identify where potential issues exist within the service system and to examine how Connected Health technological solutions may support service efficiencies. We explore the application of social network analysis (SNA) as a modelling technique which captures the dynamic nature of a healthcare service. We demonstrate how it can be used to map the ‘Careflow Network’ and guide Connected Health innovators to examine specific opportunities within the healthcare service. Our results indicate that healthcare technology must be correctly identified and implemented within the Careflow Network to enjoy improvements in service delivery. Oftentimes, prior to making the transformation to Connected Health, researchers use various modelling techniques that fail to identify where Connected Health innovation is best placed in a healthcare service network. Using SNA allows us to develop an understanding of the current operation of healthcare system within which they can effect change. It is important to identify and model the resource exchanges to ensure that the quality and safety of care are enhanced, efficiencies are increased and the overall healthcare service system is improved. We have shown that dynamic models allow us to study the exchange of resources. These are often intertwined within a socio-technical context in an informal manner and not accounted for in static models, yet capture a truer insight on the operations of a Careflow Network.
Keywords
Introduction
The world around us is changing dramatically through the use of technology, both hardware and software. It is not unusual in many of our everyday environments to use smart phones, Internet, mobile technology, integrated software systems and ubiquitous computing. This has resulted in systematic changes in how people undertake everyday activities. Within a healthcare context, the growth of health technology, digital media and mobile devices has contributed towards technology-enabled care. 1 Data are now exchanged across personal and professional technology platforms, for example, via smartphones apps, biosensing wearables or healthcare monitors. 2 As these can provide real-time healthcare information, they can ultimately facilitate improved healthcare quality outcomes. 3 This has given rise to the emergence of Connected Health (CH) – a new socio-technical model for healthcare management which exploits the use of information technology (IT) for clinical or wellness decision-making tasks. 4 CH software innovation contributes towards the coverage and quality of healthcare services, improved health outcomes, reduced costs and improved quality of care (QoC).
Research question
Our research has indicated that in order to improve a healthcare service, we must successfully model the network in which the service operates. This allows us to assess where improvements may be made and examine whether improvements actually occurred due to innovation enabled by IT. Failing to do so can hamper efforts to clearly align healthcare needs and software development. Within a healthcare context, this is often overlooked and has not been addressed. Thus, to address this gap, we formulate the following research question: How can we model the connectedness of a Careflow Network to identify potential service bottlenecks and opportunities for Connected Health solutions? This article addresses this question using social network analysis (SNA). We describe how it presents significant potential to model Careflow Networks and how it supplements other existing modelling techniques.
Research methods
Literature review
We conducted an exploratory literature review to examine the concept of a healthcare system and careflow systems. For example, the objective of this exploratory research was to gather preliminary information to support the definition of the problem in modelling healthcare systems and to suggest how SNA can offer a suitable approach to capture the dynamic nature of Careflow Networks. Within the literature review process, we identified that there is a need to model the dynamic interaction within a healthcare service, for example, the exchange of healthcare resources between actors. We explored current modelling techniques and network properties within the Careflow Network, and our resulting thesis is that Social Network Analysis (SNA) is a suitable tool to model a Careflow Network.
Case study
To illustrate our thesis, we present a hypothetical scenario within a case study as a particular instance within a Careflow Network. We provide a scenario and describe how the interactions within the Careflow Network can be easily replicated in a real-work context. Our objective here is simply to demonstrate the potential of employing SNA to model the connectedness of a Careflow Network and to identify potential service bottlenecks and opportunities for CH solutions.
Careflow systems
There are ample sources of literature which explain how clinical guidelines describe the activities of a medical team in a comprehensive manner for the purpose of defining best practice for patient management. Within clinical guideline literature, the concept of ‘careflow’ largely focuses on behavioural aspects of medical practice with increasing attention on possible IT-enabled support solutions.5–8 These are often referred to as ‘careflow systems’ which implement workflow concepts in the clinical domain. 6 Workflow involves the coordinated execution of multiple tasks performed by different agents to handle the delivery of a healthcare service as effectively and efficiently as possible. Thus, workflow defines, executes and automates specific processes where tasks, information or documents are passed from one participant to another for action, according to a set of procedural rules. 9 These rules are often based on the presumption, represented in healthcare guidelines, of how healthcare professionals formally interact with one another. However, there is an obvious lack of a service boundary due to the complex nature of a healthcare system. 10 In addition, to date, there are few efforts which map the real-world dynamics of healthcare services to truly capture the interactions (formal and informal) of healthcare actors and to identify (a) how connected actors are and (b) identifying where technology is best placed within the Careflow Network to alleviate healthcare bottlenecks.
Careflow Network
We define a Careflow Network as the interaction within a healthcare service structure that facilitates the exchange of resources and competencies between actors through defined care pathways in order to achieve quality and safe patient outcomes (Figure 1). Building on careflow systems literature, we introduce the concept of a Careflow Network to emphasise the need to map the interactions which sustain the provision of healthcare services before we can attempt to provide effective IT solutions. The difference between careflow systems and Careflow Network is that Careflow Networks shed light on the real-world interactions which exchange healthcare resources (e.g. information, medicines or support) rather than simply focusing on the formalised workflow approach to identify where linear process execution could be supported through IT. The Careflow Network approach goes beyond the ‘traditional’ view of healthcare, where a patient interacts with a clinician only. We consider all meaningful dynamic interactions, some of which will be supported by technology and some that often goes undocumented on a day-to-day basis. Thus, we need to introduce applicable modelling techniques to capture these healthcare dynamics.
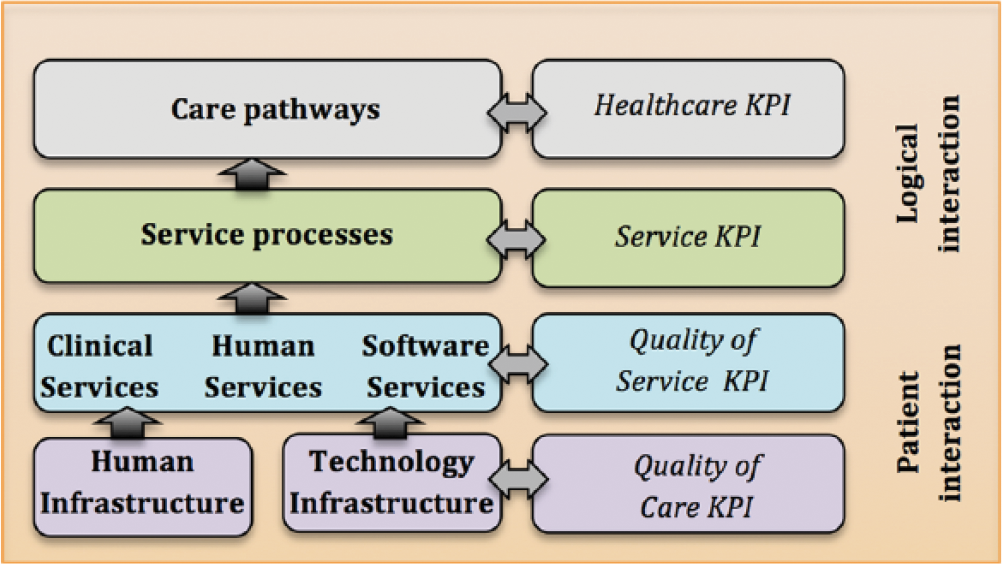
Key layers of a Careflow Network.
Figure 1 illustrates the key layers of a Careflow Network which are linked to different performance measures or key performance indicators (KPIs). The Careflow Network comprises the following:
Care pathways. The main tools used to manage healthcare quality concerning the standardisation of care processes. This layer focuses on the clinical services of other layers and describes clinical practice. It also establishes healthcare KPIs to assess the overall healthcare service performance.
Service processes. Deliver valuable capacities for action to a particular client/patient. This layer also focuses on the logical interactions of other layers and identifies service KPIs to indicate where strengths and opportunities exist to enhance the overall service.
Clinical services. Provides services relating to the medical treatment that are provided to patients to treat a medical problem. This layer focuses on the patient interactions from a clinical, human and software service perspective to assess quality of service (QoS) KPIs.
Human services. Provides an interdisciplinary approach to meeting healthcare needs through an applied knowledge base, focusing on prevention as well as treatment of healthcare conditions to improving the overall quality of healthcare service through various skills. It sheds more insights on how these services contribute towards QoS KPIs.
Software services. Executes services guided by a set of related software functionalities that can be reused for different purposes to support practice and policies. It supports other related services to enhance the QoS KPIs.
Human service infrastructure. Defines the social service structure of a healthcare network which is sustained by social networks to deliver a healthcare service. It provides some insight on how various health-related and non-health-related services contributes towards QoC KPIs.
Software service infrastructure. Focuses on the business rules of the healthcare environment, for example, a service-oriented infrastructure to support the enterprise, the application architecture and the infrastructure via a pool of resources (web servers, application servers, database servers, servers, storage instances). It explores both strengths and opportunities on how these services contribute towards QoC KPIs.
Defining KPIs ensures that performance across each layer directly impacts on the other layers. This ultimately supports the provision of care through defined care pathways, for example, QoC, quality of experience (QoE), process performance, service performance and healthcare performance. Of particular interest is the connectedness between the various layers and how the healthcare stakeholders interact to sustain a healthcare service. We contend that the human service infrastructure layer offers us a very important insight into this and argue that there is a need to understand the human infrastructure before we can design software solutions within a healthcare context to support the connectedness of healthcare services.
Applicable modelling techniques
Through the concept of the Careflow Network, we capture healthcare dynamics and build on the characteristics of modelling techniques such as workflow, resource flow, clinical pathways, social networks and careflow management systems which can assess healthcare environments:
Workflow. A defined pattern of activity enabled by the systematic organisation of resources into processes that is, defined, executed, registered and controlled processes. 11 However, as identified by Krogstie 12 (p. 65), the problem is not formality in workflow modelling, but the lack of interaction whereby ‘a model must be formally complete to prevent ambiguity and deadlock from paralysing the process’. Within a healthcare context, this does not capture the nature of healthcare systems.
Resource flow. Links among and within organisations which define the environment as a network flow of resources (i.e. valued activity, service or commodity) over a specific period of time. 13 This is largely used in organisational studies to capture the main formal resources considered, that is, money, information and support. 14 Based on this insight, we are reminded of the three main patterns of information flow identified by Galaskiewicz and Marsden: 15 symmetry in which bidirectional information flow within a channel; exchange in which bidirectionality is supported through the use of different channels; and multiplexity in which information flows unidirectionally in multiple channels. Within a healthcare context, communication is multifaceted which can be guided by formal healthcare guidelines and exchanged through informal networks of healthcare professionals.
Clinical pathway. A standardised multidisciplinary plan of care which executes care processes within a specific timeframe which reduces the variability in clinical practice and improves outcomes. 16
Social network. A social structure comprising a set of social actors (e.g. people or healthcare institutions) and a set of the dyadic ties (or interactions) between these actors. 17
Careflow management systems. A system which defines, creates and manages the execution of careflows to improve performance in delivering to administer, support and monitor the execution of healthcare services through the use of software according to a process definition. 7
At a more simplistic level, Jun et al. 18 provides an overview of some of the key healthcare modelling techniques (Table 1). Healthcare requires dynamic interactions between a patient and healthcare professionals (i.e. careflow) throughout the patient’s journey that is supported through various resources being exchanged within a network. This exchange process is of particular interest if we are to truly understand and capture the provision of care within a Careflow Network.
Overview of modelling techniques.
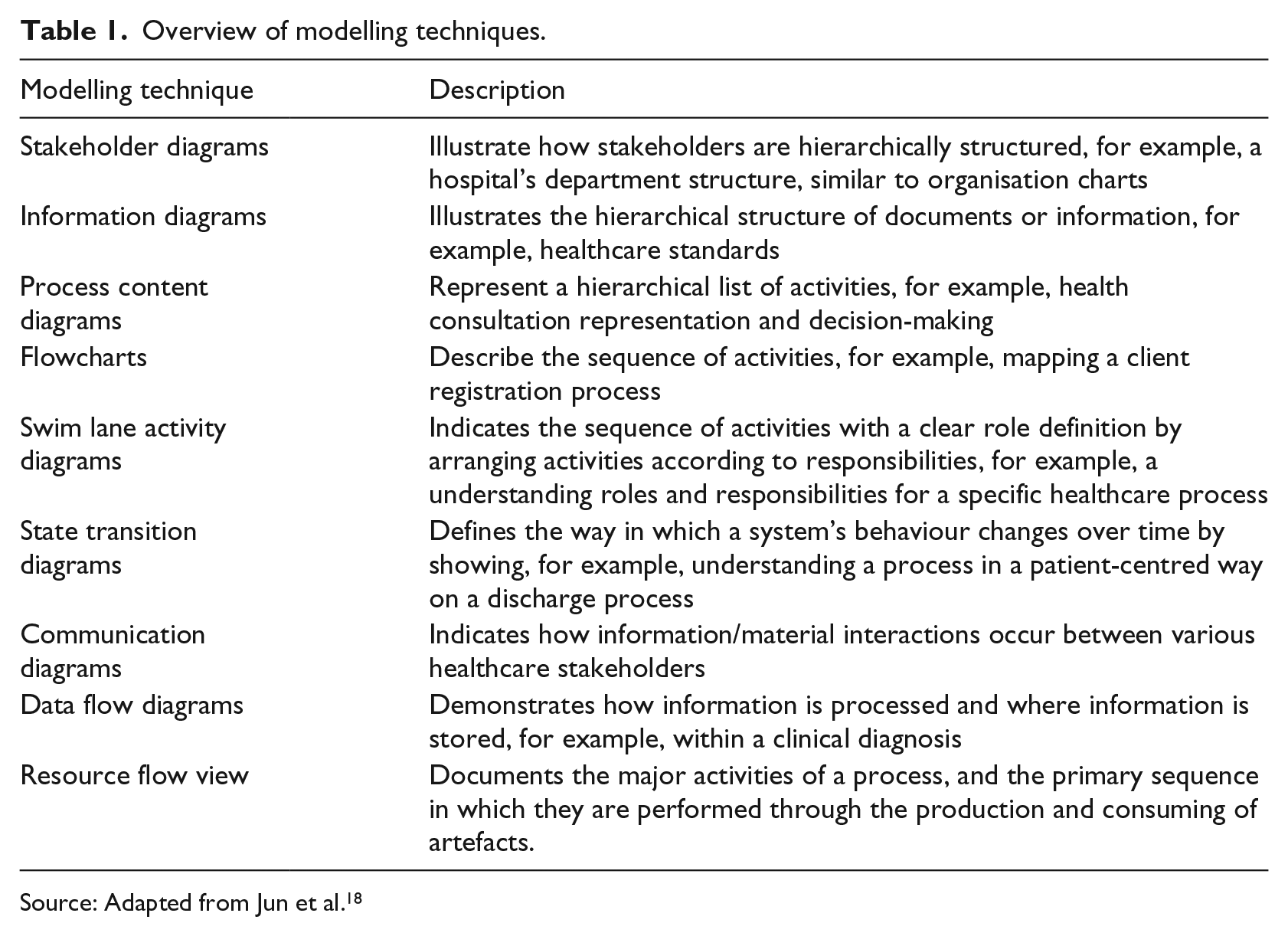
Source: Adapted from Jun et al. 18
The connectedness of healthcare services
A key concept a Careflow Network builds on the ‘connectedness’ of technological enabled solutions to provide various healthcare services. 19 Given that there is a growing interest in examining how IT is used within such networks,20,21 Careflow Networks will play a critical role in sustaining evolving partnerships between all healthcare service system stakeholders.22,23 To truly assess the impact of technology, we must identify suitable techniques to model Careflow Networks within existing healthcare systems. A healthcare system may be described as the organisation of people, institutions and resources that deliver healthcare services to meet the health needs of society. Thus, healthcare comprises of an extremely diverse group of people who interact with one another to deliver a service. 24 These include the following:
Patients with a known condition;
Patients at risk of various healthcare conditions;
Family members or friends concerned about patient wellbeing;
Persons interested in their personal wellness;
Informal carers who comprise of family members and neighbours providing voluntary care;
Formal carers such as homecare assistants who provide care as part of their profession;
Clinicians in the community such as public health nurses, general practitioners (GPs), social workers, physiotherapists;
Clinicians within the hospital setting such as specialist consultants, nurses, radiographers.
Healthcare (non-clinical) support services including, for example, administration, suppliers, buildings and maintenance.
In addition, when we refer to services, a service may be described as the end product of human assemblage, knowledge, innovation, interaction and consumption. 25 Within a healthcare context, people also interact with non-human elements to facilitate healthcare provision services which include medical devices (e.g. X-ray machines or cardiographs) and information sources (e.g. patient records or NICE standards (https://www.nice.org.uk/standards-and-indicators)). The interactions that exist between socio-material elements (humans and non-humans) may be described as the relational infrastructure, 17 whereby collaboration between actors supports the exchange of resources and competencies, for example, healthcare information. 26 To uncover the dynamics of the relational infrastructure, the connectivity of various stakeholders within the health management system can reveal insights on the healthcare system. 27 For example, it can inform us how the healthcare network is structured, who or what are the most influential/powerful stakeholders, 27 what is the resource flow and where are the service bottlenecks. 24 Understanding and analysing the relational infrastructure can present opportunities of where technology could potentially optimise healthcare service operations to support a healthcare ecosystem. Thus, while there are some existing modelling techniques which apply to certain context, their application to examine the relational structure of a Careflow Network is inadequate. Rather than just focusing on technical flows, the shifting socio-material assemblages of service dynamics should also be presented. What is interesting here is the idea that one can map the, what is often considered ‘invisible’,28,29 relational infrastructure to visualise the exchange of resources and patterns of interactions17,28, and explain that there needs to be increased efforts to ‘delayer organisations and reduce functional boundaries, coordination increasingly occurs through networks of informal relations rather than channels tightly prescribed by formal reporting structures or detailed work processes’ (p. 25).28 We explore this within a Careflow Network context in our research question.
Key findings and analysis
Our literature review on modelling techniques indicated how various representations of a real-world system are used to address a specific question. To understand, for example, information flows and network elements, service networks are typically viewed through process models. However, these often fail to capture the real-world dynamic nature of services exchanging resources and competencies and often remain an underexplored and ‘invisible’ infrastructure. 30
Taking one of the above techniques (outlined in section ‘Applicable modelling techniques’), for example, resource flow model (Figure 2), we can learn how the static modelling techniques fail capture the dynamic nature of healthcare. Undoubtedly, the resource flow view 31 indicates how a nominal sequence of activities is involved in the treatment of a set of symptoms: the patient presents himself to a specialist clinician, an examination is undertaken and after which a diagnosis is made followed by a course of treatment. However, detail in healthcare is of vital importance to quality and safety, yet models such as the resource flow model ‘does not seek to capture every detail and nuance of a knowledge-intensive process. (p. 44). 31 Of course, a model cannot capture ‘everything’, but we will demonstrate how our Careflow Network approach is more effective in capturing healthcare dynamics. Thus, to truly optimise healthcare operations, we must move beyond the resource flow approach and introduce methods which complement and capture interactions within a dynamic healthcare environment. 21 This will ultimately inform us on ‘how’ and ‘where’ healthcare solutions can better support healthcare innovation, clinical practice and patient engagement. 4
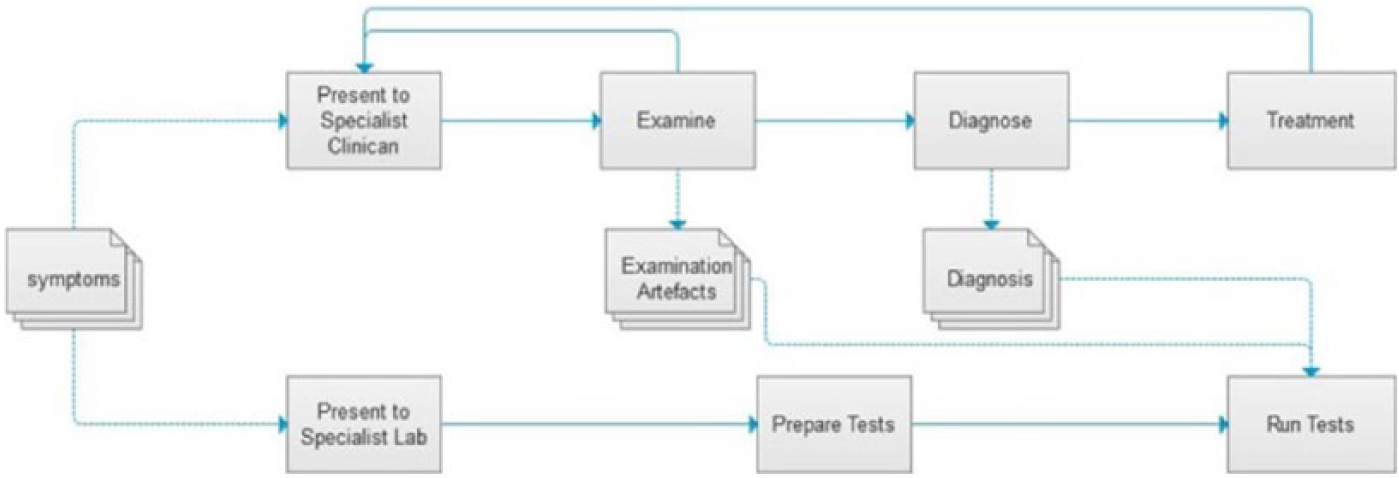
Resource flow model.
It has been claimed that organisational managers have ignored the ‘dynamic characteristics of networks and the ways that dynamic qualities of networks affect organisations’ flexibility and change’ (p. 133). 29 This is also witnessed in healthcare, that is, how care is delivered 32 and how networks hinder the adoption of healthcare change. 33 This has unavoidably led to organisations such as hospitals failing to capture the true operations of their service networks performance (e.g. behavioural, functional, compositional and structural) and the overall contributory value of service linkages (i.e. relational structures).
Principles of a social network
SNA is the study of social relations among a set of actors, 34 for example, people, groups, organisations or computers. The nodes within the network represent the people and groups under investigation, while the links demonstrate the relationships or flows between the nodes. Thus, SNA offers a specific approach and set of techniques that supports the study of resource exchanges (e.g. information) among actors. 17 There is a large body of literature which suggests that SNA presents a unique method to model and monitor the interactions and potentially contributory value of actors within a service network such as healthcare,17,30,34 –41 all of which direct our attention to the need to understand the principles of a network before we can begin to understand and/or improve the network under investigation. These network principles offer us a lens to view healthcare service operations that is, viewing Careflow Networks as a network of interconnecting elements that sustain a specific structure, bound by various interactions to deliver a healthcare service (Table 2).
General principles of a network.
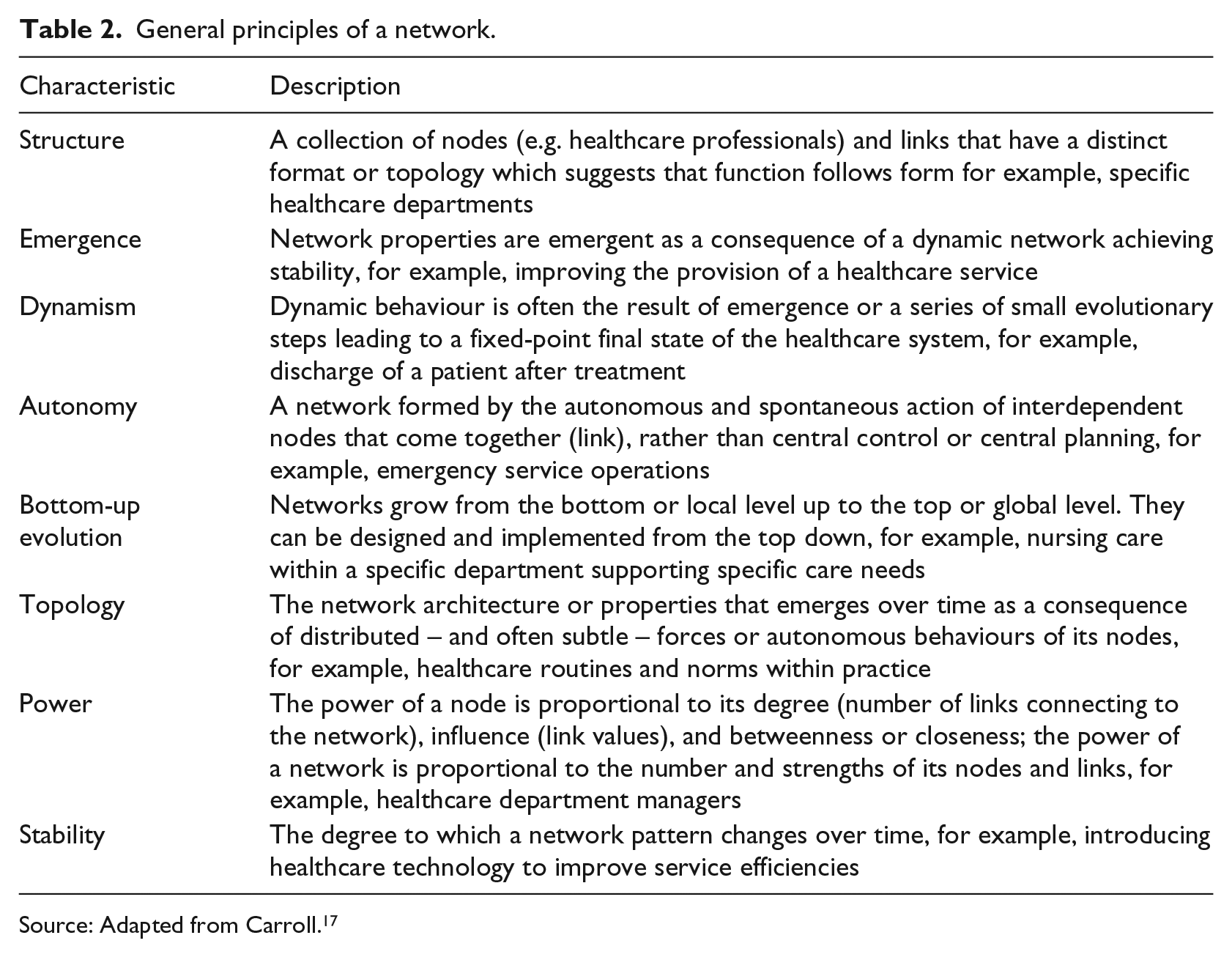
Source: Adapted from Carroll. 17
Why SNA?
A social network is a set of actors (or nodes) that supports some form of relationship (or edges, or ties) with another node. 28 In a Careflow Network, these actors include stakeholders such as patients, carers, GP, physiotherapists, healthcare administration, community carers, formal/informal carers and social carers. Therefore, to exploit the potential of SNA, it is important to define what actors comprise the network and to develop an understanding of the Careflow Network under investigation. This provides a comprehensive and rigorous description of a pattern of social relationships to support our analysis. 17 Often, it is difficult to fully appreciate how connected a social network is within a specific population,28,29 but there are a number of techniques to support us identify the ‘boundaries’ of a specific network and to define the social network. From this, we can begin to identify emerging patterns of social structure. This is particularly important to enable us to visualise Careflow Network patterns or graphs and offers us a suitable approach to illustrate the connectedness of a healthcare service system, identify inefficiencies and explore opportunities to integrate technological innovation. Using formal methods to represent a social network is achieved through mathematical software applications to analyse the network data and derive structural analysis. From a clinical, technology, social science and business perspective, the results from such analysis present us with the structures of a Careflow Network. SNA can provide answers towards descriptive and exploratory research questions to provide empirical findings regarding the networks structures. Visualising healthcare interactions has the potential to offer us a real insight on how a healthcare service truly operates as opposed to how it ‘ought’ to work. To achieve this, SNA can assist us in examining the relational structures of a Careflow Network environment, providing us with a lens to examine the socio-technical entities. SNA software is vital to support the visualisation and relational descriptions of the Careflow Network. This approach also complements what Spohrer and Maglio 42 describe as the importance of implementing new modelling methods in modern service environments and the intertwining complexity and dynamic configuration of people, knowledge, activities, interactions and intentions that creates and delivers value. We explain the motivation of this through the potential application of SNA to Careflow Networks.
The connectedness of Careflow Networks
A dynamic healthcare environment involves various stakeholders at different organisational levels, yet many of the modelling techniques to map healthcare behaviour provide a rather static view of healthcare systems. 43 Careflow Networks reproduce and embody the complex interplay of professional, healthcare, technical, economic and political factors. Thus, the involvement of multiple factors in healthcare systems has made IT-based healthcare systems expensive, competitive and complex. 44 The deployment of different programming languages, platforms and data management standards has led to restrictions in flawless exchange, integration and reuse of information across different systems. 44 Therefore, modelling healthcare and its dynamics is a critical first step to understand the healthcare environment and its behaviour. Building on our Careflow Network concept, we revisit 38 and examine the network concepts and network properties as summarised in Table 3. These are also considered fundamental to Careflow Network dynamics.
Social network analysis concepts and network properties.
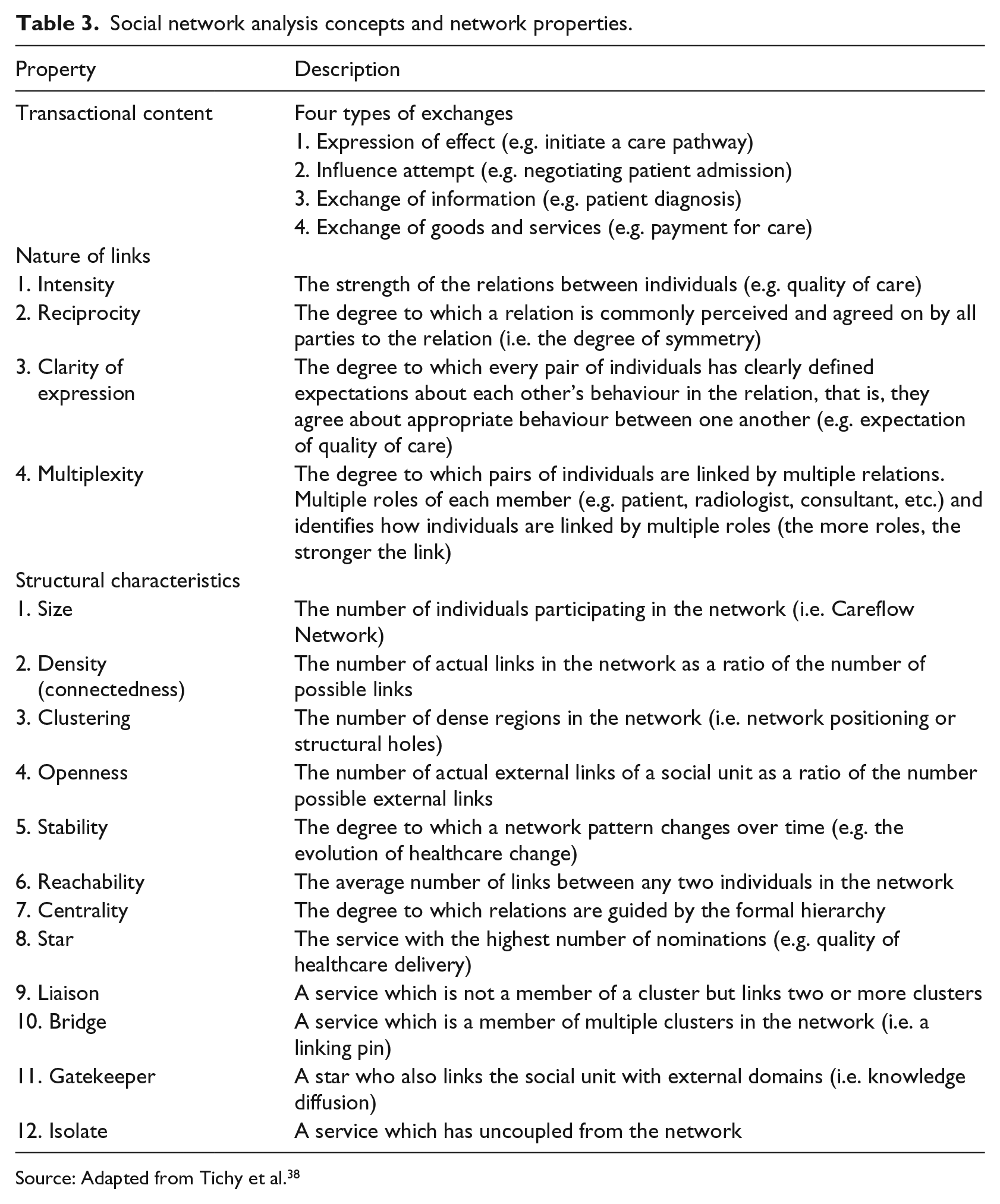
Source: Adapted from Tichy et al. 38
SNA can be employed as a technique to graphically represent and visualise service relational structures. More importantly, SNA is an approach and set of techniques which can assist in to study the exchange of resources and competencies. The nature of the links considers the strength and qualitative nature of the relation between two or more actors or nodes. The structural characteristics examine the overall pattern of relationships between the actors, for example, clustering, network density and special nodes on the network are all structural characteristics. Watts and Strogatz 45 report that real-world networks are neither completely ordered nor completely random, but rather exhibit properties of both. In addition, they claim that the structure of a network can have dramatic implications for the collective dynamics of a system, whose connectivity the network represents, and that large changes in dynamic behaviour could be driven by even subtle modifications to the network structure. Therefore, the orchestration of structural relations (emergent property of the connection, for example, the exchange process) or attributes (intrinsic characteristics, for example, value of an exchange) become a central factor to analyse a network’s structural properties. This complements what one might describe as the connectedness of Careflow Networks which contributes towards delivering healthcare services. The properties of a network listed in Table 3 provide us with a new vocabulary to develop Careflow Network metrics, for example, the intensity of links, the structural size of the network, the stability of a network, the key actors who act as a bridge within a network. Gathering this information requires a specific methodology, which can be executed across the healthcare community within a specific context and identify key factors that influence the Careflow Network dynamics.
Scenario: examining Careflow Network operations
A Careflow Network may comprise of hundreds or thousands of actors including home, family, friends, community, hospital, healthcare professional and social care. Therefore, defining the network and its boundary will influence the data gathering process. In this section, we demonstrate how SNA can be used to model the Careflow Network.
Through this hypothetical scenario, we examine one set of actors within a socio-matrix, which are linked through various relationships at a specific period of time. Table 4 provides the simple view of a traditional healthcare service which captures the healthcare professional’s interactions in order to deliver quality care for a patient, Noel, a 60-year old who has broken his leg. When he engages in the clinical pathway, he interacts with a number of actors. Initially, Julie, his GP, performs a diagnosis and informs him that he must undergo an X-ray. To do so, he must visit the hospital and interact with various healthcare professionals (listed as follows):
John, the porter, for assistance, for example, provision of a wheelchair;
Mary, the receptionist, to sign healthcare documents and ensure insurance coverage is adequate;
Joe, the consultant, who diagnoses the specific injury and prescribes the treatment plan;
Susan, the student doctor, who refers Noel to a radiologist to identify the extent of the breakage;
Pat, the radiologist, who conducts the X-ray on Noel;
Susan, the doctor who places a plaster cast on Noel’s leg;
Sean, the physiotherapist, who instructs Noel on various rehabilitation procedures and exercises;
Frank, the homecare provider, who checks in on Noel every week to check on his progress;
Julie, the GP who re-examines Noels progress and recovery once every month for 3 months.
Example of a simple socio-matrix demonstrating the impact of a Connected Health (C) solution on the Traditional Healthcare system (T).
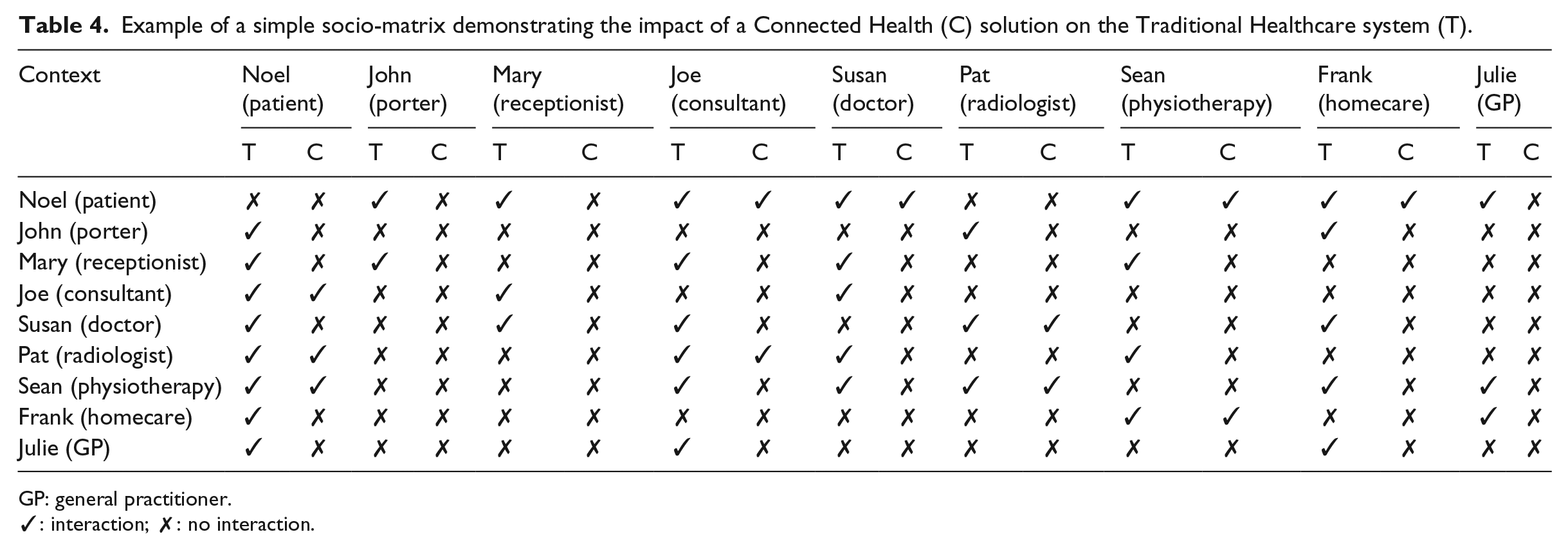
GP: general practitioner.
✓: interaction; ✗: no interaction.
Capturing this interaction among the actors provides us with a map of the Careflow Network. To do so, we used UCINET (https://sites.google.com/site/ucinetsoftware/home) to map the Careflow Network. Figure 3 represents the actors and their interactions with other healthcare staff in order to successfully complete a specific process (the arrows illustrate the direction of the relationship).
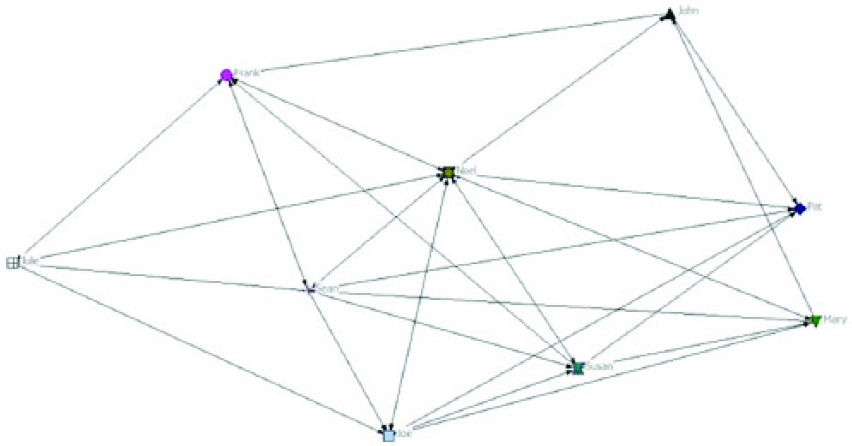
Mapping a traditional Careflow Network.
Discussion on the Careflow Network
Through the hypothetical scenario, we examine one set of actors which are linked through various relationships at a specific period of time which provides a socio-matrix. Table 4 provides the simple view of a traditional healthcare service which captures the healthcare professional’s interactions in order to deliver quality care for a patient (i.e. Noel). While this is a small sample to demonstrate the use of SNA, it is important to examine the service network by reaching a sufficient sample size which can be achieved through a survey tool. The survey should capture background information to profile participants, examine with whom a person must interact with to complete a process within the service, explore people’s attitudes or opinions of service operations and identify ideas for change. To support the analysis, it is also a good idea to interview respondents to learn more about the actual relationship between actors. Within a healthcare context, we may examine who is involved with admission, post-admission and discharge of a patient. For demonstration purposes, we merge the traditional healthcare service (T) and Connected Health (C) within Table 4 to highlight the changes in each context, that is, the impact of CH solutions on the Careflow Network. It is worth noting that traditionally, the GP was considered a gatekeeper of healthcare services46,47 within a community context and directed patients to specific services or consultants depending on the nature of the patient’s condition presented to the GP. 48 For the purpose of this study, the CH solution is a technical solution that is envisaged to empower patients to be directly assessed by a doctor (Susan) and then referred to the most suitable service within the Careflow Network. This eliminates the need for a GP (Julie) to interact initially with the patient and then refer a patient to the doctor and later onto a consultant. This can be achieved via an online consultation process with Susan rather than having to go through the traditional face-to-face visit with the GP service and thereby streamlining the healthcare process. However, the focus of this article is to highlight the need modelling techniques such as SNA to generate new insights and analysis to trigger questions on the process flow and process efficiency of a Careflow Network.
The interactions/links within the network are represented using arrows. The SNA offers a clear view of the service operations and provides an overview of the interactions. Mapping the network provides us with an opportunity to visualise the complexity and identify potentially service bottlenecks by investigating social structures. From here, we can begin to identify the network size through the number of actors (nodes) in a Careflow Network. Then, we can assess the density of the network which measures the proportion of all possible ties that are actually present. The density informs about us the efficiency in which information or resources diffuse among the nodes, that is, the more nodes that receive information from multiple others, the network may be described as not ‘efficient’. This may be also as a result of the reachability within a network, that is, average number of links between any two individuals in the network. The reachability informs us whether two actors are connected through either direct or indirect pathways. Such insights can support us in managing or redesigning a care pathway and we can begin to explore efficient ways to deliver healthcare. For example, we can use geodesic distance. This examines the number of relations in the shortest possible path from one actor to another and suggests the most efficient connection between two actors. We could experiment with the inclusion of technology as an additional actor, thus investigating the potential contribution and impact of CH innovation (Figure 4).
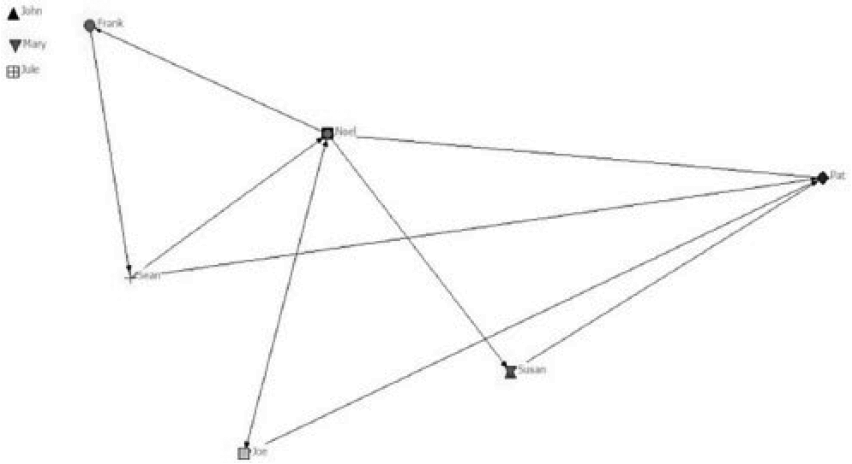
Mapping a Careflow Network with integration of a Connected Health solution.
Our preliminary findings suggest that CH innovation brings about improved healthcare efficiency since the CH solution reduces the density of the Careflow Network, that is, the number of ties which suggest that resources such as information may be received in a more efficient manner. For example, introducing an online appointments system could remove the need for the receptionist and perhaps the porter within this Careflow Network. However, each of these connections can be of different nature. One cannot simply argue that the geodesic distance indicates how two different actors can closely communicate or share information. Patients may value the interaction with homecare staff and have built up a holistic healthcare relationship with them, whereas the consultant may be very disease-focused. This requires further research such as the adoption of ethnography methods and design thinking techniques 4 in order to fully understand the weighting or contribution each actor has on the delivery of care.
When ties are directed, we can calculate the total number of ties sent (out-degree) and ties received (in-degree). The out-degree is typically used to examine the influence. The in-degree may be used to assess the popularity of another node which may represent a QoS, that is, expertise of a doctor. However, the degree centrality does not take into account indirect ties which an actor has. Closeness centrality emphasises the distance of an actor to all others in the network. The degree centrality measures local position, while closeness centrality measures global position. Closeness is indefinite for disconnected nodes and is meaningful only for a connected network. The more dependency placed on a particular actor through various connections (e.g. Joe the consultant), the more powerful the actor becomes within the network.
From a CH perspective, removing some administrative and support actors while introducing a patient platform software solution removes tasks such as porter assistance, reception administration and homecare instruction while offering a more healthcare-focused solution. Such a solution could enable the patient to book an appointment online, locate the consultant’s practice within a hospital building, avail of online support and physiotherapy rehabilitation instructions. Online GP/consultant meetings may also be arranged to achieve greater healthcare efficiencies and community-based care. With the use of SNA, for example, we begin to learn how density represents the proportion of possible relationships in a network that are actually present. A sparsely connected network has fewer links to nodes within the network. By contrast, densely connected networks indicate a more evenly distributed network. However, we may argue that sparsely connected networks offer more patient-centric opportunities, adding greater connectivity to patient care. In addition, the average degree of a node indicates the number of edges connected to it which suggests that the CH solution(s) may offer more efficient and direct solutions to service users. A measure called betweenness centrality is the extent to which an actor falls on the geodesic paths between other pairs of actors in the network. For example, the betweenness measures of Sean’s position post-implementation of the CH solution has decreased compared to the pre-implementation position as there is now less interaction and demand on his service since he can offer a physiotherapy solution online. While removing the need for direct interaction between Noel (patient) and Sean (physiotherapist) via a home-based exercise prescription service and e-learning tool, the evidence base provides both Noel and Sean with a rich insight of Noel’s progress. Adopting such measures and applying them as Careflow Network metrics may enable us to explore the causes of such bottlenecks and examine the potential of applying healthcare technology solutions to enhance the health service efficiency. For example, through introducing new pathway measures, we can calculate total network cohesion. We can compare these measures to determine the impact of CH innovation on a specific network. This type of activity also demonstrates the value of SNA to map a Careflow Network. For example, we visually identify the impact of a CH solution (a patient platform that offers a self-service check-in tool and physiotherapy interactive e-learning tool) on the overall Careflow Network.
Adopting SNA for Careflow Network metrics
A further requirement for efficient modelling is that metrics are provided, and within the Careflow Network, the key focus must be on delivering quality information to support the delivery of quality care. The nature of Careflow Networks is changing rapidly due to the integration of CH innovation. For our scenario, Table 5 presents the density measure using SNA. When comparing two populations (i.e. traditional healthcare and CH) we can identify how many actors are connected in one network and may not be connected to another (‘isolates’). For example, John, Mary and Julie are removed from the Careflow Network (Figure 4, top left of image). We can conclude that, based on interactions, the operations are now very different in the two populations. Measuring the density gives us an index of the degree of dyadic connection in a network. This is important to demonstrate the level of interaction and the resources exchanged between actors. It also highlights the potential service bottleneck and the importance an actor plays within the Careflow Network. Measuring the ties among actors with various values, for example, strengths, closeness, probabilities, density is usually defined as the sum of the values of all ties divided by the number of possible ties. That is, with valued data, density is usually defined as the average strength of ties across all possible ties.
Impact of Connected Health innovation of density of Careflow Network.
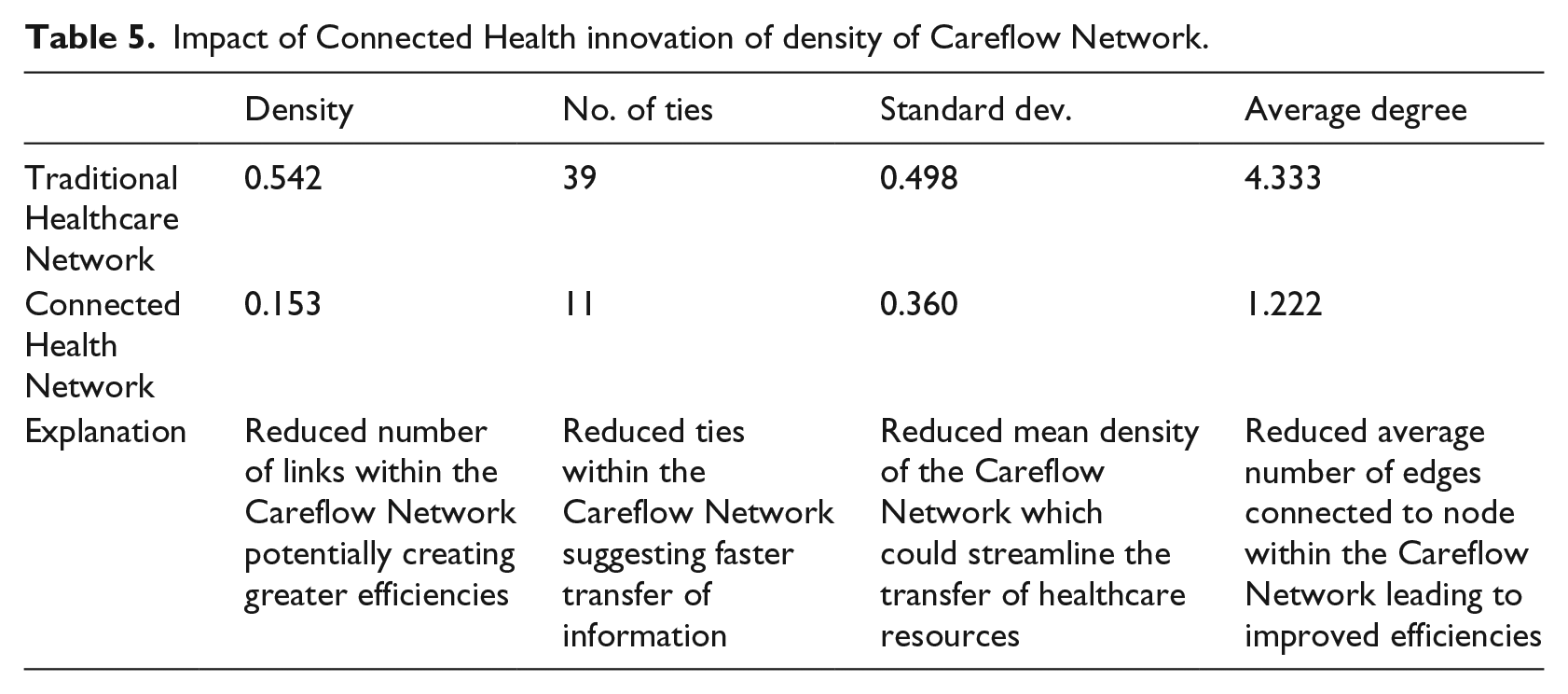
The characteristics of the Careflow Network can provide researchers with the ability to introduce new metrics into CH to support decision-making and derive improved healthcare analytics. Such an approach can provide us with a visual aid to map a healthcare network to understand ‘what the current situation is’ and how tasks are ‘really done’ rather than high-level workflow charts which offer us little insights on the dynamic nature of a healthcare environment. From a Careflow Network perspective, for example, using SNA we can begin to examine how network science measures inform us of Careflow Network behaviour. The SNA technique will provide other measures such as degree of centrality, closeness and betweenness (see Table 3), which may also be employed to assess healthcare service operations and structure. Thus, they will support us in determining the impact of IT to improve operations and/or service structure.
Adopting SNA to model Careflow Networks
Based on this initial exploratory research, we have identified the suitability of applying SNA to map and measure Careflow Networks and develop thorough insights on the connectedness of a healthcare service system. SNA offers a unique approach to model the exchange of various resources to provide a healthcare service. Through its inherent inclusion of resource flow dynamics, SNA can successfully supplement traditional methods of modelling care pathways. It will be useful in providing rich insights on how a health service operates and where the introduction of CH technological innovation may enhance various activities, such as decision-making, within the pathway.
Figure 5 illustrates how different modelling techniques can complement each other when examining care pathways. The resource flow view 31 indicates how a nominal sequence of activities involved in the treatment of a set of symptoms: the patient presents himself to a specialist clinician, an examination is undertaken and after which a diagnosis is made followed by a course of treatment. However, this does not reflect the dynamic nature of healthcare delivery and the level of interaction (formal and informal) that is executed to deliver a particular healthcare service. SNA provides such insights. Implementing a combination of both approaches may also offer a dual lens (or multiple layers) on how Careflow Networks may be modelled in terms of the standardisation of resources and the dynamics of actor interaction.
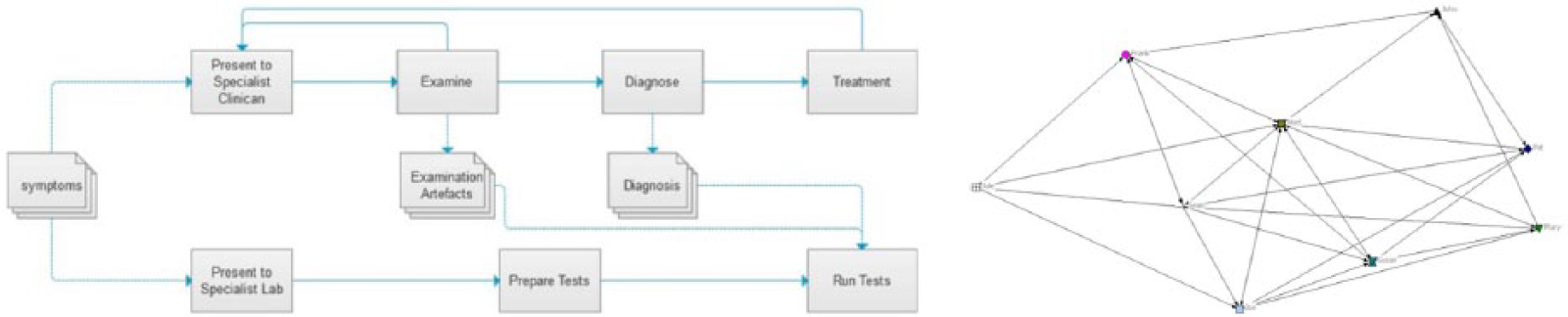
Complementary models: Resource flow and SNA view of care pathway.
Discussion and conclusion
We set out to describe the impact of which CH is having a rapidly developing field that has the potential to transform healthcare service systems by increasing its safety, quality and overall efficiency. However, as part of our research developments, we identified a significant gap to employ suitable models and modelling techniques to capture the dynamic nature of CH. To address this gap, we study and model the dynamic nature of healthcare delivery. This allowed us to identify where issues exist within the service system and to examine how CH technological solutions may support service efficiencies. This study is important for a number of reasons. First, healthcare is a complex service and is increasingly reliant on accurate and timely data and networking. GPs and specialist consult with patients, healthcare teams develop and execute treatment plans, pharmacists review and fill prescriptions, and patients’ research and communicate with peers and it is important to uncover the dynamic interaction within a healthcare system. Second, the Careflow Network is introduced to demonstrate how vast the healthcare system is and relies on numerous actors to interact and provide a healthcare service in many forms. Therefore, a third key contribution of this work includes the application of SNA as a technique to map and explore how we can begin to improve the efficiency of this network with connected technologies with a view to improve healthcare outcomes and quality of life, while reducing costs. Our research supports the need to reconsider how we can design healthcare systems and operationalise Careflow Networks. Specifically, we challenge the need to reconsider how we view a GP as a healthcare service gatekeeper46,47 within a community healthcare context. We support Greenfield et al. 48 analysis on the need to rethink primary care’s gatekeeper role. We suggest that CH solutions can empower patients to self-manage their healthcare while reducing the need for interactions with specific Careflow Network actors. In so doing, this can improve the effectiveness and efficiency of delivering care.
The Careflow Network is a first attempt to develop an understanding as to what the actual network is, who participates, what is its structure, how is formal and informal work undertaken within the network, where are the inefficiencies across the healthcare system exists. Ultimately, this can also influence decisions on whether care pathways can be redesigned. Technology can also be included in this analysis. Networked devices and healthcare are already improving QoC. This article has presented a discussion on the suitability of SNA to model Careflow Networks and demonstrated this through the case study. It also provided both a technique and a vocabulary to inform healthcare managers and entrepreneurs how the delivery of healthcare could be potentially improved. SNA allowed us to establish insights through our hypothetical scenario and examine led us to new research ideas which we describe in section ‘Future research’.
Study limitations
This section offers a discussion on the limitations of this overall study. For example, considering the novelty of this work and the research gap identified by the authors, the literature review was a challenge to identify suitable sources to support our work. However, separating the literature into CH/E-health, healthcare systems and SNA, to identify the gap allowed the authors to argue the need to explore the benefit of this work using a hypothetical scenario. While another limitation of this research is that the case study employs a hypothetical Careflow Network scenario, we also explain that this can be carried out in a real-world context by adopting the same technique using SNA. This will also form part of our future research. In fact, the hypothetical scenario became a key asset to demonstrate the promise of applying SNA to map the Careflow Network and connectedness of CH. To successfully conduct a real-world case study, ethical considerations may present some additional limitations particularly regarding the need to track actors’ interactions within a healthcare system. However, if one can incentivise research participants while upholding ethical, privacy and data protection policies, such a study could be presented as a means to improve a healthcare system and alleviate the burden on healthcare professionals’ day-to-day interactions. While the behaviour of any unit of analysis of a person, group or organisation such as a Careflow Network, it can influence the outcome of interactions of the entity. However, while we accept this as a limitation of a case study, we are focused on the technique used to model the interactions and not the behaviour that influences such interactions. Thus, we use the hypothetical scenario to demonstrate how SNA can be employed to map such interactions with a view to identify bottlenecks and uncover how or where CH innovation may be best placed within a Careflow Network.
Future research
As part of our future research, we will model healthcare environments to include the connectedness of various Careflow Networks in various settings including hospitals and homecare. In addition, we will also continue to explore how SNA can be combined with other modelling techniques such as resource flow and value stream mapping, thereby offering a multi-layered view of Careflow Networks. Identifying a suitable tool such as a staff identification key-fob which captures human interactions may prove to be a very useful way to gather a large dataset within a Careflow Network. Ethical approval will be a critical element to employ such research methodologies. We recognise that SNA does have some limitations. For example, additional information is required to capture the weight or importance of a node in a complex health setting rather than merely focusing on the number of connections. We also need to understand how weights may be assigned to the importance of healthcare actors and the influence they have in the provision of safe and quality care services, for example, from a patient experience perspective. We can expand on the Careflow Network categories (transactional, nature of links and structural characteristics) to elaborate on the SNA. These will allow us to establish service metrics (Carroll et al. 2012) that inform us on how various factors are influenced by social behaviour, service structures and decision-making. Table 5 offers an insight on what may be achieved by employing SNA concepts and properties as Careflow Network metrics. Further research must be carried out to expand on establishing metrics that can stem from Table 3 (listing key concepts and network properties). Ultimately, this will allow us to recognise where CH innovation may optimise the impact of healthcare delivery.21,49 Combined with other modelling techniques, we consider that SNA is a suitable modelling technique for the assessment of the impact of healthcare innovations on Careflow Networks.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported, in part, by ARCH - Applied Research for Connected Health Technology Centre (![]() ), an initiative jointly funded by Enterprise Ireland and the IDA, by Science Foundation Ireland (SFI) grant 13/RC/2094, and SFI Industry Fellowship Grant Number 14/IF/2530.
), an initiative jointly funded by Enterprise Ireland and the IDA, by Science Foundation Ireland (SFI) grant 13/RC/2094, and SFI Industry Fellowship Grant Number 14/IF/2530.