
Abstract
Development and implementation of eHealth is challenging due to the complexity of clinical work practices and organizations. Standardizing work processes and documentation procedures is one way of coping with these challenges, and acceptance of these initiatives and acceptance of the clinical information system are vital for success. Clinical simulation may be used as “boundary objects” and help transferring of knowledge between groups of stakeholders and help to better understand needs and requirements in other parts of the organization. This article presents a case study about design of electronic documentation templates for nurses’ initial patient assessment, where clinical simulation was used as a boundary object and thereby achieved mutual clinical agreement on the content. Results showed that meetings prior to and in between workshops allowed all communities of practice an opportunity to voice their point of view and affect the final result. Implications of considering clinical simulations as boundary objects are discussed.
Keywords
Introduction
Clinical simulation refers to simulation performed by real users enacting realistic clinical work scenarios in close to real-life environments. Clinical simulation can be a valuable method for the evaluation of clinical information systems as the testing can take place in a controlled environment where there is no risk of injuring real patients.1,2 Simulation-based evaluation may take place in all stages of the life cycle of an information technology (IT) system3,4 and may be used for a number of different purposes. Clinical simulation methods have been used in health informatics to study various aspects of human–computer interaction in a number of research domains including human factors, usability evaluation, doctor–patient interactions involving technology, health professional information needs, health professional decision-making, new device testing and studies of medical errors.5–8 In contrast to field studies, clinical simulation studies allow for the possibility of examining different, complex and extreme usage scenarios during a short but highly intense testing phase. 8
As seen in Figure 1, clinical simulation may be used for various purposes in the different phases in the life cycle of a clinical information system. In the early phases, clinical simulation may be used to analyze user requirements, 7 assess how the system supports existing or future work processes, 6 and obtain the knowledge of user work practice. 6 In the design phase, clinical simulation may be used for encouraging user involvement and providing iterative feedback to the design of prototypes or real systems, 7 and it may combine elements of laboratory testing and field study. 9 In the implementation phase, particular aspects of the implementation can be visualized using clinical simulation, for example, user interaction in work practice, the need for training and the impact of decision support. 10 Unintended consequences of new systems such as changes in work processes and patient outcomes can be detected and provide organizational decision-makers with the option of early correcting actions if required. 6 By providing a sufficient degree of realism, various elements affecting work practice and the use of new technology may be evaluated 11 and can help support healthcare organizations to identify potential issues arising from the introduction of new technology before it is implemented in real-world settings.
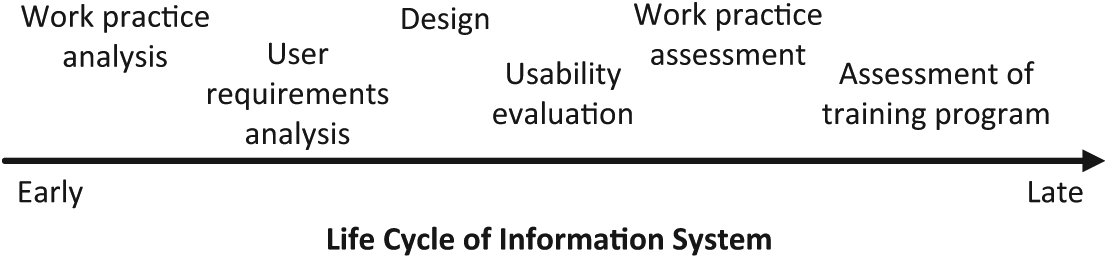
Activities using clinical simulation in life cycle of information system.
Applying simulation in information system evaluation allows for a high degree of experimental control while concurrently maintaining a high degree of realism, particularly in high fidelity testing.3,9,12 In such testing, clinicians are invited to use the information system in a realistic but controlled environment, resembling the clinical setting with respect to surroundings, patient cases, interaction with other staff members, information systems and so on. Hence, the context feels real, but shields consequences of system use and testing from patients. The simulation thereby provides a psychological safe space for the participant in which to try out new systems. By providing a sufficient degree of realism, evaluators can address how various elements may affect the simulated work practice and the use of the clinical information system.11,13 During the clinical simulation, it is possible to observe the clinicians’ interaction with the information system and to assess to what extent the information system influences work practices and the organization. Work practices that cannot be verbalized are not uncommon, 14 and clinical simulation increases the visibility of such “invisible” work. Use of clinical simulation as a common ground for discussion of design and organizational issues does, however, not come by itself. A certain focus needs to be placed on using clinical simulation as a medium for dialog and communication across different organizational groups and healthcare professions, with specific attention on the design of the simulation and evaluation set-up. Furthermore, the mandate of each of the participants needs to be clear.
The aim of this article is to describe how clinical simulation may be used as a boundary object to transfer and translate knowledge between different communities of practice. In the presentation, we will draw on related theoretical perspectives.
Boundary objects
Symbolic Interactionism considers meanings to be “social products,” creations that are formed and transformed in and through the defining activities of actors, as they interact. 15 When actors deal with the world of their objects and act in relation to it, this might result in creation and refinement of meanings. To understand the actions of people, it may be best to understand the worlds of their objects. Meaning thus created may be provisionally externalized through symbolic representations and concrete artifacts. Sometimes the same objects may appear in different worlds, which leads to a flexible interpretation and thereby a possible coordination between the actors of the different worlds. These objects are called Boundary objects. The next section expands on this topic.
Star and Griesemer 16 define boundary objects as “flexible epistemic artefacts that inhabit several intersecting social worlds and satisfy the information requirements of them.” “They have different meanings in different social worlds but their structure is common enough to more than one world to make them recognizable, a means of translation” (p. 393). Boundary objects may be repositories (e.g. a library or a database), ideal types (e.g. a diagram or a roadmap), coincident boundaries (e.g. the boundaries of a state) and standardized forms (e.g. classifications). Objects become boundary objects when they are used at the interface of different communities of practice. A community of practice has a shared understanding of what the community does, of how it does it and of how it relates to other communities and their practices. A community of practice will develop the same world view or mental model. 17 Boundary objects may be physical objects as well as symbolic objects. They are a kind of socio-technical hybrid spanning across boundaries of different worlds enabling and constraining knowledge sharing across boundaries 18 carrying information and context that may be used in translating, transferring and transforming knowledge between communities of practice. 19 Boundary objects may be a sort of arrangement that allows different groups to work together without consensus, something people act against, toward and with. 20 Technology may be considered a boundary object that can induce transformational learning in practices related to integrated design. 21
Carlile19,22 describes the following three approaches to knowledge boundaries in product development: syntactic, semantic and pragmatic. The syntactic approach to boundaries is based on the existence of a shared and sufficient syntax at a given border and ensures accurate communication between sender and receiver across a boundary to solve challenging communication or information processing problems.23,24 The semantic approach recognizes that even though a common syntax or language is present, interpretations are often different, which makes communication and collaboration difficult. In product development, differences in meaning or language across functions are challenging 25 and make communication difficult because individuals use different meanings in their functional setting. Integrating devices should be seen as processes or methods for translating and learning about the differences and dependencies at a boundary. The pragmatic approach highlights the importance of understanding the consequences that exist among things that are different and depend on each other. Here transforming knowledge refers to a process of altering current knowledge creating new knowledge and validating it. This may be done by letting users interact with prototypes. 26 Integrating devices, in this case, suggests that knowledge has to be transformed and in order to create new knowledge old knowledge has to be changed.
Boundary objects may be used to evaluate structures within an organization 27 and can include computer-assisted design, sketches and drawings in design engineering 28 and as a strategic tool. 29 Boundary objects are used for gaining a shared understanding of collaboration processes in the development of future collaborative processes, products, services and business models 30 and as a framework for modeling and categorizing organizational interfaces. 31 Boundary objects can be seen as appearing in many places in eHealth, for example, in clinical documentation and classification.23,32 To the extent that boundary objects provide stability, they do so through the consent of actors on all sides of the boundary. 33 They involve the participation of actors from both sides of the boundary and professionals, who serve as mediators, and they exist at the border of the two somewhat different social worlds, but they have distinct lines of accountability to each of them.
Clinical simulation contains many objects and representations which themselves may be considered as boundary objects, and at a high conceptual level, an entire clinical simulation can be considered to be a boundary object itself. Apart from describing related theoretical perspectives to boundary objects, this article presents a case study where we describe how clinical simulations can be viewed as boundary objects to improve communication and shared mental models (i.e. “common ground” 34 ), and what this approach can gain from the development of eHealth applications will be outlined and discussed.
Related theoretical perspectives
Shared mental models
Theoretical perspectives on shared mental models may elucidate how boundary objects support the process of achieving mutual agreement. The concept of mental models varies from field to field. A mental model of an IT system may consist of knowledge of the system or knowledge about the different tasks that may be performed in relation to the system 35 and may allow people to explain and predict the behavior of an IT system. Mental models help people to understand the world because they provide them with the possibility of constructing a working model in their minds and enable them to understand phenomena, to decide what actions to take and to control system mechanism. 36 Scientists in cognitive science and cognitive psychology suggest that mental models are important to the more general understanding of how humans interact and cope with the world. 37 Shared mental models for teams can be defined as “knowledge structures held by members of a team that enables them to perform accurate explanations for the task, and, in turn, to coordinate their actions and adapt their behavior to demands of the task and other team members” (p. 228). 31 In this article, we define mental models as described by Rouse and Morris 37 as a “mechanism whereby humans generate descriptions of system purposes and form, explanations of system functioning and observed system states, and predictions of future system states” (p. 360).
Mental models support interaction with the environment 35 and enable people to structure information in meaningful patterns36,37 containing several classes of information: concepts, features and their relationships. 38 Mental models allow knowledge about situations, objects and environments to be classified and afterward reorganized based on their features. 39 The purpose of mental models is that they support people in the description, explanation and the prediction of system behavior 37 and allow skilled decision-makers to forecast the outcome of a decision before it is taken. 40 Mental models can also be used as means to evaluate a user’s knowledge of the performance of a complex system supporting the analysis of effective and ineffective performance.41,42 Shared mental models are valuable for improving system design and may be used to explain human cognitive functioning and human–computer interaction. They may also be used as common models of a problem or a situation, 43 providing a context where communication can be interpreted and thereby giving a basis for predicting behavior and needs of other members. 44 Shared mental models support decision-making 40 and hence lead to an improvement in communication and coordination. 45 Shared mental models do not imply identical mental models. 31 Instead shared mental models are compatible mental models that lead to common expectations.
The degree of efficiency of collaborative teamwork depends on how well the team exchanges knowledge for continual learning and how well the team members develop shared mental models. Their individual mental models are bounded within their specialized practices and their work. Visualization enhances development of shared mental models 46 and is effective for improving shared mental models between negotiators and supports a pro-social climate. Visualization also supports communication and offers participants the ability to develop a sense of “what is seen” 47 which may be transformed into evidence. Thereby visual evidence may be perceived as being powerful. Communication in connection with visual evidence supports socialization. Problem solving in groups requires communication and collaboration, and communication breakdowns are often experienced due to differences in cultures, norms, symbols or representations. Supporting communication and the process of reflection within a shared context enhances the creation of shared understanding and may lead to new insight and new ideas. 48 Technology may be used as a medium for creating such environments providing opportunities and resources for design activities embedded in social debates and discussions actively involving all stakeholders.
Common ground
A similar idea to the shared mental model that has been applied into healthcare is common ground. Common ground refers to the knowledge shared between two persons or agents communicating with each other 49 and thereby relates to the process of transferring and translating knowledge. The agents or persons involved in the conversation have to share knowledge about language and about the subject under discussion. In healthcare, discussions about a medical problem with a clinical colleague lead to very different conversations than discussions with patients. Messages may be concise and mutual knowledge may be assumed between colleagues. On the other hand, explaining an issue to a non-expert requires that the main message is sent along with background knowledge, which is needed to make the message understandable. 34 Sharing of common ground may be seen as a key reason for similar agents to find it easy to communicate with each other.
Case study of clinical simulation as a boundary object
The case study described in this article concerns the design of electronic documentation templates and overview reports for nurses’ initial patient assessment 50 using clinical simulation. The case study took place in the Capital region of Denmark where a set of electronic documentation templates had previously been rejected by end-users and hospital management due to disagreement about the documentation procedure among the various stakeholders across the organization. Problems regarding acceptable time consumption due to technical difficulties as well as the need for rigorous design of the templates (i.e. clinical content, amount of structured fields and overview of patient data and differences in work practices) were key issues in the rejection of the templates. It was decided to address the organizational disagreements by redesigning the templates using a participatory design (PD) approach and clinical simulation through which the various stakeholders in the design process were to be thoroughly involved. PD focuses on involvement of stakeholders, overcoming organizational barriers and establishing ownership of the design solution within an organization. 51 Three issues dominate the discourse about PD: (1) the philosophy and politics behind the design concept, (2) the tools and techniques supplied by the approach and (3) the ability of the approach to provide a realm for understanding the socio-technical context and business strategic aims where the design solution are to be applied. 52 A core principle of PD is that stakeholders actively participate in design activities, where they have the power to influence the design solutions, and that they participate on equal terms.52,53
PD is not a predefined method, but an approach that includes a conglomerate of tools and techniques to be applied. These tools and techniques serve as ways to establish a shared realm of understanding based on the knowledge of how work is carried out, and how it can be carried out in the future, and may be used as boundary objects. Among these tools are observational studies, questionnaires, diagrams, pictures, photos, interviews, workshops, role-playing and simulated environments, mockups and prototyping 51 as well as clinical simulation. 50
Methodological approach
The overriding aim of the re-design process was to create a new set of structured templates that concurrently supported the daily clinical work practices of the nurses and that adjusted the documentation in accordance with the regional guidelines and accreditation requirements. In order to achieve this, it was necessary to gain consensus about the template design among the clinical nurses, quality units and nursing managers across the 12 hospitals in the region. Furthermore, the templates should be applicable for use by nurses in all types of bed wards. In essence, “one size had to fit all.” Specifically, the re-design had to respond to all the major critiques that were disclosed from the first pilot implementation. As a result, it was argued that the templates should
Handle highly structured data entry in an efficient manner. The previous highly structured data entry templates had led to increase in time to complete tasks (i.e. nurses had complained about the time taken to complete documentation using the templates).
Support daily nursing work practices. During the first pilot implementation, focus had been mainly on fulfilling documentation standards and accreditation requirements.
Besides these specific demands for change within the templates, a main lesson from the first pilot implementation was that there are many stakeholders involved in nursing documentation. Not only do registered nurses in the wards have an interest in the design of documentation templates so do quality coordinators, regional planners and hospital managers.
Stakeholders 54 may also be called communities of practice 55 or social worlds. 56 A community of practice is defined by Wenger et al. 55 as “groups of people who share a concern or a passion for something they do and who interact regularly to learn how to do it better.” It is the combination of three elements—domain, community and practice—that constitute a community of practice. The knowledge of its members is communicated by unique vocabulary, artifacts and patterns of practice. In healthcare, both “domains” and “practice” are significant in relation to different specialities and different parts of the organization. Different communities in different hospitals may also differ in their cultural behavior, and clinical simulation can be used to evaluate how new technology supports daily work practice in different healthcare contexts. In the following, we will use the expression “community of practice” when talking about the different parts of both healthcare and technology organizations. The terms “community” and “practice” aptly describe the essential elements which differentiate the different groups involved in the design of the templates. Patient care processes are supported by teams or communities of health professionals, for example, nurses and physicians. Each newcomer to a health profession learns the language of care as part of the process of membership. This varies from community to community. A community may be a department or a speciality. Furthermore, a community may be a quality unit or a patient safety unit. In the case study, the different communities included different departments and hospitals, the quality unit in the region, clinical documentation experts, clinical management and the IT department, which was responsible for the design and the development of templates as well as the pilot implementation.
By choosing a PD approach for the re-design process, all communities of practice were actively involved in the design activities and had the power to influence the design solutions. 52 Additionally, clinical simulation was used as a boundary object to translate and visualize the impact of the information system in work practice and thereby gain a shared mental model. By using clinical simulation, knowledge was transferred and transformed between the different communities of practice to support gaining a shared understanding. The aim was to overcome the organizational barriers that were experienced during the first pilot implementation of structured documentation templates. The first pilot implementation had led to considerable disagreement about the documentation procedures among the various communities of practice across the organization. The clinical simulation allowed the different groups to work together to arrive at consensus based on the simulation rather than preconceived notions.
The use of boundary objects is especially important when the communities are geographically separated, as in this case. The ability to work together is correlated to how well the geographically distributed communities share information and knowledge at the interfaces. 27 This was also the case here. The quality control department is located outside the hospitals and the hospitals themselves are also geographically separated. Clinical simulation as a boundary object was used to represent, learn about and transform the knowledge to determine the consequences that exists at a boundary. It may explain how knowledge is localized, embedded and invested in practice, as described by Carlile.19,22
A core principle in PD is that communities of practice are actively participating in design activities, where they have the power to influence the design solutions.53,57 The different communities of practice were invited to and took part in some of the central steps in the design process during the clinical simulation. In the end, the participants consisted of two regional quality experts, two hospital quality experts, one hospital director, four nursing managers from different hospital departments, six documentation nurses and two health informatics experts, who were experts in the design and configuration of documentation templates. All hospitals showed great interest in participating, and some of the hospitals actually asked to have more than one participant. It was, however, decided that each hospital would have just one participant.
The activities in the re-design process are illustrated in Figure 2. Before the first workshop, all relevant documents were analyzed and meetings were held with one regional quality expert, one nursing manager and one documentation nurse in order to develop a shared understanding of the internal disagreements and potential ways of addressing them, and site visits were conducted at various hospitals to gain knowledge about work practice. On the basis of document analysis and site visits, a prototype of the templates was developed. The templates were presented and used to initiate the development and discussions about user requirements and the need of clinical content at the first workshop. All communities of practice, that is, clinical nurses, quality managers and nursing managers from all the regional hospitals, attended the workshops as well as health informatics experts and technical experts. The nursing processes were compared to the features of the prototype. Modifications in content and user interface design were agreed on at the workshop, and after the workshop, the templates were modified according to the agreed changes. Issues, which the participants could not agree on, were noted and were to be dealt with at a later time, that is, at the next workshop, during the clinical simulation or after the pilot implementation. Follow-up meetings to the first workshop, where more detailed matters were settled, were held with a few representative nurses and quality experts before the second workshop. These details were discussed at the second workshop where a new version of the templates based on the comments was presented and discussed. Again not all issues were agreed on. Some issues were to be addressed in the clinical simulation, and some issues were to be addressed in the pilot implementation. Issues to be examined in the clinical simulation concerned the amount of structured data and the terms used to guide and label the structured spaces as well as support of work practice. Furthermore, the quality experts were asked to clarify some disagreements concerning how the regional standard was interpreted. Some of the clinical nurses wanted a space in the documentation to record how the patient felt, whereas other nurses wanted the patient’s opinion to be part of the rest of the documentation. These disagreements were not actually positioned to specific hospitals or specific specialities, but were merely rooted in different graduate educational backgrounds. After the second workshop, the templates were further adjusted based on the outcome of the workshop. As such the meetings made it possible to take the discussions at the workshops to a higher level supporting a fast PD process.

The re-design process including clinical simulation.
The next step was to let a group of end-users simulate the use of the templates in a clinical simulation. In the first attempt to create the documentation templates, clinical simulation had also been used, but at that time, the purpose of the simulation had been to let the end-users evaluate the templates, and the outcome had afterward been discussed at a workshop with the different communities of practice. The end-users in the first attempt came from eight pilot departments located at eight different hospitals. In the second attempt, the pilot site was an entire hospital in the region instead of having pilot departments scattered all over the various regional hospitals. The idea was to prove that the templates were usable in an entire hospital and thereby usable in the rest of the hospitals in the region. In the second attempt, the participating end-users involved in the clinical simulation came from all departments at the pilot hospital. The purpose of the clinical simulation was broadened to focus not only on end-users but also to use the clinical simulation actively as an observation site and boundary object for discussions among the different communities of practice.
The clinical simulations were performed in realistic environments and with realistic scenarios from actual patient cases. All scenarios were based on patients assessed at the hospital within the first 24 h. In some scenarios, one nurse made a full initial nursing assessment, whereas in other scenarios, half of the assessment was already documented and the nurse had to finish the documentation. Thereby, the scenarios covered hand-over situations. Eight nurses simulated the scenarios. An actor played the role of the patient, in order to make the simulation realistic. Delegates from other communities of practice observed the simulation from an adjoining control room. Debriefing interviews were held with the nurses after the simulations. The observers also participated in the interview and were able to ask questions during the interview. After each interview, the observers discussed their observations and the outcome from the interview. The observers had also attended the workshops, and each delegate contributed depending on their background and organizational relation and each had well-defined roles and responsibilities. 31 The purpose of the clinical simulation and the discussion that followed the simulation was not to gain unanimous consensus but, just as importantly, to provide input for others to make the final decision. The participants were in no way homogeneous either with respect to expertise, roles and responsibilities. Results from the observations, interviews and discussions were gathered and presented at a third workshop. At the workshop, the final modifications to content and user interface design were agreed on. Issues that were not solved at the third workshop were noted and were to be examined during the pilot implementation. The prototype was modified and accepted by the regional patient record committee. Following that the system was evaluated during a 3-month pilot implementation at an entire hospital in the region. The pilot implementation was evaluated through field observations, clinical simulation in situ, audit of 50 patient records, questionnaires and focus group interview and technical monitoring. The evaluation served as basis for decisions on further implementation of the templates in all hospitals in the region.
Results
Use of clinical simulation as a boundary object resulted in an increased focus on the practical challenges when working with the templates on a daily basis, such as how to have a genuine conversation with a patient and concurrently document the conversation using a computer. The key differences between the first version and the second version of the templates were the following:
Requirements for structured data were reduced to a minimum to ease the nurses’ documentation processes. Many structured fields were removed, and a few were added.
The overview of the patients’ record was improved. The original overview was optimized and an additional version of the overview was designed.
Requirements concerning the content of the templates were aligned for most parts, and it was decided that minor elements would be evaluated during the pilot implementation. The modified content focused on the most generic areas and elements of the initial nursing assessment, e.g., details concerning hearing aids were reduced.
The evaluation of the implementation of templates at the pilot hospitals resulted in the following:
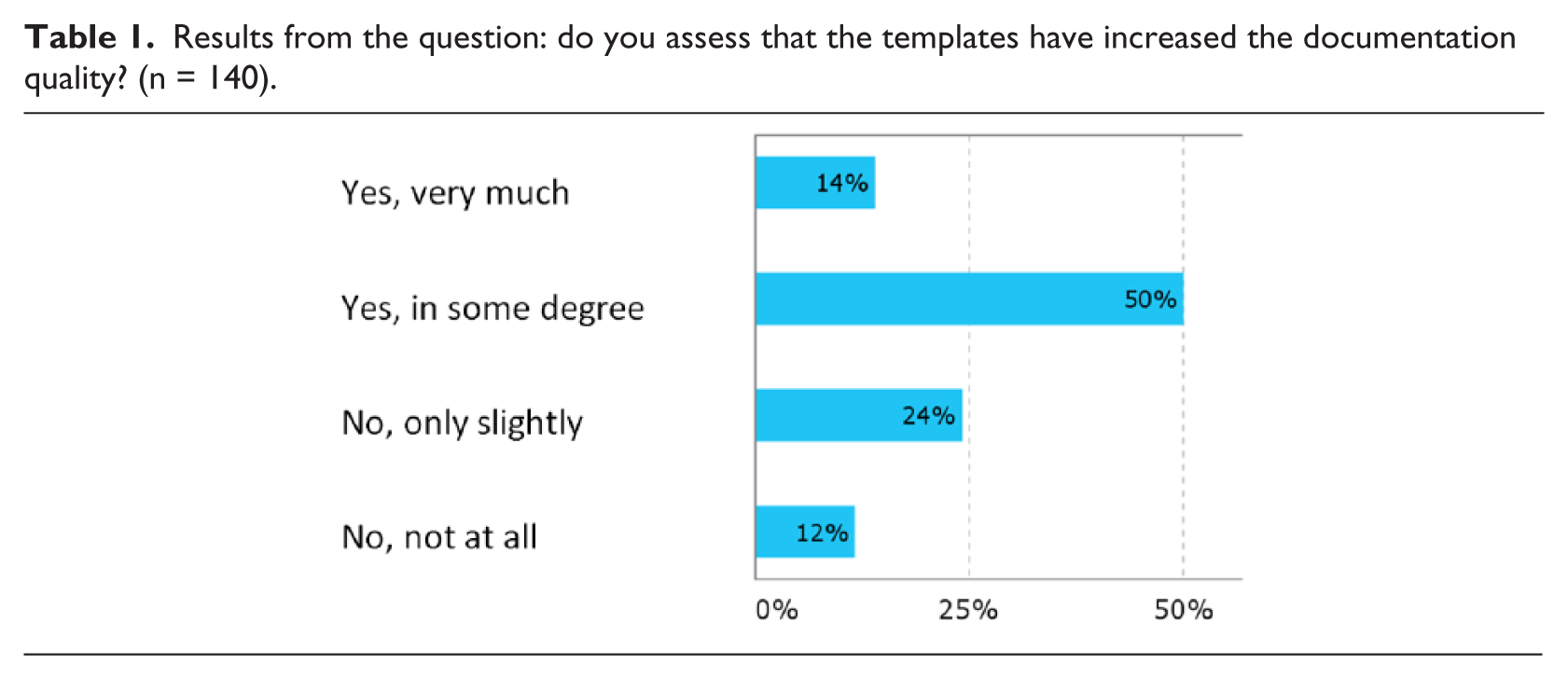
Higher quality of nursing documentation. As shown in Table 1, 14 percent of the nurses perceived that the quality had increased considerably, 50 percent felt the quality had increased in some degree, 24 percent did not perceive any difference and 12 percent felt that the quality had decreased. The audit of 50 patient records showed increased documentation of the patients’ habitual and actual condition in up to 25 percent of the electronic templates, as compared to paper-based nursing documentation. In the paper-based records, it was difficult to distinguish the patient’s own assessment from the assessment made by the nurses.
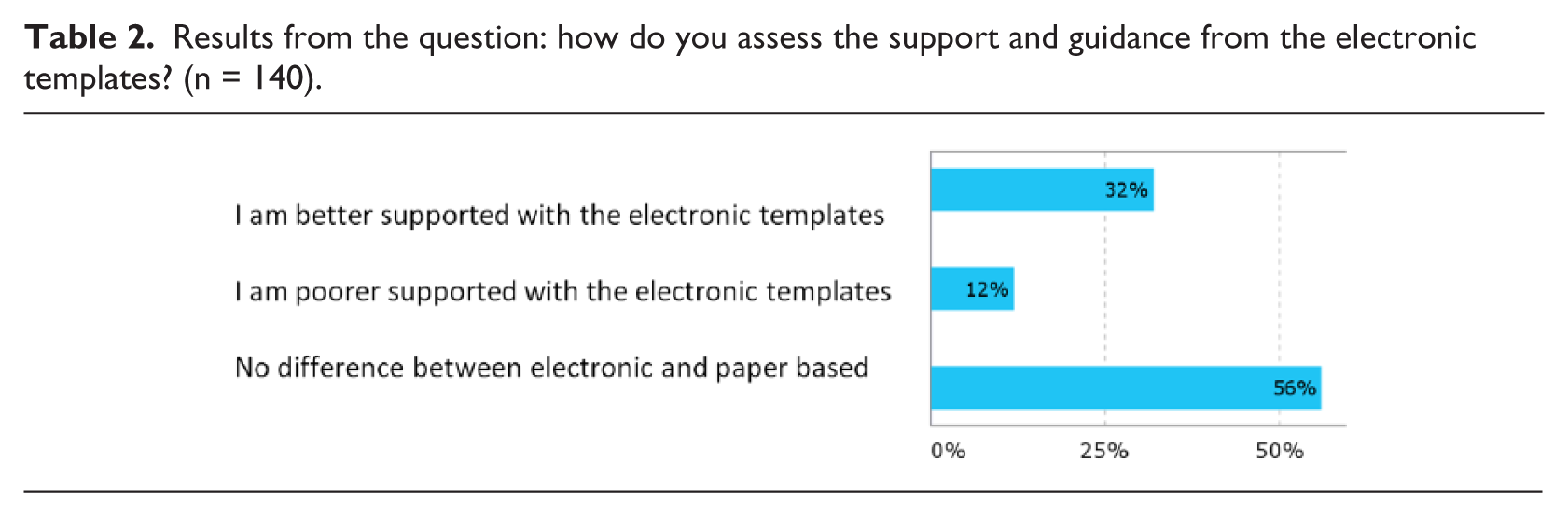
Higher support and guidance. As shown in Table 2, 31 percent of the nurses assessed that the templates supported their work very much, 12 percent assessed that the support had decreased and 56 percent did not experience any difference.
Measurements of time spent in doing initial assessments showed an almost equal amount of time was used for documentation using paper-based documentation and electronic documentation. An observational study found that 10.07 min (mean time for 30 initial assessments) was spent in doing initial nursing assessments using the paper-based documentation, while 11.45 min (mean time for 14 initial assessments) was spent when using electronic documentation. Furthermore, six laboratory tests were conducted where the time spent on documentation of an initial assessment test case was measured. These tests indicated that 8.29 min was the mean time spent on paper-based documentation, while 9.18 min was the mean time spent on electronic documentation.
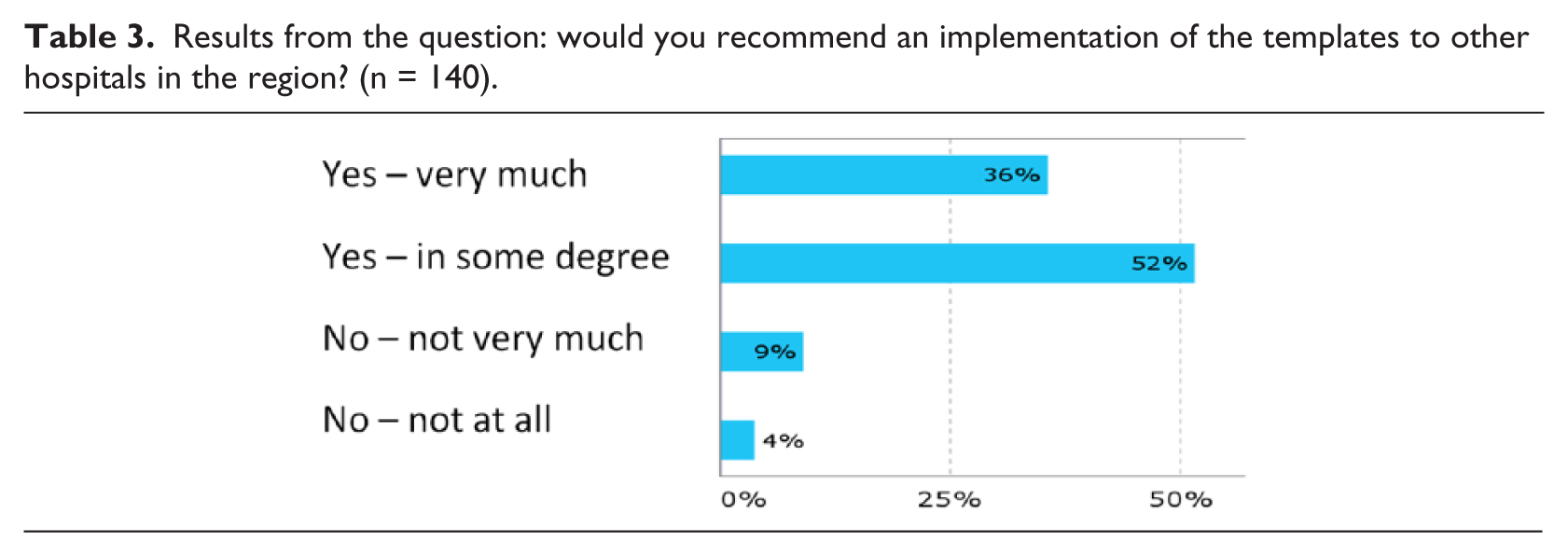
In total, 87 percent of nurses would to some degree recommend the use of the templates. As shown in Table 3, 88 percent of the nurses would in some degree or very strongly recommend the implementation of the templates in other hospitals in the region.
Results from the question: do you assess that the templates have increased the documentation quality? (n = 140).
Results from the question: how do you assess the support and guidance from the electronic templates? (n = 140).
Results from the question: would you recommend an implementation of the templates to other hospitals in the region? (n = 140).
The evaluation resulted in the recommendation to continue the implementation, and the templates have now been implemented at all hospitals in the region. The representatives from each separate hospital who participated in the design process of the templates were each responsible for the implementation in the departments at their own hospital. These users did not have any problems in not being able to participate in the clinical simulation and the pilot implementation as long as users (nurses) from another hospital had already evaluated the templates. The implementation has resulted in changes in the documentation process at some departments in ways that depended on their existing processes. At one hospital, the templates were implemented as paper templates before the implementation of the electronic templates, and therefore, the documentation process was changed before the implementation of the electronic templates. At another hospital, a disagreement emerged concerning whether the templates should contain a separate field for the documentation of the patient’s own view of their illness or whether this should be encompassed in the other fields. This disagreement has not been overcome yet; however, the templates are being used as planned. Overall, the implementation of the templates has been one of the most successful implementations in the region.
New documentation templates for psychiatric departments have also been developed, and the development of documentation templates for pediatric departments has also taken place.
The results of using boundary objects and the specific design method include the following:
All communities of practice were involved and showed great interest in participating.
Ownership was obtained by including all communities of practice in the process, leading to a wide adoption of the system in the organization.
The gap between quality nurses’ theoretical approach and the ward nurses’ practical approach was overcome.
Using clinical simulation as a boundary object helped to visualize the use of the templates and to obtain a shared mental model.
Debriefing interviews and discussions and workshops helped to align expectations about the templates and gave input to final decisions about design and content of the templates.
Clinical simulations may be used as boundary objects. Clinical simulation as boundary objects are constructed at the intersection of the communities of practice of design and the use of clinical information systems. They reveal the divergences between the different communities, and during the process, they reshape the relations and shift alliances and the overall balance of power. 59 Clinical simulation makes it possible to actively participate in design activities. Choosing a PD approach empowers the participants to influence the design solutions on equal terms, which ensures ownership in the subsequent implementation of the information system.
Clinical simulation also consists of many features and aspects which themselves may be been seen as boundary objects. We can also “open the box” and consider the objects (i.e. artifacts and activities) that make up clinical simulation that can be shared. As can be seen in Figure 3, these include simulation artifacts (i.e. scenarios and prototypes), activities (i.e. observation, interview and questionnaire) and evaluation artifacts (i.e. notes, screen recording, video recording and audio recording).
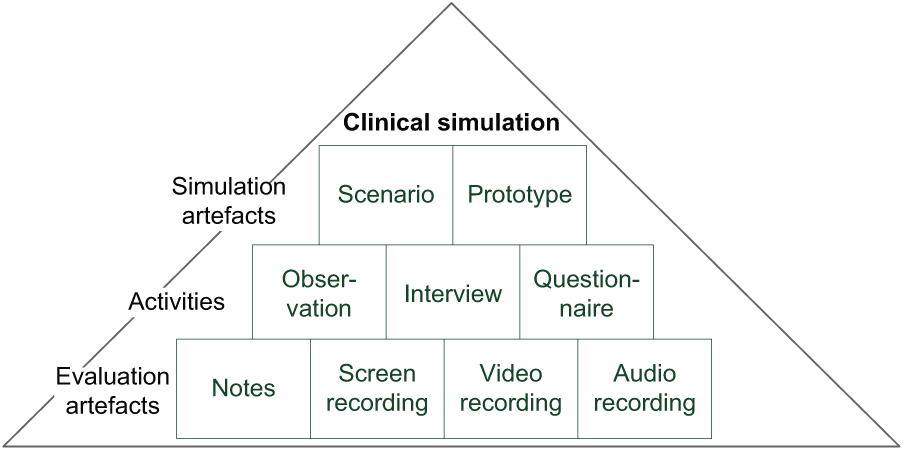
Artifacts and activities in clinical simulation.
Simulation artifacts
Simulation artifacts are used during clinical simulation in order to simulate the use of technology for clinical work practice in clinical contexts.
Scenarios are used as basis for simulations. Scenarios are narrative descriptions of work practices, a kind of story about people and their activities 63 reflecting typical tasks in a smaller or larger fraction of work practice. Scenarios may be described as “springboards,” artifacts serving as boundary objects, where scenarios represent the essential and typical aspects of a situation. 64 A scenario can be regarded as an ideal type of boundary object, 16 carrying information and context that can be used in translating, transferring and transforming knowledge between communities of practice. 22 In the case study, scenarios were used to outline the context of clinical work practices that are being looked into as well as the content of the work practice.
Prototypes and mockups allow for commentary early in the design phase and offer a way to involve and consult communities of practice. 60 In the case study, the prototype enhanced the communication between users and developers, 61 but they can also be used to describe the work done by technicians. 62 In relation to clinical simulation, prototypes are useful for participants and observers during the simulation and for the debriefing interview and discussion.
Activities
A range of activities are performed during the simulation and afterward as part of the evaluation. Evaluation activities involve both users and observers. The process of observation as a group became a group shared experience and a kind of boundary object. Questionnaires were not used in the case study, but they can be used as a supplement to interviews in evaluation studies. A questionnaire survey is a standardized method that may be used for common communication across dispersed work groups 16 and may hereby also be regarded as a boundary object. Interviews may in the same way be regarded as boundary objects. The results from the interviews were discussed in other situations and locations, and the different interviews took place in different places and time.
Evaluation artifacts
Evaluation artifacts are used for manual and electronic data collection during the simulation, during the evaluation and discussion with users and observers and afterward as part of the analysis and evaluation and at follow up workshops with different communities of practice. Notes and transcriptions from observation of users were shared and used for common discussion across the dispersed work groups in different situations and locations, and created shared mental models and shared understanding. Recordings from screens and videos as well as audio recordings may be used as tools for communication, discussion and transferal of knowledge across distance and time and offer the possibility of gaining shared understanding as the people watching and listening to these recordings may use this to gain a shared mental model. In the case study, recordings of the simulation were not used. Instead, the results from the simulation and debriefing discussions were presented at the third workshop.
Clinical simulation and the various objects and representations were used as boundary objects to improve communication and shared mental models (i.e. “common ground” 34 ). The participants subsequently reported that the clinical simulations had supported them in gaining a shared mental model, and the result was, as described by Rouse and Morris, 37 that shared mental models can help in delineating the requirements of a new system (e.g. eHealth system) as well as providing shared understanding of how the system operates and was used effectively during the design process. None of the participants had experienced any problems related to the use of resources as their participation was highly prioritized in all parts of the organization.
Discussion
The simulation provided an important input about how to solve some of the practical challenges facing the daily work with the documentation templates and itself became a boundary object as it was used at the interface of different communities of practice. By observing end-users using the templates, the discussion among the different communities of practice served as common ground, supported a shared understanding and changed the focus to the usage of the templates from a less informed approach according to the stakeholders’ own specific area and practice. Bowker and Star 23 argue that “the more at home you are in a community of practice, the more you forget the strange and contingent nature of its categories seen from outside” (p. 294). Clinical simulation is a pragmatic approach to considering boundary objects and visualizes the consequences and the impact of implementing an information system. Clinical simulation transforms the knowledge about a process and creates new knowledge. Things are depicted differently by different communities of practice and in different contexts; 23 however, as in the example provided by Iansiti’s 26 work on the role of prototypes, clinical simulation enhanced the process of transforming knowledge.
In the first design round, the debriefing interview was not used to the same degree as a medium for dialog and discussion. In the second round, clinical simulation as a boundary object provided the different communities of practice with the opportunity to observe and discuss the impact of the re-designed template and offered a way to manage the tension between divergent viewpoints, which was of great assistance in this case study, especially, concerning different views on content and structure of documentation. As some of the participants subsequently expressed, “We no longer discussed based on our own ideological attitude. Instead we gained a shared mental model to discuss from.” Some communities of practice found that the highly structured nature of the templates limited the flexibility of the conversation with the patient and made the documentation unnecessarily complicated. Thus, clinical simulation was used as a boundary object to facilitate meetings such as debriefing interviews and workshops and as part of the design process. 21
Prentice argues 64 that “surgical learning occurs at the interface of bodies and instruments, through simultaneous sculpting of the surgical site and training of the surgeons body,” a process she calls “mutual articulation.” 58 In the same way, clinical simulation provided the opportunity to investigate the impact of work practice before it affects the daily work in a hospital. Another way of expressing the use of boundary objects is stated by Bowker and Star: 23 “the medium of an information is not just wires and plugs, bits and bytes, but also conventions of representation, information both formal and empirical. A system becomes a system in design and use, not the one without the other.” Clinical simulation provides the opportunity to observe the system in both design and use.
Not all communities of practice were able to participate either by using the information system themselves or by observing the use of the system. Therefore, the results were presented and discussed at a third workshop. At the workshop, issues addressed for the clinical simulation and new issues that had been identified during the simulation and the debriefing interview with the end-users were discussed. Not all issues were agreed on but had to be addressed at the pilot implementation. As mentioned, the pilot implementation was conducted at an entire hospital, and as a consequence, the benefits of using electronic templates became more obvious. In the first attempt, the initial nursing assessment had to be printed when the patient was moved from a department using electronic templates to a department using paper-based templates. Initial assessment documentation that had started out digitally but not yet finished was documented using paper-based template at the next department.
The major difference between the initial design project and the re-designed project was that the re-designed project used clinical simulation and a PD approach, involving a number of communities of practice, not only proponents of the highly structured nursing documentation. The simulation, the debriefing interview and the subsequent workshop made it possible to achieve the mutual clinical agreement on the actual content of the templates and thereby design. Furthermore, the meetings prior to and in between the workshops allowed all the community of practice an opportunity to voice their point of view and to affect the final result. The templates were regarded as “one size fits all” templates for adults with somatic illnesses. Although the psychiatric departments and the pediatric departments were not able to use the templates, new documentation templates for these departments have now been developed using the same design process as in the case study with the original templates as a basis for the design.
Implications of clinical simulation as boundary object for eHealth
The complexity of both organizational and work practices in healthcare creates challenges regarding the choice and application of methods used for the development and implementation of clinical information systems. 65 As in the case study, the complexity of health organizations and the varied types of healthcare actors complicate the specification of user requirements and the design and implementation of clinical information systems. These issues in eHealth influence the cost and resources needed in acquiring and implementing new technology at hospitals as well as adoption afterward and may be due to lack of acceptance and lack of understanding among end-users. As described in the case study, clinical simulation may be useful in gaining shared mental models and shared understanding of user requirements, work practice and organizational requirements. The study of boundary objects provides a significant way to analyze these issues and can serve as a reflective approach to improve solutions to the problem. This case study shows that the adoption and acceptance of new technology may be greatly improved by involving end-users as well as other parts of the organization in both the design of new technology and the design of future work processes. If users are not adequately involved in these processes, the new technology developed may end up endangering patient safety and result in unintended events and increased mortality.
Considering clinical simulations as boundary objects in the design phase of the development of clinical information systems offers a means to transfer knowledge from one part of the organization to another and thereby creates shared understanding of complex work practices and requirements. In the case study, organizational differences were overcome, and shared understanding was made possible in achieving a mutual clinical agreement on the basis of shared mental models and joint discussions. Acceptance of new technology may be gained by giving voice to the different communities of practice and thereby supporting the acceptance and use of new technology.
Other case studies13,66 show the possibilities in having different healthcare actors participate in clinical simulation and subsequent debriefing discussion. Clinical simulation as a boundary object offers an opportunity to create a space where healthcare professional working in different locations or healthcare sectors can meet and exchange knowledge about work practices and requirement needs. This approach proved effective in identifying important unintended benefits or challenges, 13 gaining knowledge about the effect that new technology may have on work practices, 66 or patient safety issues. 67
Conclusion
We conclude that clinical simulations (and their components) can be considered and used as boundary objects for transferring and translating knowledge among different communities of practice. In the case study described in this article, clinical simulation helped in transferring knowledge from one community of practice to another and helped different parts of an organization in gaining shared understanding about needs and requirements. Clinical simulation offered a means to achieve a mutual clinical agreement on the design of a new information system. Furthermore, subsequent discussion allowed all the communities of practice an opportunity to voice their point of view and to affect the final result. We recommend that the use of clinical simulation as a boundary object should be expanded and propose further research in this area. This might involve further identifying, characterizing and optimizing components of clinical simulation that serve to promote shared understanding. Comparisons among different types of boundary objects, including their forms and formats, could be conducted in order to identify optimal ways of providing shared understandings among different stakeholders in the design, deployment and testing of health information systems. We are currently undertaking such work and find the approach to considering clinical simulations in the context of boundary objects as promising.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.