
Abstract
Past research has found that older US adults (aged 50–75 years) exhibit high levels of cancer information overload and cancer worry; however, no study to date has examined whether these perceptions are related to information seeking/scanning. To explore this relationship, older adults (N = 209, Mage = 55.56, SD = 4.24) were recruited to complete a survey measuring seeking, scanning, cancer information overload, and cancer worry. Most participants were high-scan/seekers (40.2%) followed by low-scan/seekers (21.1%), high-scan/no seekers (19.6%), and low-scan/no seekers (19.1%). Low-scan/no seekers had significantly higher cancer information overload compared to all other groups, consistent with the postulate that overload and seeking/scanning are negatively related. Low-scan/no seekers and high-scan/seekers both exhibited higher cancer worry severity, consistent with past research suggesting that cancer worry explains high levels of activity/inactivity.
Health information seeking and scanning has become increasingly important over the last several decades.1–6 Individuals can access an abundance of health information by actively using various search tools (information seeking) or by passively taking in desired information as they encounter it (information scanning). 7 Health information seeking and scanning are directly and indirectly related to individuals’ performance of health behaviors. 7
Modern communication technologies rapidly create, duplicate, and disseminate health information. However, the quality and quantity of health information could prove problematic,8,9 especially for traditionally underserved groups.10–12 For instance, the ever-increasing volume of accessible health information and proliferation of information channels—accompanied by a lack of cancer-relevant knowledge and cognitive ability to comprehend cancer information—could cultivate cancer information overload (CIO). Information overload is not a new concept in information science generally;13,14 yet CIO specifically has recently drawn the attention of health communication scholars.15,16 CIO is of interest to health communication researchers because surveys of the US public have suggested that approximately three-fourths of adults show signs of overload. 8 Secondary data analysis has suggested that CIO is related to lower socioeconomic status, poor health, low media attentiveness, and high affective components of information seeking. 17
CIO is a perception of the information environment that is likely shaped by past information seeking/scanning experiences. 15 The information overload model (IOM) postulates that individuals with dispositional overload for a particular type of content will attack, disregard, and/or avoid that content over time; 18 yet no study to date has tested this postulate with a validated measure of information overload. The recent validation of a multi-item measure of CIO 15 allows researchers to test postulates of the IOM, including whether individuals with higher overload avoid particular content.
Past research has mostly focused on the antecedents and consequences of health information seeking, such as how it influences subsequent decision-making 19 rather than factors that trigger or motivate seeking/scanning behavior. 20 The purpose of the current study is to investigate how cancer information seeking and scanning behaviors (SSBs) are influenced by CIO and cancer worry. The latter advances our understanding of dispositional cancer worry 21 and provides an alternative cancer-specific affective disposition to compare/contrast with CIO. Although researchers have found that CIO is distinct from other similar constructs—such as cancer fatalism 15 —the utility of measuring different cancer-specific dispositions is still an unresolved question. Thus, investigating whether CIO and cancer worry relate to health seeking/scanning will help researchers to decide whether one or more of these constructs is essential to future information acquisition models. It is especially important to address these questions with older populations, as the United States has an unusually large older demographic at the moment (i.e. the Baby Boomers) who are increasingly utilizing modern communication technology to seek/scan for health information.22–25
Cancer information seeking and scanning
In 2008, 45 percent of individuals in the United States had searched for cancer-related information at least once in their lives; among them, three of four had searched in the past 12 months. 8 As individuals typically engage in different levels of information seeking and scanning activities based on their individual interests and characteristics, Shim et al. 7 developed an instrument to measure health information SSB. SSB is important to measure because it has the potential to influence an individual’s decision-making, and consequently, it can impact health outcomes. For instance, Shim et al. 7 found that health information seeking and scanning were both associated with healthy food consumption and cancer knowledge.
Previous research has primarily studied health information seeking by focusing on two main aspects: antecedents and outcomes. Lambert and Loiselle 26 suggested that personal and situational factors can influence the type of information an individual seeks, how much information he or she seeks, what sources he or she uses, and how he or she ultimately obtains this information. The literature notes that information seeking behavior could be influenced by a number of personal factors, including self-efficacy, health status, affect, the type of communication(e.g. face-to-face communication, mediated communication), preexisting anxiety about a particular communication channel, and demographic variables such as age, gender, and income.31–33 With regard to situational factors that can influence information seeking, the literature identifies news coverage 34 and the accessibility and quality of online health information 35 as the main factors to consider. Health information seeking is a behavior that can lead to specific positive health outcomes, including facilitating individual involvement in personal health care, 8 increased quality of life, 36 and decreased negative emotions. 37
Individuals are not always active health information seekers, and there is growing recognition that less effortful information exposure also has the potential to influence an individual’s health behavior. Previous research has focused primarily on active health information seeking, while less attention has been devoted to studying passive health information exposure. In this study, we follow the definition of information scanning provided by Niederdeppe et al. 34 as “… information acquisition that occurs within routine patterns of exposure to mediated and interpersonal sources” (p. 154). Although information seeking and scanning share some common aspects, we suggest health information scanning is distinct from health information seeking behaviors based on previous research.
Most research on cancer information seeking has focused on cancer patients;38,39 consequently, the frequency of cancer information seeking and scanning within the general population is currently unclear. 40 Therefore, to fill this gape in the knowledge, the current study focuses on cancer information seeking and scanning patterns present among the general population, as opposed to cancer patients.
Wilson41,42 indicated that information behavior is a broad term that encompasses both active information seeking and passive information reception. Even though the importance of passive information gathering has been recognized by researchers,7,43 Longo et al. 44 suggested that there is insufficient research that explicitly examines “passive receipt” of information, which also refers to scanning, incidental, or mere exposure to information. While many passive information gathering terms are used exchangeably, there are still some differences between these terms. For example, information scanning and passive information seeking differ from incidental or mere exposure to information as individuals pay more attention or are motivated to process the information when they scan or seek information passively. While acknowledging some conceptual overlap with other terms, cancer information scanning is the focus of this research as the goal is to study individuals attending to a particular piece of idea or fact in the normal flow of information that goes beyond incidental exposure. 7 Kelly et al. 40 also argued that the term “information scanning” does “a careful balancing act between seeking and completely passive exposure” (p. 737).
CIO and the IOM
Although “the potential for overload has existed since information became an important input to any human activity” (p. 33), 45 information overload is an increasingly concerning byproduct of the overwhelming amount of information produced today. Bawden and Robinson 46 indicated that information overload is caused by too much information at hand and worsened by multiple competing formats and channels.
The IOM was developed to theorize causes and effects of overload. 18 The IOM is based on decades of research devoted to social cognition and information processing. Research in those areas has consistently demonstrated that human beings have deep information storage capacity tempered by limited immediate processing ability.47–49 To survive, humans only devote time and energy to select information. 47 For example, Lang 48 argued that receivers are cognitive misers who selectively focus on information that is consistent with their goals and/or indicative of change.
In a larger sense, the IOM is consistent with fear control as articulated by the extended parallel processing model (EPPM; for a review, see Witte and Allen 50 ). Fear control occurs when people perceive limited efficacy—but significant threat—and thus engage in an emotion controlling behavior (e.g. avoiding information so it does not trigger fear). Moreover, the IOM is also akin to research that suggests messages can produce unintended effects (such as obfuscation, see Cho and Salmon 51 ), unintended construct activation, 52 or avoidance, blunting, and coping. 53 That is, information overload is an unintended byproduct of the saturated information environments.
Information overload also occurs in health settings. CIO is a concept that addresses cancer specifically. CIO is defined as “… feeling overwhelmed by the amount of cancer-related material in the information environment.” 15 According to data from 2013 Health Information National Trend Survey, 69.94 percent of respondents (N = 3630) agreed with the statement, “There are so many different recommendations about preventing cancer, it’s hard to know which ones to follow.” Even though a large portion of participants reported high levels of CIO, few studies have investigated how health information seekers actually cope with this overload. 17
Previous research has suggested that online health information seeking/scanning is not significantly associated with information overload. 17 However, this particular study may not be generalizable, as it used an unvalidated measure of CIO and focused on online information seeking specifically, rather than general health information SSBs. Moreover, the IOM postulates that overload is context specific. 18 For example, highly arousing content, like cancer information, may require additional resources to process, a situation that facilitates cognitive or information overload.18,54 Thus, we hypothesize that individuals who perceive higher levels of CIO are less likely to engage in cancer information seeking activities.
H1: CIO is negatively related to health information seeking.
H2: CIO is negatively related to health information scanning.
Cancer worry
Previous research has shown that emotional status is a good predictor of one’s health and health behavior.55,56 Different types of negative emotions, such as anxiety, fear, and worry, are closely related but distinct constructs that can have very different impacts on an individual’s health behaviors. 29 For example, research suggests that health anxiety may moderate the relationship between online health information seeking and health care utilization decisions. 57 A number of previous studies focused on the negative health outcomes caused by negative emotions.58,59 For instance, Sirois and Burg 60 indicated that negative emotions could cause cardiac risk factors. A separate line of research from Davey 61 has demonstrated that negative emotions such as worry could also lead to positive health behaviors, in cases where day-to-day worry motivates individuals to cope with the threats that are causing them to worry.
Cancer worry is a concept that is empirically distinct from worry in general. 21 Cancer worry is defined as “an emotional reaction to the threat of cancer” (p. 571). 62 Jensen et al. 21 suggested that dispositional cancer worry has two underlying factors: severity and frequency. Previous research has examined the effects of dispositional worry on various health preventive behaviors, including screening behavior,63,64 breast self-examination, 65 and skin cancer preventive behaviors. 66 Cameron and Diefenback 67 demonstrated that cancer worry can lead to greater interest in, and more favorable beliefs toward, genetic testing for breast cancer. Additionally, Renahy et al. 68 found that worry about one’s health is positively associated with online health information seeking.
Most cancer worry research to date has focused on how cancer worry relates to risk perceptions and cancer-screening behavior, while little research has been conducted to examine the relationship between cancer worry and cancer information seeking specifically. Beckjord et al. 29 indicated that high levels of cancer worry are associated with more attention to health information and worse information-seeking experiences. However, their findings are limited by their use of a one-item scale to measure cancer worry.
The current study adheres to the conceptual framework of dispositional cancer worry established by Jensen et al. 21 and utilizes a newly validated multi-item scale as a more comprehensive measure of this construct. We intend to examine the relationship between dispositional cancer worry and cancer information SSBs. Based on past research, we propose the following research questions:
RQ1: What is the relationship between health information seeking and dispositional cancer worry?
RQ2: What is the relationship between health information scanning and dispositional cancer worry?
Method
Study design
Adults aged 50–75 years completed a survey assessing their information SSBs. Participants received US$25 for completing the study. The study protocol was approved and monitored by a university institutional research board.
Participants
Adults (N = 209) were recruited from one of eight worksites (six hospitals and two manufacturing plants) via their human resource (HR) representatives. HR representatives at each respective site sent out recruitment e-mails to employees who were 50–75 years of age. The mean age of participants in the current sample was 55.56 (SD = 4.24) with a range of 50–71. Most participants were female (71.8%) and Caucasian (97.1%). Education was distributed as follows: high school degree (27.3%), some college (8.6%), associate degree (19.1%), and bachelor degree or higher (45.0%). In terms of household income, approximately 18.7 percent of the sample earned below the US average ($51,000 per year).
Measures
CIO
Overload was measured using the 8-item CIO scale. 15 The CIO scale measures feelings about the overwhelming quantity of cancer information. Sample items include, “there are so many different recommendations about preventing cancer, it’s hard to know which ones follow,” “Information about cancer all starts to sound the same after a while,” and “It has gotten to the point where I don’t even care to hear new information about cancer.” Participants indicated their feelings using four response options (strongly disagree to strongly agree) where higher scores indicate greater overload (M = 2.37, SD = .77, α = .87).
Cancer worry
Dispositional cancer worry was measured using an 8-item scale from Jensen et al. 21 Participants responded using a 7-point Likert scale ranging from not at all to very much. Dispositional cancer worry has two underlying dimensions: severity and frequency. Sample severity items include, “I feel anxiety when I think of the possible consequences of getting cancer” and “I brood about the physical consequences of getting cancer.” Sample frequency items include, “I have dreams about cancer” and “Pictures about cancer have popped into my mind.” Accordingly, four of the items measured cancer worry severity (M = 3.26, SD = 1.53, α = .86) and four measured cancer worry frequency (M = 1.39, SD = .85, α = .82).
Seeking and scanning
Seeking and scanning were measured in line with Shim et al. 7 For cancer information seeking, participants were asked “Have you looked for information about cancer from any source?” and “About how long ago was that?” The two items were combined into a single score that reflected whether they had looked for cancer information in the last year (coded as a 1) or not (coded as a 0), referred to as high and low scanners, respectively (M = .60, SD = .49). Scanning was measured using five items that asked, “How much attention do you pay to information about health or medical topics on/in [source]?” Participants reported information scanning for radio, television, newspapers, magazines, and the Internet using a 4-point scale (not at all, a little, some, and a lot). The last source (Internet) was not included in Shim et al. 7 but was added here due to increased use of the Internet as a source of health information (M = 2.64, SD = .62, α = .75). Scanning was transformed into a dichotomous measure by splitting the variable at 2.5 (in line with Shim et al. 7 ). Those above and below 2.5 were referred to as seekers and no seekers, respectively (M = .61, SD = .49). Information scanning focuses on health information in general (rather than cancer) per Shim et al. 7
Results
Seeking and scanning measures can be used to form a 2 × 2 information seeking/scanning table. The information seeking/scanning table categorizes participants as low-scan/no seekers, low-scan/seekers, high-scan/no seekers, and high-scan/seekers (see Table 1). In the current study, the largest category was the high-scan/seekers (40.2%).
2 × 2 categorization of participants as seekers/scanners.
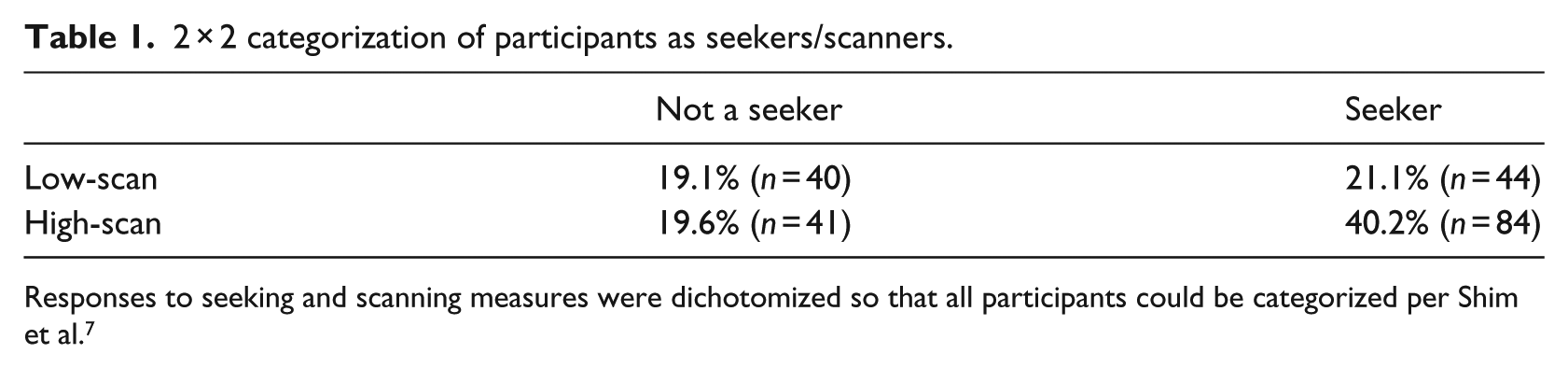
Responses to seeking and scanning measures were dichotomized so that all participants could be categorized per Shim et al. 7
H1 and H2 postulated that health information seeking and scanning would be negatively related to CIO. A two-way analysis of covariance (ANCOVA) was conducted with CIO as the outcome, seeking and scanning as fixed factors, and gender, age, and education as covariates. There was a significant main effect for seeking, F(1, 200) = 5.91, p = .016, r = .18, and a marginally significant main effect for scanning, F(1, 200) = 3.21, p = .075, r = .15. Consistent with H1, information seekers had lower CIO scores (M = 2.25, SD = .79) than those who did not seek cancer information (M = 2.52, SD = .71). Consistent with H1, information scanners had lower CIO scores (M = 2.27, SD = .72) than those who did not scan for cancer information (M = 2.50, SD = .82). There was also a marginally significant interaction between seeking and scanning, F(1, 200) = 3.04, p = .083. Post-hoc tests revealed that low-scan/no seekers had significantly higher CIO scores than participants in all other categories (see Figure 1).
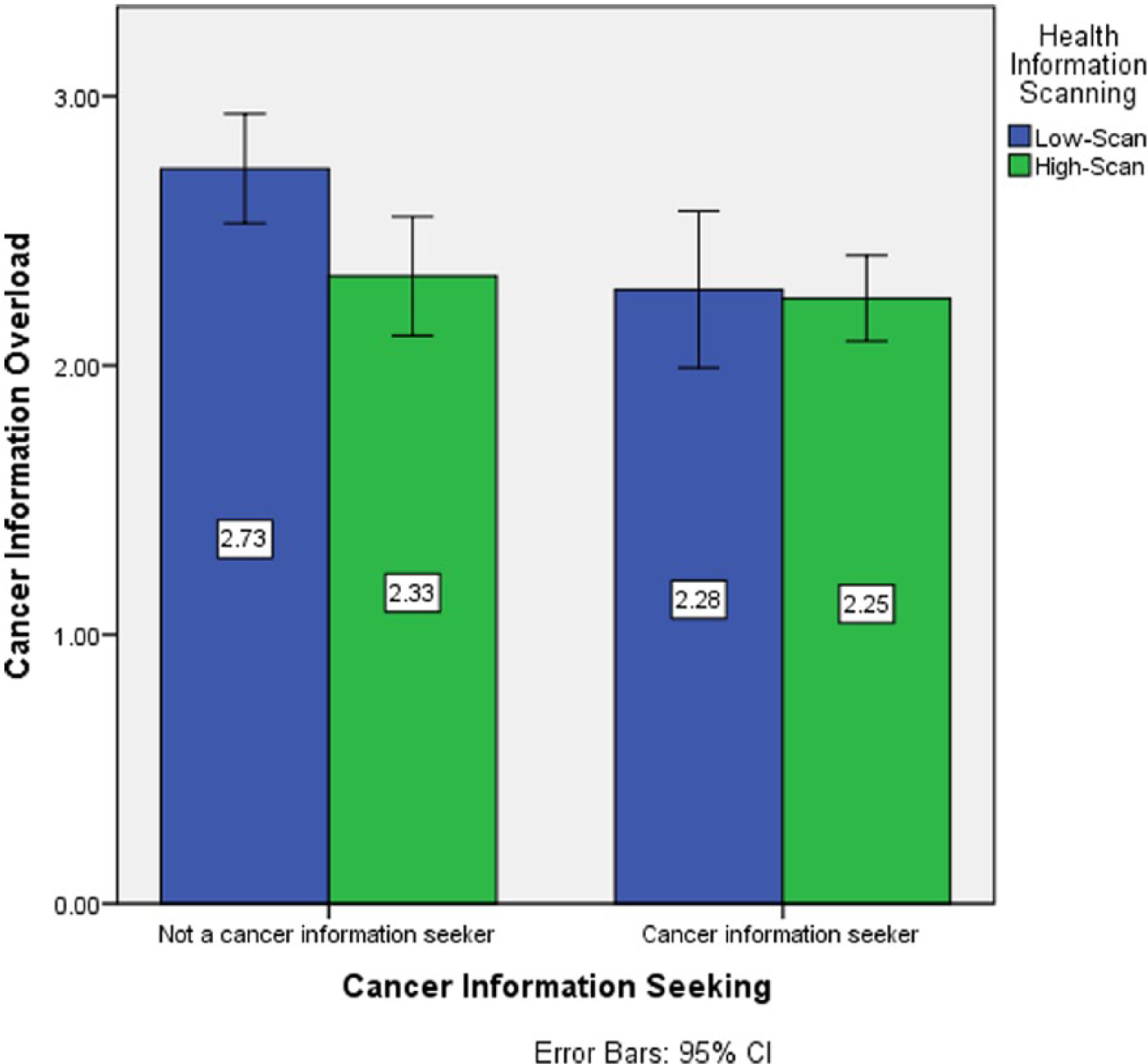
Cancer information overload (CIO) by seeking/scanning behavior. Bars present mean (in boxes) and 95 percent confidence intervals (brackets). Post-hoc tests revealed that low-scan/no seekers had the highest CIO scores.
RQ1 and RQ2 questioned the relationship between health information seeking and scanning and dispositional cancer worry. Two-way ANCOVAs were conducted with cancer worry severity/frequency as the outcome and all other variables identical to the CIO analysis. For cancer worry severity, there were no significant main effects for seeking, F(1, 193) = .10, p = .758, or scanning, F(1, 193) = .44, p = .508. There was a significant seeking × scanning interaction effect, F(1, 193) = 5.63, p = 019. Post-hoc tests revealed that low-scan/no seekers and high-scan/seekers had higher cancer worry severity scores than those in the other conditions (see Figure 2). For cancer worry frequency, there were no significant effects for seeking, F(1, 193) = 2.09, p = .150, scanning, F(1, 193) = .95, p = .331, or the seeking × scanning interaction, F(1, 193) = .75, p = .387.
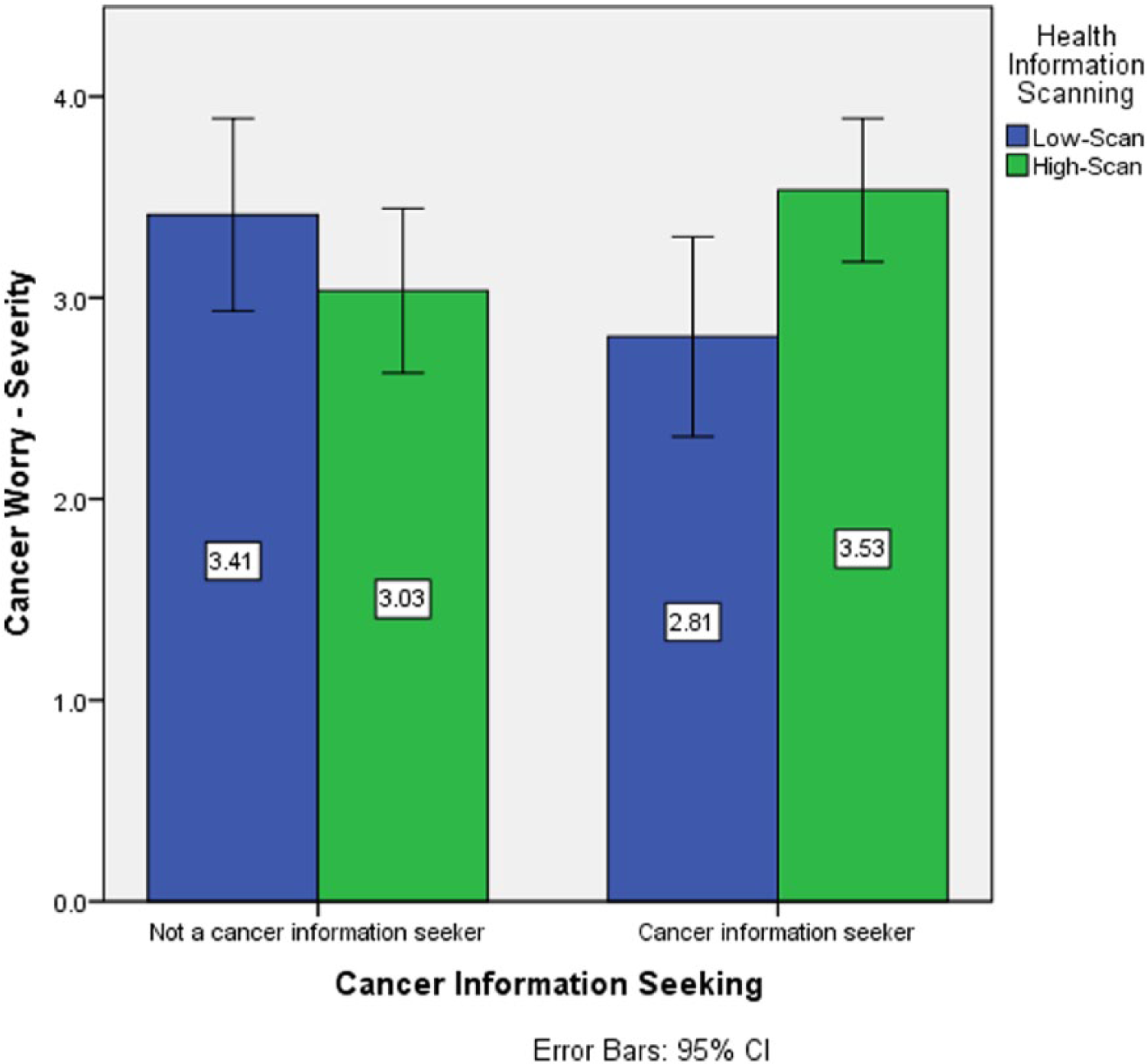
Cancer worry—severity (CWS) by seeking/scanning behavior. Bars present mean (in boxes) and 95 percent confidence intervals (brackets). Post-hoc tests revealed that low-scan/no seekers and high-scan/seekers had higher cancer worry severity scores than those in the other conditions.
Discussion
We tested the relationship between cancer information seeking/scanning and CIO. As expected, cancer information seeking and scanning was negatively related to CIO. Even though a significant effect was not found between information seeking and scanning and cancer worry, interestingly, the results did indicate a significant effect for the seeking × scanning interaction, with low-scan/no seekers and high-scan/seekers having higher cancer worry severity. The results of our study are consistent with the findings of Kim et al. 17 that information seeking is far from being a linear process or a single event. Overall, our study offers a preliminary analysis of the relationship between cancer information seeking and scanning and CIO.
This study also highlights the role of dispositional cancer worry as a two-dimensional concept. We used eight items to measure dispositional cancer worry, in an effort to address the limitations of previous studies that have either utilized single item measures or failed to specify the total number of items dedicated to worry. 69 Most research tends to assume that the relationship between negative affect and health prevention behavior is linear; 69 however, the relationship appears to be more complex than a linear relationship allows. This study reveals that the interaction between information seeking and scanning is significant for cancer worry severity. The fact that only low-scan/no seekers and high-scan/seekers have high cancer worry severity could be explained by several possibilities. Ramanadhan and Viswanath 70 indicated that non-seekers are those who have lower education and income, who typically score lower on attention to health in the media, and who are less trusting of health information from mass media. Since individuals with lower education and income have less resources and skills to seek health information, either from health professionals or from media channels, it is reasonable to assume that these people may have higher levels of cancer worry. For the high-scan/seeker group, previous research suggests that worry about one’s health is positively associated with online health information seeking. 68 Individuals who frequently experience cancer worry are more likely to actively seek and scan cancer-related information.
These results also shed light on cancer information seeking and scanning patterns of older populations. According to statistics revealed by the Administration on Aging (AoA), 71 the number of older US adults (persons who are 65 years or older) will be 72.1 million by 2030, more than twice the number in 2000. Older populations generally have more health problems than younger populations. There is evidence that the vast majority of cancer occurs in people aged over 50 years, 72 and this is also the group of people who are most likely to suffer from CIO—as information processing ability decreases with age. Future studies should more closely examine how older individuals cope with CIO and cancer worry.
The results of this study also point toward several actionable steps health practitioners can take to enhance cancer-related health behaviors. First, both highly active (high-scan/seekers) and inactive (low-scan/no seekers) exhibit high levels of cancer worry severity. The former are showing signs of active avoidance 50 which often stems from low efficacy. Moreover, low-scan/no seekers also exhibit high levels of CIO. Taken together, practitioners looking to reach highly inactive individuals/groups should avoid passive informational sources (e.g. pamphlets, brochures) in favor of interactive, efficacy promoting alternatives (e.g. personal stories about individuals successfully navigating challenges, games that teach basic skills). Second, approximately 60 percent of participants were passive in information seeking, scanning, or both. In a larger sense, this suggests practitioners should devote resources to promoting more active information seeking and scanning activities.
Limitations
This study has several limitations. The causal relationship between cancer information seeking/scanning and CIO still remains unclear. Even though we treat CIO as the outcome in the analysis, there remains the possibility that the level of overload also influences information seeking/scanning behaviors. Indeed, it seems more plausible to conceptualize the relationship between CIO and dispositional cancer worry as mutually causal, perhaps influencing one another slowly over time. A rigorous examination of this possibility will require a longitudinal design measuring CIO and dispositional cancer worry at multiple points in time. This is more than a semantic query as a mutually causal relationship would suggest that some of our theoretical frameworks might be a suboptimal fit. For example, the EPPM posits that worry triggers fear control which can take the form of backlash. 50 The current study conceptualized CIO as a form of backlash; yet this idea would appear flawed if the hypothesized one-directional relationship was instead mutually causal.
There are also other limitations that are worth noting. The measure we used for cancer information seeking and scanning is adopted from Shim et al.’s 7 study, which was originally created for the Health Information National Trends Survey (HINTS). The problem with the current measure of information scanning, as pointed out by Shim et al., 7 is that the wording of the measure may not represent the actual construct because it may confound attention to one medium with exposure to this medium. For the cancer information seeking measure, the two-item measure does not account for the frequency of information seeking/scanning behavior and the number of sources used. 40
Conclusion
In summary, the results of our study suggest that cancer information seeking and scanning is negatively related to CIO. Our data also show that the interaction between information seeking and scanning is associated with one underlying dimension of dispositional cancer worry: severity. This study sheds light on the importance of cancer information seeking and scanning patterns of older populations as well as offers support for a key postulate of the IOM: CIO is related to information avoidance. Future work should continue to explore the relationship between overload, information avoidance, and other cancer-related dispositions with the goal of explicating a single comprehensive theoretical framework to guide cancer control research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.