
Abstract
Background
While previous studies indicated that seeking online health information could reduce individuals’ cancer information overload, the results are inconsistent and have remained unknown in China. This study focuses on cancer patients’ family members to determine whether online health information seeking helps lessen cancer information overload and the processes underlying this association.
Objective
To examine the relationship between online health information seeking and cancer information overload through psychological empowerment and anxiety in the sequel, we carried out a quota sampling online survey in mainland China in 2023. We also looked at the underlying mechanism's moderated role in eHealth literacy.
Methods
We standardized all variables from 0 to 1 using a Min-max normalization and conducted Model 6 and Model 92 of Process Macro to examine the mediation and moderation effects. The final sample size was 628 cancer patients’ family members.
Results
We found that online health information seeking negatively impacted cancer information overload through psychological empowerment and anxiety (bp = −.007, CI: [−.013, −.002]). Specifically, online health information seeking was positively related to psychological empowerment (bp = .201, CI: [.149, .252]), which eased family members’ anxiety (bp = −.271, CI: [−.420, −.122]) and eventually reduced cancer information overload (bp = .120, CI: [.063, .177]). Moreover, we observed that while online health information seeking increased family members’ anxiety (bp = .126, CI: [.023, .228]), eHealth literacy served as a moderator to mitigate this association (bp = −.668, p < .05).
Conclusion
The findings can be used by healthcare workers, public health policymakers, and online health information providers to advise Chinese cancer patients’ family members about the overwhelming amount of information they may encounter when seeking online health information.
Keywords
Background
Cancer has become a considerable part of public health issues in China, affecting all involved. 1 Patients who have been diagnosed with cancer, their family members, and patients themselves would have large information needs. 2 When individuals seek and process information that exceeds their information-processing capacity, they will undoubtedly feel overwhelmed and experience information overload. Cancer information overload (CIO), a specific issue of information overload, is described as those who feel confused and overwhelmed when confronted with a large volume of cancer-related information. 3 Thus, CIO focuses on individuals feelings about the cancer information environment rather than their cognitions (e.g., cancer worry, perceived cancer risk, and cancer fatalism). 3
Health information seeking through media channels, such as print media and the Internet, has been identified as a major motivation-related indicator for the CIO4–6. However, previous studies have found that Internet use for online health information seeking (i.e., OHIS) either increased or decreased CIO.4,6,7 The mixed results are attributed to two factors. First, geographical disparities in sample selection provide inconsistent results. For example, while studies found that OHIS reduced CIO in a representative sample of the US population, 4 others found that OHIS increased CIO in Turkish respondents. 6 With the Internet's emergence as a significant source of health information for the Chinese, 8 the impact of OHIS on the CIO has not been well understood in China. Second, previous studies have not explored the underlying mechanisms of this relationship. Indeed, individuals who finally respond to an information environment are subject to cognitive and (or) emotional feedback.9–11. For instance, individuals who encountered the threat of COVID-19 information had the intention of information avoidance by experiencing anxiety and sadness (i.e., affective response) and cognitive dissonance (i.e., cognitive response). 9 Failing to explore the mechanisms that respond to the information environment could make explaining the differences in outcomes difficult. According to this, it is crucial to investigate the mechanisms between OHIS and CIO to understand the mixed findings in this relationship.
Based on previous studies, to better understand the functions of OHIS on CIO in the Chinese digital environment, the current study focuses on cancer patients’ family members (CPFMs), who are relatives of cancer patients and can provide physical, emotional, and practical support and help to cancer patients, 2 but are more prone to suffer from CIO. 4 In China, the National Health Commission has implemented lung, rectal, colon, and breast cancer screening and treatment programs in recent years, 12 as well as expanded its social media campaign. These have unavoidably increased the susceptibility and perceived risk to cancer information among Chinese CPFMs. Coupled with the fact that CPFMs already have high information needs and frequent OHIS,2,13,14 if they lack the information processing ability (e.g., CIO), this may have more detrimental health beliefs.15,16 Moreover, compared to patients’ self-determination in the Western healthcare system, the role of Chinese CPFMs are more likely to serve as “surrogate decision makers” in the Chinese healthcare system (e.g., exercising the right to information, choosing treatment options), 2 which makes CPFMs bear the double cognitive load of interpreting patients’ medical information and judging risks. The uniqueness of such “surrogate decision makers” makes the study of CIO in this group of people more ecologically valid. On these terms, focusing on CIO among Chinese CPFMs appears to be a more significant and challenging issue than focusing on other demographics.
Overall, the current study considered the functions of OHIS among Chinese CPFMs, and answered the following question: How does OHIS affect the CIO in China? We investigated (1) the underlying mechanisms between OHIS and CIO from the perspectives of interactions between organisms and the environment, and (2) potential disparities among groups with varying extents of eHealth literacy.
Theoretical framework
Of particular interest in this study is how OHIS affects CIO, the stimuli-organism-response model (S-O-R) provides a theoretical framework for better understanding the link between OHIS and CIO. S-O-R is proposed by Mehrabian and Russell 17 based on environmental psychology. They argued that individuals’ environmental factors in a specific environment could stimulate internal emotional states, which in turn shape individuals’ final cognition judgment and behaviors. In the S–O–R, various stimuli (S) that individuals can encounter in the environment could affect individuals’ various cognitive beliefs and affective responses, known as organisms (O). Eventually, individuals state and decide on certain environmental cues (R), such as whether to approach or avoid the environment. This model has been extensively applied by public health in studying health cognitive and affective functions18,19 and health decision-making20–22 in recent years and proved that the S–O–R model can effectively analyze the impacts of the resources of health information acquisition on health cognitive responses and health behavioral changes. In the current study, the S-O-R model can be employed to explore one possible underlying mechanism for managing information overload through OHIS. The Internet serves as a resource for individuals’ OHIS (S) may influence internal emotional states, that is, how individuals perceive health information (O), which in turn affects how they process it (R).
Hypotheses development
OHIS as stimuli
Information seeking is operationalized as active efforts to gather information, where people are motivated to seek out helpful and credible information and carefully assess it.23,24 Since the Internet “pulls” information to users at their accessible, rather than “pushes” information to the public, Internet users are eager to search for health information tailored to their needs online with less control.25,26 Thus, OHIS can be depicted as something that drives individuals to obtain, appraise, and adopt beneficial online health information purposefully27,28 via the Internet. CPFMs exhibit different preferences in various digital media29–31. It is worth noting that CPFMs’ responses to digital environmental stimuli are based on specific information needs, which are affected by their contextual factors, such as Chinese culture 2 and self-rated health. 13 First, Chinese culture emphasizes protecting patients from disclosing their medical condition. 32 Hence, the majority of CPFMs choose to conceal cancer results from patients to reduce their psychological load and have a surrogate make treatment decisions for them instead of patient autonomy.2,33 This encourages them to seek additional information to broaden their medical knowledge and help them with decision-making. Second, Confucianism is deeply rooted in Chinese people's mentality requiring family members and their patients to value close relationships and keep each other informed. 34 CPFMs are obliged to provide care for patients, 35 and patients highly rely on them for information sharing and supplementation. 13 Thus, CPFMs need information not just to become better carers for recipients, but also to support cancer patients with information.2,13,14 Lastly, previous studies showed that the majority of the issues that CPFMs wrote about are regarding their personal well-being on the Internet 36 and CPFMs with lower self-rated health were more likely to seek health information on their health, 13 which suggests that CPFMs have started to focus on their health conditions and the lack of health information available for themselves.
Cognitive and Affective Organisms
Given these specific information needs, CPFMs respond to OHIS stimuli in two primary ways: cognitive and affective responses. These responses are strongly correlated with the self-health condition and well-being of CPFMs. On the one hand, OHIS could arouse individuals’ agency. For instance, OHIS could promote health self-management among groups with chronic diseases,37,38 as well as Chinese older adults’ patient activation. 39 Likewise, it could have the power to reawaken the agency of self-care among CPFMs, i.e., psychological empowerment, while the fact that CPFMs have a common lower confidence in self-care. 40 Psychological empowerment refers to the process of enhancing individuals’ ability to make decisions and turn those decisions into behaviors and results. 41 OHIS arousing CPFMs’ psychological empowerment is mainly influenced by the existing intervention programs of health-promoting self-care. Health-promoting self-care emphasizes the ability of individuals to take care of their own wellness and health. It can help individuals make healthier decisions and develop self-responsibility, or accountability for their actions, in relation to their health.42,43 Various Internet channels serving as educational platforms provided health-promoting self-care intervention programs for CPFMs, such as psycho-education and healthy behaviors recommendations,43,44 motivating CPFMs to take personal responsibility for their health43,45 and fuelling self-health management efficacy to obtain self-related knowledge and skills instead of disregarding their health.
On the other hand, OHIS could also trigger negative emotional states. A systematic review and meta-analysis showed that online health information seeking was more likely to result in health anxiety. 46 Scholars believe that OHIS could be driven by a desire to meet individuals’ informational needs and objectives as well as uncertainty regarding health-related concerns. 47 Consequently, individuals who actively find health information were more prone to develop threatening beliefs, overestimate their medical condition, and exaggerate their anxiety when they perceive danger or interpret threats ambiguously. 46 In turn, anxiety can trigger behavioral changes that strengthen negative perceptions about health, creating a vicious cycle. 48 Long-term and uncertain information seeking may, in particular, make CPFMs feel more threatened by information about cancer, causing self-doubt and psychological load. Moreover, CPFMs may be more likely to experience cancer-related anxiety49,50 because of their higher chance of inheriting cancer.51,52 Consequently, participation in OHIS might amplify these unfavorable feelings. Therefore, we proposed the following hypotheses.
H1: OHIS is positively associated with psychological empowerment.
H2: OHIS is positively associated with anxiety.
CIO as response
When the cognitive and affective organisms contribute to the Internet information environment jointly, Nahl 53 suggested a serial interactive effect between affection and cognition, in which high cognitive skills can positively alter affective states and affective responses can positively promote subsequent cognitive processes. That is, individuals’ online information processing begins with a proximal cognitive response, which changes their distal affective states and ultimately affects their cognition. Empirical studies have found that psychological empowerment could be effective in negative affective states. 54 For instance, psychological empowerment (i.e., agency of self-care) strengthened individuals’ positive affect and reduces their psychological burden. 43 Thus, psychological empowerment could be regarded as a potential way to reduce CPFMs’ anxiety. Moreover, existing studies have consistently held that anxiety unavoidably could cause CIO.4,55,56 This is because individuals in negative affective states may selectively attend to threat-related information rather than knowledge and then may interpret such information as frightening or depressing,57,58 which could hinder the information-processing ability and results in CIO. Thereby, anxiety may have an immediate role in final cognitive processing. Building up those theoretical and practical findings, we proposed the following hypotheses:
H3: Psychological empowerment is negatively related to anxiety.
H4: Anxiety is positively associated with CIO.
The moderated role of eHealth literacy
Combining information and media literacies, eHealth literacy refers to an individual's ability to locate, understand, and evaluate health information using digital technology, and then use that capacity to address or resolve a health issue.59,60 According to previous studies, eHealth literacy has exacerbated cognitive and affective differences in the digital age when individuals were seeking online health information.10,61 Likewise, when it came to evaluating online health information for cancer decision-making, CPFMs with lower eHealth literacy levels were less confident. 62 The caregiver burden was higher for CPFMs with lower education levels (i.e., less than high school education), which was influenced by eHealth literacy. 63 Nonetheless, examining the moderating effect of eHealth literacy on the hypotheses is the main goal of the current study. Previous research has identified the moderating role of eHealth literacy64–66. For instance, eHealth literacy against emotional distress was associated with OHIS. 66 Individuals with higher eHealth literacy could reduce the effect of OHIS on emotional distress, whereas this association was stronger among those who had less eHealth literacy. Overall, eHealth literacy could function as a positive moderating role in health promotion in the digital environment. Examining the various eHealth literacy levels among CPFMs and the possible differences in the OHIS stimuli to organisms and responses is essential for educating and intervening in CPFMs’ physical and mental health management. Therefore, we proposed the following hypotheses.
H5a: eHealth literacy can positively moderate the association between OHIS and psychological empowerment among CPFMs.
H5b: eHealth literacy can negatively moderate the association between OHIS and anxiety among CPFMs.
H5c: eHealth literacy can negatively moderate the association between psychological empowerment and anxiety among CPFMs.
H5d: eHealth literacy can negatively moderate the association between anxiety and CIO among CPFMs.
The conceptual model is shown in Figure 1.

Conceptual model.
Method
Design and participant
The authors’ institution approved the study on September 13, 2022. Prior to the survey going online, the English survey with all items mentioned were translated into Chinese by PhD students, who then used back-translation to ensure the translation was accurate. 20 master's graduates participated in the questionnaire pretest, during which we collected feedback on the conciseness, content design, and any other issues they may have had. The questionnaire was slightly modified in response to their comments. The formal survey was conducted in 31 provinces across mainland China between June 11 and October 12, 2023. The online survey link was emailed to participants who were recruited by Qualtrics (https://www.qualtrics.com/) and gave written informed consent before participation. We conducted a quota sampling by the Seventh National Population Census 67 with a focus on age and gender distribution. The criteria for CPFMs included adults who were at least 18 years old and had a first- or second-degree family member(s) (e.g., parents, brothers and sisters, children, grandparents, aunts and uncles, nieces and nephews) with a history of cancer. CPFMs who were unsure of their family history of cancer, however, were not included. Following listwise deletion to exclude missing values, this study included a total of 628 cancer family members.
Measurement
Cancer information overload was measured using five items derived from a modified 8-item CIO scale suggested by Costa and his colleagues. 68 The respondents were asked to indicate the extent of perceived CIO with a five-point Likert scale (from 1 = strongly disagree to 5 = strongly agree). We averaged these scores to measure CIO and a higher score indicated a stronger agreement with the statement (M = 3.32, SD = 0.79, Cronbach's α = .82).
Similar to previous studies,69,70 online health information-seeking behavior was measured by three items respondents reported the frequency of seeking health information to three Internet-based media channels by a four-point Likert scale (from 1 = never to 4 = always), including website, mHealth app, and social media. A new variable (OHIS) was developed by averaging three items (M = 3.07, SD = 0.62, Cronbach's α = .66).
The first mediator, psychological empowerment, was adapted from the Psychological Empowerment Scale. 71 Consistent with the study done by S. Jiang and Street, 72 respondents were asked to evaluate the extent of their empowerment across eight items, using a five-point Likert scale (from 1 = strongly disagree to 5 = strongly agree). We averaged scores to assess psychological empowerment with higher scores indicating more agreement with the statement (M = 4.01, SD = 0.57, Cronbach's α = .85).
The second mediator, anxiety, was measured using a previously validated two items anxiety scale. 73 Respondents were asked to assess their anxiety with a four-point Likert scale (from 1 = none to 4 = every day). Anxiety was averaged by these scores (M = 1.74, SD = 0.77, Cronbach's α = .77), with higher scores indicating more severe anxiety symptoms.
The moderator, eHealth literacy, was measured using eHealth literacy scale with eight items. 74 Respondents were asked to evaluate the extent of their eHealth literacy using a five-point Likert scale (from 1 = strongly disagree to 5 = strongly agree). We averaged these scores to assess respondents’ level of eHealth literacy. (M = 3.89, SD = 0.60, Cronbach's α = .84).
Finally, the control variables in this study were four sociodemographic variables: age, gender, personal income, education and marital status.
Data analysis
All the mediation pathways in this study were analyzed by SPSS (v26) and Process Macro. 75 First, we tested the relationships among all key variables by a Pearson correlation test. Then, to better understand the impacts and make comparisons of variables, we standardized all variables with the range of 0 to 1 using a Min-max normalization, often known as a percentage scale (bp). 20 We conducted Model 6 and Model 92 of Process Macro 75 to examine the mediation and moderation effects. The P-value was calculated to evaluate statistical examination, and 95% confidence intervals (CIs) were used to estimate the effects of all variables with 5000 bootstrapped samples.
Results
Preliminary analysis
As shown in Table 1. The average age of CPFMs in this study was 39.32 years, with 47.0% male and 53.0% female. 20% of CPFMs reported that they had completed high school or less, 32.8% of them reported that personal income increased between 5001 and 8000 RMB per month, and 79.1% were married. Furthermore, almost all CPFMs (99.4%) reported that they used at least one Internet channel to seek health information. Websites was the most prevalent Internet channel for OHIS in this study. Notably, at least 31.3% of CPFMs reported suffering varied degrees of CIO-related distress, approximately 60% reported having higher levels of anxiety than the mean level, and 47% of CPFM had poorer eHealth literacy than the medium level.
Descriptive characteristics of the sociodemographic and related variables.

Note. M: mean; SD: standard deviation.
Bivariate correlation results revealed significant relationships between most essential variables. Specifically, OHIS, psychological empowerment, anxiety, and eHealth literacy have a positive link with CIO (Appendix 1). The descriptive statistics are shown in Table 1, and the results of bivariate correlations are presented in Table 2.
Zero-order correlation of predicting CIO.

Note. * p < .05; ** p < .01; *** p < .001.
Control variables: age, gender, education, personal income, marital status; CIO: cancer information overload; OHIS: online health information seeking; PSE: psychological empowerment.
Mediation and moderation analysis
H1 predicted that OHIS was positively associated with psychological empowerment. As shown in Table 3 and Figure 2, the association between OHIS and psychological empowerment was statistically significant (bp = .201, CI: [.149, .252]). Thus, H1 was supported.

The results of hypotheses testing. Note. bp stands for percentage scale; *P < .05; **P < .01; ***P < .001.
Path analysis testing the mediation and moderation models.

Note. Control variables: age, gender, education, personal income, marital status; bp: percentage scale; SE: standard error; CI: confidence interval; CIO: cancer information overload; OHIS: online health information seeking; PSE: psychological empowerment.
H2 predicted that OHIS was positively associated with anxiety. The results statistically acknowledged this association (bp = .126, CI: [.023, .228]). H2 was supported.
H3 predicted that psychological empowerment was negatively related to anxiety. Table 3 demonstrated a statistically significant negative correlation between anxiety and psychological empowerment (bp = −.271, CI: [−.420, −.122]), supporting H3.
H4 predicted that anxiety was positively associated with CIO. As shown, the positive association between anxiety and CIO was significant (bp = .120, CI: [.063, .177]), supporting H4. Based on the results of H1, H3, and H4, a sequel mediation involving psychological empowerment and anxiety was observed between OHIS and CIO (bp = −.007, CI: [−.013, −.002]),
Regarding H5, H5a predicted that eHealth literacy played a positive moderating role in the association between OHIS and psychological empowerment among CPFMs. However, the moderating effect was not significant (bp = −.039, P > .05), and H5a was not supported.
H5b predicted that eHealth literacy played a negative moderating role in the association between OHIS and anxiety among CPFMs. Our results showed that this moderating effect was statistically acknowledgeable (bp = −.668, P < .05), supporting H5b. As shown in Figure 3, when seeking online health information more frequently, CPFMs with higher eHealth literacy experienced a slight reduction in anxiety (Mean + 1SD), whereas, CPFMs in the medium (Mean) and lower (Mean-1SD) groups felt considerably more anxious.
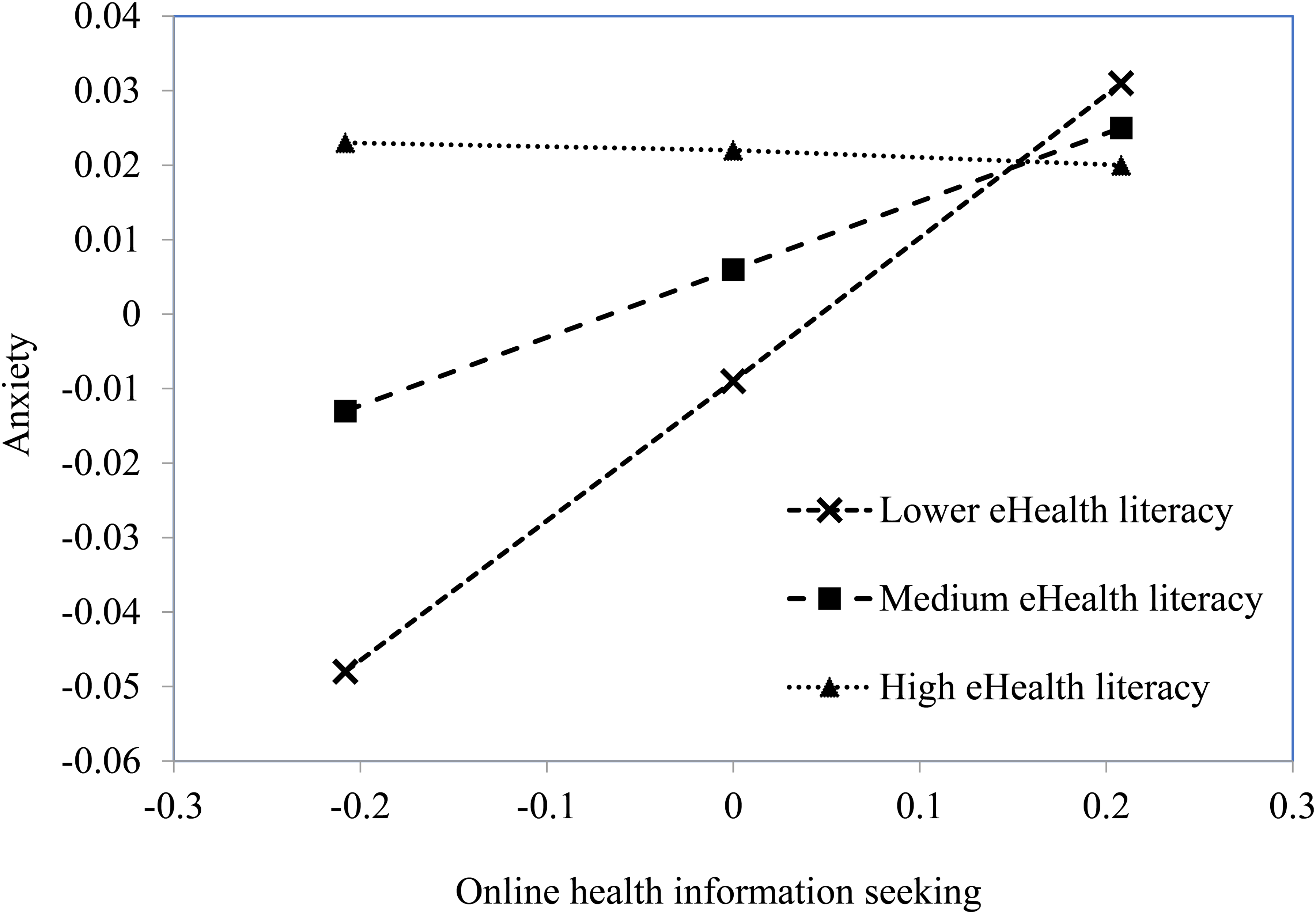
The moderating effect of eHealth literacy on the association between OHIS and anxiety.
H5c predicted that eHealth literacy played a negative moderating role in the association between psychological empowerment and anxiety among CPFMs. However, there was no statistical significance (bp = .453, P > .05). H5c was not supported.
H5d predicted that eHealth literacy played a negative moderating role in the association between anxiety and CIO among CPFMs. The moderating effect was not significant (bp = .059, P > .05), and H5d was not supported.
Discussion
The association between OHIS and CIO
Inspired by S-O-R, our study contributes to the existing literature on the association between OHIS and CIO4,6,7 by shedding light on the mechanisms of this association in the Chinese digital environment among the highly vulnerable group of CPFMs. We revealed the two critical responses of OHIS among CPFMs, namely psychological empowerment and anxiety, and identified two distinct pathways linking OHIS and CIO. Specifically, OHIS could exacerbate CPFMs’ anxiety and thereby improve CIO, whereas OHIS could relieve CIO by enhancing CPFMs’ psychological empowerment and subsequently decreasing their anxiety. These findings could clearly explain the mixed findings in previous studies,4,6,7 which point to several underlying mechanisms that either increased or decreased CIO. Details are discussed in this section below.
It is acknowledged that anxiety has a detrimental influence on OHIS facilitating CIO among CPFMs. As shown in our results, anxiety is commonplace among CPFMs; nearly 60% of them had higher levels of anxiety than the average level. The heightened anxiety experienced by CPFMs is more likely to stem from their unique psychological and physical vulnerability rooted in familial cancer history.51,52 Critically, CPFMs’ anxiety could get worse with the increased uncertainty of OHIS. 46 Chronic engagement in this situation does not merely increase anxiety; it actively impairs rational information processing. 4 This finding highlights that improving the negative influence of anxiety in this mechanism seems to need a crucial yet important first step: lowering anxiety.
Our results, fortunately, demonstrated that OHIS can lessen anxiety by encouraging psychological empowerment and eventually hinder the CIO. Such a finding is particularly significant for CPFMs, who often suffer from higher health anxiety. 76 Compared to blind OHIS creating anxiety with uncertainty, intentionally seeking and processing health information, such as health-promoting self-care intervention programs,43,77 could improve their capacity for knowledge evaluation, self-determination, and self-health management effectiveness while encouraging individual accountability for their health.43,78,79 Thus, CPFMs may be able to prevent unnecessary worries about their health problem and lessen the cognitive impairment brought on by redundant information. As a result, OHIS-enhanced psychological empowerment serves as a nearby yet advantageous factor that elevates affective moods. CIO may be further decreased by this follow-up mediation. Our findings theoretically highlight the sequentially interactive effect of affection and cognition on health information in the online environment.
Moreover, our results are in line with the indirect-only mediation, with an indirect effect existing, but no direct effect, 80 indicating that CIO may not immediately influence CPFMs by merely looking for health information online. This is consistent with previous studies, instead of directly influencing patients’ health outcomes (such lifestyle management and emotional well-being), OHIS could affect them through psychological and cognitive processes like self-motivation and cancer attitude.39,81 Both indirect and direct effects provide theoretical insight into analysing whether and how OHIS positively or negatively affects CIO, demonstrating that elucidating the relationship between OHIS and CIO requires exposing the fundamental mechanism rather than just linking them. Further studies could explore more elements and underlying mechanisms to reveal this complicated association.
The moderated role of eHealth literacy
The current study identified variations in the association between OHIS and CIO among groups with varying eHealth literacy, providing an alternative method of OHIS lowering CIO and new insights into understanding previously inconsistent findings. Our results showed that eHealth literacy moderated affective response (i.e., anxiety), but not cognitive responses (i.e., psychological empowerment and CIO). This implies that eHealth literacy as a skill is another crucial and extra stimulus that could influence the affective response by acting as a moderator. 82 In other words, the reduction of OHIS-induced anxiety can be improved with further eHealth literacy development. Accordingly, CPFMs in the medium and lower literacy groups would experience significant anxiety when seeking online health information. This is particularly crucial for the Chinese CPFM population. In China, CPFMs have massive information needs,2,83 and eHealth literacy could play a pivotal role in building positive expectations toward information sources. 84 However, lower eHealth literacy is one of the most critical causes of reducing their trust in information access, 84 making CPFMs have difficulty in seeking information with clearer search aims and assessing information more objectively and scientifically. 85 This moderation suggests that digital literacy interventions should systematically integrate affective training modules alongside traditional information literacy components, enabling healthcare practitioners to observe the positive functions of eHealth literacy in reducing negative feelings and encouraging CPFMs to develop their eHealth literacy along with affective training.
Moreover, the findings on eHealth literacy may enhance theoretical discussions regarding its conceptual framework. Existing studies on eHealth literacy indicated that eHealth literacy included multi-dimensional components such as cognitive and affective dimensions.10,86,87 While previous studies failed to identify the affective dimensional role of eHealth literacy on cancer worry from a moderation perspective, 10 this study provides empirical support for the affective intervention on anxiety, highlighting how eHealth literacy can have different affective effects on affective buffering in information management. Future studies could track the dynamic impact of emotional literacy through a longitudinal design to show its functions in various contexts. Furthermore, our study has not found a significant moderated role of eHealth literacy on cognitive response (i.e., psychological empowerment) among CPFMs, which suggests that the cognitive dimension of eHealth literacy may not operate uniformly across all populations.84,88 The issue of disparities in application within current conceptual frameworks must be acknowledged. Specifically, our findings highlight that it is context-dependent, especially in cancer patients-family member dynamics, where its cognitive benefits may be diminished by emotional strain, time constraints, or relational complexities. This is in contrast to previous studies that positioned eHealth literacy as a unidirectional enhancer of health-related cognition.
Implications and limitations
This study has several practical implications. First, given the significant indirect effects of OHIS and CIO, as well as the insignificant direct effect in this relationship, healthcare providers and health education institutions ought to recognize the essential elements in this association. Second, we adapted S–O–R to reveal the complicated information filtering when CPFMs seek online health information, indicating empowerment's critical bridging role in this association. Healthcare workers and governments should provide positive insight into the CPFMs’ psychological intervention from OHIS and utilize online channels to promote and educate them. Third, given the positive moderating role of eHealth literacy, enhancing CPFMs’ information literacy skills is just as important as lowering anxiety toward online health information. Health information providers could use this finding to effectively coach and teach CPFMs how to handle their psychological burdens and enhance their information-processing abilities.
Some limitations should also be noted in this study. First, the cross-sectional and self-reported survey was done to only examine the effects of OHIS on CIO through two mediators (i.e., psychological empowerment and anxiety) during a limited period. Further studies could consider conducting panel data to investigate the variations in other cognitive and affective responses among Chinese CPFMs over time. This would provide a comprehensive understanding of the long-term consequences of online information seeking on information-processing abilities. Second, previous studies found that cancer and non-cancer OHIS resulted in different CIO outcomes.4,5,7 However, we only examined the effects of general health information seeking on CIO in this study; further studies could focus on cancer information seeking to explore its implications on CIO. Third, Niederdeppe and his colleagues 89 have stated that individuals would come across cancer information while scanning. Exposure to cancer-related material or scanning information might also have a potential impact on CIO. Thus, we suggest additional studies into the effects of health information-scanning behavior on CIO to compensate for this study's limitation of measuring only active health information-seeking behaviors.
Conclusion
In the digital environment, OHIS presents a dual-edged weapon for health promotion. Understanding its positive side is more practicable for health practitioners. Through practical implications for enhancing CPFMs’ cognitive response and reducing their negative affective response, this study investigated the underlying mechanisms that explain how OHIS helped to mitigate CIO in Chinese CPFMs. Moreover, CPFMs with higher eHealth literacy having less anxiety throughout their OHIS indicated that the extra stimuli could also directly influence affective responses. A deeper understanding of these relationships can guide healthcare workers, policymakers, and health information providers to utilize online sources to increase instructional effectiveness for CPFMs.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251336308 - Supplemental material for Linking online health information seeking to cancer information overload among Chinese cancer patients’ family members
Supplemental material, sj-docx-1-dhj-10.1177_20552076251336308 for Linking online health information seeking to cancer information overload among Chinese cancer patients’ family members by Yifang Wu, Luxi Zhang and Xinshu Zhao in DIGITAL HEALTH
Footnotes
Abbreviations
Ethical considerations
The study was approved by the University of Macau (SSHRE22-APP065-FSS) on September 13, 2022.
Consent to participate
All participants provided written informed consent before participating.
Author contributions/CRediT
Yifang Wu: Conceptualization; writing – original draft (equal). Luxi Zhang: writing - review and editing; software. Xinshu Zhao: Writing – review and editing; supervision; funding acquisition. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Universidade de Macau (grant number CRG2021-00002-ICI, ICI RTO-0010-2021, CPG2023-0000).
Conflicting interests
All participants provided written informed consent before participating.The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data will be available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Appendix 1
Measurement wording and variable construction (N = 628)
1. CIO, cancer information overload, Q. How do you agree with the following statement?
Strongly disagree
Disagree
Somewhat
Agree
Strongly agree
Total
Right: coding
1
2
3
4
5
1. There are so many different recommendations about preventing
cancer, it's hard to know which ones to follow.
3.8
9.2
30.3
42.4
14.3
100
2. It has gotten to the point where I don’t even care to hear new information about cancer.
5.9
25.8
31.5
26.1
10.7
100
3. Information about cancer all starts to sound the same after a while.
3.2
14.6
33.6
37.9
10.7
100
4. I forget most cancer information right after I hear it.
4.3
25.8
23.7
33.4
12.7
100
5. I feel overloaded by the amount of cancer information I am supposed to know.
5.1
19.6
28.0
36.3
11.0
100
2. OHIS, online health information seeking. Q. How often do you use the following media platforms for health information?
Never
Sometimes
Usually
Always
Total
Right: coding
1
2
3
4
1. Search engines
3.2
17.0
41.4
38.4
100
2. mHealth app
4.5
17.4
50.5
27.7
100
3. Social media
3.8
18.0
48.1
30.1
100
3. PSE, psychological empowerment. Q. How do you agree with the following statement?
Strongly disagree
Disagree
Somewhat
Agree
Strongly agree
Total
Right: coding
1
2
3
4
5
1. I will make use of necessary means and goods to effectively manage health
2.9
3.0
15.1
59.9
19.1
100
2. I can understand my disease better than anyone
0.5
3.5
19.7
49.7
26.6
100
3. I can motivate myself to manage my health and make a better life
1.0
2.9
14.6
56.5
25.0
100
4. I can make every possible effort to achieve health goals
0.5
1.9
15.8
49.7
32.2
100
5. I am enthusiastic about my own efforts to manage health
1.0
2.7
12.4
50.2
33.8
100
6. I know where I can ask for help to manage my disease
0.5
4.3
13.5
53.5
28.2
100
7. I can manage my disease conditions
0.8
2.9
18.6
50.5
27.2
100
8. I can make a realistic health plan
0.6
4.0
23.4
49.8
22.1
100
4. Anxiety. Q. How often have you been bothered by any of the following problems?
Not at all
Several days
More than half the days
Nearly every day
Total
Right: coding
1
2
3
4
1. Feeling nervous, anxious, or on edge
48.1
36.8
10.2
4.9
100
2. Not being able to stop or control worrying
45.7
37.9
11.0
5.4
100
5. eHealth literacy. Q. How do you agree with the following statement?
Strongly disagree
Disagree
Somewhat
Agree
Strongly agree
Total
Right: coding
1
2
3
4
5
1. I know how to find helpful health resources on the Internet
1.8
2.4
19.9
55.4
20.5
100
2. I know how to use the Internet to answer my health questions
0.2
4.5
18.3
53.7
23.2
100
3. I know what health resources are available on the Internet
0.8
3.7
22.1
51.0
22.5
100
4. I know where to find helpful health resources on the Internet
0.6
4.3
20.1
48.1
26.9
100
5. I know how to use the health information I find on the Internet to help me
1.0
3.0
18.2
54.6
23.2
100
6. I have the skills I need to evaluate the health resources I find on the Internet
0.3
5.3
29.3
44.3
20.9
100
7. I can tell high quality from low-quality health resources on the Internet
1.1
6.4
24.7
47.6
20.2
100
8. I feel confident in using information from the Internet to make health decisions
1.3
6.2
26.0
43.5
23.1
100
7. AGE. Q. What is your age? (Min = 18, Max = 70) 8. Gender. Q. On your original birth certificate, were you listed as male or female? Recoding as 1 for males (47.0%) and 0 for females (53.0%). 9. Education. Q. What is the highest grade or level of schooling you completed?
Response range
Below primary school
Middle school
Post high school
Some college
College graduate above
Total
Coding
1
2
3
4
5
Frq. (%)
1.9
4.1
14.0
29.8
50.2
100
10. Income range. Q. What is the range of your personal income per month?
Response range (¥)
5000 and below
5001∼ 8000
8001 ∼ 12,000
12,001 ∼ 20,000
20,001 and above
Total
Coding
1
2
3
4
5
Frq. (%)
18.6
29.9
32.8
12.4
6.2
100
11. Marital status. Q. What is your marital status?
Response range
Married
Cohabite
Divorced
Widowed
Separated
Single
Total
Coding
1
2
3
4
5
6
Frq. (%)
74.7
4.5
0.6
0.8
1.3
18.2
100
12. CPFM, cancer patients’ family members. Q. Have any of your first- or second-degree biological relatives (parents, brothers and sisters, children, grandparents, aunts and uncles, nieces and nephews) ever had cancer?
Response range
Yes
No
Not sure
Total
Coding
1
2
3
Frq.(%)
628
3844
429
4901
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.