
Abstract
Backgrounds
Thanks to their accessibility and low cost, electronic personal health information (ePHI) technologies have been widely used to facilitate patient–physician communication and promote health prevention behaviors (e.g. cancer screening). Despite that empirical evidence has supported the association between ePHI technology use and cancer screening behaviors, the underlying mechanism through which ePHI technology use influences cancer screening behaviors remains a topic of discussion.
Objective
This study investigates the relationship between ePHI technology uses and cancer screening behaviors of American women and examines the mediating role of cancer worry.
Methods
Data for this study were from the Health Information National Trends Survey (HINTS) collected in 2017 (HINTS 5 Cycle 1) and 2020 (HINTS 5 Cycle 4). The final sample included 1914 female respondents in HINTS 5 Cycle 1 and 2204 in HINTS 5 Cycle 4. Mann–Whitney U test, two-sample t-test, and mediation analysis were performed. We also referred to the regression coefficients generated by min–max normalization as percentage coefficients (bp) for the comparison.
Results
This study reports increased usage of ePHI technologies (from 1.41 in 2017 to 2.19 to 2020), increased cancer worry (from 2.60 in 2017 to 2.84 in 2020), and a stable level of cancer screening behaviors (from 1.44 in 2017 to 1.34 in 2020) among American women. Cancer worry was found to mediate the ePHI effect on cancer screening behaviors (bp = 0.005, 95% confidence interval [0.001, 0.010]) in a positive complementary mediation in 2020.
Conclusions
The research findings support a positive association between ePHI technology use and cancer screening behaviors, and cancer worry has been identified as a salient mediator. An understanding of the mechanism that prompts US women's cancer screening practices provides practical implications for health campaign practitioners.
Keywords
Introduction
Breast and cervical cancers are the two most common cancers among American women, 1 with an estimated 290,560 women diagnosed with breast cancer and 14,100 women with cervical cancer by 2022 according to the American Cancer Society. 2 It is observed that less than 1% of all diagnosed breast cancers are found in men. As per the estimates for the year 2022, around 2700 men were anticipated to develop this condition, which is significantly lower than the number of women affected, which is approximately 287,000. 3 Women with these cancers have 5-year survival rates at or better than 90% if discovered at a localized stage.4,5 Due to the high survival rate of breast and cervical cancers, numerous public health programs, including the National Breast and Cervical Cancer Early Detection Program, have emphasized the importance of regular screening and early detection of breast and cervical cancers. Diagnosing cancer earlier enables more treatment options and increases the chances of survival. 6 Despite that screening tests are recommended for early diagnosis and treatment of cancer, statistics showed that the cancer screening rate among American women was still low. Healthy People 2030 recommendations strive to boost the percentage of women receiving uterine cancer screenings to 84%. Despite this, recent data indicate that approximately 10% of women between the ages of 21 and 65 have not undergone a cervical cancer screening within the past 3 years. 7
Electronic personal health information (ePHI) technology use refers to the use of information communication technologies, such as the Internet, mobile phones, or wearable devices, to link healthcare workers with one another and with patients and families in order to provide safer, more reliable, effective, equitable, and sustainable quality care, and plays a salient role that may elicit screening behaviors. 8 Mounting scientific evidence consistently shows that the usage of ePHI technologies may contribute to health promotion goals.9,10 According to Kreps and Neuhauser, 11 ePHI technologies can activate and engage patients in the health-decision-making process, and enhance their compliant health behaviors. Compared to traditional health intervention tools, ePHI technologies, on the one hand, provide patients with more diverse information channels, prompting patients to further consult with medical professionals to be able to make a comprehensive evaluation of their cancer risk. 8 On the other hand, the diversity of ePHI technologies can also be considered a useful resource for cancer care. Patients can take advantage of the multi-component combination of ePHI technologies (e.g. social media and online groups for social support) to engage in health care. 12 For example, people reporting poor health status can use a variety of services in the electronic health records (EHRs) system to track their medical records and seek more relevant information. However, most research on the use of ePHI technology over the past years has primarily focused on identifying antecedent factors of ePHI technology uses, such as literacy, household income, and education levels.13,14 Our knowledge about how ePHI technology uses impacts people's health-related attitudinal and behavioral change remains scattered and incomplete. Although the positive association between ePHI technology uses and health behaviors has been documented in some studies,15,16 scholars suggest that there is more than a bivariate relationship between ePHI use and health behaviors, and research scrutinizing the mediation mechanisms is called for. In the cancer prevention and control literature, scholars have proposed various models and theories on the mediation mechanism by which emotion impacts technology adoption and health behaviors (e.g. somatic marker hypothesis and behavioral affective association model). For example, the somatic marker hypothesis17,18 has highlighted that emotion can serve as a cognitive shortcut that simplifies complex processes in decision-making behavior. Similarly, the stimulus-organism-response (S-O-R) framework also emphasized the primitive role of emotion between environmental stimuli and human behavior. In the context of cancer screening, as the use of ePHI technology can enhance patients’ awareness/consciousness of consuming health-related information, a positive relationship between ePHI technology use and cancer worry may exist. While existing theories support this reasoning, research regarding the positive relationship between ePHI technology use and cancer screening behaviors is currently lacking. In this study, we argue that cancer worry may mediate the impact of ePHI technology use on cancer screening behaviors.
Hence, given the sustained evolution of ePHI technologies, it is practically and theoretically significant to: (1) identify and quantify whether the associations between ePHI technology use and cancer screening behaviors have changed over time; and (2) explore the mediation mechanism of ePHI technology use and cancer screening behaviors. Inspired by the S-O-R framework, this study used two iterations of a nationally representative survey, the Health Information National Survey (HINTS), from 2017 to 2020, to propose and test mediation pathways linking ePHI technology uses to cancer screening behaviors.
ePHI technology use and cancer screening behaviors
The benefits of using ePHI technology in healthcare include patient-provider convenience and ease of accessing health-related information, and it allows healthcare providers to provide personalized feedback to patients.19,20 Previous research has shown the vital role of ePHI in increasing health-related awareness and improving cancer prevention behaviors.21–23 For instance, ePHI technology, including EHRs, can effectively remind at-risk women patients about breast and cervical cancer screening through follow-up visits or regular reminders, thereby improving the quality of communication between providers and patients. 24 Liu 25 highlighted the impact of ePHI technology on women's health. Specifically, Internet-based ePHI technologies allow people to obtain health information and engage in health management activities (e.g. online health consultation) that contribute to the increase of Human Papillomavirus (HPV)-related knowledge and cervical cancer screening behaviors. HPV is a group of related viruses, and high-risk forms of the virus are likely to progress to cervical cancer. 26 Moreover, as compared to traditional face-to-face patient-centered communication (PCC), email PCC also has been shown to increase the likelihood of American adults participating in cancer screening by allowing patients to raise questions, receive clear explanations, and participate in shared decision-making. 27 Hence, we proposed the following hypothesis:
ePHI technology use is positively associated with cancer screening behaviors.
S-O-R framework
Mehrabian and Russell 28 stated that individuals’ behavior depends on internal emotional states aroused by environmental or psychological factors. The relationship between environmental influences and their impact on the internal states and behavioral responses of humans was represented as a chain of events: S-O-R. In the S-O-R framework, stimulus (S) represents the psychological or environmental stimuli (e.g. the ePHI technology uses) that affect people. Individuals’ emotional states (e.g. fear, anxiety, and worry) are referred to as organisms (O). Responses (R) refer to individuals’ behavior in response to a certain stimulus, such as cancer screening behaviors.
The S-O-R framework has been widely applied in various fields, and it also provides an appropriate framework for public health research. For instance, based on the S-O-R framework, scholars 29 demonstrated that engagement and satisfaction with telemedicine services can directly impact continuance desires for telemedicine uses. Sitar-Taut and Mican 30 showed that fear and risk perception could mediate the relationship between social media exposure and attitudes toward generic vaccination. Thus, the S-O-R framework can be applied in the current study to explore the psychological mechanisms behind eHealth uses and cancer screening behaviors. Specifically, ePHI technology uses (S, stimulus) may affect how people feel about cancer (O, organism), which might influence if they go for cancer screening or not (R, responses). In other words, the link between stimuli (ePHI technology uses) and behavior (cancer screening behaviors) is mediated by cancer worry as a state of the organism.
The mediating role of cancer worry
Disease-related information via ePHI technologies, particularly about the risk and the uncertainty of cancer, may cause patients’ negative feelings about diseases. 31 Patients are concerned about the likelihood of a recurrence, the effectiveness of cancer treatment, and suspicious symptoms. 32 In this context, worry is an important decision factor in health behavior that receives increasing theoretical and practical attention. 33
Cancer worry is defined as the frequency and severity of worry, or repetitive negative emotional reactions of cancer-related uncertainty. 34 Since cancer is a significant threat to the lives of individuals that are frequently associated with mortality and inevitability, 35 ePHI technology use is likely to cause worry about getting cancer. This is because ePHI technologies allow patients to acquire health-related information, communicate with healthcare professionals, and check their health test results, all of which enable patients to better understand their health and equip them with the necessary knowledge about cancer. For example, the existing literature has generally proved that obtaining health information through electronic means can somehow increase one's health consciousness and health-related worry.36,37 Yang et al. 37 found that patients with electronic health experience were more concerned about their health and tend to motivate to maintain their ideal health status. By the same token, it is likely that ePHI use can elicit cancer worry, and to reduce cancer worry, a propensity to seek reassurances of good health such as cancer screening is expected. We, therefore, proposed the second hypothesis:
ePHI technology uses are positively associated with cancer worry.
Cancer worry may directly influence cancer screening behaviors. 38 Personal vulnerability or the probability of getting cancer may be directly related to perceived susceptibility, one of the key predictors of cancer screening intention, meaning that people do not act until they are aware that they are at real risk. 39 Specifically, people worry about their risks of developing cancer when they are exposed to knowledge on the danger of cancer or getting cancer, which motivates them to engage in preventive activities such as cancer screening. 40 For example, empirical evidence has been documented in Zhao and Nan's 41 study suggesting that cancer worry prompted women to evaluate their health risks and can motivate cervical cancer screening behaviors. Likewise, Li and Bautista 42 also found that cancer worry was positively associated with compliance with recommended health behaviors, such as getting vaccinated against HPV. As such, we formulated the third hypothesis:
Cancer worry is positively associated with cancer screening behaviors.
H2 predicts the first leg of the indirect effect, while H3 predicts the second leg. Together, they imply an indirect effect of cancer worry on the relationship between eHealth technology uses and cancer screening behaviors. However, very little is known about how cancer worry influences the relationship between ePHI technology uses and cancer screening over time. Thus, the fourth hypothesis is put forward:
ePHI technology use is positively and indirectly associated with cancer screening behaviors through cancer worry.
Methods
Data sources
A secondary analysis was conducted on nationally representative survey data obtained from two iterations of the Health Information National Trends Survey (HINTS) in 2017 (HINTS 5 Cycle 1), and 2020 (HINTS 5 Cycle 4). HINTS is a national cross-sectional survey using stratified sampling conducted by National Cancer Institute to document the American public's health information use and health behavior. HINTS 5 was a self-administered mailed questionnaire, using a sampling frame provided by the Marketing System Group of addresses in the US (see http://hints.cancer.gov/ for more details about sampling procedures). Cycle 1 was conducted between January and May 2017 (response rate: 32.4%), and Cycle 4 was conducted between February–June 2020 (response rate: 36.7%). Based on a dichotomized question about respondents’ gender, the current study only included female adults (18 years or older). The final sample size was 1914 in the HINTS 5 Cycle 1 and 2204 in the HINTS 5 Cycle 4. We conducted a power analysis by means of G*Power software 43 to estimate the minimum sample size required for the difference test and ordinary least squares regression. With an alpha level of 5% and a power of 80%, the minimum size estimated to identify a medium effect size is 128. The sample size in this study satisfied this requirement.
Variables and measurements
Cancer screening behaviors were measured using two items, adapted from national surveys using the same data source.44,45 Respondents were asked to report: (1) “How long ago did they have their most recent Pap test to check for cervical cancer?”; and (2) “When did they have their most recent mammogram to check for breast cancer, if ever?” (1 = never to 6 = a year ago or less). Each item was on a six-point scale and then linearly transformed to a 0–1 scale. The items were summed to form a 0–2 scale where 2 indicates the presence of both cancer screening, and 0 indicates zero possession of either behavior (M = 1.44/1.34, SD = 0.55/.057; samples 2017 to 2020).
ePHI technology use was measured with four items, drawn from previous research. 8 Respondents were asked whether in the past 12 months, they had used a computer, smartphone, or other electronic means to: (1) look for health or medical information; (2) communicate with a doctor or a doctor's office; (c) lookup medical test results; and (4) make appointments with a health care provider. The answers (0 = no, 1 = yes) of the items were summed to create the index of ePHI technology use. Larger numbers meant greater use of ePHI technology (Cronbach's alpha = 0.64/0.71, M = 1.41/1.67, SD = 1.08/1.15; samples 2017 to 2020).
Cancer worry was operationalized with one single item, similar to prior research. 46 Respondents were asked to rate their cancer worry with the question “how worried are you about getting cancer?” A five-point scale was used (1 = not at all to 5 = extremely), where higher scores represented higher cancer worry (M = 2.60/2.84, SD = 1.16/1.24; samples 2017 to 2020).
Sociodemographic variables were used to reduce the confounding effects, including age (2017: ranging from 18 to 95; 2020: ranging from 18 to 104), race (1 = white, 0 = others), marital status (1 = Married, 0 = Unmarried), household income (ranging from 1 = $0 to $9999 to 9 = $200,000 or more), and education level (1 = below high school to 7 = college or above). Family cancer history (0 = no, 1 = yes) was also included as a control variable because it may have confounding effects on cancer worry and cancer screening behaviors.47,48
Statistical methods
All analyses were conducted using SPSS 28. The two iterations of the dataset were separately analyzed. To begin, each variable was subjected to descriptive analysis. Second, since ePHI technology uses and cancer screening behaviors are ordinal variables, a Mann–Whitney U test was performed to examine the differences in these two variables. Two-sample t-test was used to explore whether there was a difference in cancer worry. Third, the SPSS PROCESS macro was used to investigate the proposed mediation relationships.
49
Moreover, to interpret the mediation effect, a min–max normalization
50
was conducted to rescale all variables to 0–1. As suggested by statisticians,
51
we referred to the regression coefficients of the variables calculated on the 0–1 scale as percentage coefficients (bp). That is, a larger bp meant greater efficiency. Percentizations were done using the following Equation (1), where sp is the percentage score after transformation, sos is the original score, scx is the conceptual maximum on the original scale, and scn is the conceptual minimum on the original scale. The legitimacy of this scale transformation has been supported by Cohen et al.
52
(i.e. percent of maximum possible score), and has been used in health studies.53,54

Results
Descriptive data
A total of 1914 and 2204 female respondents to the HINTS 5 Cycle 1 and HINTS 5 Cycle 4 were involved in this study. Table 1 presents the descriptive characteristics of the study variables of the two iterations (in both natural scales and the 0–1 scales). Throughout the two iterations, the mean age of the responders was around 56 years (55.82 years in 2017 and 56.53 years in 2020); the vast majority were White (74.2% in 2017 and 70.0% in 2020). The statistics also showed that 63.8% of respondents in 2017 and 2020 received college or above. Regarding marital status, 49.6% of participants in 2017 were married and 46.6% in 2020. The mean level of household income was between $35,000 and $74,999 in 2017 (M = 5.21) and 2020 (M = 5.39). Moreover, 22.3% of respondents in 2017 reported a family cancer history and 17.2% in 2020.
Descriptive statistics of the sociodemographic and health-related controls.

SD: standard deviation; M: mean; N/A: not applicable.
1 = US$0 to US$20,000.
Comparisons of cancer screening behaviors, ePHI technology use, and cancer worry
Mann–Whitney U test was conducted to compare the difference in ePHI technology use and cancer screening behaviors that occurred in the two iterations. Two-sample t-test was used to explore the difference in cancer worry. As seen in Table 2, the cancer screening rate in 2020 was slightly lower than that in 2017 (z = −5.12, p < 0.001). Table 2 also shows that the rate of ePHI technology uses slightly increased from 1.41 in 2017 to 2.19 in 2020 (z = −8.25, p < 0.001), in concordance with the statistically acknowledged increase in cancer worry from 2017 to 2020 (t = 6.34, p < 0.01).
Comparison of cancer screening, eHealth technology uses, and cancer worry between 2017 and 2020.
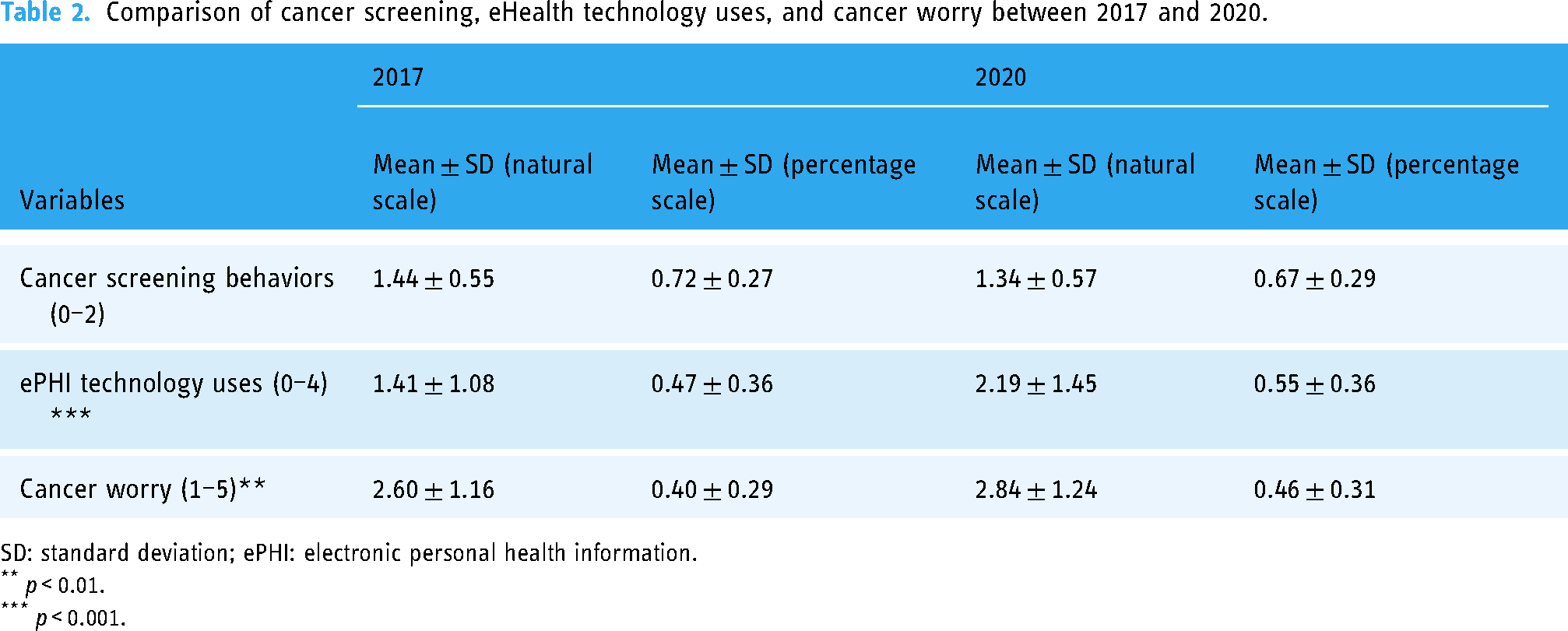
SD: standard deviation; ePHI: electronic personal health information.
p < 0.01.
p < 0.001.
Associations among cancer screening behaviors, eHealth technology use, and cancer worry
H1 predicted a positive effect of ePHI technology uses on cancer screening behaviors. In accordance with this, Table 3 shows that the effect was statistically acknowledged positive in 2017 and 2020 (b = 0.069/0.110; bp = 0.104/0.164; p < 0.001/<0.001; samples 2017 to 2020). bp indicates that a whole-scale increase in ePHI technology uses by 100 percentage points is associated with an increase in cancer screening behaviors by 16.4 percentage points in 2020.
The effect of ePHI technology uses on cancer screening behaviors via cancer worry.

Note. Unstandardized betas are shown in each cell, with percentage coefficients in parenthesis.
ePHI: electronic personal health information.
p < 0.05.
p < 0.01.
p < 0.001.
H2 predicted that ePHI technology uses will increase the level of cancer worry. As seen in Table 3, H2 was not statistically acknowledged in 2017. However, in 2020, eHealth technology use had a statistically acknowledged positive relationship with cancer worry (b = 0.096; bp = 0.072; p < 0.01). H2 was partially supported.
H3 proposed that cancer worry would associate with cancer screening behaviors. As depicted in Table 3, only the effect of cancer worry on cancer screening behaviors in 2020 passed the statistical threshold (b = 0.020/0.035; bp = 0.041/0.069; p > .05/<0.01; samples 2017 to 2020). Thus H3 was partially supported.
H4 predicted a positive indirect effect of ePHI technology uses on cancer screening behaviors via cancer worry. In 2020, the indirect effect was statistically acknowledged according to PROCESS-estimated bootstrap confidence intervals using 10,000 bootstrap samples (95%CI [0.001, 0.010]). However, following the same protocol, the indirect effect of cancer worry in 2017 was not statistically acknowledged, since its bootstrap 95%CI contained 0. Hence, H4 was partially supported.
In addition, according to Zhao et al.'s suggestions, 55 the mediation model in 2020 is identified as complementary since the indirect and direct-remainder paths are positive and statistically acknowledged. As illustrated in Figure 1, cp of the indirect effect of cancer worry is 2.96%, which means that 2.96% of the effect of ePHI technology use on cancer screening behaviors is mediated by cancer worry.

Effect of ePHI technology uses on cancer screening behaviors mediated by cancer worry (2017–2020).
Discussion
This trend analysis examined how the usage of ePHI technology influences American women's cancer screening behaviors, and whether the ePHI technology use increases the level of cancer worry with a subsequent increase in the rate of cancer screening, with two recent cycles (2017 and 2020) of a nationally representative survey of HINTS.
The findings herein indicated that there was a modest decline in cancer screening among American women, which was inconsistent with previous findings suggesting that the rates of breast and cervical cancer screening adoption have steadily increased in the US. 56 This decline could be due to the outbreak of COVID-19 in 2020 which may have resulted in a considerable reallocation of healthcare resources, causing difficulties in regular cancer screening practices. 57
The finding that supports the growing usage of ePHI technologies among American women is also consistent with previous research.58–60 In the past decades, electronic health infrastructure development has enabled patients to access a range of ePHI services. 61 Against this backdrop, the adoption of EHRs became widespread. 53 Online patient-center communication tools, including video conferencing, email, social media, and the Internet, have also been widely used. 62 Many national initiatives, such as the HITECH Act, have been implemented by government agencies to facilitate ePHI adoption. 63
Cancer worry increased across the 4 years from 2017 to 2020. One possible explanation could be that the death rates from breast cancer and cervical cancers remain high for American women in these years. In 2020, approximately 4% of American women were at risk of cervical HPV-16/18 infection which causes 71.2% of invasive cervical cancers. 64 While breast cancer is the second leading cause of cancer death in women. A woman's chance of dying from breast cancer is about 1 in 39. 65 In a study of cancer survivors, Hawranek et al. 66 found that women reported a significantly higher level of cancer worry than men.
As scholars 67 explained, women may feel worried when they believe that they are at higher risk of cervical cancer than their peers or friends, which in turn prompts them to follow cancer screening recommendations.
As predicted, this study identified the mediating role of cancer worry in the relationship between ePHI technology use and cancer screening behaviors. As suggested by the S-O-R framework, the individual's emotional responses could further induce them to engage in certain behaviors. More frequent use of ePHI tools can make it easier for patients to gain cancer-related knowledge, communicate with healthcare providers, participate in health decisions, and check their health test results, all of which can potentially increase users’ health awareness. It is thus understandable that ePHI technology users were more concerned about their cancer risk which has been conceptualized as cancer worry in our study. This result was accordant with the finding in Liu's study 36 suggesting that during the COVID-19 pandemic, the use of Internet-based ePHI technologies, such as social media, can elicit strong COVID-19-related worry and, in turn, increase people's preventive behaviors. Different from some negative emotions such as fear, anger, and anxiety, worry can motivate people to take action to prepare for prospective hazards and is favorably connected with a variety of problem-oriented coping mechanisms.33,68,69 Although the contribution of cancer worry is just 2.96%, we anticipate that the advancement of electronic technology and associated medical research will increase the contribution of cancer worry.
Theoretical implications and practical implications
Cancer worry mediating the relationship between stimulus information and behavioral response is a central theme of the S-O-R framework, which identified three relevant factors: stimulus (ePHI technology use), organism (cancer worry), and response (cancer screening behaviors). In other words, the present study extends the applicability of S-O-R to a new and important phenomenon—ePHI use and cancer screening behaviors—and explains the psychological mechanisms behind them. This study also has several practical implications. First, the positive effects of using ePHI technology on cancer screening behaviors should receive more attention. Physicians should incorporate ePHI technology to provide personalized medical advice or diagnosis to support patients in taking informed medical decisions that are consistent with their needs, values, and preferences. Also, based on the simultaneous growth of ePHI technology uses and cancer worry, we are concerned that the use of ePHI technologies may contribute to some degree to high levels of cancer risk perception or cancer worry, leading to unnecessary health information and behavioral avoidance. As such, as Braithwaite et al. 70 suggested, doctors and clinicians may have a greater need for personalized counseling to identify patients at high risk for cancer and to reduce the unrealistically high-risk perception and cancer worry. Patients should also use ePHI technology appropriately to provide their physicians with accurate and detailed information about their personal health status. In addition, we should note that as medical research advances and communication tools rapidly evolve, ePHI tools have to be designed to complement other health communication channels, be easy for health professionals to use, and communicate effectively with diverse consumers.
Second, emotional factors influencing cancer screening behaviors need to be viewed more positively. ePHI technology partially promotes the level of cancer screening adoption by evoking cancer worry. Therefore, health professionals may consider designing and delivering health messages that evoke cancer worry. Zhao and Nan 41 also pointed out that people may interpret complex health information via simple emotional judgments and reactions (e.g. cancer worry). For example, for a woman who rarely considers her cervical cancer risk, a health message stating that 10% of women develop cervical cancer in their lifetime may cause her to worry about the disease, even if she doesn’t fully comprehend the message's significance. Her concern may prompt her to get a Pap test.
Limitations
This study has some limitations. First, the use of cross-sectional data from HINTS inevitably hinders the possibility of observing causal relationships. Other research designs are needed in the future to investigate the causality of these key variables. Second, the reported cancer screening behaviors involved multiple types of cancer. American women may have different levels of worry about different types of cancer.25,71 In addition, it has been documented that significant media attention given to breast and cervical cancers may make people: (1) more familiar with certain types of cancer screening procedures and thus use of preventive services compared to other cancer types; and (2) more familiar with the objective risks of cancer, resulting in higher levels of cancer worry. Thus, the differences in cancer worry and cancer screening behaviors deserve more targeted and in-depth research. In addition, as only the general use of ePHI technology was considered in this study and the contribution percentage of cancer worry was relatively low (around 3%), we cannot generalize our results to other functions or technology uses and claimed that cancer worry is the only psychological mechanism within the relationships between ePHI technology use and other cancer preventative behaviors. More in-depth and detailed measurements of ePHI technology may be needed in the future to compare the effects of ePHI technology between different techniques or between different subgroups. Future studies could focus on defining health behavior more precisely, rather than emphasizing the channel through which these activities are conducted. Future research should also seek to find more dominant mediating factors, such as health self-efficacy, fear, and other psychological factors. In addition, since most of the variables we tested are ordinal variables, the current data methods may have some statistical bias, future research should also adopt some valid and effective approach to replicate the results.
Conclusion
ePHI technology offers significant opportunities to access, seek, and comprehend health information that essentially contributes to health promotion and disease prevention. The research findings suggest that the adoption of ePHI technology continues to grow. Besides, the usage of ePHI technology was positively associated with American women's cancer screening behaviors either directly or indirectly via cancer worry. Understanding these relationships can help increase the use of ePHI technology, raise awareness of cancer, and eventually engage people in cancer preventive care practices.
Footnotes
Contributorship
PLL, XZ, and JFY developed the concept of this study. Material preparation, data collection, and analysis were performed by PLL, JFY, and HSA. The first draft of the manuscript was written by SS and JFY. YZ, QL, GCF, and HW contributed to the methodology and the interpretation and made critical revisions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study used secondary data. The HINTS data meet established ethical standards and have obtained ethics approval.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported in part by grants of University of Macau, including CRG2021-00002-ICI, ICI-RTO-0010-2021, CPG2022-00004-FSS and MYRG2020-00233-FSS..
Guarantor
Xinshu Zhao
Informed Consent
This study used secondary data. The HINTS data make sure that participants provided informed consent for participation in the study.