
Abstract
Objective
This study investigates how fitness technology (FT) influences cancer screening behaviors among American women, focusing on the role of social media communication and cancer worry as mediators.
Methods
We used data from 9245 women across four cycles (2017–2020) of the Health Information National Trends Survey. Descriptive analyses, one-way ANOVA, and sequential mediation analysis were conducted to assess the relationship between FT use and cancer screening behaviors.
Results
The results indicate that between 2018 and 2020, social media communication and cancer worry sequentially mediated the relationship between FT use and cancer screening behaviors (b = 0.001/0.001/0.001, 95% confidence interval (CI) [0.0002, 0.002]/[0.0002, 0.002]/[0.0001, 0.001]). Additionally, there was an upward trend in FT use (from 0.74 in 2017 to 0.93 in 2020), social media communication (from 1.17 in 2017 to 1.39 in 2020), and cancer worry (from 2.60 in 2017 to 2.84 in 2020). However, cancer screening behaviors declined over the same period (from 4.59 in 2017 to 4.35 in 2020).
Conclusion
The study highlights the role of FT in influencing cancer screening behaviors through its impact on social media communication and cancer worry. Despite an increase in FT use, cancer screening behaviors showed a decline, suggesting the need for targeted interventions to bridge this gap and enhance screening behaviors.
Introduction
Cancer remains one of the leading causes of death in the United States, 1 with women particularly at risk for breast and cervical cancers. Breast cancer is the most prevalent type of cancer among women, accounting for approximately 30% of all new female cancer cases annually. 2 Similarly, cervical cancer contributes significantly to cancer-related mortality in women. 1 Given the high mortality risk associated with these cancers, it is essential to promote preventive measures such as regular cancer screenings.
In recent years, fitness technology (FT) has emerged as a tool for promoting health behavior change, especially smartphone applications and wearable devices have demonstrated potential in facilitating various health behaviors,3–6 with a primary focus on fitness and self-monitoring. 7 These technologies also offer opportunities for healthcare providers to monitor health metrics, set goals for patients, and support their efforts in achieving behavior change. 8 Data from the United States show that nearly half of smartphone and tablet users have at least one fitness or health-related app installed. 9 Despite the widespread adoption and known benefits of FT,10–13 existing studies have largely concentrated on its influence on diet and physical activity.5,14–16 Given that women are significant users of fitness technologies compared to men,17–20 there remains a gap in understanding how FT affects cancer screening behaviors among women. Understanding this relationship is crucial for enhancing cancer prevention efforts.
Another key factor in influencing health behaviors is social media
Given this background, the present study posits that communication behaviors on social media and cancer worry act as sequential mediators between FT use and cancer screening behaviors. To explore this relationship, the study draws on Social Cognitive Theory 25 and the Communication Mediation Model.26,27 This study aims to: (1) Examine the relationship between FT use and cancer screening behaviors among women; (2) Investigate the sequential mediating roles of social media communication and cancer worry in the link between FT use and cancer screening behaviors and (3) Analyze trends in the relationship between these variables across four years of data from the Health Information National Trends Survey (HINTS) collected in 2017, 2018, 2019, and 2020.
Literature review
FT and cancer screening behaviors
FT, including smartphone applications and wearable devices. 14 Users have the option to select standalone wearable devices, wearable trackers paired with a companion fitness app, or solely use a fitness app on their smartphone or tablet without any additional tracking devices. 28 FT allows to track a range of health-related behaviors, such as weight management, diet monitoring, and sleep tracking.8,29 These technologies are becoming increasingly popular among women. 18 A Pew Research study revealed that around 25% of women in the United States use a smartwatch or fitness tracker, compared to 18% of men. 18 FT not only enhances their’ health knowledge, 30 but has the potential to empower women to take preventive actions, such as undergoing cancer screening, when they perceive themselves at risk.31,32
Early detection through cancer screening plays a critical role in reducing cancer mortality.2,33 Numerous studies emphasize that early detection of breast and cervical cancers significantly increases survival rates,34–36 and highlight the need to promote screening behaviors among women.37–40 FT, with features like goal setting, feedback, and tracking, has the potential to motivate users to engage in preventive health behaviors, including cancer screening.8,28 In fact, 47% of health-related apps focus on managing specific conditions or promoting disease prevention. 41 Research also supports the role of fitness technologies in increasing intentions and actions related to health behaviors,7,14,42–45 suggesting that FT has the potential to enhance cancer screening behaviors.
The role of social media communication and cancer worry
Social media platforms, such as Facebook, LinkedIn, and YouTube, have become significant venues for health communication. 46 These platforms allow users to share and discuss health information, and women who share health-related information on social media may be influenced by FT use, as the provision of personalized data and social network connectivity are key features of FT.8,47–51
Research indicates that FT is positively associated with communication behaviors on social media. 14 Many FTs offer features that allow users to share personal health data, such as weight or dietary habits, fostering communication and motivation among social media users. 49 Users frequently share personal health information to strengthen social connections and reinforce their motivation for healthy behaviors.49,52,53 Additionally, FT, as a communication facilitator, may indirectly influence personal responses by prompting further communication. According to the Communication Mediation Model, communication shapes thoughts, emotions, and behaviors, 27 Shah, McLeod 26 revise this model by highlighting that communication fosters ongoing dialogue, leading to additional interactions. Building on this framework, FT users are likely to engage in more health-related discussions and seek complementary information across social platforms,26,54,55 which may have both motivational and psychological effects.
While these interactions often reinforce positive health behaviors,14,56,57 they can also contribute to anxiety and concern, particularly related to cancer.23,24,58 Specifically, FT may heighten cancer worry indirectly through social media communication, such as sharing personal health data or seeking health information. For example, when users post early warning signs detected by FT, like unexplained weight loss, changes in menstrual cycles, or breast lumps,59–62 their social media friends can comment, react, and engage. These interactions not only foster discussion but also expose users to potentially alarming content related to cancer risks, prompting them to seek further health information. 27 Increased exposure to risk information has been linked to higher levels of cancer worry.23,24,58 Given that women are generally more active on social media11,21,63 and frequently seek cancer information,64,65 thus, it is plausible that FT, by encouraging greater social media use, may contribute to higher levels of cancer worry among women.
Cancer worry, defined as persistent negative emotions related to cancer risk, 66 can drive preventive behaviors like cancer screening,23,24,67 as when individuals aware of the dangers posed by cancer, people become increasingly concerned about their likelihood of developing it, which may motivate them to engage in preventive measures such as screening. Research consistently shows a positive correlation between communication factors and cancer screening behaviors via cancer worry among women.23,24,68 For example, eHealth technologies that induce cancer worry have been shown to encourage women to undergo cervical cancer screenings. 24 Furthermore, studies by Jizhou Francis and Shenting Zheng suggest that patient-centered communication increases cancer worry, which in turn drives women to pursue breast and cervical cancer screenings. 68 Besides, drawing on social cognitive theory (SCT), which posits that behavior is influenced by reciprocal interactions between personal, environmental, and behavioral factors, 25 social media serves as a critical environmental factor that may shape perceptions of cancer risk and, consequently, motivate screening behaviors.
In summary, this study, grounded in the Communication Mediation Model and SCT, examines the potential for serial mediation between FT use, social media communication, and cancer worry in influencing cancer screening behaviors (see Figure 1). The Communication Mediation Model suggests that FT, as a digital tool, can facilitate increased communication on social media, which may in turn heighten cancer worry. SCT posits that social media, as an environmental factor, shapes perceptions of cancer risk, motivating preventive behaviors like cancer screening. Although numerous studies have independently explored the mediating roles of social media communication and cancer worry,23,24 little is known about their role in the relationship between FT use and cancer screening behaviors, or how these factors interact over time. Thus, this study proposes five hypotheses:
H1: FT use will increase cancer screening behaviors. H2: FT use will increase communication behaviors on social media. H3: Communication behaviors on social media will increase cancer worry. H4: Cancer worry will increase cancer screening behaviors. H5: FT will impact cancer screening behaviors through the sequential mediation of increased social media communication and heightened cancer worry.

Conceptual framework of the sequential mediation model (consistent direction across 2017–2020).
Method
Sampling
This study uses a quantitative research method based on HINTS data collected in the United States from 2017 to 2020. The data from these years were selected because the core variables were consistently measured during this period. Additionally, previous research on cancer screening among women has used this period as a reference. 24 HINTS is a nationally representative survey administered by the National Cancer Institute to assess American adults’ access to health information, as well as their health-related knowledge, attitudes, and behaviors. More details about HINTS are available at https://hints.cancer.gov/. The total sample size across the four cycles was 15,408. After applying the final survey weights provided by HINTS, the weighted sample represented a total of 331,449,281 individuals. These final survey weights were used to ensure nationally representative estimates and were normalized across cycles to account for differences in sample sizes. Based on a dichotomous question about respondents’ gender, this study included only individuals designated as female on their original birth certificates. To compare the overall changes in cancer screening behaviors over four years, we selecting women aged 18 and above, the final analytic sample consisted of 9245 women, representing 166,663,517 women in the U.S. population. In the pooled sample, these normalized weights were applied in all analyses to maintain proportional representation of the U.S. population. The final pooled sample size includes 1914 participants from HINTS 5 Cycle 1 (2017), 2054 from HINTS 5 Cycle 2 (2018), 3073 from HINTS 5 Cycle 3 (2019), and 2204 from HINTS 5 Cycle 4 (2020). To ensure the robustness of the findings, participants were divided into two groups based on USPSTF and ACOG screening guidelines to compare different types of cancer screening behaviors: the breast cancer screening group (women aged 40 and above) and the cervical cancer screening group (women aged 21 to 65).69,70 The breast cancer screening group included 7249 participants, while the cervical cancer screening group included 6048 participants.
Measures
FT use was measured with two items, similar to prior research using the same data source. 14 Participants were asked if, in the past 12 months, they had (1) used a health or wellness app on a tablet or smartphone and (2) used an electronic wearable device (e.g., Fitbit, Apple Watch, or Garmin Vivofit) to monitor health or activity. Responses were coded as “yes” (1) or “no” (0), and the two items were summed to create an additive measure of FT use, with higher scores indicating greater use. M = 0.74/0.929/0.86/0.932, SD = 0.76/0.81/0.785/0.793, corresponding to 2017, 2018, 2019, and 2020, respectively.
Communication behaviors on social media were measured using four items, adapted from national surveys using the same data source.14,71 The question began with the statement: “Sometimes people use the Internet to connect with other people online through social networks like Facebook or Twitter; this is often called social media.” Participants were then asked if, in the past 12 months, they had used the Internet for any of the following: (1) to visit a social networking site, such as Facebook or LinkedIn, (2) to share health information on social networking sites, such as Facebook or Twitter, (3) to participate in an online forum or support group for people with a similar health or medical issue, and (4) to watch a health-related video on YouTube. Respondents who answered “yes” to any of these categories were classified as using social media and defined as social media users. M = 1.17/1.272/1.273/1.39, SD = 1.04/1.080/1.069/1.09, corresponding to the years 2017, 2018, 2019, and 2020, respectively.
Cancer worry was operationalized with one single item, similar to previous research. 44 Respondents were asked to rate their cancer worry with the question “How worried are you about getting cancer?” A five-point scale was used (1 = not at all to 5 = extremely), where higher scores represented higher cancer worry. M = 2.603/2.599/2.50/2.84, SD = 1.158/1.17/1.157/1.19, corresponding to the years 2017, 2018, 2019, and 2020, respectively.
Cancer screening behaviors were measured using two items, similar to prior research. 24 Respondents were asked to report: (1) “How long ago did they have their most recent Pap test to check for cervical cancer?” (cervical cancer screening); and (2) “When did they have their most recent mammogram to check for breast cancer, if ever?” (breast cancer screening) (1 = never to 6 = a year ago or less). The six-point scale was chosen to balance simplicity and granularity. The choice of cutoff points “never” as “1” and “within the past year” as “6” was designed to capture the most recent screening behavior, which is highly relevant for understanding the timeliness of cancer screening. The two items were averaged to form a composite measure afterward, where higher scores indicate more timely and recent screening behaviors, reflecting a higher frequency of adherence to recommended screening schedules. We chose cervical/breast cancer screening as the focus of our study variable because these screening frequencies were consistently recorded across all waves of the HINTS data we analyzed. Given that both screening behaviors were measured using the same six-point scale and that previous studies,23,24 using HINTS data have used the same composite score for these two screening behaviors, we selected the composite score for our analysis. The two screening behaviors are significantly correlated across years, r = 0.197/0.220/0.213/0.157, p < .001/<.001/<.001/<.001, M = 4.59/4.39/4.43/4.35, SD = 1.37/1.44/1.43/1.42, corresponding to the years 2017, 2018, 2019, and 2020, respectively.
Data analysis
SPSS version 25 was used for data analysis. Four types of analyses were conducted: (1) SPSS PROCESS (Model 6) 72 was used to examine the sequential mediating effects of communication behavior and cancer worry between FT use and general cancer screening behaviors. This model was chosen because it is well-suited for analyzing sequential mediation effects, where multiple mediators are tested in a specific order. Path coefficients were assessed using 10,000 bootstrap samples to obtain 95% bias-corrected CIs; (2) To ensure the robustness of the findings, Model 6 was then used separately to examine the sequential mediating effects of communication behavior and cancer worry between FT use and breast cancer screening behaviors, as well as cervical cancer screening behaviors. (3) one-way ANOVA with post hoc Games-Howell analysis to compare focal variables; and (4) year, treated as a continuous moderator, to examine changes over the years. Missing data were handled using listwise deletion.
Results
Descriptive statistics
Descriptive statistics for the independent, dependent, and control variables are presented in Table 1. In the weighted pooled sample, the average age was 50 years (SD = 17.90), and the mean household income was between $35,000 and $74,999 (M = 5.50). Most participants had a college education or higher (62.2%), and nearly half (49.2%) were married or living as married. Additionally, nearly 30% of participants were single and had never been married (see Table 1 for more details). More information about the breast cancer screening group and the cervical cancer screening group is provided in Supplemental Table S1.
Descriptive statistics of the independent, dependent, and controlled variables (2017–2020) (unweighted N = 9245; weighted N = 166,663,517).

Note. SD stands for standard deviation.
Mediation results
H1 predicted the positive relation between FT and cancer screening behaviors. As shown in Table 2, FT had a statistically significant relationship with cancer screening behaviors in 2018, 2019, and 2020 (b = 0.062/0.052/0.046, p < .01/<.01/<.05; respectively), providing partial support for H1.
The effects of fitness technology use on cancer screening behaviors through social media communication and cancer worry each year.

Note. Unstandardized betas are shown in each cell; * p < .05. ** p < .01. *** p < .001.
H2 predicted that FT use would be positively associated with communication behaviors on social media, and this was supported by the results (b = 0.293/0.266/0.279/0.322, p < .001/.001/.001/.001; samples from 2017 to 2020, respectively).
H3 predicted the positive relation between communication behaviors on social media and cancer worry. Results partial support for H3 (b = 0.110/0.091/0.061, p < .001/<.001/<.05; samples from 2018, 2019, and 2020, respectively).
H4 predicted that cancer worry would be positively associated with cancer screening behaviors, and this was supported (b = 0.027/0.036/0.034/0.027, p < .05/<.01/<.01/<.01; samples from 2017 to 2020, respectively).
H5 posited that FT use would be positively associated with cancer screening behaviors through the sequential mediation of communication behaviors on social media and cancer worry. Results partially supported H5 (b = 0.001/0.001/0.001, 95% CI [0.0002, 0.002]/[0.0002, 0.002]/[0.0001, 0.001]; samples from 2018, 2019, and 2020, respectively). To ensure the robustness of the findings, two parallel analyses were conducted within the breast cancer screening group (women aged 40 and above) and the cervical cancer screening group (women aged 21 to 65), utilizing both four years of data and the total data over the four years. The results remained consistent in terms of the direction of coefficients and the statistical significance of the impact of FT on screening behaviors, as shown in Table 3 and Supplemental Table S2. To evaluate the influence of the year, we adhered to established textbook guidelines 73 and prior methodologies by aggregating data over four years and treating the year as a moderating variable.74,75 The interaction term (year × FT) did not yield statistically significant results in predicting cervical cancer screening behavior (b = 0.009, p > .05), breast cancer screening behavior (b = 0.021, p > .05), and combined cancer screening behaviors (b = 0.006, p > .05) in the analysis using combined data from 2017 to 2020. This indicates that the relationship between FT use and cancer screening behaviors did not significantly change over time during the study period.
Summary of different path effects in two types of cancer screening behaviors each year.

Note. DV: dependent variable; CI: confidence interval.
All models control for age, household income, education, and marital status.
*p < .05; **p < .01; ***p < .001.
The trends of core variables
As shown in Figure 2 and Table 4, the results based on the weighted sample (ANOVA) showed a significant decrease in cancer screening behaviors from 2017 to 2020, with a mean difference of −0.26 (p < .001). In contrast, the unweighted annual mean values revealed a decrease from 4.59 in 2017 to 4.35 in 2020, indicating that, without weight adjustment, the results were consistent in direction. The level of FT use increased from 0.74 in 2017 to 0.93 in 2020, indicating a statistically significant increase (Mdiff = 0.22, p < .001). The level of cancer worry increased from 2.60 in 2017 to 2.84 in 2020 (Mdiff = 0.26, p < .001), with statistically significant differences observed every two years. Communication behaviors on social media increased from 1.17 in 2017 to 1.39 in 2020 (Mdiff = 0.20, p < .001) with statistically significant differences observed every two years.
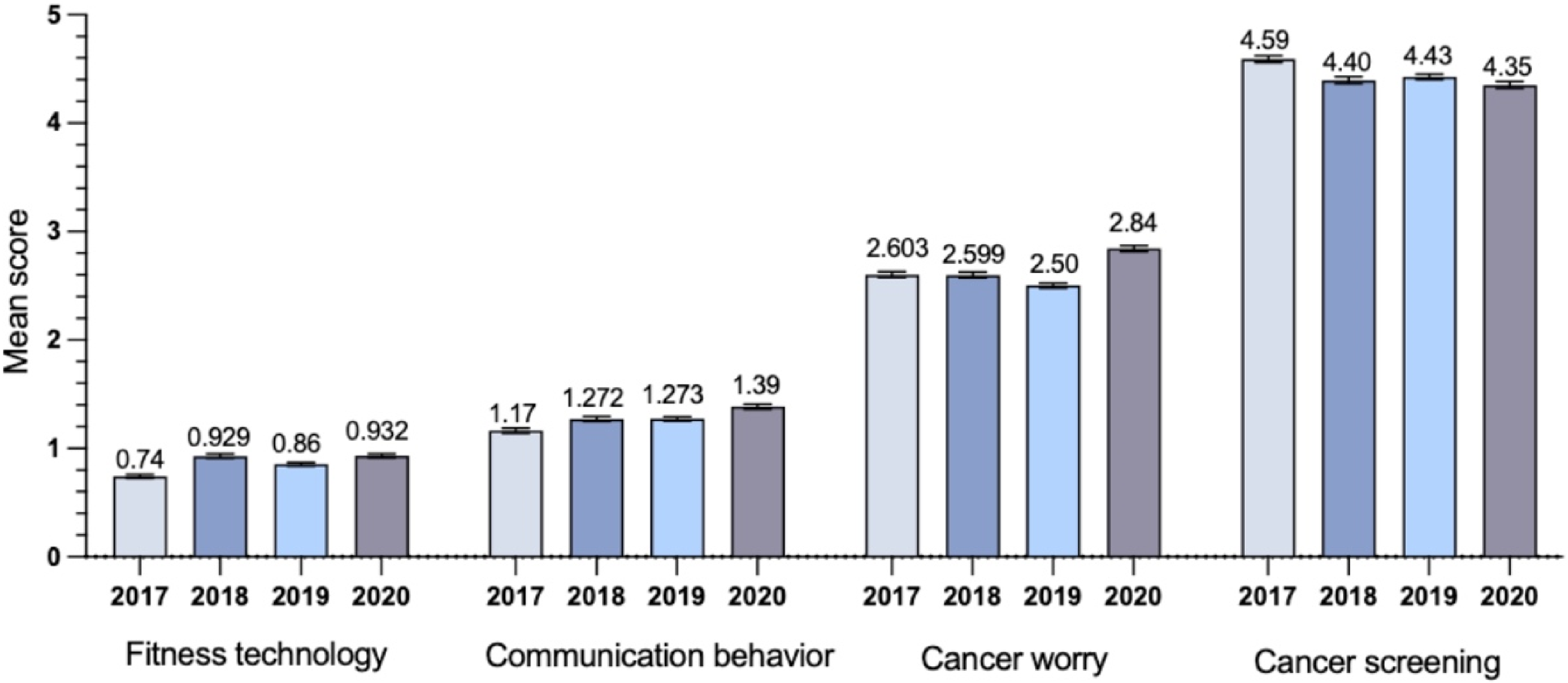
The comparison of combined cancer screening behaviors, fitness technology, communication behavior and cancer worry.
Multiple comparisons of the cancer screening, fitness technology, communication behavior, and cancer worry (weighted).

Notes. The main cell is the difference in mean; one-way ANOVA analysis with post hoc analysis (Games-Howell method) was used.
***p < .001.
Discussion
This trend analysis study explored the influence of FT use on cancer screening behaviors among American women, investigating whether increased use of such technology promotes greater engagement in social media communication and heightens cancer worry, ultimately leading to higher rates of cancer screenings. The study drew on four recent cycles (2017–2020) of nationally representative data from the HINTS survey.
Analysis of the trends of core variables
First, our findings reveal an upward trend in cancer screening behaviors from 2018 to 2019, following declines from 2017 to 2018 and from 2019 to 2020. The increase during this period could potentially be related to social media platforms spreading health information and promoting public health campaigns.47,76 Additionally, the growing adoption of smartphones and the increasing accessibility of more user-friendly wearable devices became particularly influential from 2018 onward.77,78 By this time, wearable devices were more advanced, offering features such as heart rate monitoring, sleep tracking, and personalized health insights, which likely made them more useful and appealing for individuals focused on health management. 79 These technological shifts might have contributed to making fitness tracking and health-related information more accessible and appealing, 79 possibly influencing interest in preventive health behaviors, such as cancer screening. Health literacy may also be important in this context, as individuals with higher health literacy are more likely to engage with these technologies and health information effectively, 80 which potentially leads to increased cancer screening behaviors. Moreover, access to healthcare may play a significant role in enabling individuals to act on health information. Those with better access to healthcare services may be more likely to participate in screening programs, while those with limited access may face barriers despite the technological advancement. 81
The decline from 2017 to 2018 could be attributed to changes in healthcare policies and economic factors, as individuals facing reduced financial security may be less likely to prioritize preventive health measures.82,83 Additionally, regional differences in healthcare access and infrastructure might have contributed to varying levels of cancer screening participation. For instance, individuals in rural areas or regions with fewer healthcare resources may have experienced greater challenges in accessing screening services. 84 The drop in screening behaviors from 2019 to 2020 could potentially be influenced by the COVID-19 pandemic, which disrupted healthcare services and led to the postponement or cancelation of many screening programs. 85 Specifically, during the COVID-19 pandemic, healthcare resource strain and restrictions on nonessential procedures likely caused delays in cancer screenings for some individuals. 86 This impact may have been felt more by those using health monitoring technologies, like wearable devices, which, while helpful, cannot replace medical screenings. Although these technologies may have increased health awareness, actual screening behaviors were still influenced by healthcare access and policy restrictions. A study found that, compared to previous years, breast screenings in the United States. decreased by 87% and cervical screenings by 84% in April 2020. 87 This underscores the potential effect of healthcare disruptions on essential services, including cancer screenings. Second, the increased use of FT may be attributed to the advancements in its design and functionality, 88 making it more appealing and accessible to a broader audience. Third, communication behaviors on social media exhibited a steady year-over-year increase from 2017 to 2020. The potential reason could be the widespread adoption of smartphones and internet access, 21 which made social media more accessible, while the rise of visual and interactive content, such as videos and live streaming, enhanced user engagement. Finally, there was an overall increase in cancer worry from 2017 to 2020. possibly due to persistently high mortality rates associated with breast and cervical cancer in the United States.89–91
Mediation analysis
As anticipated, this study identified the sequential mediating role of communication behaviors on social media and cancer worry in the relationship between FT use and cancer screening behaviors. FT use was positively associated with communication behaviors on social media, which, in turn, positively linked to cancer worry and subsequently to cancer screening behaviors.
H1 predicted a positive relationship between FT and cancer screening behaviors in 2018, 2019, and 2020. The p-values indicate that these relationships are statistically significant, suggesting that the use of FT is potentially reliably associated with increased cancer screening behaviors among women during these years. The association between FT use and cancer screening behaviors in 2017 was nonsignificant, which may reflect the early stage of adoption of FT at that time, 92 and users have limited ability to operate FT during that period. 93 While fitness apps and wearable devices were gaining popularity, their usage was not yet widespread or consistent. 92 Many individuals were hesitant to adopt these technologies due to concerns over their usability, accuracy, and effectiveness,42,94 which could have limited their integration into daily health behaviors like cancer screening. Additionally, early-stage fitness technologies primarily focused on tracking physical activity rather than comprehensive health-related behaviors, such as cancer prevention and screening. 42 This limited functionality may have hindered users from perceiving FT as a tool for promoting cancer screening. The relatively low adoption rate, combined with the early-stage nature of the technologies, likely explains why a significant relationship between FT and cancer screening behaviors was not observed in 2017. Furthermore, the findings revealed a diminishing trend in the direct effect of FT on both cervical and breast cancer screening. This may be due to the advancements in cancer screening options. For instance, cervical cancer screening has transitioned from the traditional Pap test to more sensitive methods like HPV testing and co-testing.95,96 These newer options provide more accurate results and longer intervals between screenings, 97 reducing the necessity for regular reminders delivered through fitness technologies. Similarly, Improved breast cancer screening methods, such as digital mammography, have contributed to more accurate and efficient detection of early-stage cancers, reducing false positives and unnecessary follow-up tests, 98 this may increase patient confidence in screening results, lessening the perceived need for additional reminders or health monitoring.
As predicted by hypotheses H2, H3, and H4, this study identified a significant sequential mediation model. The use of FT positively influences cancer screening behaviors through its impact on communication behaviors via social media and cancer worry. The findings are consistent with existing research that suggests technological affordances may play a role in influencing behavioral changes.48,50,88 For example, Zheng and Li 14 demonstrate that applications and trackers equipped with features that promote sharing personal health information and viewing supplementary health-related videos facilitate behavioral changes. Moreover, the cost-effectiveness and ease of integrating FT with social media platforms may enhance user engagement.99,100 Specifically, the p-values for each year (all < .001) suggest that the relationship between FT use and communication behaviors on social media is statistically significant across all four years, indicating that this effect is unlikely to be random. Additionally, the CIs for each year, ranging from [0.230, 0.356] in 2017 to [0.260, 0.385] in 2020, show that the impact of FT remained positive. The growing effect size over time may reflect the increasing integration of FT into daily life, which could have encouraged more frequent health-related discussions online. The widening CIs also suggest a potential strengthening of this relationship over time, possibly due to greater user engagement and a growing focus on health-related content. 26
The findings align with the Communication Mediation Model, 26 indicating that FT, as a digital tool directly may enhance communication behavior on social media. As users engage with FT, they are more likely to share and seek health experiences and information, 24 which may foster discussions about health topics such as cancer and connecting with communities facing similar health challenges. While these interactions can promote awareness and knowledge, 101 they also expose users to health information and risk-related content, heightening their awareness of potential health threats 102 and intensifying anxiety about health risks. 103 Consequently, it is plausible that this exposure to social media increases cancer worry. Furthermore, the p-values for 2018–2010 (all <.05) suggest that the relationship between communication behaviors on social media and cancer worry was statistically significant and unlikely to be due to random chance. However, it is noteworthy that the positive influence of communication behaviors on social media on cancer worry has decreased over the years, particularly by 2020. The CIs for 2018 ([0.047, 0.173]) show a relatively strong effect, with the lower bound still indicating a meaningful relationship. However, in 2020, the interval ([0.003, 0.119]) narrowed and moved closer to zero, suggesting a weaker effect and potentially indicating a shift in how individuals engage with cancer-related content on social media. This decreasing trend may be attributed to the increasing volume of health-related content on social media, which, over time, may overwhelm users. 104 The proliferation of both credible and misleading information could lead to “information fatigue,” making it increasingly difficult for users to distinguish reliable sources from misinformation. 105 Over time, individuals may have become desensitized to the constant flow of health-related information,106,107 further weakening its impact on cancer-related concern.108,109 As a result, the effectiveness of social media as a health communication tool diminishes, thereby reducing its impact on cancer worry and potentially lessening its influence on cancer screening behaviors.
As suggested by SCT, social environmental factors can influence personal factors, thereby shaping behavior. 25 Social media platforms serve as an external factor for users to share and seek health information, exposing them to risk-related content that increases awareness of health threats like cancer. 102 This heightened awareness can lead to increased worry about cancer risk, motivating individuals to engage in preventive behaviors such as screening.23,24,67 Cancer worry, often prompted by communication factors, can directly enhance cancer screening behaviors among women, consistent with previous research findings.23,24 For instance, studies show that anxiety related to cancer, spurred by eHealth technologies, can encourage women to participate in cervical cancer screening. 24 Similarly, research by Jizhou Francis and Shenting Zheng demonstrates that patient-centered communication can elevate cancer worry among women, prompting them to undergo screenings for both breast and cervical cancer. 23 Moreover, our findings reveal that the direct positive effect of cancer worry on cancer screening behavior diminished each year from 2018 to 2020. This trend may be attributed to the advancements in screening technologies in recent years, such as the introduction of HPV testing, which allowed for longer screening intervals,95–98 reducing immediate concerns.
In conclusion, this study demonstrates that FT is positively correlated with cancer screening behavior through the sequential mediation of communication behaviors on social media and cancer worry. While the magnitude of the pathway effects fluctuated over time, the overall sequential mediation effect remained relatively stable. The directional relationships between variables in the model were consistent and not significantly impacted by temporal changes. However, it is important to note that, given the repeated cross-sectional design of this study, the findings indicate correlations rather than causal relationships. The observed trends may be influenced by multiple factors, and future longitudinal or panel studies would help confirm the directionality of these effects.
Supplementary analysis
As indicated in Supplemental Table S1, the mean score of FT use is lower in the breast cancer screening group (M = 0.800) compared to the cervical cancer screening group (M = 0.955). However, as shown in Supplemental Table S2, both the direct and sequential indirect effects of FT on cancer screening over the four years appear to be stronger in the breast cancer screening group than in the cervical cancer screening group. Additionally, as shown in Table 3, the mediating effect of FT on breast cancer screening became significant in 2018, while its effect on cervical cancer screening seemed to emerge a year later. This disparity could potentially be influenced by the earlier promotion and public awareness of breast cancer in the United States compared to cervical cancer. For instance, the American Cancer Society advocated for breast self-examinations 110 earlier than for routine cervical cytology screening. 111 Thus, the public might have more health knowledge and health literacy related to breast cancer than cervical cancer. One study suggests that public knowledge about breast cancer tends to surpass that of cervical cancer. 112 Based on the reasoning from the “mediation analysis,” this difference in awareness may have contributed to a greater focus on breast cancer screening as FT gained popularity, which could have led to more communication on this topic through social media and potentially heightened cancer worry, thereby possibly influencing screening behaviors for breast cancer more than for cervical cancer. Public health departments could consider leveraging fitness technologies, such as health apps and wearable devices, to enhance breast cancer screening participation. They may incorporate personalized health reminders and data monitoring to optimize outreach strategies.
For cervical cancer screening, however, the relatively weaker impact of FT may suggest a need for further alignment between the technology design and the specific data monitoring needs of cervical cancer prevention. Policymakers may need to explore additional strategies, such as strengthening educational campaigns to improve health literacy around cervical cancer and enhancing the accessibility of screenings, to address the relatively limited influence of technology and increase engagement in preventive behaviors. However, it is important to note that these findings suggest correlations rather than causal relationships. The observed trends could be influenced by multiple factors, and further longitudinal or panel studies are needed to confirm the directionality of these effects. These findings highlight the potential of FT as a tool for promoting both breast and cervical cancer screening, but further research is required to explore its role in health interventions.
Theoretical and practical implications
This study contributes to the growing body of research linking FT use with health behavior change by integrating the Communication Mediation Model and SCT into a sequential mediating model. Through the lens of CMM, the findings demonstrate how FT use drives communication behaviors on social media, illustrating how external digital tools influence the sharing of health-related information. This establishes the first step in the sequential mediation, where FT use indirectly affects health behavior through its influence on communication. Building on this, SCT explains the subsequent steps in the mediation, where social media communication enhances cancer worry, and cancer worry then motivates women to engage in cancer screening behaviors. This aligns with SCT's focus on how personal perceptions, shaped by external communication, lead to behavior change. This dual-theoretical framework contributes significantly to the theoretical understanding of how digital health interventions can influence preventive health behaviors among woman. Future digital health interventions targeting women's health can utilize this dual-theoretical framework to design strategies. For example, CMM can be used to create and strengthen online communities where women share experiences and health information. Meanwhile, SCT can be integrated to promote social learning and peer influence, enhancing women's cancer worry and transforming it into a constructive force that motivates cancer screening behaviors. By combining these theoretical insights, interventions can not only effectively communicate health information but also better engage and motivate women, ultimately improving the overall effectiveness of preventive health programs. Overall, the sequential mediation model highlights how FT shapes cancer screening behaviors by first fostering online health communication and then influencing personal psychological factors such as cancer worry, particularly in the context of cancer prevention among women. By integrating these two theoretical perspectives, this study provides a comprehensive framework for understanding how digital health tools influence preventive health behaviors through a layered process.
Practically, the results highlight the potential for integrating fitness technologies with social media platforms to enhance public health interventions, especially for women. Healthcare providers and policymakers can incorporate tools like health-tracking apps, personalized notifications, and online peer support groups within fitness technologies to drive cancer prevention behaviors. For example, mobile fitness apps could be used to send personalized cancer screening reminders or host virtual support groups where women can share their experiences and health concerns. These activities may help appropriately increase cancer-related worry, thereby further motivating women to engage in cancer screening. Given the consistent impact of communication behaviors and cancer worry on screening, tailored interventions that combine FT with educational content on social media can further motivate women to participate in regular cancer screenings. Moreover, as digital health tools and platforms continue to evolve, interventions must remain adaptive, incorporating emerging technologies. For example, new features such as AI-driven chatbots could be integrated into fitness apps to offer personalized, real-time health advice and reminders, helping to keep users engaged and informed. Expanding telehealth capabilities within fitness technologies could also provide women with access to remote consultations, further offering psychological incentives for cancer screening behaviors. This adaptability ensures that public health initiatives stay relevant and effective in promoting proactive health management and cancer prevention. Additionally, given the waning effect of social media communication on cancer worry over time, it is crucial that future interventions move beyond simply increasing content volume. Instead, they should incorporate nuanced communication strategies, such as targeted messaging and credible sources, to maintain engagement and effectiveness in addressing cancer-related concerns.
Finally, it is worth noting that while this study demonstrates statistically significant sequential mediation effects over three years, the small effect sizes suggest that FT may not be an independent driver of cancer screening behaviors. In other words, the impact of FT may be more significant when integrated with broader public health strategies. Other factors, such as health literacy, socioeconomic status, and social support, should also be considered when using FT to promote health behaviors, previous research has shown that these factors can facilitate the positive effects of health technology on health behaviors.113–115 For instance, one study found that individuals with higher health literacy are more likely to use health technology to engage in health behaviors. 116 In real-world settings, FT could complement other interventions aimed at increasing cancer screening rates, such as health education campaigns or improvements in healthcare accessibility. Future research should explore how FT can work in conjunction with other health promotion initiatives, such as educational programs or policy interventions, to create more comprehensive cancer screening strategies.
Limitations and future directions
This study has several limitations. First, the use of self-reported data may introduce recall bias, as participants might inaccurately report their technology usage or cancer screening behaviors. Self-reports are susceptible to various biases, including forgetfulness and social desirability bias. Future research could utilize objective data from fitness apps or wearable devices, such as device-tracked physical activity and cancer screening reminders, to validate participants’ self-reported behaviors, thereby enhancing accuracy. Secondly, given the repeated cross-sectional design, it cannot establish causal relationships between FT use, social media communication, cancer worry, and screening behaviors. To address this issue, future research could use longitudinal or panel data to track individual changes over time. This approach would provide a clearer understanding of how changes in FT use influence cancer screening behaviors. Longitudinal data can also control for individual-level confounders, helping to clarify the directionality of causal relationships. The third limitation of this study is the comprehensiveness of cancer screening. For instance, colorectal cancer screening was not included because the 2017 HINTS dataset only covered individuals with a history of cancer and did not represent the general female population. Given the significance of colorectal cancer in women's health, future studies should incorporate additional cancer screening programs to provide a more comprehensive understanding of cancer screening behaviors among women. Finally, emerging digital health technologies, such as AI-driven interventions, have the potential to overcome some of the limitations identified in this study. For example, AI-powered tools could analyze users’ behavior in real-time and deliver more personalized interventions that adapt to users’ specific health needs. These technologies could also provide more accurate tracking of health behaviors, reducing reliance on self-reports, and improve the accessibility and effectiveness of health interventions. Future research could explore how such technologies might enhance engagement with cancer screening behaviors, particularly in underserved populations, by offering more targeted and timely health communication.
Conclusion
This study demonstrates that FT positively influences cancer screening behaviors through communication on social media and cancer worry. While the effects fluctuated over time, the overall mediation remained stable. Future interventions should focus on nuanced communication strategies, like targeted messaging and credible sources, and incorporate emerging technologies such as AI-driven chatbots and telehealth to enhance engagement and effectively address cancer-related concerns.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251331893 - Supplemental material for The influence of fitness technology use on cancer screening behaviors among American women: Mediation by social media communication and cancer worry (2017–2020)
Supplemental material, sj-docx-1-dhj-10.1177_20552076251331893 for The influence of fitness technology use on cancer screening behaviors among American women: Mediation by social media communication and cancer worry (2017–2020) by Yingxia Zhu, Qingqing Xie and Xinshu Zhao in DIGITAL HEALTH
Footnotes
Ethical considerations
HINTS received approval from the Westat Institutional Review Board and was designated as exempt by the U.S. National Institutes of Health Office of Human Subjects Research Protections due to the deidentification of the data. Analyses using the HINTS database met the criteria for research involving nonhuman subjects, as determined by the Johns Hopkins University School of Medicine Institutional Review Board. Consequently, this analysis did not require additional review. Expedited approval for HINTS was obtained under project number 6048.14 (FWA 00005551).
Informed consent
This study used secondary data. The HINTS data make sure that participants provided informed consent for participation in the study.
Author contributions/CRediT
Yingxia Zhu developed the concept of this study; material preparation, data collection, and analysis were performed by Yingxia Zhu and Qingqing Xie; Xinshu Zhao contributed to the methodology and interpretation and made critical revisions.
Funding
This research was supported in part by grants of the Universidade de Macau and Macau Higher Education Fund (Grant Nos. CRG2021–00002-ICI, ICI-RTO-0010–2021, CPG2022–00004-FSS and SRG2018–00143-FSS, and HSS-UMAC-2020–02).
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.