
Abstract
The Internet has become an important and preferred source of health information. Although the literature has highlighted several key predictors that influence an individual’s online health information seeking behavior, insufficient attention has been paid to the changes in the predictors’ roles and effects over time. This study explores and compares the effects that specific predictors had on online health information seeking behavior over a period of 10 years by integrating and analyzing two Pew datasets collected in 2002 and 2012. Hierarchical regression analyses indicate that socio-demographic factors and overall health condition are significant predictors that had an increasing impact on online health information seeking behavior. However, the impact of Internet usage decreased significantly from 2002 to 2012. A comparison across time contributes to a vertical understanding of the changes in online health information seeking behavior and its predictors and helps health professionals and researchers tailor their informational interventions to meet the up-to-date needs and preferences of users.
Keywords
Introduction
The rapid growth of the Internet has significantly changed the landscape of information worldwide. In the health-care domain, the Internet has become an important and preferred source of public health information. 1 Unlike years ago when information was only available through medical professionals, individuals nowadays can conveniently access information at a low cost. 2 Evidence supports the benefits of online health information seeking behavior (HISB). For example, online HISB has been found to positively affect patients’ treatment decisions and coping mechanisms.3,4 In Fox’s 3 study, more than half of the respondents indicated that they felt better due to the health information they obtained online. Given the growing importance of online HISB as an active coping mechanism, a deep understanding of this concept and its promotion for individuals with various health concerns are highly desirable. 5
Several important predictors of online HISB, such as socio-demographic characteristics, overall health condition, and Internet usage, have been highlighted in the literature.6 –8 Individuals with a low socio-economic status are provided limited opportunities for high-speed, private, home-based Internet access. This socio-demographic digital divide prevents certain individuals from engaging in sufficient online HISB. Rice’s 8 study on general US populations demonstrated that being female, young, healthy, and highly educated contribute to increased online HISB. In addition, people with poor health tend to exhibit increased Internet usage for health-related purposes. 9 Many studies further assume that poor health and/or medical problems are the primary motivations for health-related uses of the Internet. 10 Individual Internet usage may also reflect one’s online HISB. For example, according to a 2008 Harris Poll, 11 81 percent of US adults have used the Internet to obtain health information. A similar result was reported by a European study wherein 71 percent of Internet users were found to use the Internet for health purposes. 12
In addition to descriptive studies, research with well-articulated conceptual frameworks has also been conducted to investigate the variables and relationships in the health information seeking domain. Marton 13 developed and tested a theoretical model of online HISB based on an exploratory multi-method study of 264 women. In her model, two situational factors, health condition and family caregiving, were found to be positively related to the frequency of HISB on the web. In addition, three demographic factors, racial identity, occupation, and household income, were found to have a statistically significant correlation with online HISB. Another model proposed by Fox 14 suggested that employed individuals with high incomes exhibit HISB more extensively than others because they have better Internet access. Fox’s study also indicated that Caucasians search for web-based health information more frequently than non-Caucasians. The study further noted that racial differences in the HISB of Caucasians and African Americans are disappearing in the United States.
The aforementioned studies have advanced our knowledge of the factors that influence the frequency and behavior of individuals seeking health information online. However, given that society is undergoing rapid and significant social development, these factors have changed significantly in recent decades. Similarly, the roles of these factors and their effects on online HISB may have also changed over time. Limited attention has been devoted on investigating these changes in online HISB. To address this research gap, the current study explores and compares the effects of the predictors of online HISB over the 10 years from 2002 to 2012.
Methods
This study integrated and re-analyzed two second-hand survey datasets that are available at the Pew Research Center’s website (http://www.pewinternet.org/). Permission was obtained from the Pew Research Center for the secondary analysis. The two survey datasets15,16 were selected for two reasons. First, the datasets are from the same research project, the Pew Internet and American Life Project. Therefore, most of the measurement items in the two datasets match and are comparable. Second, the datasets are both nationally representative datasets that investigate the Internet use of the general public in the United States. The findings from the two datasets are reliable and representative of the general population of the United States. The two datasets were collected by Princeton Survey Research Associates International through random phone interviews (both landline and cell phone) in December of 2002 and September of 2012. A total of 5477 adult respondents were involved in the study, with N = 2463 in 2002 and N = 3014 in 2012.
In the current study, we focused on the questionnaire items that measured socio-demographics, overall health condition, Internet usage, and online HISB. Although most of the items matched in the two datasets, we recoded the unmatched items to enable equivalent comparisons. For example, the self-rated health status was measured by a 4-point Likert scale in the 2002 dataset (1 (Excellent), 2 (Good), 3 (Only fair), 4 (Poor)), but it was measured by a 5-point Likert scale in the 2012 dataset (1 (Excellent), 2 (Very good), 3 (Good), 4 (Only fair), 5 (Poor)). We recoded the 5-point Likert scale (2012 dataset) into a 4-point Likert scale by combining the options of “Very good” and “Good” into the new option “Good”. The detailed recoding process can be found in Appendix 1.
Independent variables
Basic socio-demographic information was collected including age, gender, educational level, race, employment, income, marital status, and child guardianship. Overall health condition was measured with two indicators: (1) a 4-point self-rated health status (from 1 = “Excellent” to 4 = “Poor”), and (2) medical history over the past year. Internet usage was assessed by asking whether the respondents use the Internet frequently.
Dependent variables
In the original Pew survey, online HISB was measured by a series of questions asking whether the respondents had exhibited searching behaviors on several health-related topics. In the current study, we recoded these topics into the following five categories (see Appendix 1 for the recoding procedure): (1) a specific disease or medical problem, (2) a particular medical treatment or procedure, (3) a particular medication or drug, (4) healthy behaviors, such as nutrition and body maintenance, and (5) information related to health insurance. An overall score of online HISB for each individual was calculated by summing the number of “yes” responses to these five online search topics.
IBM SPSS was used to conduct the data analyses. Descriptive statistics were calculated to demonstrate the key characteristics of the respondents. A Chi-square test was then performed to investigate the changes in online HISB between 2002 and 2012. Finally, two hierarchical regression analyses were conducted to examine the effects of the predictors on online HISB in both 2002 and 2012. In the regression model, socio-demographic variables were entered into the first block. Overall health condition and Internet usage were entered into the second and third blocks, respectively.
Results
The key characteristics of the respondents in the study are shown in Table 1. Compared with those in 2002, the respondents in 2012 are generally older, less Caucasian, and less highly employed, but have a higher income level and decreased child guardianship; in addition, the respondents in 2012 include a higher number of females. In terms of overall health condition, the respondents in 2012 indicated a slightly lower level of self-rated health status. However, a much higher percentage of the respondents in 2012 had no medical history of visiting the emergency room or being hospitalized in the previous year. As expected, a higher percentage of the 2012 respondents were reported to be frequent Internet users.
Key characteristics in 2002 and 2012.

HISB: health information seeking behavior; SD: standard deviation.
Except for Gender (both 2002 and 2012) and Frequency of Internet usage (2012), other variables have missing data.
Percentages showed in this variable are counted only for valid cases.
Mean and SD for counts of individual participant’s “yes” responses from the five online HISB topics.
Changes in online HISB
Among the five health-related topics, disease was reported to be the dominant online search topic in both 2002 (64.3%) and 2012 (56.5%), followed by treatment and healthy behavior (see Table 1). According to the Chi-square test, with the exception of treatment (χ2 = 3.736, p = 0.053), online searches for the topics significantly decreased from 2002 to 2012. In other words, compared with the 2002 respondents, the 2012 respondents performed fewer online searches for health-related information on disease (χ2 = 23.548, p < 0.001), medication (χ2 = 71.348, p < 0.001), healthy behavior (χ2 = 86.044, p < 0.001), and health insurance (χ2 = 10.277, p < 0.005). As a result, their overall online HISB also showed a significant decrease from 2.3 to 1.9 (t = 8.078, p < 0.001) over the 10-year period.
Changes in the effects of the predictors
The results of the hierarchical regression analyses are shown in Table 2. The demographic factors that strongly predicted online HISB in both 2002 and 2012 were gender and education, indicating that being female and receiving a higher level of education led to increased online HISB. Additional characteristics, such as age, income, and child guardianship, were significant predictors in 2012, but not in 2002. Socio-demographics provided an increasingly significant explanation of the variance in online HISB (from 3.7% in 2002 to 7.5% in 2012). Overall health condition as a single block also provided an increasing contribution to online HISB (from 3.0% to 4.2% over 10 years). In other words, as time went by, overall health condition became a more significant predictor of online HISB. Among the variables comprising overall health condition, medical history was virtually the strongest predictor in both the 2002 (β = 0.146, p < 0.001) and 2012 (β = 0.166, p < 0.001) models. This result implies that individuals with denser medical histories (such as visiting the emergency room or being hospitalized) tend to exhibit a greater number of online health-related seeking behaviors. However, Internet usage exhibited a declining contribution from β = 0.121 (p < 0.001) in 2002 to β = 0.038 (p < 0.1) in 2012. The overall predictive ability of the independent variables in this study increased over 10 years, with the total variance explained ranging from 8.2 percent in 2002 to 11.9 percent in 2012.
Regression analysis predicting online health information seeking behavior in 2002 and 2012.
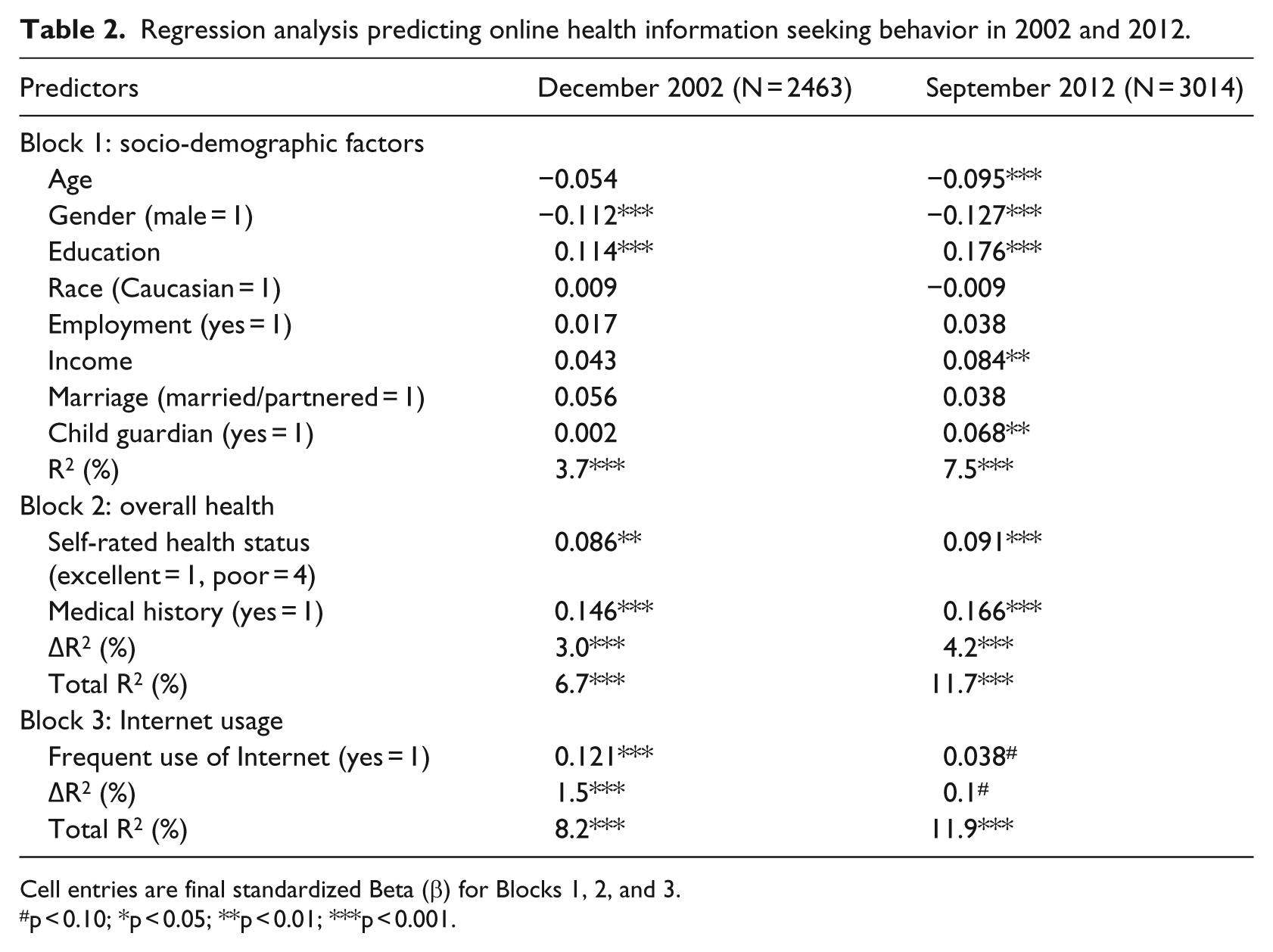
Cell entries are final standardized Beta (β) for Blocks 1, 2, and 3.
p < 0.10; *p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
This study is one of the first attempts to investigate how the effects of online HISB predictors change over time. By re-analyzing two survey datasets from the Pew Research Center, the current study has considerably extended the descriptive results of prior reports and contributed to individual studies on the Internet and health communication. The results suggest that seeking information on specific diseases, medical treatments, and healthy behaviors were the three primary factors that influenced online HISB in both 2002 and 2012. This implies that these three search topics are important motivations for online HISB, regardless of any social changes that occurred over a period of 10 years. However, for the majority of the topics under study, online HISB exhibited an unexpected decline from 2002 to 2012. A growing concern over online misinformation is a possible explanation for this decline. Given that the Internet is unregulated, a substantial proportion of the health information on the Internet might be inaccurate, erroneous, misleading, or fraudulent.17,18 With respect to the potential harm of misinformation, people have become more cautious in their online HISB in recent years. Another possible explanation is the methodological limitations of HISB measurements. In the original Pew survey dataset, an individual’s HISB was solely assessed with simple “yes or no” questions. The amount of information and search frequency, that is, how much information (about health content) one seeks and how frequently one searches for information over a period of time, are not reflected in the HISB measurements. Because individuals vary greatly along the dimensions of search quantity and frequency,19 –21 the changes in overall HISB in the study need to be interpreted with caution.
Overall, socio-demographics and health condition played an increasingly important role in affecting individuals’ online HISB over the 10-year period. The findings suggest that being female, young, and highly educated increased the respondents’ online health seeking, particularly in 2012. The results are consistent with those of previous studies22,23 reporting that female, educated, and young individuals are often active information seekers. Lee et al. 7 obtained a similar conclusion in their study, which was conducted on Hispanics in 2012. However, in contrast with previous studies that identified race24,25 and employment 8 as strong predictors, these two demographic factors had no significant influence on online HISB in the current study. Overall health condition was confirmed to be a consistent factor that explains online HISB. This finding supports the illness behavior model proposed by previous researchers,26,27 which indicates that individuals in poor health are more likely to seek health information online. Poor personal health status significantly causes a buildup of individual health concerns, which leads to an increase in health-oriented motivations for going online to search for relevant information.
Previous researchers have found that an increased exposure to Internet usage and other Internet activities supports online health information seeking. 8 However, the results of the present study showed that although this factor had a significant impact in 2002, Internet usage was an insignificant predictor in 2012. Given that the Internet continues to gain increasing popularity among the general public, overall Internet usage may possibly suffer from a decreased correlation with specific types of usage, such as the search for health information. These diminishing significant correlations may also be attributed to the relatively recent prevalence of mobile device–based Internet access. 14 Further investigation is needed to confirm and understand the impact of Internet usage on online HISB.
Conclusion
Studying the predictors of HISB is of great interest to health professionals and researchers. In addition to confirming the predictors identified in the HISB literature, the current study integrated and analyzed two Pew datasets. This study contributes to exploring the changes in the effects of these predictors from 2002 to 2012. The results suggest that socio-demographics and overall health condition had increasingly predictive effects on online HISB over the 10-year period, and that Internet usage became an insignificant predictor in 2012. Such a comparison across time provides a vertical understanding of the changes in HISB and its predictors and further inspires researchers and clinicians to tailor their informational interventions to meet individuals’ up-to-date needs and preferences.
Footnotes
Appendix
Newly recoded measurement items for unmatched items in 2002 and 2012 datasets

| Variables | December 2002 |
September 2012 |
New recoded measurement scale | ||
|---|---|---|---|---|---|
| Original scale | Recoding a | Original scale | Recoding a | ||
| Education | 1. None, or Grades 1–8 | 1 → |
1. Less than high school (Grades 1–8 or no formal schooling) | 1 → |
|
| 2. High school incomplete (Grades 9–11) | 2 → |
2. High school incomplete (Grades 9–11 or Grade 12 with NO diploma) | 2 → |
|
|
| 3. High school graduate (Grade 12 or GED certificate) | 3 → |
3. High school graduate (Grade 12 with diploma or GED certificate) | 3 → |
|
|
| 4. Business, technical, or vocational school AFTER high school | 4 → |
4. Some college, no degree (includes community college) | 4 → |
|
|
| 5. Some college, no 4-year degree | 5 → |
5. Two-year associate degree from a college or university | 5 → |
|
|
| 6. College graduate (BS, BA, or other 4-year degree) | 6 → |
6. Four-year college or university degree/Bachelor’s degree (e.g. BS, BA, AB) | 6 → |
|
|
| 7. Postgraduate training/professional school after college (master’s degree/PhD, law, or medical school) | 7 → |
7. Some postgraduate or professional schooling, no postgraduate degree | 7 → |
||
| 8. Postgraduate or professional degree, including master’s, doctorate, medical, or law degree (e.g. MA, MS, PhD, MD, JD) | 8 → |
||||
| Employment | 1. Employed full-time | 1 → |
1. Employed full-time | 1 → |
|
| 2. Employed part-time | 2 → |
2. Employed part-time | 2 → |
|
|
| 3. Retired | 3 → |
3. Retired | 3 → |
||
| 4. Not employed for pay | 4 → |
4. Not employed for pay | 4 → |
||
| 5. Disabled (VOLUNTEERED) | 5 → |
5. (VOL.) Have own business/self-employed | 5 → |
||
| 6. Student (VOLUNTEERED) | 6 → |
6. (VOL.) Disabled | 6 → |
||
| 7. Other (VOLUNTEERED) | 7 → |
7. (VOL.) Student | 7 → |
||
| 8. (VOL.) Other | 8 → |
||||
| Self-rated health status | 1. Excellent | Not recoded | 1. Excellent | 1 → |
|
| 2. Good | 2. Very good | 2 → |
|
||
| 3. Only fair | 3. Good | 3 → |
|
||
| 4. Poor | 4. Fair | 4 → |
|
||
| 5. Poor | 5 → |
||||
| Frequent use of Internet | 1. Several times a day | 1 → |
1. Yes | Not recoded |
|
| 2. About once a day | 2 → |
2. No |
|
||
| 3. 3–5 days a week | 3 → |
||||
| 4. 1–2 days a week | 4 → |
||||
| 5. Every few weeks | 5 → |
||||
| 6. Less often | 6 → |
||||
| Online HISB b | a. Information about a specific disease or medical problem | a → |
a. A specific disease or medical problem | a → |
|
| b. Information about a certain medical treatment or procedure | b → |
b. A certain medical treatment or procedure | b → |
|
|
| c. Information about experimental treatments or medicines | e → |
c. Health insurance, including private insurance, Medicare, or Medicaid | c → |
|
|
| d. Information about alternative treatments or medicines | f → |
d. Pregnancy and childbirth | e → |
|
|
| e. Information about diet, nutrition, vitamins, or nutritional supplements | g → |
e. Food safety or recalls | f → |
|
|
| f. Information about exercise or fitness | j → |
f. Drug safety or recalls | h → |
||
| g. Information about prescription or over the counter drugs | o → |
g. Medical test results | k → |
||
| h. Information about immunizations or vaccinations | p → |
h. How to lose weight or how to control your weight | (Drop items of d, g, i, j, l) | ||
| i. Information about how to quit smoking | (Drop items of c, d, h, i, k, l, m, n) | i. How to reduce your health-care costs | |||
| j. Information about problems with drugs or alcohol | j. Caring for an aging relative or friend | ||||
| k. Information about depression, anxiety, stress, or mental health issues | k. A drug you saw advertised | ||||
| l. Information about environmental health hazards | l. Any other health issue | ||||
| m. Information about sexual health | |||||
| n. Information about a particular doctor or hospital | |||||
| o. Information related to health insurance | |||||
| p. Information about Medicare or Medicaid | |||||
GED: General Educational Development; HISB: health information seeking behavior.
Numbers/Alphabets in bold are the recoded scale.
Participants were asked to answer whether they have ever looked for health topics listed in each item. We count individual participant’s “Yes” responses from each item.
Acknowledgements
The two datasets used in the study are originally from Pew Research Center. Pew Research bears no responsibility for interpretations presented or conclusions reached based on analysis of the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Singapore National Research Foundation under its International Research Centre @ Singapore Funding Initiative and administered by the IDM Programme Office.