
Abstract
Disasters can hinder access to health information among cancer patients. However, little is known regarding overall health information exposure (HIE), its barriers and its impacts on attitudes toward healthcare among cancer patients in the long-term aftermath of disasters. The aims of this study were threefold: assess the extent of HIE; identify associations between family composition and a non-engagement with HIE; and examine the effects of HIE on attitudes toward healthcare among local cancer patients—5 years after the 2011 triple disaster (earthquake, tsunami, and nuclear disaster) in Fukushima, Japan. We conducted self-administered surveys with all cancer and non-cancer surgery department outpatients at Minamisoma Municipal General Hospital (MMGH), Minamisoma City, from October 2016 to January 2017. In total, 404 patients (263 cancer patients and 141 non-cancer patients) voluntarily participated in the study. The results revealed that a regular level of HIE occurred among 90.5% of the cancer patients. In cancer patients, family composition was not significantly associated with HIE, and HIE was not associated with attitude toward healthcare. In conclusion, most cancer patients visiting the MMGH surgical department were regularly engaged in HIE.
Keywords
Introduction
The National Academy of Medicine, formerly known as the Institute of Medicine, regards patient-centered care as one of six important qualities of healthcare. 1 To achieve this goal, it is important for healthcare professionals to guarantee that patients gain necessary health information according to their own health information needs. 2 Previous studies investigated health information behaviors specifically in conditions with chronic and fatal natures; including cancer, 3 chronic heart failure, 4 and chronic pulmonary diseases. 5 Health information behaviors among cancer patients have drawn the most prominent attention because of their unique characteristics: including strong stigma, 6 wide range of social impacts,7,8 and accelerated development of treatment in recent years.9,10
Cancer patients have extensive health information needs (e.g. disease/treatment, self-care management, health services, and work/finance) to manage their treatment and daily lives. 11 Health information from medical (healthcare professionals) and non-medical (family and friends, mass media, and the Internet) sources is important for this population, as interaction with these sources can not only help them properly understand their own diseases, but also enhance their medical compliance, healthy lifestyle changes, and more active health-related decision making.12–14
Concepts of health information behavior can be categorized mainly as health information exposure (HIE) and active avoidance of health information.14,15 The mode of HIE can be further classified into health information seeking (HISE; active seeking of health information) 16 and health information scanning (HISC; unintentional or serendipitous encounter with health information). 17 Traditionally, HISE has been a primary study focus in health information research.12,14 However, there has been an increasing awareness that HISE occupies only one mode of HIE, and that HISC is a more prevalent and natural way to obtain health information during an individual’s daily routine. 18 Consequently, HISC has also become an important topic in research for health information behavior. Previous studies have found that the amount and frequency of HISE and HISC differs between individuals according to their demographic characteristics (e.g. sex, age, ethnicity, marital status, and education),17,18 eHealth literacy, and more. 19
In addition to individual characteristics, in the past several decades there has been a growing understanding of how the subjective matter of HIE can be influenced by broader contexts that shape experiences of the population under study, including profession, social roles, and community and cultural norms. 14 As such, disasters are important but underrepresented contexts that deserve an in-depth study of health information behavior. Further, given the detrimental impact of disasters on cancer patients, overall HIE should be a priority for assessment. Major disasters often cause healthcare facility closures and an outflow of healthcare professionals (HCPs), which can impair access to necessary health information, such as where to continue cancer treatment and factors to be considered during evacuation.20,21 In addition, some types of disasters (such as nuclear disasters) lead to long-term relocation of cancer patients’ family members and friends, thereby restricting social support channels for patients who remain in the affected area.22–26 Cancer patients’ family members and friends facilitate timely medical consultations and treatments,22–26 and their absence may impair patients’ access to necessary health information. Further, such disasters are reported to induce intangible and long-term tensions in affected societies and communities.27,28 However, there is little information regarding the long-term effects of disasters on cancer patients’ overall HIE and its barriers, and how HIE might affect their attitude toward healthcare following disasters. This information would enable local HCPs to develop policies that would effectively provide health information to support cancer patients in the long-term aftermath of disasters.
On 11 March 2011, an earthquake and tsunami struck the Fukushima Daiichi nuclear power plant (FDNPP; Figure 1), and the subsequent nuclear accident broadly disseminated radioactive materials in the surrounding area. Minamisoma City (Figure 1), which is located 10–40 km north of the FDNPP, was struck by all three disasters. 29 Some parts of Minamisoma City fell into the mandatory evacuation or sheltering zone, which were first determined by the central government on March 12, 2011, with subsequent modifications (Figure 1). 30 While five hospitals had been engaged in cancer treatment in Minamisoma City before the disasters, the disasters caused closure of the Watanabe hospital (Figure 1). 24 Further, post-disaster evacuation accelerated depopulation and population aging in the city,30,31 with the population decreasing from 70,878 on October 1, 2010 to 54,455 on October 1, 2018, 32 and the proportion of residents 65 years or older increasing from 26.5% to 35.5% during this period. 32
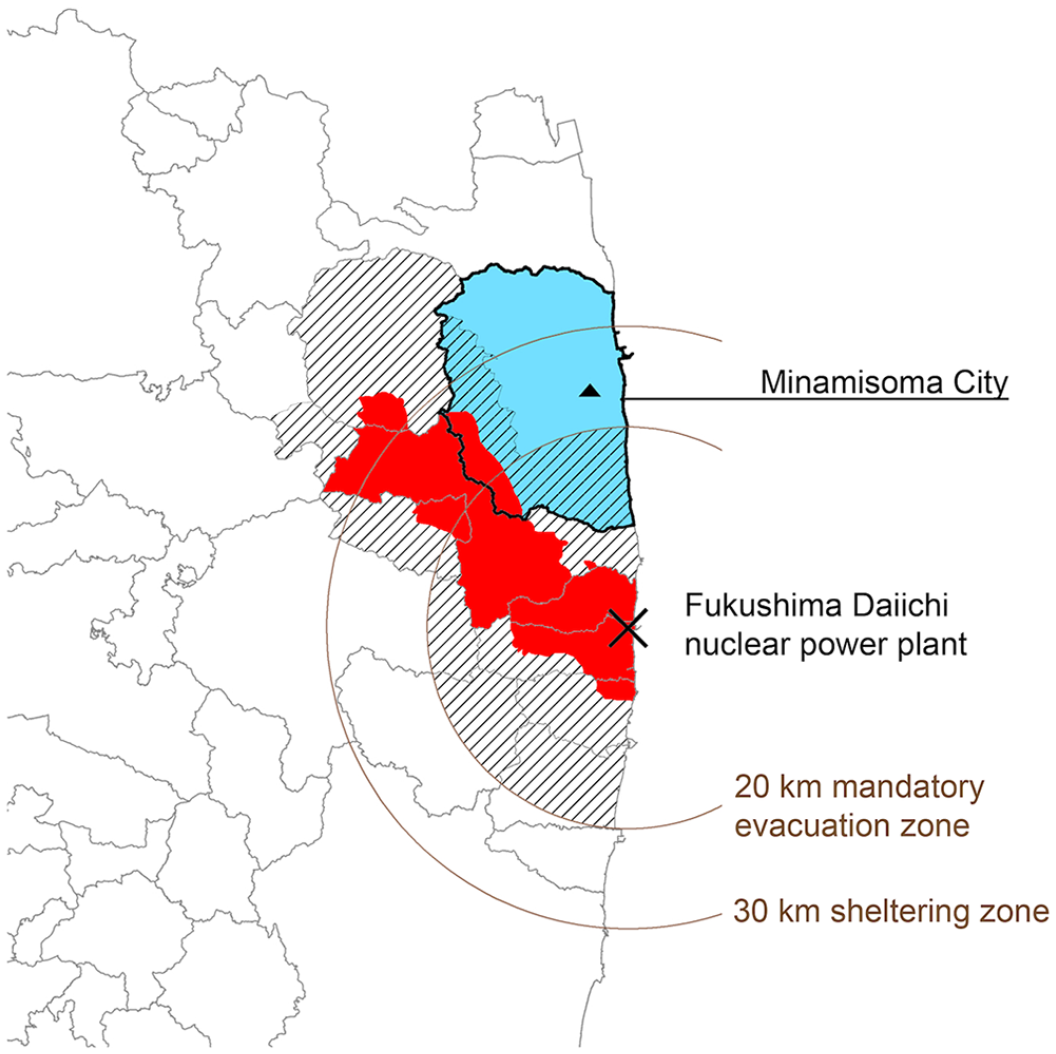
Geographical location of Minamisoma City and the Fukushima Daiichi Nuclear Power Plant, with transition of evacuation zones over time. Minamisoma City is located 10–40km to the north of the Fukushima Daiichi Nuclear Power Plant. Following the earthquake and subsequent tsunami on March 11, 2011, an initial hydrogen explosion occurred at reactor 1 of the nuclear power plant on March 12, 2011, and the areas within 20 and 30 km radius of the power plant were designated as mandatory evacuation and sheltering zones, respectively. The evacuation zone was expanded (in border, red) on April 22, 2011, and again at later dates, lifting orders from certain places (in border) with the progress of restoration work; however, the order remained in effect primarily in areas with severe contamination near the power plant (in red), as of June 1, 2019. Minamisoma Municipal General Hospital (triangle) is located 23 km north of the power plant, which is within the sheltering zone. Permission for the use of this image has been granted by ESRI Japan Corporation.
In this context, we previously reported a male colorectal cancer patient who had originally lived alone and further lost opportunities for socialization with friends after the 2011 Fukushima disaster. 22 While he had been aware of his bloody stool for over 1 year, a lack of knowledge about its seriousness led to a delayed presentation and an advanced stage diagnosis of colorectal cancer 5 years after the disaster (June 2016). 22 In this regard, we believe that a further evaluation on the larger population is required to more comprehensively grasp health information behavior among cancer patients in the long-term aftermath of the present disaster. Given that both HISE and HISC would comprise only one part of the approach that cancer patients use to deal with health information, 14 we considered that HIE—a combined measure of HISE and HISC—would be a suitable indicator to adopt in an initial attempt to evaluate health information behavior in the affected cancer patients. This means that, in addition to the task oriented HISE among the cancer patients, we followed their unintentional encounters with health information.
The primary objectives of this survey-based study were to assess the extent of HIE among cancer patients in the disaster-struck area in Fukushima, to examine family composition associated with non-engagement in HIE, and to assess potential associations between HIE and cancer patients’ attitudes toward healthcare.
Materials and methods
Settings and participants
The study setting was a surgery department outpatient office at Minamisoma Municipal General Hospital (MMGH; Figure 1), which is located 23 km to the north of the FDNPP. While MMGH structural damages were limited in the 2011 disasters, normal care was suspended at its outpatient offices on the day of the disaster (March 11, 2011). 33 Further, given the risk of potential irradiation, the total number of hospital employees decreased from 239 to 71 by March 14, 2011, 33 and delivery of medical and other essentials supplies (e.g. food) from outside the area were stopped. 34 As a result, the 195 and 43 patients hospitalized before and after the disaster were all discharged by March 20, 2011 (five were discharged by death, 134 were self-discharged or discharged with their families, and). 33 However, MMGH restarted normal outpatient and inpatient functions in multiple departments, including the surgical department, in June 2011. 24 Thereafter, MMGH provided all types of cancer care except for radiation therapy. 26 The MMGH surgical department has treated breast, thyroid, and gastrointestinal cancers and non-cancer diseases, including inguinal hernia, cholecystitis, and trauma, both pre- and post-disaster. When the study was planned and undertaken in 2016, four surgeons worked for the MMGH surgical department and performed approximately 300 operations per year. Both the number of surgeons and number of surgeries were the highest in the city; other city hospitals had only one or two surgeons.
Following a previous study, 17 all adult cancer and non-cancer patients (⩾18 years old) who visited the MMGH surgical department outpatient office from October 17, 2016 to January 31, 2017 were eligible. This study period (3 months or more) was determined based on an assumption that most of the patients who routinely visited the outpatient office could be invited to participate in the study since patients are allowed to receive a maximum of a 3-month prescription for most drugs in Japan. The non-cancer patients from the same department were enrolled as a control group. Since this study aimed to present an overview of HIE among cancer and non-cancer patients in the disaster-struck area, we did not set inclusion or exclusion criteria based on clinical factors among the cancer patients, including disease stage or type of active treatments. According to previous studies, a large proportion of the cancer patients who regularly visited the MMGH had continuously lived in Minamisoma City or the surrounding area prior to the disaster.24,35 In contrast, the non-cancer patients were more likely to have migrated from different areas for recovery works after the disaster. 36
Survey
This survey was conducted using a voluntary self-administered questionnaire, and survey items were created by the authors through review of previous literature,17,18,37 while considering the local and post-disaster context of cancer care in Minamisoma City. Trained hospital staff briefly introduced the study and distributed it (described below) to patients who agreed to participate in the study. We informed the patients that the obtained data would be anonymized and analyzed for academic publication. Patients could request assistance from hospital staff or attendants during completion of the survey. The survey was first piloted with our colleagues, and their feedback was used to finalize it.
Variables
Primary diagnosis
We extracted participants’ primary disease from their medical records and categorized it into cancer and non-cancer conditions. Those designated as cancer patients had already been diagnosed when recruited for the study.
Clinical factors relating to cancer (only for cancer patients)
For cancer patients, we collected data on clinical characteristics including disease stage (Stage 0, Stage I, Stage II, Stage III, or Stage IV), receipt of surgery before the survey was conducted (no (or no planned surgery) or yes), active treatment (no active treatment, hormonal therapy, cytotoxic agents, molecularly targeted therapy and cytotoxic agents, molecularly targeted therapy and hormonal therapy, and molecularly targeted therapy), and disease recurrence before the survey was conducted (yes or no). As for disease stage, we used the final stage following surgeries for primary diseases, and clinical stage for the rest.
Sociodemographic factors
Sociodemographic factors included age at survey administration, sex, educational attainment (junior high school or below, high school, business or junior college, or university or higher), employment status (full-time job or self-employed, part-time job, or unemployed), marital status (married, separated or widowed, or never married), and family composition before and after the disaster. Age and sex were also extracted from the medical record. All other measures came from the participants’ survey responses. Regarding family composition, we separately asked whether the patients lived together with a partner, children, or those other than a partner and children in both periods. We combined the responses to these items and created variables addressing change of family composition pre- and post-disaster for the following categories of family compositions: any types of family member, a partner, children, and those other than a partner and children. For instance, in the case of a partner, the variable was categorized into four groups (living together with a partner both pre- and post-disaster; not living together with a partner pre-disaster, but living together with a partner post-disaster; living together with a partner pre-disaster, but not living together with a partner post-disaster; or not living together with a partner pre- or post-disaster).
General health-related factors
General health-related factors included self-rated health, from the item “How much do you agree that you are currently in a good health condition?” measured on a four-point scale (strongly agree, agree, disagree, or strongly disagree). We also asked about family history of cancer (yes or no), total count of medications (five or above, four, three, two, one, or zero), smoking status (currently smoke, previously smoked, or never), care or support need certification (yes or no), 38 and activities of daily living status (independent or not independent). 39
Exposure to health information
To assess the extent of HIE, we used the item “How frequently are you usually exposed to health information” (everyday, once every few days, once per week, once per month, or never). Since our primary interest was overall HIE, we considered all kinds of health information, unlike the Health Information National Trends Survey in the US.18,40 Further, according to the previous literature, it is not always the case that more information is better, since too much information may lead to information overload among patients. 14 Thus, this variable was transformed into a dichotomous measure (other than never or never) for the analyses. We coded the “other than never” response as the base outcome.
Reliable non-medical sources of information
To assess reliable non-medical sources of information, we used the item “Do you rely on the following information sources?” The patients reported whether they relied on family and friends, television, radio, newspaper, magazine, central government, municipality government, newsletters, personal websites, institutional websites, and social networking services, using a two-point scale (yes or no).
Attitudes toward healthcare
Attitudes toward healthcare were assessed using the following item for cancer patients, “How much do you agree that it would be important to regularly see a physician for your cancer at the surgical department?” (strongly agree, agree, disagree, or strongly disagree). While the response of this item was transformed into a three-group measure (strongly agree, agree, or disagree) owing to the small number of “disagree” and “strongly disagree” responses, we attempted to capture differences between the responses used in the Likert scale.
Data analysis
We conducted three analyses. First, we conducted descriptive analyses of the sociodemographic and clinical variables, comparing the cancer and non-cancer groups based on these measures. We used the Mann-Whitney U test for continuous variables and Fisher’s exact test and chi-squared test for categorical variables, as appropriate. Similarly, we calculated the proportion of patients who were usually exposed to health information, with the variable “exposure to health information,” and that of the patients who relied on 11 non-medical sources of information. Furthermore, cancer patients’ attitudes toward healthcare were evaluated.
Second, to clarify the characteristics of cancer patients who were not exposed to health information (no exposure to health information), a logistic regression model for the variable “exposure to health information” was constructed, coding the patients who answered “other than never” as the base outcome. As covariates, we considered all clinical factors relating to cancer as well as sociodemographic and general health-related factors, and variables relating to reliable non-medical sources of information, using the backward stepwise variable selection method (inclusion criteria, p < 0.1). The primary interest of this analysis was to detect any association between the exposure to health information and family composition, and covariates other than family composition were treated as confounding factors. As mentioned above, regarding family composition, we considered a partner, children, family members other than a partner and children, and any type of family member. Of these four variables, only one in the final model was retained, determined by the significance of the association with the variable “no exposure to health information.” The covariates with a small number of participants were re-grouped, as necessary. The same model was constructed for non-cancer patients for comparison (clinical factors were only available for cancer patients). Effects of missing data were examined using the multiple imputation method under the missing at random assumption as a sensitivity analysis. The variation inflation factor (VIF) for the variables used in the final model to assess multi-collinearity was estimated, using the Stata command “Collin.” 41 Third, to assess associations between exposure to health information and cancer patients’ attitudes toward healthcare, we created ordinal logistic regression models for attitudes toward healthcare, coding the “disagree” response as the base outcome. Alongside the exposure to health information, all clinical factors relating to cancer as well as sociodemographic and general health-related factors were considered, using the backward stepwise variable selection method (inclusion criteria p < 0.1). Regrouping of the covariates, estimations of VIF, and analyses using multiple imputation methods were similarly performed in the second analysis, but the control group (non-cancer patients) was excluded in this analysis, given the nature of the item. All analyses were performed using Stata/IC 15.0.
Ethics approval
The MMGH ethics committee (approval number: 30-10) and Fukushima Medical University (approval number: 3064) assessed and granted approval for this study.
Results
A total of 493 successive patients (305 cancer and 188 non-cancer patients) who visited the MMGH surgery outpatient office during the study period were eligible for the study. Of these, 404 (82.0%) agreed to participate (263 (86.2%) cancer patients and 141 (75.0%) non-cancer patients). All participants were included in the analyses. When compared with those who did not participate in the study, those who participated tended to be younger (p = 0.022), female (p = 0.026), and cancer patients (p = 0.002; Table 1).
Baseline characteristics of the patients who participated in the study and those who did not.
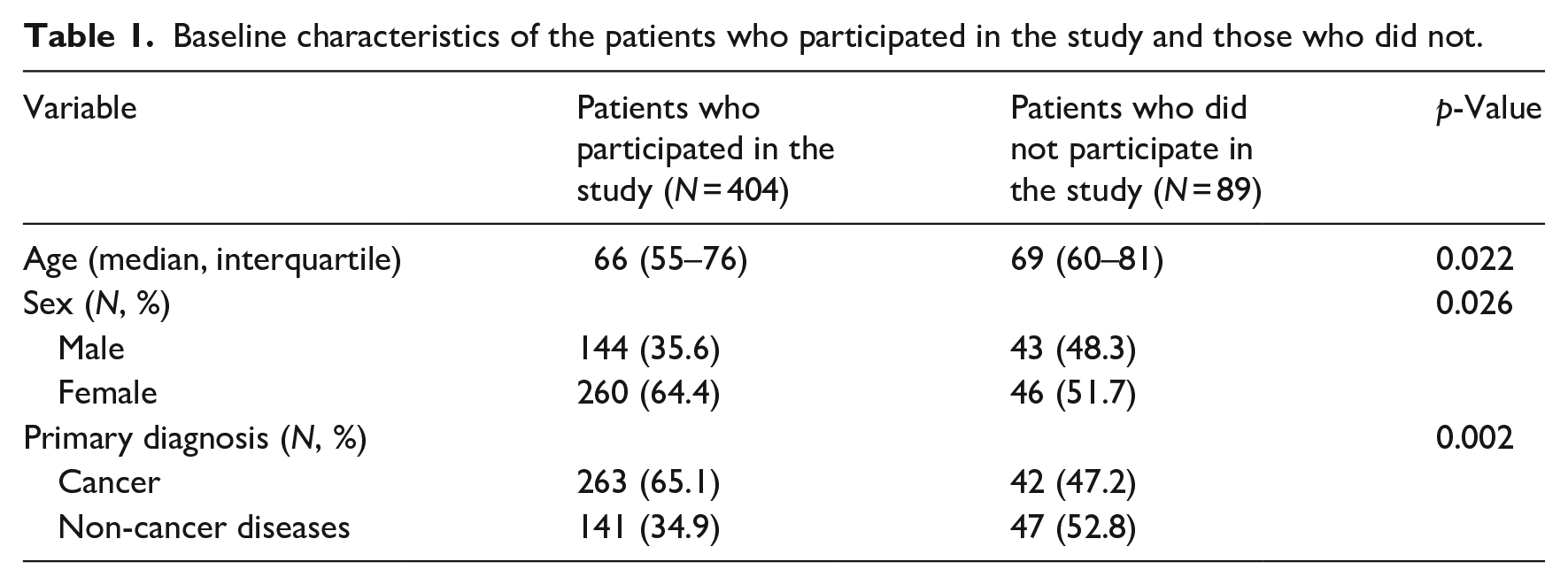
Table 2 shows the primary diagnosis, and sociodemographic and health-related characteristics of the patients. Breast cancer accounted for 45.6% of all cancer patients, while, among the non-cancer patients, the most common condition was thyroid/parathyroid diseases (23.4%).
Patients’ primary diagnosis, clinical, sociodemographic, and general health-related characteristics. a

Proportions and p-values were calculated for the patients without missing values.
As for clinical factors of cancer patients, Stage I disease was the most common (40.2%), and 55.5% of the patients did not receive active treatment for cancer when the survey was conducted. Further, 8.8% of the patients had experienced disease recurrence by the time the survey was conducted.
Cancer patients were significantly older (67 vs 63, p < 0.001) and tended to be women (70.0% vs 53.9%, p = 0.001) than non-cancer patients. There were also significant differences between cancer and non-cancer patients in the distribution of employment (p < 0.001) and marital status (p = 0.011), while no difference was found in educational attainment (p = 0.097) and changes in family composition.
Self-rated health (p = 0.230), the proportion of care or support need certification (4.4% vs 6.5%, p = 0.351), or the proportion of impaired activities of daily living (19.1% vs 20.7%, p = 0.693) did not significantly differ between the cancer and non-cancer patients. The proportion of patients who had a family history of cancer was larger among cancer patients than non-cancer patients (68.3% vs 53.3%, p = 0.004).
Table 3 shows the frequency of health information exposure, sources of health information, and attitudes toward healthcare among the patients. In total, 90.5% of the cancer patients and 88.7% of the non-cancer patients were exposed to health information at least once per month. Among both cancer and non-cancer patients, the most reliable source of information was television (73.0% vs 66.7%, p = 0.182). Newspapers (49.4% vs 39.7%, p = 0.062) and family and friends (47.5% vs 56.0%, p = 0.103) were other information sources that both populations relied on. In contrast, newsletters (2.3% vs 0.0%, p = 0.071), social networking services (1.5% vs 2.8%, p = 0.365), and personal websites (3.0% vs 7.1%, p = 0.060) were unpopular sources of information. The proportion of cancer patients who strongly agreed or agreed that it was important to regularly see a physician at the surgical department for their cancer was 80.4% and 17.3%, respectively.
Frequency of health information exposure, information sources, and attitudes toward healthcare. a

Proportion and p-values were calculated for the patients without missing values.
Table 4 shows the multivariable logistic regression analyses for no exposure to health information. Among the cancer patients, those living together with a partner either pre- or post-disaster did not have a significantly lower or higher probability of no exposure to health information, compared to those who lived together with a partner neither pre- nor post-disaster (odds ratio (OR) 0.82, 95% confidence interval (CI) 0.30–2.30). In contrast, among non-cancer patients, those living together with a partner either pre- or post-disaster had a significantly lower probability of no exposure to health information than those who lived together with a partner neither pre- nor post-disaster (OR 0.26, 95%CI 0.08–0.89). Among cancer patients, older patients had a higher probability of no exposure to health information compared to younger patients (OR 1.05, 95%CI 1.01–1.10). Similarly, those who had no family history of cancer had a higher probability of no exposure to health information than those who did (OR 3.19, 95%CI 1.22–8.36). Furthermore, those who relied on newspapers as an information source had a significantly lower probability of no exposure to health information than those who did not (OR 0.33, 95%CI 0.11–0.97). Among non-cancer patients, those with an education level of junior high school or below had a higher probability of no exposure to health information than those with an education level of high school or above (OR 8.56, 95%CI 2.55–28.68). The VIF for each variable used in the models for cancer and non-cancer patients was sufficiently low. The variable “recurrence before the survey was conducted” did not converge in the model, since all of those with the recurrent diseases were exposed to health information at least once per month (data not shown). We found that all of the sensitivity analysis estimates from the multiple imputation method were similar to the main analysis (Table 5).
Multivariable logistic regression models for no exposure to health information among cancer and non-cancer patients. a

CI: confidence interval.
Only the variables which were kept in the final models for the cancer and non-cancer patients are presented in the table.
VIF of the variables included in the final model ranged from 1.01 to 1.02 and was judged to be sufficiently low.
VIF of the variables included in the final model ranged from 1.02 to 1.06 and was judged to be sufficiently low.
Multivariable logistic regression models for no exposure to health information among cancer and non-cancer patients with multiple imputation method.

CI: confidence interval.
IF of the variables included in the final model ranged from 1.01 to 1.03 and was judged to be sufficiently low.
VIF of the variables included in the final model ranged from 1.01 to 1.05 and was judged to be sufficiently low.
Table 6 shows findings of the multivariable ordinary logistic regression model for attitudes toward healthcare among cancer patients, which were constructed to assess the association between health information exposure and attitudes toward healthcare among the cancer patients. After adjusting for covariates, exposure to health information was not significantly associated with attitudes toward healthcare among the cancer patients (OR 1.44, 95%CI 0.47–4.42). In contrast, educational attainment, marital status, and family history of cancer were all associated with attitudes toward healthcare. Those with lower educational attainment (OR 0.50, 95%CI 0.22–1.12), those other than married (OR 0.49, 95%CI 0.24–1.02), and those without a family history of cancer (OR 0.42, 95%CI 0.20–0.86) tended not to agree with the statement that it would be important to regularly see a physician at the surgical department for their cancer. Again, VIF for each variable used in the models for cancer patients were sufficiently low, and the sensitivity analysis estimates from the multiple imputation methods were similar to the main analysis (Table 7).
Multivariable ordinary logistic regression model for attitudes toward healthcare among cancer patients (N = 242). a

CI: confidence interval.
VIF of the variables included in the final model ranged from 1.03 to 1.09 and was judged to be sufficiently low.
Multivariable ordinary logistic regression model for attitudes toward healthcare among cancer patients, using the multiple imputation method (N = 263). a

CI: confidence interval.
VIF of the variables included in the final model ranged from 1.03 to 1.11 and was judged to be sufficiently low.
Discussion
We primarily found that approximately 90% of cancer patients were routinely engaged in HIE. Other important findings were: (1) while variables relating to family composition were not significantly associated with HIE among cancer patients, the cancer patients may have relied the most on newspapers as a health topics information source, and disease recurrence strongly motivated the patients to be committed with HIE; and (2) there was no clear association between HIE and attitude toward healthcare among the cancer patients. This study is the first to comprehensively assess HIE among cancer patients in the long-term aftermath of a nuclear disaster.
It is difficult to directly compare these results with previous findings, given the difference in contexts where the studies were undertaken (disaster or non-disaster settings; Japan or outside of Japan) as well as concepts (HIE, HISE, or HISC), survey items, type of health information (cancer-related health information or other types of health information), participants (cancer survivors or general population), and time scales (1 month, 1 year, or throughout the past) of health information behaviors to be assessed between studies.15,17,18,40,42,43 Considering these facts, it is still meaningful to explore the previous findings to deepen the interpretation of the observed findings. For example, previous studies conducted with non-cancer general populations in non-disaster settings in the US have reported that 29%–65% and 49%–90% of the participants were routinely engaged in cancer-related HISE and HISC.17,18,42 Similarly, studies among non-cancer general populations in non-disaster settings in Japan have reported that 52% of the population were engaged in HISE in the past 2 years. 43 With regard to cancer survivors in the US, those who had been engaged in HISE increased from 67% in 2003 to 81% in 2013.
Nevertheless, the proportion of participants engaged in HIE can be regarded as reasonably high in our study. This can be considered a good sign, given that HIE is a key element for enhancing cancer patients’ health.17,18 There are three plausible explanations for this. First, we did not split HISE and HISC unlike previous studies.17,18,42 As a result, a larger proportion of the participants may have been identified as being engaged in HIE than those estimated using an individual measure of HISE or HISC as in past studies. Second, the target populations in previous studies differed from our target population. Chiefly, the previous studies targeted a general population outside medical institutions, while this study targeted patients who visited a health facility for their illnesses. In this sense, it is possible that our patients had higher baseline interest in health information than previous study participants, and a high interest in health information may have led to enhanced engagement in HIE. Third, this study involved a unique local context—the aftermath of a nuclear disaster. After the 2011 disaster, health concerns associated with potential irradiation remained strong in Minamisoma City. 44 Further, increases of non-communicable diseases, including diabetes mellitus have been also reported. 30 Such situations may have elevated the baseline interest in health information among the local residents, enhancing their engagement in HIE.
Associations between family composition and health information exposure differed between cancer and non-cancer patients. In the cancer patients, family composition did not predict health information exposure. In contrast, in non-cancer patients, not living together with a partner predicted a lack of health information exposure. One possible reason for this difference may be related to the baseline interest in health information of the two populations. The cancer patients may have had a higher baseline interest in health information than the non-cancer patients, possibly because of differences in the nature of their illnesses. Another possible explanation is that the cancer patients may have gained more necessary health information from HCPs than the non-cancer patients, because cancer patients would likely visit hospitals and clinics more regularly and for a longer period than non-cancer patients. Moreover, patients’ condition and cancer staging varied widely among cancer patients; hence cancer patients’ physicians may be more adept at tailoring health information to patients than patients’ family members. Previous studies have suggested that HCPs were cancer patients’ preferred health information source. 12 Therefore, it may be unnecessary for cancer patients to rely on family members for health information.
Newspapers were another important information source among cancer patients. Half of the cancer patients in our study indicated that they relied on newspapers as an information source, while those who did not were significantly less likely to be routinely exposed to health information. Reliance on television, radio, or magazines as information sources did not predict health information exposure, despite their popularity as information sources. Compared with other types of media, newspapers provide more comprehensive information, including health-related information, on a daily basis, likely increasing health information exposure. This may be particularly true in Fukushima, where two major regional newspapers (Fukushima Minpo and Fukushima Minyu) are published, along with other nationwide newspapers, playing an important role as information sources for many local residents after the disaster. 45
In contrast, only a small proportion of the patients in our study relied on Internet-related health information sources, such as online newsletters, social networking services, and personal websites. Previous studies have also found that these were unpopular information sources in Fukushima after the disaster, 45 which is consistent with our findings. Although the Internet provides access to diverse health information, our patients were generally older, and the study setting was a rural area. Both old age and rural location have been reported to predict reduced Internet use.46,47 In addition, after the disaster, the area experienced a mass evacuation of young people who were the primary Internet users. 47 Thus, our patients may have had limited opportunities to learn how to use the Internet.
We found that all the cancer patients who had experienced disease recurrence were regularly exposed to health information regardless of cancer type. In contrast, other cancer-related factors such as disease stage, surgery for primary disease, and active treatment were not even significant in the univariate analysis for no exposure to health information (data not shown). In other words, disease recurrence strongly leads cancer patients to be committed with HIE. While our literature review did not detect articles on this topic, this finding is quite reasonable given our clinical experience for cancer care. Concretely, most of the disease recurrences mean that their cancer would be incurable, needing increasingly uninterrupted treatment, namely more frequent hospital visits and treatments, than curable diseases. Furthermore, the disease recurrence naturally worsens cancer patients’ state of mental health. 48 To address these health information needs, they may seek or unintentionally scan health information more often than their counterparts.
In cancer patients, HIE did not predict patients’ views on the importance of regular physician visits for their illnesses. Given that sociodemographic factors, such as lower educational attainment and unmarried status, combined with clinical factors, such as no family history of cancer, were associated with negative attitudes toward healthcare, our results could be simply interpreted as a limited effect of HIE on positive attitudes toward healthcare. Given the nature of their disease, the cancer patients may have recognized the importance of regular physician visits, regardless of the health information they were exposed to. Previous studies suggested various health outcomes associated with HIE, including increased health knowledge, increased acceptance of preventive health behaviors, and increased participation in cancer screening programs. 17 Further studies are warranted to investigate possible cancer patient health outcomes using these well-verified measures.
Limitations
This study has several limitations. First, we were only able to include data from a limited number of cancer and non-cancer patients treated at a single institution. Given that the MMGH performs the largest number of surgeries in Minamisoma City, the present findings would largely reflect those in the city. However, some patients may have visited institutions outside the city to seek better care than that provided at the MMGH; we speculate that these patients would differ from our sample on clinical and sociodemographic factors as well as level of access to health information. 49 Further, our patients may not have accurately reflected the typical cancer and non-cancer population who regularly visited the surgical department outpatient office in the area affected by the 2011 disaster, let alone the overall population of cancer and non-cancer patients in the area. However, to mitigate any potential effects of selection bias, we constructed separate regression models for no exposure to health information among cancer and non-cancer patients (Table 4) and also performed their sensitivity analyses using multiple imputation methods (Table 5).
Second, we did not investigate the types of health information patients accessed through HIE. For example, a previous study suggested four types of health information sought by cancer patients (disease/treatment, self-care management, health services, and work/finance). 11 Future studies should assess the type of health information sought by cancer patients in the post-disaster context.
Clinical implication of the study and future perspectives
Despite the abovementioned limitations, we believe that the current findings can be used to help patients meet their own health information needs in the course of their treatments. The present findings can be utilized to find populations that are not likely to be committed to HIE: those who do not have family history of cancer, those who do not rely on newspaper as an information source, and those with low educational attainments. Thus, in the initial assessment of cancer patients, the presence of these characteristics as well as the extent of HIE should be routinely evaluated. Further, a regular commitment with HIE among the cancer patients with recurrent diseases would suggest a necessity for extra support not only to meet their own health information needs, but also in other aspects of their lives with cancer. Thereby, health care professionals and other hospital staff can tailor their interaction with these patients. More specifically, given that the previous evidence clearly reveals that patients strongly trust the health information provided by HCPs, 50 and that cancer patients regularly see them, hospital staff will be primary players not only in motivating patients to be engaged in HIE, but also in directly providing health information the patients need.
Noticeably, these findings are directly incorporated into cancer care in the MMGH and surrounding medical institutions to improve their cancer patients’ care. Additionally, we believe that the findings will also become the foundation for future studies. First, more detailed assessments focusing on cancer types should be performed in the future, given differences and similarities in HIE and health information needs between cancer types. 51 In those analyses, vital cancer-related factors such as disease stage and active treatment should be considered. Second, additional assessments based on HISC and HISE should be conducted, given potential differences in their clinical implications. For example, HISE is reported to influence decision making of the participants more so than HISC.15,52 In that context, it should also be evaluated how well cancer patients use the exposed health information to cope with their own diseases. Third, it is important to evaluate whether HIE and reliable information channels will differ across locations and disasters. Thereby, better methods for providing health information to cancer patients in disaster contexts can be developed, and hopefully some of the findings can be generalizable to non-disaster settings.
Conclusion
In this study, we found that the majority of cancer patients were regularly engaged in HISC, relying mostly on newspapers as their information source for health topics. Family composition was not significantly associated with HIE among cancer patients. There was also no clear association between HIE and attitudes toward healthcare among the cancer patients. It is important to perform further studies to more comprehensively grasp HIE and its potential implication among cancer patients.
Footnotes
Acknowledgements
We express our gratitude to Mr. Masatsugu Tanaki and other staff at the Minamisoma Municipal General Hospital for data collection and management. We also express our gratitude to Ms. Yuka Harada, Ms. Kayo Harada, and Ms. Hitomi Sasaki for their constructive opinion on the study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Akihiko Ozaki receives personal fees from Medial Network Systems, MNES Inc., outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by grants from the Toyota Foundation (D17-R-0540), the program of the Network-type Joint Usage/Research Center for Radiation Disaster Medical Science of Hiroshima University, Nagasaki University, and Fukushima Medical University (![]() ), and MRT Inc. The funding sponsors had no role in the design of the study, in the collection, analyses, or interpretation of data; in the writing of the manuscript or in the decision to publish the results.
), and MRT Inc. The funding sponsors had no role in the design of the study, in the collection, analyses, or interpretation of data; in the writing of the manuscript or in the decision to publish the results.