
Abstract
Implementation of eHealth is now considered an effective way to address concerns about the health status of health care consumers. The purpose of this study was to review empirically based eHealth intervention strategies designed to improve health literacy among consumers in a variety of settings. A computerized search of 16 databases of abstracts (e.g. Biomedical Reference Collection, Cochrane Central Register of Controlled Trials, Computers & Applied Sciences Complete, Health Technology Assessments, MEDLINE) were explored in a systematic fashion to assess the presence of eHealth applications targeting health literacy. Compared to control interventions, the interventions using technology reported significant outcomes or showed promise for future positive outcomes regarding health literacy in a variety of settings, for different diseases, and with diverse samples. This review has indicated that it is feasible to deliver eHealth interventions specifically designed to improve health literacy skills for people with different health conditions, risk factors, and socioeconomic backgrounds.
Introduction
Patients with limited health literacy may not have the requisite skills to effectively interact with the health system and engage in appropriate self-care, such as know-how to take their medications and to understand labels and other health information. Literacy for health information is emerging as a key factor related to health status.1,2 There are many definitions of health literacy, but for the purpose of discussing the role of eHealth applications, the working definition of health literacy is the following: “The degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions.” 3 This definition focuses on individual capability and does imply needed skills. 4
Low health literacy has been linked to poorer health status, increased hospitalization rates, and non-adherence to medications across a number of diseases.1,5,6 It has been related to self-reported poor health, 7 risk for hospital admission,8,9 reduced participation in cervical cancer screening, 10 poor self-management in patients with diabetes, 11 and unstable hemoglobin A1C concentrations in patients with diabetes. 12 Low levels of health literacy are associated with greater use of health services7,13 and with higher health costs 14 in Medicare enrollees. Elderly persons with low health literacy report that they have more chronic health conditions, worse physical functioning, and poorer mental health,15,16 and minority elderly persons with lower health literacy report more chronic health conditions than whites with similar health literacy levels.15,17 Additional studies have linked limited health literacy to medication dosing errors and increased mortality. 18
While there is evidence to suggest that low levels of health literacy are associated with inferior health outcomes, increased hospitalization rates, and non-adherence to medications across a number of diseases, relatively few effective interventions have been developed to address low literacy and even less have been developed that target ethnic minority populations prone to lower health literacy rates. The interventions that exist, however, rely primarily on communication and education alone and have mostly failed to achieve substantial and sustainable behavioral change. 19 Increased interest in health literacy has emerged in part due to continuing changes in the delivery of health care services. These changes create new responsibilities for patients and their caregivers, which include finding and evaluating information, self-monitoring of health status, and understanding financial constraints and obligations. Thus, a person’s health depends more and more on his or her ability and willingness to carry out a complex set of related behaviors. This set of behaviors is essential for patients who often must make decisions about treatment with complex combinations of medications.
The task of obtaining optimal care is likely to be difficult for individuals with low levels of health literacy. As the US health care system becomes more complex, this problem is likely to increase further. 20 One possible approach to addressing low health literacy is to create interventions that can be easily understood, are acceptable, easily deployed, cost-effective, and readily accessible on the Internet. Yet few studies have systematically reviewed the current information technology (IT)-based interventions related to improving health literacy.
eHealth applications
eHealth is the application of information communication technologies across all range of functions involved in the practice and delivery of health care.21,22 IT-based interventions used to promote health literacy have the potential for being readily available over the Internet and on handheld devices such as smartphones and tablets. The field of eHealth is promising in that it can support and enable health behavior change and aid in the prevention and management of disease. 23 Once created, these interventions can be easily sustained as costs for their continued maintenance and deployment are relatively low. One study suggested that new advances in multimedia could be used to better disseminate patient education 25 . Technology-enabled health research and care has emerged in the past decade as a dynamic field that may offer great potential to help produce better outcomes in key risk patients. This alternate strategy for increasing patients’ knowledge of pertinent health care related information has been to provide it through computers and mobile devices.
Trends in eHealth applications and health literacy
Strategies to promote health literacy at the individual patient level have relied heavily on paper materials such as pamphlets and brochures. Some recommend emphasizing the need for drawing upon communication and social science theories of information behavior, using a range of traditional and novel formats, gaining better understanding of the public’s health information needs, and developing medical informatics solutions for tailoring applications to patients’ needs and abilities. 25 However, some studies have shown that the effectiveness and patient satisfaction with web-based health education materials are greater than if presented in a traditional format. 26 For individuals who have learned to rely upon oral forms of communication or who have low literacy levels, written information sources may be of little or no use. Current trends indicate eHealth technology will continue to expand. Due to the multiple variables involved with health care, any health literacy application will need to be multi-faceted, comprehensive, and culturally and linguistically appropriate. As a result, it is important to understand patients’ individual health decision-making abilities.
Regarding technology use, a survey conducted in Harlem 27 found that 77 percent of the 646 adult residents aged 18 years and older said they had used a computer and 87 percent reported having friends or family who use the Internet. This is useful information for understanding diffusion of and normative support for technology use. The survey also found that 68 percent of respondents had one or more computers at home and 57 percent used the Internet at home. For those who did not have a computer at home, 76 percent said they knew where a computer was publicly available. Of the respondents, 60 percent said that the most important problem in accessing the computer is overcrowding. Other problems in access were cost (2%), equipment problems (4%), location or transportation (8%), and hours of operation (13%). Such data show an interest exists in using technology in low-income minority communities.
The Harlem study also revealed that native English speakers are more likely to use the Internet, African-Americans are more likely to be Internet users than Hispanics/Latinos, and Internet users are more likely to have higher educational attainment, be employed, and have higher incomes than those who do not use the Internet. Little is known about the extent to which certain racial/ethnic minority groups have access to, or interest in, using the Internet for health-related activities. More research is needed to gain information about how health consumers from racial/ethnic minority communities use technology and seek health information.
The goal of this article was to review empirically based eHealth intervention strategies designed to improve health literacy among health care consumers. Specifically, this review aimed to (1) identify and summarize types of eHealth applications and technologies being used to improve health literacy; (2) discuss effectiveness of eHealth applications to improve health literacy based on reports of attributes; and (3) assess the gaps in knowledge and make recommendations for future research in eHealth applications to improve health literacy. This literature review also strives to add to the biomedical informatics knowledge base and demonstrates how existing health literacy strategies might be used with various populations.
Rationale for the research question
The challenge facing biomedical informatics researchers is to disseminate knowledge and enrich the perspective of both health practitioners and consumers to ensure the highest quality of care possible. One common, but incorrect, assumption is that all health consumers understand medical and health information related to their illness and are thus able to make informed decisions about their treatment protocols and health care options. In fact, physicians often overestimate patients’ literacy levels. 28
Creating eHealth interventions to improve health literacy will aid in extended duration and quality of life for patients. Traditional methods (i.e. pamphlets, talking) may not be as effective as delivering information through alternate venues. In order to promote continued research on the impact of eHealth applications that improve health literacy in patients, it is important to continually and empirically evaluate the research literature to better understand what is known, what remains unknown, and any future trends in the field. To address this gap in knowledge, we sought to identify and review the most current technology-based applications designed to improve health literacy. Observations and implications for future study in the area will also be explicated.
Methods
A review of the current state of the science regarding types of eHealth technology for health literacy interventions was conducted. We used the US Department of Health and Human Services 18 Healthy People 2010 definition of health literacy, “the capacity to obtain, process and understand basic health information and services needed to make appropriate health.” The study selection criteria flowed directly from the review question (i.e. What are the current eHealth interventions to improve health literacy?) and were specified a priori. Interventions had to include at least one eHealth delivery component (e.g. touchscreen computer, handheld electronic device, Internet delivered, and one measure of (or components related to) health literacy to promote positive change in lifestyle behaviors for improved health outcomes). Studies also had to have been completed with outcome reports; interventions not yet implemented were excluded.
Search strategy
Inclusion and exclusion criteria
Inclusion and exclusion criteria were established in advance. Studies were included when their authors (1) were published in scholarly (peer reviewed) journals, (2) discussed eHealth interventions that included at least one health literacy component or measure, (3) evaluated eHealth applications addressing health literacy likely to be accessed by consumers, and (4) provided quantitative and/or qualitative results or information on the effectiveness of the applications.
Identification of studies
A computerized search of 16 databases of scientific abstracts were explored in a systematic fashion to assess the presence of eHealth applications to improve health literacy or conceptually related terms within their taxonomies, to identify refereed journals in which articles explicitly referring to eHealth and health literacy are contained and the topics covered, and to identify published definitions of the concept. Using the initial keyword search “health literacy” AND “health information technology” AND “eHealth” OR “e-Health,” 466 articles were identified from 16 databases: AgeLine, Applied Science & Technology Full Text (H.W. Wilson), Biomedical Reference Collection: Comprehensive, CINAHL Complete, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Cochrane Methodology Register, Computers & Applied Sciences Complete, Family & Society Studies Worldwide, General Science Full Text (H.W. Wilson), Health Technology Assessments, International Pharmaceutical Abstracts, MEDLINE, Nursing & Allied Health Collection: Comprehensive, OmniFile Full Text Mega (H.W. Wilson), and Social Sciences Full Text (H.W. Wilson) with limits for English language, AND published within the past 10 years. Studies that dealt with development or evaluation of psychometric instruments to measure the construct of health literacy itself (e.g. Test of Functional Health Literacy in Adults (TOFHLA) and the Rapid Estimate of Adult Literacy in Medicine (REALM)) were excluded.
Data extraction
After this broad search was conducted, a Boolean/phrase search using the keywords “health literacy” AND “computer” AND “technology” was conducted, yielding 45 citations (duplicate articles were eliminated). Journals associated with eHealth and health literacy (i.e. Journal of the American Medical Informatics, International Journal of Medical Informatics, Patient Education and Counseling, Journal of Medical Internet Research) were searched manually for relevant research. Reference lists from the most pertinent articles were also examined. General Internet searches using combinations of the search terms at the Google search engine were also conducted. After extracting only those studies on eHealth interventions that met the above inclusion, criteria were selected, leaving a total of 12 studies retained for this review (see Figure 1).
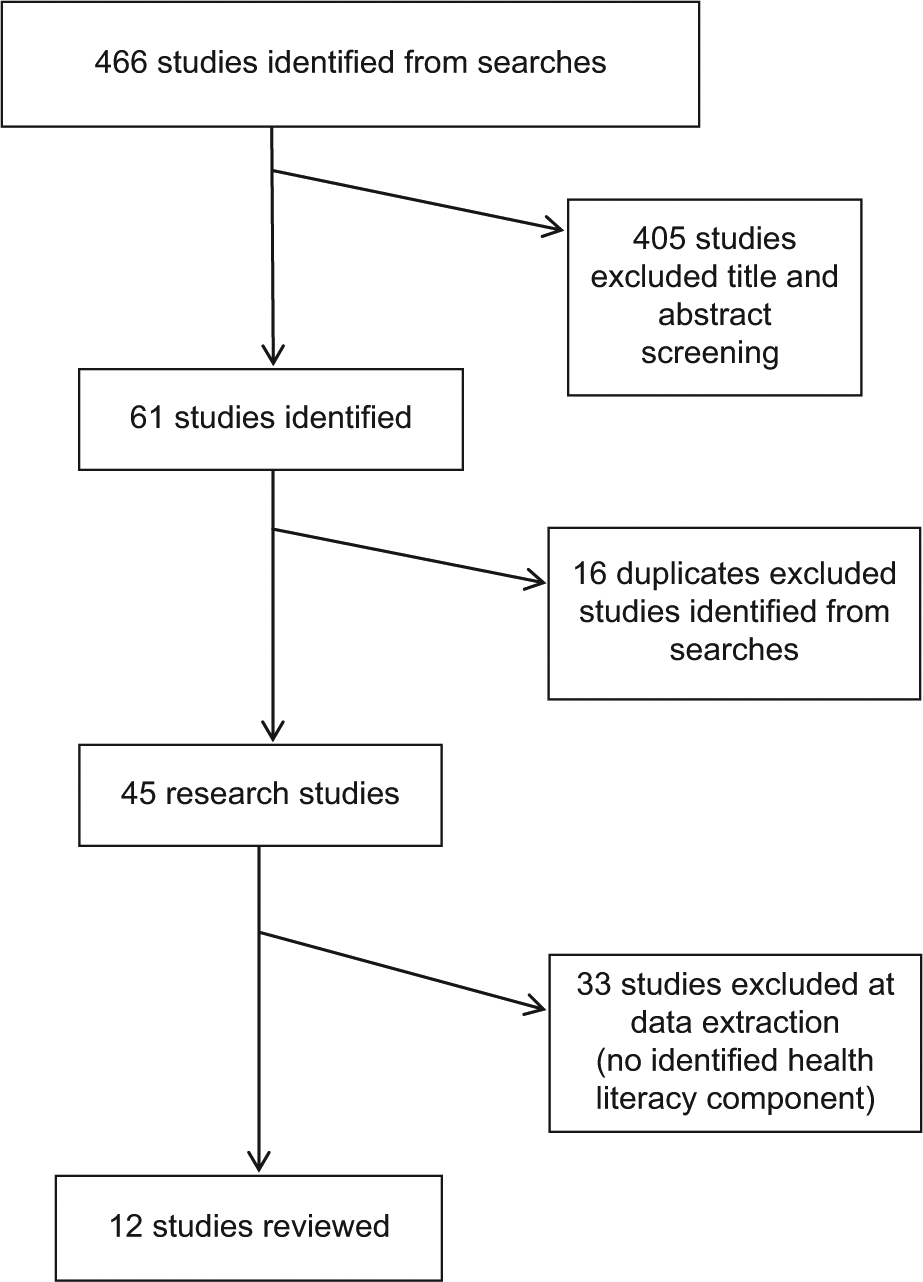
Flowchart of review.
Due to differences in study methods and rigor, quality criteria, study population, and topic chosen (e.g. specific illness or condition), study results and conclusions on computer-based applications for improving eHealth literacy vary widely. Thus, only overall descriptions of the major types of eHealth application technologies currently being used or tested are reported.
A number of health literacy outcome scales and measures were identified for the review. For functional health literacy, these included the Wide Range Achievement Test (WRAT), REALM, TOFHLA, Health Activity Literacy Scale, Newest Vital Sign, Short Assessment for Spanish Speaking Adults, and the disease-specific knowledge assessment, the Diabetes Care Profile. Interventions were assessed to be effective if a statistically significant positive change was reported for health literacy and/or one health risk behavior. Experimental and quasi-experimental studies, descriptive, and controlled and non-controlled before and after studies were included.
Results
In total, 12 intervention studies identified were implemented in hospitals (n = 1), the community (n = 7), or other settings such as outpatient clinics (n = 3) and worksite (n = 1). Studies were from the United States (n = 9), Australia (n = 2), and The Netherlands (n = 1). There were four randomized-controlled trials, four before and after studies, two quasi-experimental/non-randomized-controlled trials, one descriptive study, and one beta test (see Table 1). Some studies used standard care to compare against eHealth intervention format (i.e. Gerber et al., Kiropoulos et al., Yager and O’Dea, and Cook et al.) or a no intervention waiting-list control group to compare against their eHealth intervention (i.e. Oenema et al.). The reminder used a “before and after” or descriptive study (see Table 1).
eHealth interventions to promote health literacy.
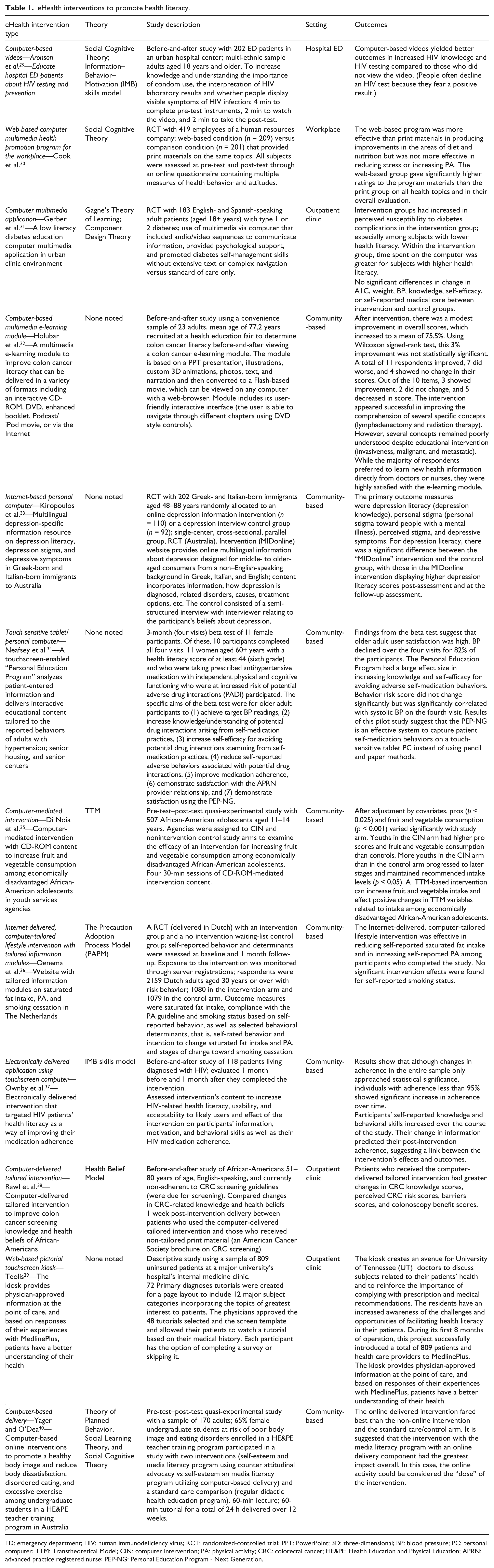
ED: emergency department; HIV: human immunodeficiency virus; RCT: randomized-controlled trial; PPT: PowerPoint; 3D: three-dimensional; BP: blood pressure; PC: personal computer; TTM: Transtheoretical Model; CIN: computer intervention; PA: physical activity; CRC: colorectal cancer; HE&PE: Health Education and Physical Education; APRN: advanced practice registered nurse; PEP-NG: Personal Education Program - Next Generation.
The interventions targeted a variety of health risks, lifestyles, and disease (illness) management: cardiovascular disease risk of individuals with familial hypercholesterolemia; diabetes; colon cancer; body image and eating disorder risk; dietary practices, stress, physical activity; depression; human immunodeficiency virus; neonatal intensive care issues; hypertension; hemodialysis; and multiple medical issues.
Theoretical underpinnings of the interventions included Transtheoretical Model (TTM), Theory of Planned Behavior, Social Learning Theory, Social Cognitive Theory, Health Belief Model, Information–Motivation–Behavior (IMB) skills model, The Precaution Adoption Process Model (PAPM), Gagne’s Theory of Learning, and the Component Design Theory. Of the 12 interventions, 4 did not specify a theoretical foundation.
The eHealth platforms included personal computers (desktops/laptops), tablets, netbooks, touchscreen computers, and personal digital assistants (PDA) with web-based applications that included multimedia applications such as videos and interactive self-help tools.
General characteristics of the interventions
Computer-based applications were the most common intervention delivery platform; three of those used touch-sensitive screen computers. Interventions of all types had a health literacy component and were associated with significant positive changes in health outcome and/or health literacy scores. The majority of studies compared electronically delivered interventions that measured changes in participant’s health-related behavior. All eHealth intervention types were similarly effective for changes in health behavior activity. Samples were multicultural and ages of participants ranged from 11 years to adults aged 65 years and older. The majority of the interventions (n = 9) were in English only, one was offered in Spanish and English; one was offered in Greek, Italian, and English; and one was offered in Dutch only. Quantitative and/or qualitative reports of user satisfaction were high in all the interventions where satisfaction was evaluated.
Multiple interventions used a mix of modalities for delivering content. For example, one used multiple video segments (on HIV prevention, symptoms, and testing literacy) who otherwise not be reached and examined how context can be optimized for greater effectiveness as measured by cognitive and behavioral outcomes. 29 Holubar et al. 32 developed a multimedia educational module based on a PowerPoint presentation and included illustrations, custom three-dimensional (3D) animations, photos, text, and narration. Articulate e-learning authoring software was used to export the PowerPoint presentation to a Flash-based movie. This multimedia e-learning module (to improve colon cancer literacy) can be delivered in a variety of formats including an interactive CD-ROM, DVD, enhanced booklet, Podcast/iPod movie, or via the Internet. Another intervention used a computer-mediated intervention with CD-ROM content without the need for Internet to affect positive dietary behavior changes among economically disadvantaged African-American adolescents who may not have easy access to the Internet. 35 Tailoring the type of delivery modality for different patient groups and subgroups was thought to be more beneficial than a one-size-fits-all approach.
Four of the interventions were not theoretically grounded.32–34,39 Interventions that were theoretically grounded all used some type of decision-oriented health behavior theory. Due to the diversity of the interventions and the scope of this analysis, it is not feasible to comparatively assess whether having a theoretical foundation made a difference in outcomes.
Compared to control interventions (e.g. standard care without technology), the interventions using IT reported significant outcomes in both health literacy and/or at least one lifestyle behavior. These interventions varied in intensity from a onetime 2-min video to 24-h intervention (in 60-min intervals) delivered over 12 weeks. There were significant positive outcomes in increased HIV knowledge and HIV testing; 29 fruit and vegetable consumption among adolescents; 35 colorectal cancer knowledge scores, perceived risk scores, and colonoscopy benefit scores; 38 and healthy body image and reduction in body dissatisfaction, disordered eating, and excessive exercise. 40 A web-based pictorial touchscreen kiosk provided physician-approved information at the point of care, and based on responses of their experiences with MedlinePlus®, patients have a better understanding of their health. 39 A total of 72 primary diagnoses tutorials were created for a page layout to include 12 major subject categories incorporating the topics of greatest interests, allowing their patients to watch a tutorial based on their medical history.
Interventions with mixed results
A diabetes education computer multimedia application delivered in an urban clinic environment found intervention groups increased perceived susceptibility to diabetes complications in the intervention group, especially among subjects with lower health literacy. Within the intervention group, time spent on the computer was greater for subjects with higher health literacy. However, no significant differences in change in A1C, weight, blood pressure, knowledge, self-efficacy, or self-reported medical care between intervention and control groups. 31
Participants in an intervention with outcome measures of diet, stress, and physical activity reported significantly higher ratings for the web-based program materials than the print program on all health topics and in their overall evaluation. However, the e-intervention was not more effective in reducing stress or increasing physical activity compared to the control intervention. 30
A multilingual depression-specific information resource on depression literacy, depression stigma, and depressive symptoms in Greek-born and Italian-born immigrants in Australia showed that for depression literacy, there was a significant difference between the intervention and the control group, with those in the intervention displaying higher depression literacy scores post-assessment and at the follow-up assessment. However, there was no significant difference in stigma or depression levels between the intervention and the control group at pre-assessment, post-assessment, or at the follow-up assessment. 33
A multimedia e-learning module to improve colon cancer literacy showed only a modest improvement in overall scores. Using Wilcoxon signed-rank test, this 3 percent improvement was not statistically significant. A total of 11 respondents improved, 7 did worse, and 4 showed no change in their scores. Out of the 10 items, 3 showed improvement, 2 did not change, and 5 decreased in score. The intervention appeared successful in improving the comprehension of several specific concepts (lymphadenectomy and radiation therapy). However, several concepts (i.e. invasiveness, malignant, metastatic) remained poorly understood despite educational intervention. 32
Findings from the beta test of a touchscreen “Personal Education Program” that analyzed patient-entered information and delivered interactive educational content tailored to the reported behaviors of adults with hypertension showed blood pressure declined over the four visits for 82 percent of the participants. The Personal Education Program had a large effect size in increasing knowledge and self-efficacy for avoiding adverse self-medication behaviors. However, behavior risk score did not change significantly but was significantly correlated with systolic blood pressure on the fourth visit. 34
The Netherlands-based randomized-controlled trial of an Internet-delivered, computer lifestyle intervention using tailored information modules on saturated fat intake, physical activity, and smoking cessation was effective in reducing self-reported saturated fat intake and in increasing self-reported physical activity among participants who completed the study, but no significant intervention effects were found for self-reported smoking status. 36
The results from an Internet-delivered computer-based intervention that targeted HIV patients’ health literacy as a way of improving their medication adherence showed that although changes in adherence in the entire sample only approached statistical significance, individuals with adherence less than 95 percent showed significant increases in adherence over time. Participants’ self-reported knowledge and behavioral skills increased over the course of the study. Their change in information predicted their post-intervention adherence, suggesting a link between the intervention’s effects and outcomes. 37
Four of the interventions34,36–38 utilized tailoring techniques. Expert recommendations for health literacy interventions include rejecting a “one-size-fits-all” approach 41 and creating interventions that promote participant engagement and retention through interactivity, interesting multimedia elements, and ensure learning through an interactive teach-evaluate-reteach-when-needed algorithm. 42 Ownby et al.37,43 reported that computer-delivered tailored information intervention focused on promoting HIV-related skills and knowledge was effective in improving knowledge and medication adherence and eliminating race-related knowledge disparities in persons treated for HIV.
Discussion
Overall, compared to control interventions, the interventions using technology reported significant outcomes or showed promise for future positive outcomes regarding health literacy in a variety of settings, for different diseases, and with diverse samples. Several employed a variety of modalities for delivering content. Interactive media delivered via eHealth interventions and applications provide opportunities for patients to act as engaged users instead of passive receivers of information. 44
Five of the interventions yielded mixed results.30,32,34,36 This may be due to the fact that some concepts are more difficult to understand or a lifestyle behavior is more difficult to change. For example, Holubar et al. 32 multimedia intervention to promote colon cancer literacy was successful in improving the comprehension of some concepts (lymphadenectomy and radiation therapy), but several concepts remained poorly understood despite educational intervention (i.e. invasiveness, malignant, metastatic). Adjustments may be needed to accommodate different levels of difficulty in more complex concepts. Oenema et al.’s 36 Internet-delivered, computer-tailored lifestyle intervention was effective in reducing self-reported saturated fat intake and in increasing self-reported physical activity, but no significant intervention effects were found for smoking. This may have more to do with the relatively low effectiveness of nonpharmacologic smoking cessation treatments in general.
The likelihood of interventions being effective did not appear to be related to the modality (touchscreen versus traditional computer) or the length/intensity of the intervention. A few studies that evaluated lower intensity interventions (such as the use of the 2-min video on HIV testing and prevention) were effective in changing behavioral outcomes. This finding is significant in that it will influence decisions about benefits versus costs of eHealth interventions to be adopted and supported. Applications that promote health literacy do not necessarily have the need to be extensive and expensive or require huge commitment in the way of training by providers who implement them. However, it is difficult to ascertain whether accessing eHealth interventions alone was successful or whether some of the improvements may have been, at least partly, due to the wider sources of information available on the Internet.
Considerations for future research
Interventions delivered via technology should provide culturally relevant health information and decision support to consumers with low literacy. Only two interventions31,33 were linguistically and culturally adapted. Two other studies35,38 recruited participants on the basis of racial characteristics (African-Americans). Studies suggest that race and ethnicity have some association with communication processes because of the ways that race can act as a proxy for cultural factors. 45 Nonetheless, few studies have explicitly assessed the significance of race, ethnicity, or culture on participants’ interaction with and response to health ITs.
Tailoring content to make eHealth interventions more personally relevant promotes patient engagement and is related to post-intervention behavior change, including among those from minority populations and with low levels of education and computer experience.46–48 Tailoring interventions to enhance their racial and ethnic relevance enhance their effects for blacks49,50 and Hispanics. 51 Computer-based algorithms that take a person’s specific goals or needs into account in addition to characteristics such as language, age, gender, ethnicity, reading ability, and health literacy level might prove more efficacious.
Although tailoring and cultural/linguistic adaptation can be effective, it may require substantial effort if the assessment of both individual characteristics and related tailoring is required. This has led researchers to investigate the effectiveness of computer-based culturally appropriate automated tailoring applications since computer-based tailoring can require much less effort and thus be considerably more cost-effective. Achieving robust, comparable samples to measure the efficacy of tailored eHealth interventions can be challenging. Methodological complications surface when evaluating the effectiveness of tailored messaging programs because, by definition, participants do not receive exactly the same intervention. More advanced analysis strategies need to be applied in order to adequately address this challenge.
Conclusion
Understanding and measuring patients’ health literacy in relation to behavioral risk factors is an important goal in the prevention, detection, and management of chronic diseases. A concern is the fact that overall health literacy rates are poor and even poorer for individuals from lower socioeconomic and/or ethnic minority backgrounds. Implementation of eHealth and health ITs is being considered as an effective alternative in addressing current concerns about the health status and quality and safety of the US health care consumer population. Thus, it is imperative that we ascertain best practices for delivering health literacy interventions using IT that is accessible and cost-effective. There is also a risk that eHealth and use of new technologies in health care might widen health inequalities. This review has indicated that it is possible to deliver eHealth interventions specifically designed to improve health literacy skills for people with different health conditions and risk factors. There is also evidence to suggest eHealth interventions may be more effective particularly for individuals with very low literacy. What remains less clear is the extent to which patients will feel comfortable using a computer or handheld electronic device or will have access to interactive eHealth programs using these modalities. It is also likely that understanding how the health care system works in addition to eHealth interventions is an important aspect of health literacy. Before eHealth interventions can be hailed as a behavior change intervention of the future, the effective components and mechanisms need to be identified, rigorously tested, and its cost-effectiveness established in different contexts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.