
Abstract
Background
The internet is most people's primary source of (health) information. However, no validated instrument exists to assess eHealth literacy in the group of patient with cardiac diseases.
Objective
The objective of this study was the evaluation of the psychometric properties of the German revised version of the eHealth literacy scale (GR-eHEALS) in individuals with coronary artery disease (CAD) and congestive heart failure (CHF).
Methods
A cross-sectional study was conducted. N = 455 were included in the statistical analyses. The assessment compromised the GR-eHEALS, medical history, sociodemographic data, and technology-related data. Confirmatory factor analyses, correlational analyses, and tests of measurement invariance were performed.
Results
The two-factorial model reached a good model fit. The sub-scales information seeking and information appraisal, as well as the eHealth literacy total score, reached high reliability coefficients. Construct and criterion validity was fully confirmed For the two-factorial model, measurement invariance up to the scalar level could be confirmed regarding the sociodemographic characteristics sex, age, and educational level.
Conclusions
This study confirmed the two-factor structure, construct, and criterion validity as well as measurement invariance at the scalar level for sex, age, and educational level of the GR-eHEALS scale in a sample of individuals with CAD and CHF.
Keywords
Introduction
Health literacy has been defined as a Sustainable Development Goal by the World Health Organization (WHO). 1 Nutbeam 2 defines health literacy as ‘a person's ability to access, understand and use health information in ways that promote and maintain good health’. Health literacy is associated with a number of important health outcomes: Low health literacy has been connected to more hospitalizations, more frequent use of emergency care, poorer adherence towards medication use, better health understanding, better health-related self-management behaviours, and poorer health status.3–5 Today, knowledge about health-related topics is no longer only conveyed by experts. The internet offers a nearly unmanageable amount of possibilities to access (health) information. 6 Problems occur when the presented information is not fact-based or even harmful to health. 7 This makes the concept of electronic health literacy (eHealth literacy) all the more critical. The overarching concept of eHealth describes healthcare based on information and communication technology, e.g., telemedicine, mobile health (mHealth), and health informatics. 8 To conclude, eHealth literacy adapts the concept of health literacy to the age of digital media and is defined as the ‘ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to addressing or solving a health problem’. 9
Several studies have shown positive relations between eHealth literacy and health-related outcomes in the general population and clinical populations, such as health knowledge,10,11 health information seeking,12,13 health intention, 14 preventive health behaviour,11,15 and adherence. 16 Moreover, beneficial health behaviours, such as following a healthy diet and regularly exercising, are positively associated with eHealth literacy.17,18
(e)Health literacy in individuals with cardiac diseases
The WHO names cardiovascular diseases (CVDs), in particular cardiac diseases (CDs), as ‘the leading cause of death globally’, resulting in 17.9 million death per year. 19 CDs are a group of diseases encompassing several diseases, e.g., coronary artery disease (CAD), congestive heart failure (CHF), and rheumatic heart disease, resulting in heart attacks and strokes. 19 Due to risk factors, such as diet, immobility, and alcohol or tobacco, many CDs are considered ‘lifestyle disorders’.20,21
For the context of health literacy among individuals at risk of and affected by coronary heart disease, it could already be shown that low health literacy is associated with negative health behaviours and outcomes, such as feeling less equipped to implement necessary lifestyle changes, lack of proactive coping strategies, denial of CAD, more rapid physical deterioration, and less use of healthcare services compared to individuals with higher health literacy. 22 Further, sociodemographic factors such as older age, unemployment, low level of education, and low socioeconomic status are related to low health literacy in this group of patients. 22 Low health literacy in those affected by CDs has further been connected to decreased quality of life. 23
Targeted eHealth interventions for individuals with several CDs can potentially affect a number of risk factors and health outcomes positively.24–26 However, it is important to understand that adequate eHealth literacy is a significant skill in this context. In order to successfully use these services or even find these support approaches, eHealth literacy plays a key role.
In a German sample of patients with CD, diabetes, or both, eHealth literacy was related to the use of mHealth apps and the higher perceived effectiveness of such apps. 27 Richtering et al. 28 investigated eHealth literacy in individuals with moderate to high cardiovascular risk. However, the authors note that the assessment instrument used was unable to depict mean to high levels of eHealth literacy and suggest a revision of existing measurement scales. Cardiovascular risk and health-related behaviours and their association with eHealth literacy have been investigated among patients with hypertension, diabetes mellitus, and coronary heart disease. Low eHealth literacy was associated with cardiovascular risk. 29 The aforementioned relations between eHealth literacy and several health-related outcomes in patients with CDs, as well as the need for a validated instrument, have highlighted the relevance of a reliable assessment of eHealth literacy in a number of diverse populations.
As there is no study examining the validity of the measurement of eHealth literacy in people with CDs, there is a gap in understanding the assessment of eHealth literacy which is a crucial requirement in developing specific eHealth interventions for people suffering from CDs. The recently published German revised version of the eHealth literacy scale (GR-eHEALS) is a valid and reliable assessment instrument for measuring eHealth literacy in the German language. 30 Measurement invariance of the instrument, which is necessary to determine whether an interpretation of mean differences is considered valid,31,32 was confirmed for sex and educational level. This is highly relevant as different sociodemographic variables have been shown to be connected to eHealth literacy: similar to health literacy, older people and those with lower levels of education exhibit poor eHealth literacy. 33 In contrast, studies examining the association between eHealth literacy and sex showed contradictory findings.11,18,34 Therefore, the independence of the measurement instrument from sociodemographic variables is crucial for evaluating its psychometric quality. However, the GR-eHEALS was only validated on a sample from the general population in Germany. Moreover, the investigation of its validity in clinical samples is missing so far.
Objectives
eHealth literacy is an important ability for patients and the basis of the successful use of eHealth services. Measurement of this construct needs to be reliable for studies investigating eHealth literacy and the programme's efficacy in increasing this ability in patients with low eHealth literacy. Further, measurement invariance is required to interpret mean differences regarding sociodemographic determinants validly.
Therefore, three objectives were developed for this study:
We wanted to examine the factorial structure of the GR-eHEALS. Further, the construct validity should be assessed by investigating the convergent and discriminant validity of the instrument in individuals with CDs. To investigate the GR-eHEALS’ criterion validity, the associations of eHealth literacy and health-related outcomes in individuals with a CD should be considered. Further, the goal was to examine measurement invariance for sex, age, and educational level of the GR-eHEALS in individuals with a CD.
Methods
Study design and participants
A cross-sectional study design was applied. Data collection was conducted via an online survey on the platform Unipark 35 from November 2021 to December 2022. Recruitment of patients took place at the Department of Cardiology, West German Heart and Vascular Center, University Hospital Essen, and social media channels that focus on CDs. Eligibility requirements for participation in the study consisted of a diagnosis of a CD (at least one of the following: CHF or CAD), age above 18 years, sufficient command of the German language, and internet access. Electronic informed consent was obtained before the beginning of the survey. Participation was anonymous and voluntary. Compensation for participation was not offered. In order to improve the data's quality, we performed an outlier analysis regarding the completion time of the questionnaire and detected 12 cases with extremely slow completion times, which were excluded. N = 455 patients were included in the final data analysis. The sample size for this study was determined based on recommendations for factor analyses and validation studies.36,37 The study was conducted in accordance with the Declaration of Helsinki, and the Ethics Committee of the Essen Medical Faculty (19-89-47-BO) agreed to conduct the study.
Measurements
Sociodemographic and medical characteristics were collected. eHealth literacy and constructs to examine convergent, discriminant, and criterion validity were assessed via self-assessment measurement instruments.
Sociodemographic data were assessed, including sex, age, marital status, level of education, occupation, and city size. Medical data were assessed, including, e.g., patients’ smoking behaviour.
eHealth literacy is assessed with the GR-eHEALS, 30 which is based on the eHEALS by Norman and Skinner. 38 The GR-eHEALS consists of eight items. All items are rated on a five-point Likert scale. The validity and factorial structure of GR-eHEALS were confirmed by exploratory and confirmatory factor analyses in a German convenient sample before. 30
To examine the convergent validity, we used established scales to measure digital confidence, 30 knowledge of internet-based health promotion programmes,30,39,40 and a single item to assess the duration of private internet use. In accordance with Campbell and Fiske, 41 we expected significant interrelations with the GR-eHEALS to confirm convergent validity.
Regarding discriminant validity, the eight-item impulsive behaviour scale (I-8) 42 was used to measure impulsivity as a personal trait which we expected to be independent of the GR-eHEALS (eHealth literacy). These items were assessed via five-point Likert scales.
To evaluate the criterion validity of the GR-eHEALS in the form of concurrent validity, we assessed the health status (physical and mental health) as well as the quality of life with self-developed single items on 11-point Likert scales. Further, we asked whether people were smoking or not via a single dichotomous item.
Statistical analyses
Data analysis was performed using R 43 and RStudio. 44 Confirmatory factor analysis (CFA) was conducted to investigate the factorial structure of the scale. Prior to this, an exploratory factor analysis (EFA) was conducted, with results presented in Appendix 1. Hu and Bentler 45 suggest a comparative fit index (CFI) and Tucker–Lewis index (TLI) of about 0.95 and root mean square error of approximation (RMSEA) and standardized root mean square residual (SRMR) of about 0.06 and 0.08, respectively, to confirm the fit of the model. A robust likelihood estimator (ULSM: ULS = unweighted least squares, M = mean adjusted test statistic) was used to ensure a model with fewer biases 46 and consider the ordinal-scaled level of items of the instrument. 47 Interrelations of the GR-eHEALS with convergent, discriminant, and criterion validity scales, as well as sociodemographic variables, were examined with two-tailed Pearson correlations, t-tests, and analyses of variances (ANOVA) considering significance levels of α = 0.05. Before using the scales for convergent, discriminant, and criterion validity, their reliabilities (internal consistency) were investigated. Missing values were deleted listwise. Further, measurement invariances of sex, age, and educational level of the GR-eHEALS were analysed. For this purpose, we conducted consecutive multi-group CFA and considered the scalar invariance to verify measurement invariance. 48 In the CFA and tests of measurement invariance, data of N = 315 patients with complete data on eHealth literacy variables were considered. When scalar invariance is confirmed, the interpretation of mean differences is considered valid. 31 Otherwise, differences between groups of the respective sociodemographic characteristic may be attributable to the instrument's lack of ability to measure equally between different groups. Model fit indices and difference of CFI (ΔCFI) between compared models were examined. A cutoff criterion of a difference of CFI of 0.01 was applied, indicating invariance between the two models. 49 As measurement invariance testing requires sufficient large group samples, we excluded one person who indicated sex as ‘diverse’. Moreover, we dummy-coded the age via the median split-half procedure. To test measurement invariance for educational level, we excluded persons who indicated having no school certificate (n = 2) and who indicated ‘Other’ or ‘Not specified’ (n = 18) and aggregated people with any school degree as Group 1 and people with a university or academic degree as Group 2.
Results
Sample description
Table 1 shows the sample characteristics of the study. Further, the table includes the sample characteristics of the 315 participants, who completed all items of the GR-eHEALS. Out of N = 455 people who indicated to be diagnosed with a CD, n = 153 (34%) reported to have had myocardial infarction in the past. A total of 196 (43%) indicated having a diagnosed CHF, and 193 (42%) indicated to previously undergone bypass surgery or percutaneous coronary intervention.
Description of the study sample.
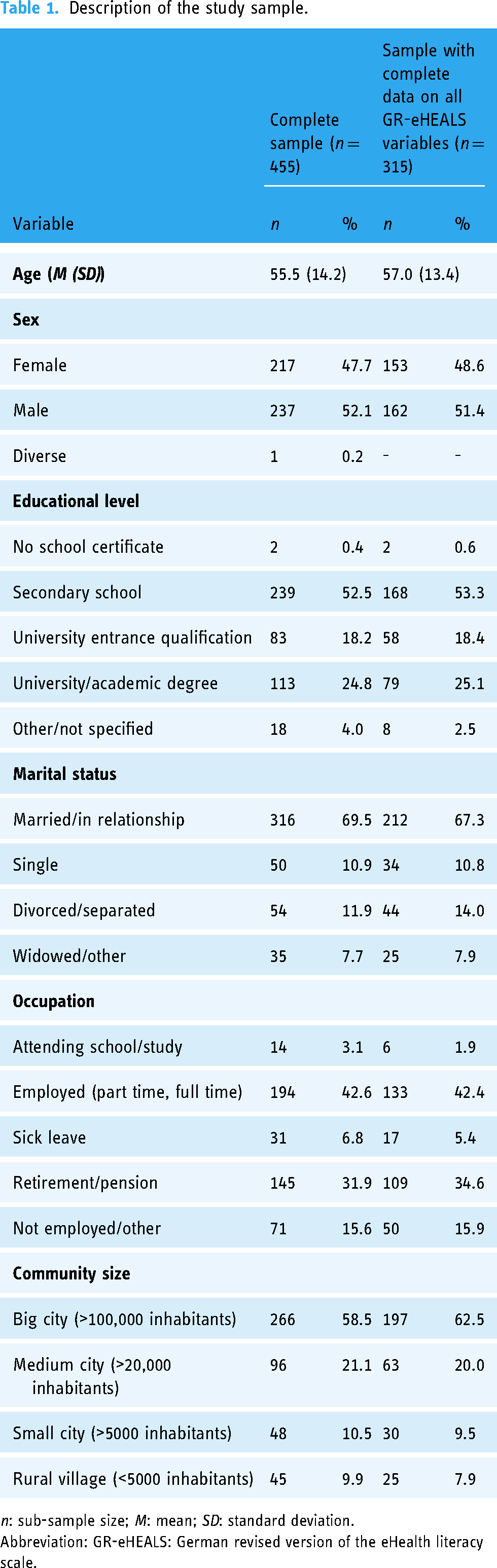
n: sub-sample size; M: mean; SD: standard deviation.
Abbreviation: GR-eHEALS: German revised version of the eHealth literacy scale.
Properties of scales used for construct validation
Three items assessing digital confidence reached excellent internal consistency of 0.94. Good internal consistency (0.87) was reached for three items measuring knowledge of internet-based health promotion programmes. Regarding impulsivity, four of the eight items of the I-8 scale were excluded due to low item discriminations indices and diminishing internal consistency. After item exclusion, good internal consistency of 0.78 was reached.
Construct validation of the GR-eHEALS in people with CD
We conducted a CFA to evaluate the factorial structure of the GR-eHEALS in the population of individuals affected by CD. In the first model, we performed a model test to evaluate the model fit of a one-factorial model. In the second model, the two-factorial structure reflecting two interrelated sub-dimensions of information seeking and information appraisal proposed by Marsall et al. 30 was tested. The results of these analyses are presented in Table 2.
Results of CFA to examine factorial structure of the GR-eHEALS.

Chi²: Chi²-coefficient; df: degrees of freedom; CFA: confirmatory factor analysis; CFI: comparative fit index; GR-eHEALS: German revised version of the eHealth literacy scale; TLI: Tucker–Lewis index; RMSEA: root mean square error of approximation; SRMR: standardized root mean square residual.
As shown in Table 2, the two-factor model reached a better model fit and replicated the findings of Marsall et al. 30 All item factor loadings were greater than 0.76. The items, as well as their descriptive characteristics, are shown in Table 3. All items had a median of 4 and were slightly negatively skewed. The two sub-dimension information seeking (Items # 1–4) and information appraisal (Items # 5–8) reached excellent internal consistencies of 0.92 and 0.91, respectively. Internal consistency of all eight items (eHealth literacy total score) was excellent, with Cronbach's alpha of 0.94.
Item statistics of the GR-eHEALS in the study population.
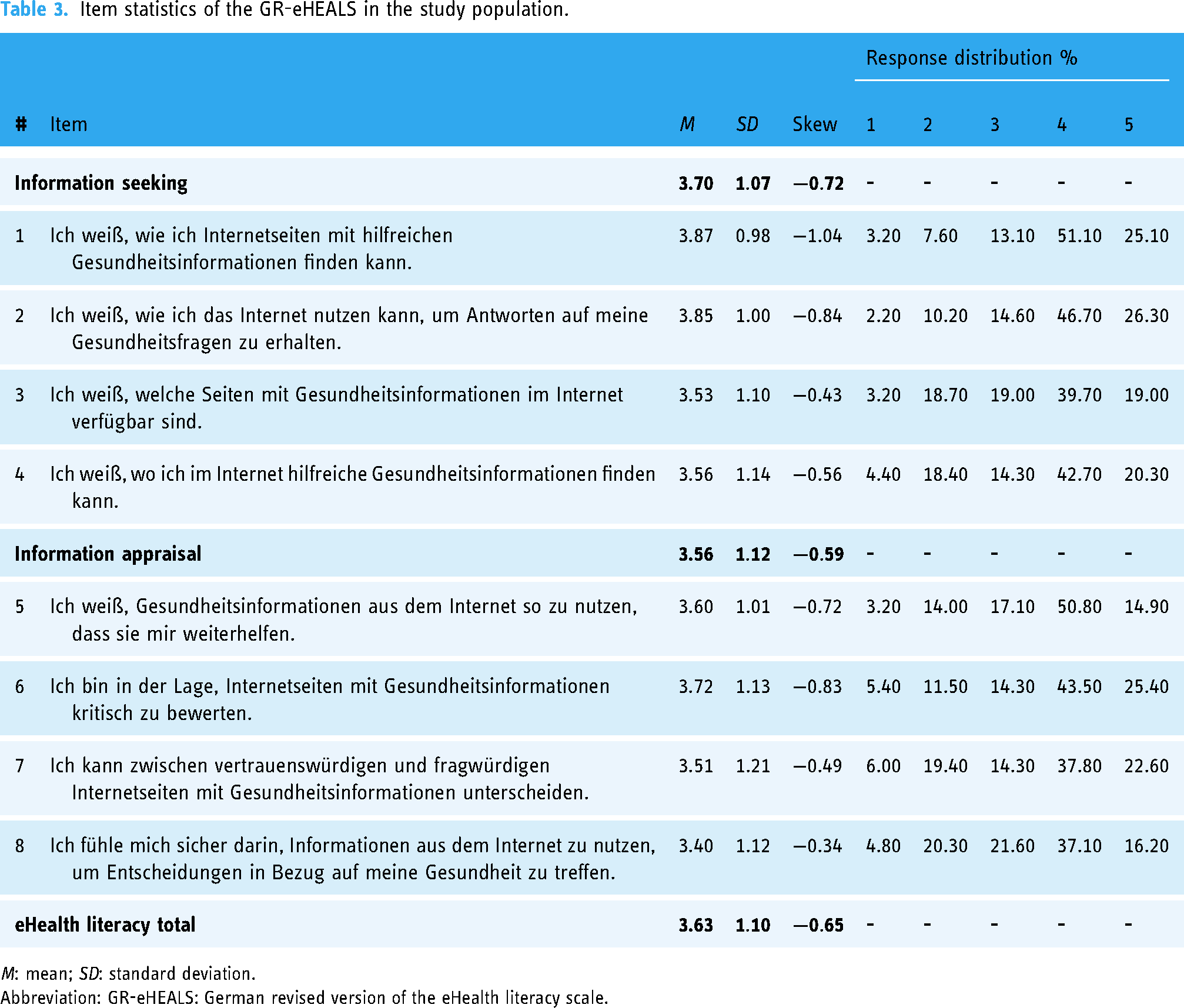
M: mean; SD: standard deviation.
Abbreviation: GR-eHEALS: German revised version of the eHealth literacy scale.
With regard to sociodemographic variables, the GR-eHEALS sub-dimensions information seeking and information appraisal were significantly related to age (r = −0.16 and −0.19, respectively). Moreover, higher educational degrees were related to higher scores of information seeking (F4,310 = 5.92, p < 0.001) and information appraisal (F4,310 = 6.50, p < 0.001) with post hoc tests indicating that both sub-scales were significantly higher in patients holding a universities/academic degree compared to patients with secondary school certificate. Further, information seeking and information appraisal differed regarding patients’ marital status (F3,311 = 7.83, p < 0.001, and F3,311 = 7.28, p < 0.001, respectively) and the community size they lived in (F3,311 = 6.12, p < 0.001, and F3,311 = 9.59, p < 0.001, respectively).
Regarding convergent and discriminant validity of the GR-eHEALS, Table 4 shows the interrelations of its two sub-dimensions as well as with the eHealth literacy total mean score with digital confidence, knowledge of internet-based health promotion programmes, and duration of private internet use (convergent validity scales) as well as impulsivity (discriminant validity scale).
Pearson correlations of the GR-eHEALS sub-dimension and the eHealth literacy total mean score with convergent and discriminant validity scales.

***p < .001.
Abbreviation: GR-eHEALS: German revised version of the eHealth literacy scale.
The results in Table 4 show that the three convergent validity scales were significantly positively related to the two eHealth literacy sub-scales information seeking and information appraisal, as well as the eHealth literacy total mean score. With regard to the discriminant validity scale, no significant relationships were found.
Criterion validity of the GR-eHEALS in people with CD
In order to examine the interrelations between eHealth literacy and health-related outcomes, correlational analyses of the GR-eHEALS sub-dimension information seeking and information appraisal as well as the eHealth literacy total mean score with health status (physical and mental health), quality of life, and smoking behaviour were conducted. The results are reported in Table 5.
Pearson correlations of the GR-eHEALS sub-dimension with criterion validity scales.

anot smoking vs. smoking.
***p < .001.
Abbreviation: GR-eHEALS: German revised version of the eHealth literacy scale.
As shown in Table 5, all criterion validity scales were significantly related to information seeking and information appraisal and eHealth literacy total mean score. Physical and mental health and quality of life were significantly higher in people with higher eHealth literacy. Further, non-smokers reported higher eHealth literacy than smokers.
Measurement invariance of the GR-eHEALS in people with CD
In order to investigate the measurement invariance of the two-factor GR-eHEALS model regarding the sociodemographic variables, sex, age, and educational level, multi-group CFA was conducted. Results of the multi-group CFA are presented in Table 6.
Results of multi-group CFA regarding sex, age, and educational level.

Chi²: Chi²-coefficient; df: degrees of freedom; CFI: comparative fit index; TLI: Tucker–Lewis index; RMSEA: root mean square error of approximation; SRMR: standardized root mean square residual.
As shown in Table 6, model fit indices for each sociodemographic variable performed slightly worse over the increasingly restrictive models of measurement invariance. Nevertheless, good model fits were found, while there was nearly no deterioration in the CFI over the increasingly restrictive models of measurement invariance. Therefore, measurement invariance up to the scalar level could be confirmed for the GR-eHEALS model regarding the sociodemographic characteristics: sex, age, and educational level.
Discussion
The aims of this study were to critically evaluate the validity of the GR-eHEALS, including the test of its measurement invariance, in people affected by CDs. The results corroborate that the GR-eHEALS is a valid and reliable instrument for measuring eHealth literacy in this clinical cohort. The two-factor model, construct, and criterion validity could be confirmed. Furthermore, measurement invariance regarding patients’ sex, age, and educational level up to the scalar level could also be confirmed.
Besides good model fit indices of the two-factor model, correlational analysis underpinned convergent and discriminant validity, confirming the instrument's overall construct validity. Regarding the convergent validity, the results showed that people with higher eHealth literacy were more confident in using digital media and had more knowledge regarding internet-based health promotion programmes. Furthermore, it was found that there was a positive relation between eHealth literacy and the duration of private internet use. This relationship has already been observed for health literacy: previous research found that low health literacy was associated with less internet use. 50 One possible explanation could be that diverse online experiences enable users to interact more competently with the information provided on the internet. At the same time, competent internet users may feel more at ease online and therefore report more frequent internet use. Summarizing these results, eHealth literacy was related to other cognitive and behavioural constructs regarding the use of digital media and the internet in terms of health-related questions, which provides clear evidence for the convergent validity of the GR-eHEALS. Referring to the examination of discriminant validity, no or just a weak relation between the GR-eHEALS with patients’ impulsivity was expected, which was confirmed by the performed analyses.
Moreover, we looked at possible health-related and behavioural outcomes to examine the criterion validity and found that people with higher eHealth literacy reported better physical and mental health statuses. This relationship was also true for patients’ quality of life. On the behavioural level, our results provide evidence that people with higher eHealth literacy are less likely to smoke cigarettes. This result is especially important in the context of people who are already affected by CDs.
In another step of our analyses, we wanted to investigate whether the GR-eHEALS is an equally valid instrument for measuring eHealth literacy in female and male persons in different age groups as well as different levels of patients’ educational background. Our results underline previously published results of the measurement invariance of the GR-eHEALS regarding sex and educational level. 30 In addition, measurement invariance regarding age could be confirmed in this study. To sum up, measurement invariance could be confirmed, which is a highly important prerequisite for the valid use of the instrument in the study of sociodemographic differences.
eHealth literacy is a critical construct that has been linked to various health-related outcomes and behaviours.10–12,14,15,17,18 Furthermore, it is the basis for the effective use of eHealth services. In the context of people being affected by CDs, eHealth literacy makes it possible to empower those patients by granting anonymity and providing convenient, flexible access to basic and advanced information about health-related topics and eHealth services. 51 However, this new form of healthcare may also further divides groups of patients into those with high and low eHealth literacy. 51 Since it has been established that barriers to accessing eHealth services include readability and availability of information and poor usability, there is a high demand for adapted and valid health literacy screening instruments. 50 In the long term, low eHealth literacy could mean that the usefulness of eHealth interventions is low among these individuals, or worse, that newly developed eHealth services do not reach these people at all. These findings are highly relevant for individuals affected by CDs. Only through valid measurement of eHealth literacy, it will be possible to develop interventions to increase eHealth literacy and close the gap of access to health information. 33
Based on these findings, eHealth literacy and its assessment should be utilized to promote positive health behaviours. Dedicated programmes to increase eHealth literacy could be beneficial to patients with CDs and positively impact their health-related outcomes.52,53 This is especially important in the area of eHealth interventions, as lack of eHealth literacy is a key barrier to the use and success of digital health programmes. 54 In this way, people with low eHealth literacy could be specially identified, so that adapted approaches to access digital services would be feasible. Furthermore, this study offers the opportunity to use the GR-eHEALS as a tool to assess the efficacy of interventions to foster eHealth literacy in the population of patients with CDs.
Limitations
When interpreting the present study's results, limitations must be considered. A limitation of the study is that eHealth literacy was only measured through self-assessment. This construct is meant to assess skills and competencies, so it would be more accurate to compare it with actual behaviours or use behaviour-based measurement methods. However, to our knowledge, there is no such tool. Furthermore, an easy-to-use tool is essential to be integrated with the clinical routine. The data collected in this study were cross-sectional, so while it can show relationships, it cannot be used to make causal inferences. Additionally, the survey was conducted online, which may have resulted in a sample that is more representative of individuals who are comfortable using the internet and digital devices and may not accurately reflect the views of those who are less familiar with the web. However, a representative study demonstrated that internet use in Germany reached 91% in 2021 and is further increasing. 55 The study sample is younger than the general population of individuals affected by CAD and CHF. 56 Moreover, the gender ratio of the participants is more balanced and does not reflect the overrepresentation of men affected by CDs. Further, a high number of participants (30.7%, n = 140) could not be included into the CFA and test for measurement invariance due to missing data on the GR-eHEALS items. Therefore, the possibility of selection bias should be considered.
Conclusion
eHealth literacy represents an important ability for people with CDs to find and understand health information on the internet. Furthermore, it is the basis of the successful use of eHealth services. This study confirmed the two-factor structure, construct, and criterion validity of the GR-eHEALS in a sample of people with CDs. Furthermore, measurement invariance up to the scalar level could be confirmed for the GR-eHEALS regarding sex, age, and educational level. To conclude, the GR-eHEALS can be used to assess associations between eHealth literacy and health-related outcomes in individuals with CDs.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231194915 - Supplemental material for Psychometric properties of the German revised version of the eHealth literacy scale in individuals with cardiac diseases: Validation and test of measurement invariance
Supplemental material, sj-docx-1-dhj-10.1177_20552076231194915 for Psychometric properties of the German revised version of the eHealth literacy scale in individuals with cardiac diseases: Validation and test of measurement invariance by Alexander Bäuerle, Matthias Marsall, Lisa Maria Jahre, Christos Rammos, Charlotta Mallien, Eva-Maria Skoda, Tienush Rassaf, Julia Lortz and Martin Teufel in DIGITAL HEALTH
Footnotes
Acknowledgements
We acknowledge Anna-Lena Frewer (Clinic for Psychosomatic Medicine and Psychotherapy, University of Duisburg-Essen, LVR-University Hospital Essen, 45147 Essen, Germany) for revising the final manuscript draft.
Contributorship
AB, MM, and MT conceptualized the study. Project administration was performed by AB, LJ, JL, and CM. Statistical analyses were conducted by MM. AB and MM interpreted the data. AB, LJ, JL, and MM wrote the original draft of the manuscript. MT, E-MS, CR, and TR supervised the project and contributed to the study design, data collection, and critical revision of the manuscript. All authors reviewed and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and the Ethics Committee of the Essen Medical Faculty (19-89-47-BO).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication is supported by the Open Access Publication Fund of the University of Duisburg-Essen.
Guarantor
AB.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.