
Abstract
Background
Enhancing oral health-related quality of life requires oral health knowledge. Mobile healthcare increases assistance and healthcare through mobile devices and wireless technologies. Using information and technology, eHealth enhances healthcare services by enabling digital administration and improving data interchange and coordination among providers, but its influence on oral health knowledge and practice is unclear. Therefore, the present article will examine how mHealth and eHealth could improve oral health knowledge and practices.
Methods
Original research on the function of mHealth and eHealth in enhancing oral health literacy was identified through searches of PubMed, Cumulative Index to Nursing and Allied Health Literature, ScienceDirect, IEEE Xplore, Dimensions, and the Cochrane Library. The potential articles were selected based on modified Patient/Problem, Intervention, Comparison, Outcome, Study criteria. The risk of bias in suitable studies was evaluated using the risk of bias visualization tool (Robvis 2.0) and the risk of bias in non-randomized studies with intervention.
Results
The database search generated 2197 entries, of which 13 publications were used in this analysis. Narrative synthesis revealed that mHealth and eHealth interventions consistently improved oral health knowledge and practices across diverse populations, including caregivers, elderly adults, and dental students. Short message service (SMS)-based interventions enhanced mothers’ knowledge and practices related to children's oral health, while virtual reality technologies improved learning outcomes for dental professionals and students compared to traditional methods. However, improvements in knowledge did not consistently translate to sustained behavior changes, with variations in practice outcomes across studies due to differences in measurement tools and intervention designs. These findings suggest that while digital interventions enhance knowledge, their impact on long-term behavior requires further exploration.
Conclusion
Mobile apps, SMS-based therapies, and virtual reality applications greatly improved oral health knowledge, habits, and literacy scores across different age groups.
Introduction
Oral health literacy is essential in improving oral health-related quality of life by understanding basic oral health information and influencing choices regarding dental treatments.1–3 According to the World Health Organization, oral health literacy is defined as the degree to which individuals can obtain, process, understand, and use oral health information to make informed decisions and take actions to improve their oral health. This concept applies primarily to the general population, including patients and caregivers, and is distinct from the professional knowledge and clinical skills acquired by dental students and practitioners through specialized education and training. While oral health literacy empowers individuals to manage their own oral health, professional knowledge encompasses academic understanding and clinical competencies required for dental practice. Promoting good hygiene behaviors, including regular brushing, and the importance of regular dental examinations, is essential.4,5 Moreover, oral health literacy assists in the early identification of oral problems, thereby reducing severe dental problems in the future.6,7 In addition, it improves communication between patients and dental practitioners, ensuring that patients understand the treatment plans and follow recommendations for optimal results. 8
Mobile health uses mobile devices and wireless technology to improve health care and services. 9 It covers many applications, such as mobile applications for health monitoring, educational resources on oral hygiene, advice on nutrition, and the importance of regular dental visits, allowing individuals to make informed choices regarding their oral health, remote patient consultations, and chronic disease management.10,11 Moreover, mHealth improves diagnosis, treatment, and monitoring by allowing the collection of real-time patient data. This significantly improves access to healthcare services in remote regions.12,13 In addition, this technology helps patients adhere to treatment, health tracking, and promotes patient engagement.14,15 Moreover, mHealth enhances public health initiatives through data collection and disease surveillance. 16
On the other hand, eHealth uses information and technology to enhance healthcare services by enabling digital management, hence, better data sharing and coordination among healthcare caregivers. 17 These include electronic health records, telemedicine, health information systems, and online health resources.18, 19 eHealth tools such as patient portals and mobile apps help individuals manage their health by accessing medical records, scheduling appointments, and communicating efficiently with providers online.20, 21 In addition, eHealth enhances healthcare by providing better healthcare by reducing costs and making it accessible to people in remote areas. 22
Mobile and electronic health are critical for improving oral health literacy by using technology to provide comprehensive information. Their incorporation into oral health routines is essential for minimizing the rise in oral health-related issues and associated economic burdens. Despite the advanced technologies in dental care, there are still many oral health-related issues in underserved areas due to limited access to accurate oral health information. Limited access to oral health information disproportionately affects vulnerable populations, including low-income communities, racial and ethnic minorities, rural residents, and elderly individuals, due to socioeconomic barriers, geographic isolation, and digital divides. mHealth and eHealth solutions would benefit rural communities by overcoming distance barriers, working individuals through convenience, people with mobility limitations, technology-savvy young adults, linguistic minorities through multilingual applications, and low-literacy populations via visual and audio content. These digital platforms can potentially democratize oral health knowledge by providing accessible, personalized information that addresses the specific barriers underserved populations face. This study critically appraises evidence of the role of mHealth and eHealth in enhancing oral health literacy.
Research objectives
The main goal of this study was to explore the impact of mHealth and eHealth on improving oral health knowledge and practices through a systematic evaluation of original research papers published in scholarly journals.
Research question
How do eHealth platforms influence patient-provider communication and access to oral health information to enhance knowledge and practices?
How do mHealth interventions affect oral health knowledge and preventive behaviors?
Methodology
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). 23 The protocol for this systematic review was registered with the International Platform for Systematic Review and meta-analysis (INPLASY202510073).
Identification and selection of studies
A review author (MK) performed a thorough search of electronic databases via PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), ScienceDirect, IEEE Xplore, dimensions, and Cochrane Library. This search aimed to locate original research on the role of mHealth and eHealth in improving oral health literacy published from inception to 6 July 2024, when the search was conducted.
Search strategy
A review author (MK) conducted a preliminary search to identify relevant keywords related to eHealth, mHealth, oral health, and literacy. The following keywords were used in different combinations to optimize the search in different databases: mHealth, eHealth, mobile health, electronic health, text messages, mobile applications, digital health, tele dentistry, virtual reality, artificial intelligence, wearable devices, mobile apps, smartphones, oral health, dentistry, literacy, and education. A comprehensive search was then conducted via the databases. Filters were used to restrict the search to phase I, II, III, and IV clinical trials, comparative evaluations, multicenter studies, validation studies, twin studies, observational studies, and randomized controlled trials in PubMed.
Screening and study selection
A two-reviewer approach was employed for the screening and selection process. Search results were exported to Zotero screening software (version 6.0.36), which detected duplicate entries by comparing the metadata. A reviewer (MK) manually merged the duplicates. Two reviewers (SC and SV) then independently screened the remaining non-duplicate records based on predefined eligibility criteria. Conflicts were resolved through discussion until consensus was reached or the intervention of a third reviewer (MC), whenever necessary.
Eligibility criteria
This study included research on the role of mHealth and eHealth in enhancing oral health literacy. Articles that fulfilled the modified PICOS criteria were selected (Table 1). 24 In addition, the studies are given in Table 1.
PICO criteria for eligible studies.

Exclusion criteria
Studies that investigated mobile and electronic health components unrelated to their influence on oral health literacy were barred from inclusion. In addition, materials such as editorials, letters, reviews, meta-analyses, research protocols, opinions, or conference abstracts were excluded. On the other hand, non-English publications and articles without full texts were excluded from this study.
Methodological quality assessment
To evaluate the quality of the studies eligible for inclusion, two review authors (MK and SC) independently used the risk of bias visualization tool (Robvis 2.0) and the risk of bias in non-randomized studies with intervention (ROBINS-I). 25 Conflicting results were resolved through discussion or the intervention of a third reviewer (MC) whenever necessary.
Data selection and extraction
A reviewer (MK) prepared a data extraction template defining the variables of interest. A second reviewer (SC piloted the data extraction template to test its reliability in extracting relevant data from the included studies. The reviewer (MC) then systematically extracted and tabulated the data using Microsoft Excel software version 2021. Based on the studies considered, the following datasets were retrieved methodically: authors, study design, locations, duration/period, purpose, results, sample size, characteristics, mean age/age range, outcome measures, and the eHealth or mHealth intervention that was used. The extracted data were tabulated in an Excel workbook using Microsoft Excel 2019.
Data analysis
The extracted data were then analyzed and reported thematically. 26 Due to the heterogeneity in outcome measures (e.g. knowledge scores and practice scores) and the focus on constructs related to but distinct from oral health literacy, a narrative synthesis was conducted to summarize the effects of mHealth and eHealth interventions. This approach facilitated a comprehensive exploration of how these interventions influenced oral health knowledge and practices across diverse populations, avoiding inappropriate quantitative pooling given the variability in study designs, measurement tools, and conceptual focus.
Quantitative data were analyzed using Review Manager software version 5.4.1. An intervention review was conducted using a full review approach. Moreover, a random effects analysis model, inverse variance statistical method, and standard mean difference effect measure were used with continuous data.
Results
Study selection
The literature search generated 2197 articles. No records were automatically removed. Merging them using Zotero software version 6.0.36 eliminated 402 duplicates. Additionally, 1692 items were eliminated after filtering the titles and abstracts. After reviewing the remaining 104 papers, 13 studies that satisfied the inclusion criteria were added. The findings are presented in Figure 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram. 23
Methodological quality assessment results
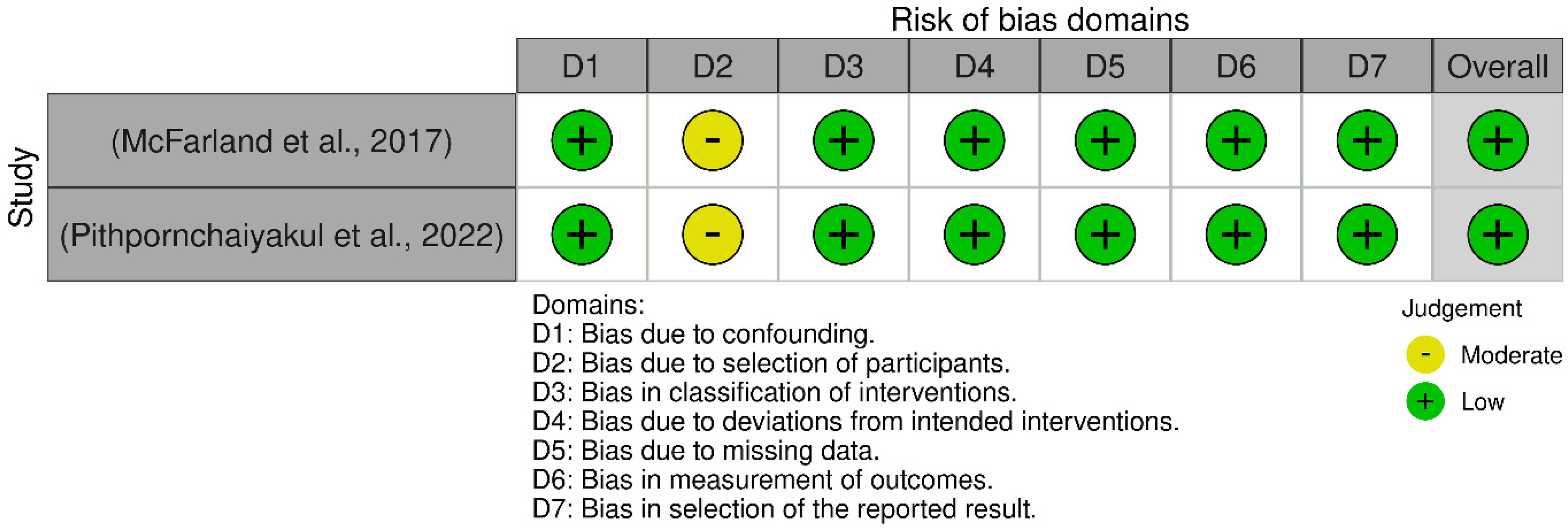
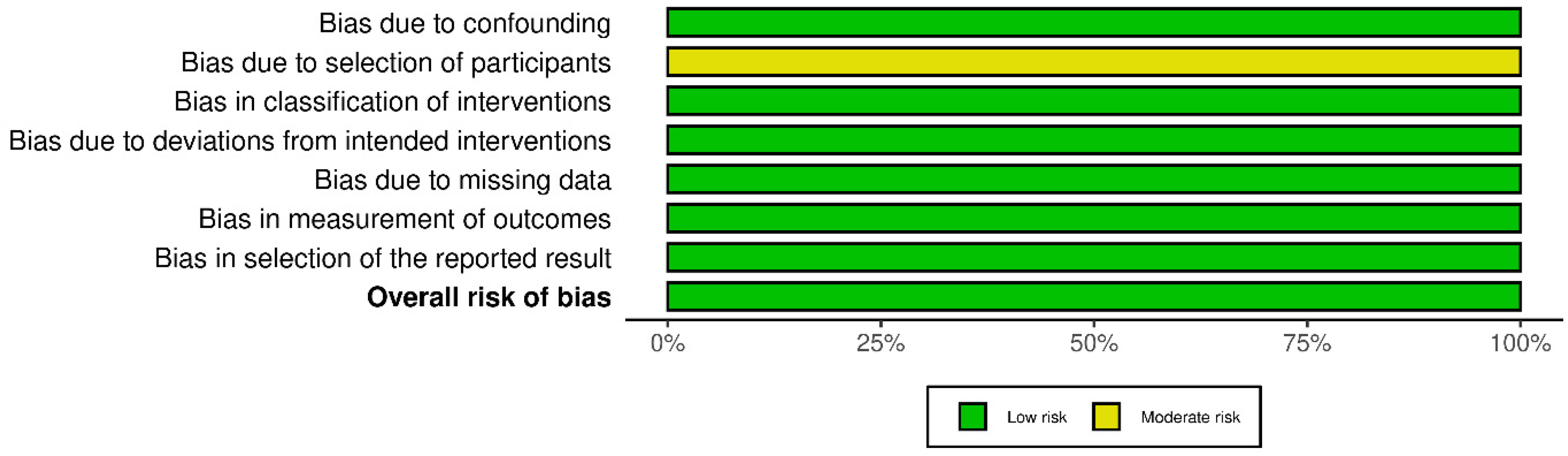
The included studies showed low risk of bias across the assessed domains. Figures 2 to 5 show the included studies’ Robvis 2.0 and ROBINS-I quality assessments.


Study characteristics
Six studies investigated mHealth and eHealth in the general population, all conducted in Asian countries (Iran, Korea, Thailand, and Malaysia) between 2016 and 2022. Five studies focused on mobile health (mHealth) interventions, including smartphone applications,30,34,37 SMS-based programs, 29 and a progressive web application. 36 Only one study 39 employed an electronic health (eHealth) approach through a chatbot program. These studies predominantly targeted caregivers. The remaining studies addressed elderly adults 30 and patients using removable partial dentures. 36 Most investigations employed randomized controlled trial designs with intervention periods ranging from 5 weeks to one full year. Across all studies, researchers consistently measured changes in oral health knowledge, with most also evaluating practical application and clinical outcomes through plaque and gingival indices (Table 2).
Studies investigating mHealth and eHealth in the general population.

Seven studies, conducted between 2017 and 2024, investigated mHealth and eHealth among dental students. Four studies employed virtual reality technology,27,28,31,32 while the remaining studies utilized various digital approaches: teledentistry, 38 mobile learning through a dental surgical forceps application, 33 and virtual learning via a learning management system. 35 One study 31 specifically addressed nursing students, while another 38 included a broader range of participants, including dental students, oral health professionals, and other professionals. The geographical distribution spanned across multiple regions, including Asia (Korea, Taiwan, and Iran), the Middle East (Qatar and Sudan), and North America (the United States).
The outcomes measured varied depending on the specific educational focus, but generally included assessment of knowledge acquisition, skills development, and participant satisfaction or perception of the digital learning tools (Table 3).
Studies investigating mHealth and eHealth among dental students.

Data analysis
Impact on the general population
mHealth on oral health literacy
This section examines the impact of mHealth and eHealth interventions on the knowledge and clinical skills of dental students and professionals, distinct from oral health literacy, which pertains to the general population's ability to use oral health information for decision-making.
Research by Khademian et al. 29 reported that gain frame and loss frame SMS improved mother's knowledge and practices about their children's oral health, with the post-test knowledge scores being 8.83 ± 2.03 in the control group, 11.87 ± 2.17 in the gain frame group, and 12.09 ± 1.94 in the loss frame group. Additionally, there was a significant difference in post-test practice scores between the control group, gain frame and loss frame SMS groups (p < 0.001), with the post-test practice scores being 56.27 ± 11.53, 60.87 ± 7.77, and 60.25 ± 8.96 in the control, gain frame and loss frame groups, respectively.
According to Pithpornchaiyakul et al., 39 there was a significant increase in caregivers’ oral healthcare knowledge with the use of the chatbot application (p < 0.001), exhibiting pre- and post-test knowledge scores of 0.73 ± 0.21 and 0.94 ± 0.09. Similarly, there was a significant increase in caregivers’ oral health care perceptions (p < 0.001), with pre- and post-test perception scores being 0.58 ± 0.19 and 0.86 ± 0.16, respectively.
According to Lee et al., 30 oral health knowledge increased significantly in the smartphone application group (p = 0.013) compared to the control group, exhibiting post-intervention knowledge scores of 38.1 ± 6.1 in the application group and 35.5 ± 7.8 in the control group. Similarly, oral health perception improved significantly in the application use group (p = 0.004), with the application group exhibiting perception scores of 39.0 ± 4.5. On the other hand, oral perception in the control group reduced from the baseline to 34.6 ± 6.2 after the intervention. 30
According to Zolfaghari et al., 37 both the simple application and its gamified version improved the oral health knowledge and practice of mothers, with both groups exhibiting a significant increase in oral health knowledge and practice scores from baseline (p < 0.001) after the intervention. However, the knowledge scores in the gamified application group were higher than those in the simple application group after the intervention, exhibiting scores of 14.3 ± 2 and 13.1 ± 1.6 in the gamified and simple application groups, respectively. Additionally, the practice scores in both groups improved from baseline, exhibiting after-intervention scores of 8.5 ± 1.7 and 8 ± 2.2 in the simple and gamified application groups, respectively.
According to Yi et al., 36 it was observed that both the group that used progressive web applications and the control group saw a noteworthy improvement in their knowledge scores compared to the baseline (p < 0.001). However, after a follow-up period of 3 months, there was no significant difference in knowledge scores between the application and control groups (p = 0.590). The mean knowledge scores for both the application and control groups were 15.08, indicating that there was no significant difference between the two groups.
According to Shirmohammadi et al., 34 the mothers’ knowledge regarding their children's oral health in the application group improved significantly compared to the baseline in the follow-up period (p < 0.001), exhibiting final knowledge scores of 13.5 ± 1.8. On the other hand, in the common training group, the knowledge scores significantly improved compared to the baseline (p < 0.001), exhibiting final knowledge scores of 14.5 ± 1.9. Similarly, practice scores regarding oral health in both the application and control groups improved significantly compared to the baseline (p < 0.001), exhibiting practice scores of 8.5 ± 2.0 and 7.7 ± 2.0 in the application and control groups, respectively.
Narrative synthesis of the included studies indicates that mHealth interventions, such as SMS, mobile applications, and chatbots, consistently improved oral health knowledge among caregivers and the general population. Studies29,30,34,36,37,39 reported significant increases in knowledge scores post-intervention, with improvements ranging from 10% to 30% across different populations. For example, SMS interventions 29 and smartphone applications34,37 led to statistically significant knowledge gains (p < 0.001), with mean score increases of 2–4 points on various scales. However, the translation of knowledge into sustained oral health practices was inconsistent. Studies like Shirmohammadi et al. 34 and Zolfaghari et al. 37 reported significant improvements in practice scores (p < 0.001), with mean increases of 1–4 points, while others, such as Lee et al., 30 noted no significant change in practice outcomes. This variability may be attributed to differences in intervention duration (e.g. 5 weeks to 1 year), measurement scales, and participant characteristics (e.g. caregivers vs. elderly adults). For dental professionals and students, eHealth interventions, particularly virtual reality,27,31,32,35 enhanced knowledge and clinical skills, with studies reporting 10%–15% higher scores compared to traditional methods. The heterogeneity in outcome measures and the short-term focus of most studies limited the ability to draw definitive conclusions about long-term impacts.
Impact of mHealth and eHealth among dental professionals and students
Dental education promotion
The use of dental surgical forceps was found to improve dental students’ academic achievement. 33 The intervention group showed significantly higher scores between the initial and subsequent test results (p < 0.05), whereas the control group showed no difference (p > 0.05). In the control group, the results were 5.87 ± 2.954 and 5.94 ± 2.31 before the test, but in the intervention group, they were 5.94 ± 2.313 and 8.34 ± 2.4839 after the test.
On the other hand, according to Choi et al., 27 the virtual reality enhanced students’ knowledge and comprehension of surgical operations than the control group (p = 0.001). The virtual reality group also had higher mean scores of 4.35 ± 0.745 points. This indicates that the virtual reality group attained a better level of insight into surgical processes. For the control group, on the other hand, the mean score values were 3.35 with a standard deviation of 0.988 points. Additionally, it was observed that the group that used virtual reality had a substantially greater level of learning motivation than the control group (p = 0.015). The virtual reality group demonstrated higher scores of 4.25 ± 0.639 points of learning motivation. In contrast, the group that served as the control had a score range of 3.60 ± 0.883 points.
According to Soltanimehr et al., 35 virtual education improved theoretical knowledge and clinical reporting skills among dental students compared to traditional methods (p < 0.05). The virtual group exhibited theoretical scores of 16.60 ± 0.91. In contrast, the control group exhibited scores of 14.89 ± 0.99. Similarly, the objective structured clinical examination mean scores were higher in the virtual group than the traditional education group, with scores of 15.13 ± 0.78 in the virtual education group and 14.71 ± 0.92 in the traditional education group.
According to Lin et al., 31 over the course of a follow-up period of four weeks, the use of virtual reality-based training on geriatric oral health care resulted in a substantial improvement in the knowledge of nursing students in the experimental group when compared to the control group (p < 0.001). Furthermore, the experimental group had superior knowledge scores, with an average of 8.84 ± 0.85, in comparison to the control group, which had an average of 7.72 ± 0.21. Similarly, according to the same research, it was reported that there was no significant difference in attitude towards geriatric oral health care in both the experimental and control groups (p = 0.279), with attitude scores of 28.92 ± 2.60 and 27.92 ± 3.75 in the experimental and control groups, respectively. Regarding the efficacy of geriatric oral health, it was observed that the experimental group exhibited a high level of effectiveness, as shown by scores of 42.96 ± 4.82. In contrast, the control group exhibited scores of 35.72 ± 6.09 (Lin et al., 2019).
Research 32 reported that mean scores of the neutral zone test in the virtual reality technology teaching group were higher compared to the mean scores of the traditional teaching group, exhibiting mean scores of 16.92 ± 1.12 and 16.14 ± 1.18 in the intervention and control groups, respectively. Additionally, teeth arrangement test scores in the virtual reality technology teaching group were higher than those in the traditional teaching group, exhibiting 16.07 ± 1.07 and 15.65 ± 1.17, respectively.
Acceptance and feasibility of mHealth and eHealth
According to McFarland et al., 38 tele-dentistry training programs positively impact the knowledge and competency of dental students and professionals. This is consistent with 58% of the participants agreeing that competencies gained are identifiable in the syllabus, and 63.4% agreeing that the training was practical and related to their professional work. Additionally, 77.4% of the participants agreed that teledentistry training improved their knowledge of the subject.
The mean rating for the effectiveness of teledentistry training in the gain of competence was significantly different between participants (p < 0.01), with dental hygienists exhibiting the highest mean rating of 4.4, followed by a mean rating of 4 by dentists and a mean rating of 3.5 by both the dental students and other healthcare professionals. 38 In addition, the mean rating of the relevance of teledentistry training to participants’ work was highest by dentists, with a rating of 4.1, followed by a rating of 4.0 by dental hygienists, and a mean rating of 3.6 and 3.4 for dental students and other professionals. Additionally, the improvement in participants’ knowledge differed significantly among participants (p < 0.01), with the highest mean rating of increase in knowledge exhibited by dental hygienists (4.5), followed by dentists (4.1), and other healthcare professionals (4.0).
According to Daud et al., 28 the response to virtual simulation training in improving dental students’ confidence during cavity preparation was 5 ± 41.67 in the virtual simulation training group. In contrast, the responses were in agreement (3 ± 27.27) in the conventional simulation group. Similarly, the response to virtual simulation training being vital in self-training of manual dexterity had an agreement of 8 ± 66.67 and 4 ± 36.36 in both the virtual reality and conventional simulation training.
Users’ satisfaction with eHealth methods
Research by Choi et al. 27 reported that the virtual reality group showed significantly higher satisfaction with the observation of virtual reality than the control group (p = 0.047), with the virtual reality group exhibiting a higher score value of 4.40 ± 0.503 points. In contrast, the control group had a score value of 3.95 ± 0.75 points.
According to Lin et al., 31 there was a higher satisfaction with the virtual reality healthcare learning system among participants in the experimental group, exhibiting satisfaction scores of 79.1 ± 10.36 (range: 57.5–100).
Research by Mansoory et al. 32 reported that the total mean score of students’ satisfaction with virtual reality technology was 41.12 ± 5.65 out of 45, with 76% of dental students showing complete satisfaction with virtual reality technology as an educational tool.
Discussion
This systematic review synthesizes evidence on the impact of mHealth and eHealth interventions on oral health knowledge and practices among the general population (patients and caregivers) and knowledge and clinical skills among dental professionals and students. For the general population, interventions such as SMS, mobile applications, and chatbots significantly improved oral health knowledge, aligning with the WHO definition of oral health literacy as the ability to understand and use information for health decisions. For dental students and professionals, eHealth tools, particularly virtual reality, enhance specialized knowledge and clinical skills, which are distinct from literacy but critical for professional practice. For instance, studies29,30,34,36,37,39 reported 10%–30% improvements in knowledge scores among caregivers and elderly adults, while studies27,31,32,35 showed virtual reality interventions improved knowledge and skills by 10%–15% compared to traditional methods.
These findings align with mHealth studies in other domains, such as diabetes management, where mobile apps improved patient knowledge by 15%–20% (Feroz et al., 2020). However, the translation of knowledge into sustained oral health practices was inconsistent. For instance, studies34,37 reported significant practice improvements (p < 0.001), while others30,36 showed limited or no change. This variability may be attributed to intervention duration—shorter interventions (e.g. 5 weeks by Lee et al., 2023) had less impact on behavior compared to longer ones (e.g. one year by Zolfaghari et al., 2021)—or to psychological factors, such as the use of gain-framed versus loss-framed messaging, which enhanced practice scores in the study. 29
For dental students and professionals, eHealth interventions, particularly virtual reality, significantly improved knowledge and clinical skills, with studies27,31,32,35 reporting 10%–15% higher scores compared to traditional methods. These results mirror findings in medical education, where virtual reality enhanced surgical skills by 12%–18% (Alaker et al., 2016). The immersive, controlled environment of virtual reality likely facilitates skill acquisition by allowing repeated practice without patient risk, explaining its efficacy over conventional training. However, the short-term focus of most studies limits understanding of long-term skill retention, a gap also noted in broader eHealth research (Carini et al., 2021).
The high acceptance and satisfaction with mHealth and eHealth interventions, as reported in studies,27,28,32,38 reflect their accessibility and interactivity, consistent with user perceptions of digital tools in chronic disease management (Tanbeer and Sykes, 2021). However, the predominance of studies from Asia (e.g. Iran and Korea) raises concerns about generalizability to low-resource settings, where digital infrastructure and literacy may be limited. This geographic bias, coupled with heterogeneity in measurement tools (e.g. varied knowledge and practice scales), complicates direct comparisons and underscores the need for standardized outcomes.
The inconsistent impact on practices highlights the complexity of behavior change, which requires not only knowledge but also motivation, environmental support, and sustained engagement. Behavioral theories, such as the Health Belief Model, could explain why SMS interventions with positive framing 29 were more effective in driving practice changes. Future research should incorporate such frameworks to design interventions that address these barriers. Additionally, the short-term nature of most studies (weeks to months) limits insights into sustained outcomes, a limitation also noted in mHealth for maternal health (McCool et al., 2021). Longitudinal studies with follow-up periods of 1–2 years are needed to assess whether knowledge and practice gains persist.
These findings have practical implications. For patients and caregivers, mHealth tools like mobile apps and SMS can enhance access to oral health information, particularly in underserved areas, reducing disparities in care. For practitioners, eHealth platforms offer scalable training solutions, improving clinical efficiency and skills. Policymakers should prioritize integrating these technologies into public health strategies, ensuring equitable access to digital infrastructure. However, limitations, such as small sample sizes in some studies (e.g. 51–73 participants in 34, 30) and the lack of clinical outcome data (e.g. caries incidence), suggest caution in overgeneralizing results. Future research should focus on large-scale, multicenter studies with standardized measures, diverse populations, and long-term clinical endpoints to strengthen the evidence base.
On the other hand, eHealth interventions have also contributed to enhancing dental education through virtual reality technology. A study by Choi et al. 27 reported that virtual reality technology observation improved dental students’ understanding of tooth extraction procedures compared to conventional methods. Similarly, Soltanimehr et al. 35 reported that virtual education contributed to higher theoretical and clinical examination scores than traditional methods. These results demonstrate the effectiveness of immersive technologies in enhancing practical skills and knowledge among dental students. Additionally, virtual reality simulations may provide a safe environment for students to practice procedures before meeting real patients. However, most studies have focused on short-term outcomes, and long-term outcomes require further investigation.
The studies indicated positive acceptance of mHealth and eHealth interventions among users. The study by McFarland et al. 38 reported that tele-density training programs positively impacted medical students’ and professionals’ knowledge, with high agreement rates on the relevance of training. Similarly, Daud et al. 28 found that dental students viewed virtual reality haptic simulation as a vital tool for improving manual dexterity. This acceptance is crucial for implementing these technologies in educational and clinical settings.
High satisfaction rates with eHealth interventions by users have also been reported. According to Choi et al., 27 there were higher levels of satisfaction with virtual reality observation than with conventional methods among dental students. In addition, Mansoory et al. 32 reported that 76% of dental students were completely satisfied with virtual reality technology as an educational tool.
Study implications and recommendations
Patients
These findings reveal significant benefits for patient populations through digital oral health interventions. Mobile applications and SMS-based solutions have demonstrated measurable improvements in patient education outcomes, enhancing daily oral hygiene practices and increasing adherence to professional dental recommendations. The personalized approach offered through mHealth technologies provides patients with comprehensive information systems tailored to their specific needs, substantially increasing their health literacy and awareness of their oral health status. Perhaps most importantly, tele-dentistry services are breaking down geographical barriers, extending quality oral health education and care to those in remote and underserved communities who previously had limited access. These digital approaches effectively reduce healthcare disparities while optimizing treatment outcomes and quality of life for diverse patient populations.
Research
Despite the promising results, the high heterogeneity among existing studies significantly limits the generalizability of findings. To advance this field, research should prioritize designing and conducting large-scale, multicenter studies with standardized outcome measures that enable more robust intervention comparisons. Virtual reality and other immersive eHealth technologies represent promising research avenues, offering unprecedented educational experiences that enhance oral health literacy among students and future practitioners. These innovations open new research areas to investigate optimal educational methodologies for patient populations and healthcare trainees, potentially transforming how oral health knowledge is transmitted and retained.
Practitioners
Integrating eHealth interventions into daily practice demonstrably enhances clinical efficiency, increases patient satisfaction scores, and improves treatment compliance rates. Furthermore, these technologies provide accessible platforms for continuous professional development, allowing practitioners to enhance their knowledge and clinical skills throughout their careers without significant practice disruption. By incorporating digital patient education tools into clinical encounters, practitioners can more effectively communicate complex information, ultimately improving treatment outcomes and the quality of care delivered.
Study strengths and limitations
The research analyzed various digital health interventions (mobile apps, virtual reality, SMS, chatbots, and web applications) separately, allowing for a nuanced understanding of which technologies are most effective for specific purposes and populations.
However, the small sample size in meta-analysis for each outcome analyzed limiting the statistical power and generalizability of the findings. This reflects the still-emerging nature of research in this field. In addition, many included studies were conducted in Iran and East Asia, potentially limiting generalizability to Western healthcare contexts or low-resource settings with different technological infrastructures and cultural factors affecting technology adoption. Moreover, most included studies featured relatively brief intervention periods (weeks to months), limiting the understanding of long-term effectiveness and sustainability of knowledge and behavior changes from digital interventions.
The present study also focused on knowledge, attitudes, and satisfaction rather than long-term clinical oral health outcomes, leaving uncertainty about whether improved literacy translates to meaningful health improvements. On the other hand, the included studies used different measurement tools and scales for assessing knowledge and practice, complicating direct comparisons across studies and potentially influencing the meta-analysis results.
Conclusion
This study investigated the role of mHealth and eHealth interventions in enhancing oral health literacy. It provides valuable insights into the impact of eHealth and mHealth interventions on the general population, including patients, caregivers, professionals, and dental students. The results of this study consistently demonstrated the efficacy of mobile applications, SMS-based interventions, and virtual reality applications in enhancing oral health knowledge, practices, and literacy scores across different populations. In addition, eHealth and mHealth interventions were accepted, exhibiting favorable satisfaction among users and showing their potential for integration into oral healthcare, awareness creation, and education.
However, the heterogeneity of the studies and emphasis on short-term outcomes necessitate more standardized and cross-sectional research to verify the long-term impact of the interventions on oral health literacy. Moreover, emerging technologies should also be comprehensively explored to optimize the integration of technological advancements in oral health education promotion.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251360955 - Supplemental material for Impact of mHealth and eHealth on oral health literacy: A systematic review
Supplemental material, sj-docx-1-dhj-10.1177_20552076251360955 for Impact of mHealth and eHealth on oral health literacy: A systematic review by Ravinder S Saini, Shubham Chopra, Yahya Ahmed Assiri, Fahad Hussain Alhamoudi, Sunil Kumar Vaddamanu, Mudita Chaturvedi, Mohamed Saheer Kuruniyan, Morteza Banakar and Artak Heboyan in DIGITAL HEALTH
Footnotes
Acknowledgements
All authors are thankful to King Khalid University, Saudi Arabia, for financial support.
Author contributions
Ravinder Saini and Yahiya Asseri: conceptualization and methodology. Mohamed Kurunian and Shubham Chopra: data curation and formal analysis. Artak Heboyan and Morteza Banakar: validation and formal analysis. Sunil Vaddamanu: investigation and resources. Ravinder S Saini and Shubham Chopra: original draft preparation. Ravinder Saini, Mudita Chaturvedi, Artak Heboyan, and Morteza Banakar: writing and reviewing, and editing. Artak Heboyan: supervision and project administration. Ravinder Saini: funding Acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors extend their appreciation to the Deanship of Research and Graduate Studies at King Khalid University for funding this work through Large Research Project under grant number RGP2/545/46.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data are available upon genuine request.
Guarantor
Ravinder Saini
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.