
Abstract
The objective of this study was to investigate perceptions of how information technology (IT) is currently utilised in the UK in the community management of cancer pain, perceived weaknesses in the current systems and expectations of future IT systems. Healthcare professionals and patient representatives (n = 46) attended two meetings that explored perceptions of current and future provision of managing cancer pain in the community and the potential role of informatics in supporting this. Discussion was captured and analysed using qualitative methods. Analysis revealed that complexities and barriers to the routine capture of data on pain and related distress focused on locations of care, circles of support, and management and sharing of data. In addition, analysis revealed IT was perceived to be peripheral to supporting delivery and organisation. Delegates shared a vision for an IT system that enabled patients to access healthcare provision by effective co-ordination and communication of patient-centred information. Gaps exist between the expectations of users and the ability of current IT systems to support care. While recognising the potential of tele-health solutions, supporting the complexity of multi-agency care delivery in rapidly evolving clinical circumstances was seen as the main challenge. There is, therefore, a need to position IT more flexibly within the delivery model of clinical care if technology is to address current limitations and enhance the community management of cancer pain.
Background
Significant barriers to the effective management of pain in patients with advanced cancer include failure by professionals to capture pain-related information and failure by information systems to communicate this across healthcare sectors. 1 Lack of effective pain management results in a poorer quality of life for patients and may lead to hospital admission with uncontrolled symptoms. 2 At a time when Western economies are looking to invest in information systems to solve the current health funding crisis there is a rapidly growing demand for more effective deployment of medical technology and drugs. 3 In particular, effective deployment of information technology may enable better symptom management in the community. 4
Despite nearly two decades of the promotion of tele-health solutions there has been relatively little penetration into routine practice and several recent analyses have drawn attention to persisting barriers to widespread adoption. 5 In part, this is due to conflicts between current health information systems deployments and the new vision of multi-provider care models. 6 Current systems are based on institutional ownership, and the data and system architectures are enterprise-based models that rarely include the patient as a user. Furthermore, although patients receive care across many institutions the integration of information is limited. In the USA this has driven the development of Personal Health Records, where individuals maintain their own records.7,8 In the UK where the National Health Service (NHS) has had the responsibility of maintaining patient records for the last 60 years, the challenge of a patient-driven record is proving difficult for the National Programme for IT, 9 as it challenges traditional models of enterprise-based information systems. In the UK, a recent white paper 10 has, again, championed the patient-centric notion of ‘no decision about me without me’. This has given even greater emphasis to shared care and patient access to information, but sets a significant challenge to system developers and providers. 11
For end-of-life (i.e. palliative) care the notion of recasting systems to incorporate this new vision presents a particular challenge as care settings extend to the voluntary sector and hospices outside the traditional NHS provision.
As part of a larger research programme to improve the community management of cancer pain, we wanted to understand the potential role of information technology (IT) in more detail.
Materials and methods
We used a soft systems approach 12 to investigate the perception of how IT is currently utilised in the management of cancer pain, the perceived weaknesses in the current system and expectations of future IT systems implemented within this context.
Participants
An introductory email was sent via local, regional and national networks to health information technology systems experts, health professionals working in cancer pain management and palliative care within NHS or voluntary sector organisations, NHS managers and commissioners from across the UK inviting them to participate in the two master class events. Prior to the events, programmes (including aims and objectives) were distributed and all invitees to event two had access to the presentations made at event 1 and the preliminary findings. In total, 46 participants accepted the invitation and attended at least one master class (master class 1: n = 28; master class 2: n = 28; delegates attending both: n = 22). The majority of participants were health practitioners (n = 22) but there was representation from health informatics, clinical engineering, product design and patient groups. All parties were represented at both master classes and the majority of single event attendees were invited speakers used to set the context of the discussions, for example an NHS pharmacist from NHS Connecting for Health.
Procedure
The master classes were part of the Improving the Management of Pain from Advanced Cancer in the CommuniTy (IMPACCT) research programme. The aim of each master class was to foster dialogue and explore with delegates their perceptions of the current and future provision of managing pain in the community.
The aim of the first master class was to explore delegate understanding of the current IT system for managing pain in the community. Selected delegates presented their own view of the current IT landscape in oncology and palliative care. Presentations included information on current electronic patient record and database systems used in Leeds within primary and secondary care sectors, and electronic prescribing systems being installed in the NHS. In addition, information was presented on the services available through the NHS Information Centre web-based information hub, the patient-reported outcomes using Allograft Information Exchange and on a local project that is exploring ergonomic technology solutions for older people.
The second master class built on the first and asked delegates to critically explore the perceived weaknesses within the current soft systems and to articulate their expectations of any future system.
Master classes were facilitated by senior researchers. Delegates worked in small groups and feedback was shared with the wider group at opportune times. To encourage dialogue, each master class followed the style of World Café.13–15 The format was to use round tables and to encourage free-thinking discussion. Where possible, all debate was captured in written format. This recording included delegates own written notes, observational notes, speaker slides, Post-it notes, written material on tablecloths and discussion summary sheets. Data was transferred into Microsoft Word. Throughout each master class one of the authors (BB) took the role of participant–observer. The role of delegate included being participant recorders as drawings, lists and written notes were retained for analysis.
Analysis
PD analysed the data using an inductive approach, which aims to reduce raw textual data into summary forms and provide models to support processes or experiences while maintaining links with the data. 16 Thematic analysis was undertaken—with themes emerging from the data. Owing to the nature of data collected the analysis process included decoding the abbreviations used by different groups (e.g. from tablecloths and group exercises); the observations noted by BB were used to aid understanding of meaning assigned to particular words. Part of this decoding involved discerning why information was placed on notes and tablecloths in particular ways through conversations with the senior facilitators present—who provided additional decoding—to aid the analyst. Proximity meanings were able to be retained using a qualitative modelling tool within NVivo8. This software was used to facilitate the analysing and grouping of the data into codes and to identify key data themes. From this, the modeller tool was used to further understand the links between written data (i.e. tablecloths and notes) and codes. Understanding and assigning meaning involved using the context of the wider IMPACCT project to aid reflections on the coded data, including relationships between codes. The coding and findings were presented at meetings of the IMPACCT project, which resulted in a distillation of thinking and important member-checking, increasing the rigour of the data coding.
Results
We identified a number of themes, including interconnectivity of services, virtual versus real support and access (e.g. to medical records, medicine, services, funding, education, training, information and support). However, we found three key themes which encapsulated the complexities of the care model that help to explain some barriers to the use of IT systems in the community management of cancer pain: locations of care, circles of support, and co-ordination and communication of information.
Locations of care
Locations of care were described as spaces used for treatment and recuperation. These spaces included the patient’s own home, beds in hospitals, permanent care in nursing homes, and respite and hospice care. The location of care is important as an in vivo phrase which focuses on the place of care as distinct from processes or agencies involved in providing care in these locations. The locations of care came up both directly and indirectly on a range of tablecloths, and in discussions and presentations. These locations were not static, but fluid, bringing additional issues into sharp focus. Furthermore, the use of friends and informal carers as an important part of circles of care are often tied directly to locations of care.
Participants recognised that multiple locations of care with relatively rapid transition between locations added more complexity to the problem of communication among and between agencies when compared with traditional tele-health monitoring. Where success has been achieved it has largely been limited to patient groups with long-term conditions, such as chronic obstructive airways disease, where alerts for early intervention appear to be the main effective benefits.5,17 In addition, in this case, our participants highlighted the frequent involvement of non-NHS services made available within locations of care, which made it more difficult to communicate across agencies as they had no access to shared notes or information held on NHS systems.
The multiple locations of care were perceived to be an additional barrier to understanding the pathway of care by patients and healthcare professionals. Without a linear pathway delegates struggled to understand how information should and/or could be passed across agencies to ensure effective pain management. Both patients and professionals were seen to change location, potentially occupying different locations at different times; this further complicated the IT requirements of organisations.
Circles of support
Analysis revealed multiple individuals providing support to patients that impacted the personal care that patients receive. These included ‘family carers, professionals, healthcare services and community organisations’. The degree of involvement of each source with a patient’s care was illustrated using the concept of ‘circles of support’ where the patient was at the centre surrounded by a number of support ‘circles’. Despite the focus of the master classes being on information technology, delegates described technology as if it were on the outer edge of the wider support circle. Technology was perceived to be peripheral, not central to the co-ordination and delivery of care. Indeed, a group of delegates drew a range of support circles into which a range of services, carers and community organisations fitted (see Figure 1). They drew a box around these circles and IT services was clearly on the outside, beyond the box, showing it to be outside of the support circles. Where delegates did describe the role of IT it was in relation to the barriers the current system presented, for example in the inability to routinely share patient records across agencies. No single technology stood out in contrast, for example, to diabetes or chronic obstructive airways disease where discrete, disease-specific monitoring tools are available.
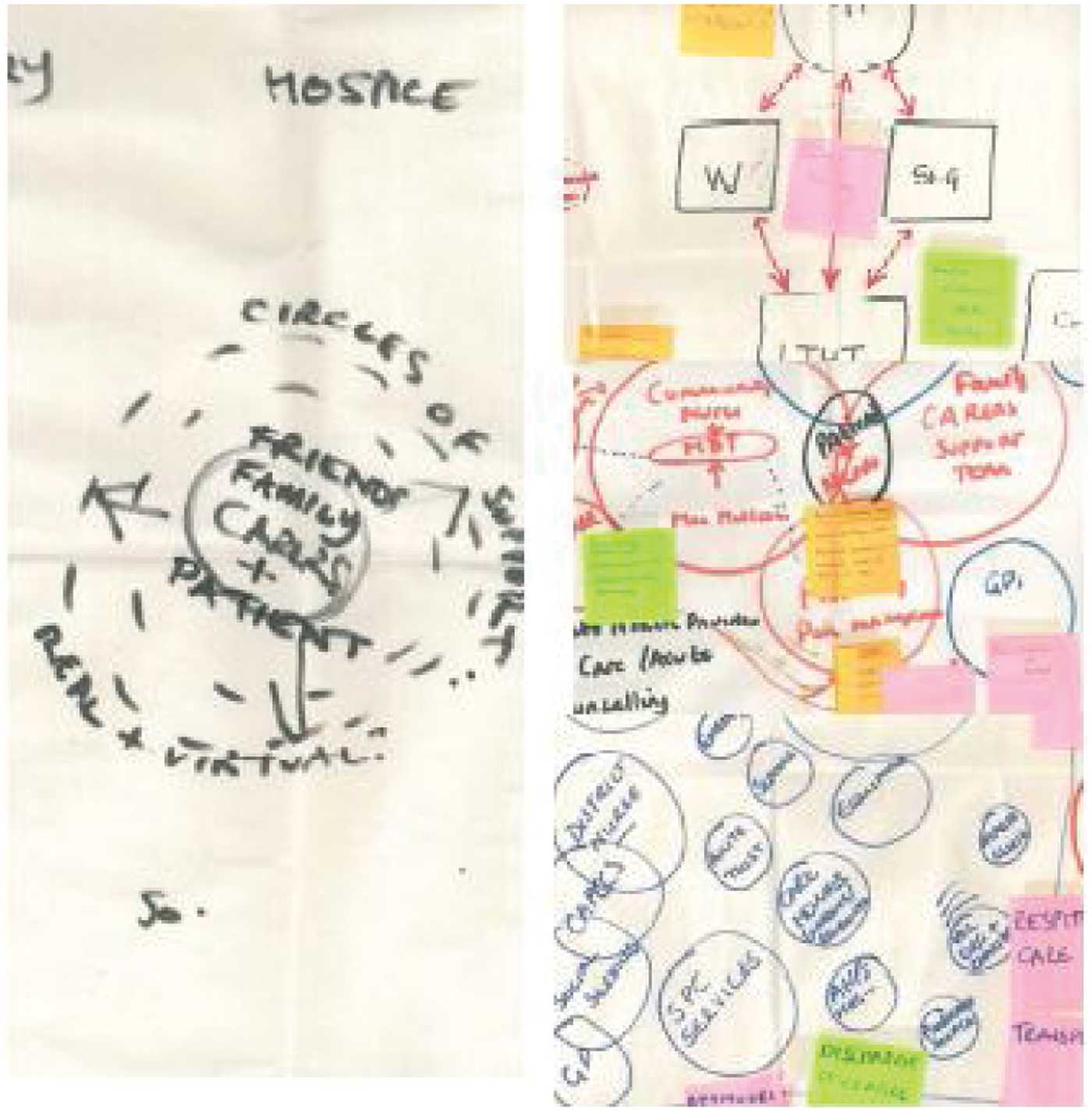
Extracts from ‘tablecloth’ group workings showing circles of support
The perceived lack of system interconnectivity was evident in the way delegates described the circles of support. Firstly, physical support provided by carers at the coal face (provided by an agency, general practitioner); secondly, support that is provided by non-medical professionals, such as family, relatives, friends, neighbours and volunteers; and thirdly, virtual support from websites or telephone helplines. These three circles were described as being a series of concentric circles, with physical support being considered closest to the patient (and of most importance) moving out to virtual support.
Co-ordination of direct care—support being provided by multiple carers and key-workers—was identified as a challenge for the effective management of pain. Delegates identified a lack of consistent dialogue between providers. There was a perception that better infrastructure was needed to support people staying at home. This included organisations being aware of which organisation (and, in some cases, which individual) was responsible for each aspect of care. For example, knowledge of the patient was described as being a series of single information bites with actions being taken in isolation. Delegates hoped that future technological solutions would provide an opportunity to co-ordinate and integrate this information to achieve better overall delivery of personalised care.
Understanding of current virtual support was primarily focused around the information needs of patients and carers. Delegates also considered the possibility of using electronic media as sources of social support (websites, social networking sites). The perceived lack of interaction between physical personal support and virtual support was identified as a barrier. Currently, systems recognise only the patient and it is therefore difficult for systems to take account of information provided by non-health professionals who can play a key role in the monitoring and management of pain (e.g. friends, family, neighbours and volunteers). Delegates suggested that patients would benefit from the development of systems that could grant access to those providing personal physical support. As well as being of benefit to patients it was suggested that carers are present at times when agencies and professionals are not. They may, therefore, be able to provide useful data and information otherwise missed.
Delegates suggested multiple circles of care mean that care pathways adapt and change to enable accommodation of changing circumstances. The current information management system was seen to struggle to accommodate this varied and dynamic pathway of care. For delegates, the system was unable to provide meaningful co-ordination between agencies and professionals, particularly between state (NHS) and voluntary sector organisations (e.g. hospices). This lack of co-ordination was exasperated by the number of different ‘access points’, with patients opting in or out of services depending on their level of need. Although individual agencies had their own IT system, delegates perceived a lack of systems able to provide a coherent overview.
Co-ordination and communication of information
Delegates identified weaknesses in the way the current IT systems dealt with the management and sharing of patient and health professional data. They desired a system that would be suitable across all agencies that deal with pain management; in particular, data-management systems that would allow the capture and communication of pain data between services and/or individuals. There was also a recognition that a common scale of measurement would be need to capture and summarise the needs of a patient, but that any instruments developed would need to take account of trade-offs between pain, medication levels and functional impairment which patients were willing to accept. The hope was for technology to facilitate collaboration, information-sharing and, ultimately, support better patient care and experiences.
One solution put forward was to develop a system where access to services was through a key agency. This single agency would have responsibility for ensuring the co-ordination of transmission of information (to, and between, all other agencies). According to delegates, a more attractive solution was one that did not depend on the patient being in contact with any particular agency to ensure co-ordination of transmission of information. This would enable co-ordination and communication of data regardless of where a patient is situated within the care pathway. As the following qualitative quote suggests, delegates considered a system that positioned the patient, rather than key agency, as gatekeeper might best be able to accommodate patient movement along the care pathway and prompt relevant people along the way.
What is needed is: “(1) patient as a portal (wherever they are); can people access relevant records at that point; (2) patient as prompter (how do they initiate call for help) this is just the alert system, signalling to the system that provides response”.
Delegates struggled to visualise how IT systems could accommodate the necessary flexibility while still providing structure to ensure communication between the relevant agencies. It was suggested a better understanding of how patients and organisations use the current care pathways may offer insight into how such capabilities could be accommodated by future systems.
Potential barriers to the creation of a system that could deliver the expected functionality were identified. Many of these were around institutional regulations concerning data management and sharing. Delegates were unclear as to who would have responsibility for effective capture, generation, storage and transmission of data. The ability to envisage how a system might be able to handle all processes was further hampered by concerns about the non-standardised nature of data that each agency collects. The heterogeneous nature of data collected was seen as a reflection of the different duties of care and organisational priorities that each agency is responsible for. The absence of a mechanism that facilitates routine collection and sharing of data collected from disparate data sources was seen as a key stumbling block to effective sharing of information.
Although much of the discussion around data capture and communication appeared removed from the lived experiences of patients, the vignettes shared by delegates highlighted the real impact miscommunication of information can have on the management of patient’s pain (see Example 1).
Example 1: Impact miscommunication of information can have on the management of patient’s pain
A patient regularly undergoes treatment that includes a number of different medications. During a patient visit to the General Practitioner (GP) the decision is made to alter the patient’s pain medication and the GP issues a prescription accordingly. In England, the GP and the Pharmacy IT system are not integrated and therefore this change is recorded only on the GP system. While the patient collects the correct script on the first occasion the list of repeat medications (stored on the pharmacy system) remains unchanged. As a result when the patient collects their next repeat prescription the original dosage is included. The patient does not question what appears to be yet another change to their dosage, believing the change must have been ordered by their GP.
Delegates suggested that if systems enabled linking of systems (e.g. GPs and pharmacists) the problem of miscommunication of data captured could be addressed. Concerns surrounding the confidentiality of patient records meant delegates did not support the viewing of the entire patient record by all healthcare providers. The ability of selected health professionals (e.g. pharmacists) to interact with relevant components of the patient record was, however, seen as paramount. Though electronic prescribing systems are being introduced into the UK, uptake has been extremely slow (<10% of all GP prescriptions 4 years after launch) and they concentrate predominantly on repeat prescriptions rather than rapidly changing requirements for controlled drugs in this situation. 18 Experience is also showing that, even where records can be shared, reconciliation of prescription information between what is prescribed, what is dispensed and what is actually being taken is extremely difficult. 19
Discussion
Delegates shared the UK government’s aspiration for an IT system that enabled patients to access effective healthcare provision by virtue of effective co-ordination and communication of patient-centred information which has been reinforced recently by the ambition to provide remote care to 3 million patients within 5 years. 20 The process of engaging in the master classes enabled delegates to voice their concern over the ability of current systems to cope with the drive towards increased provision of care in the white paper. 21 While they could foresee the desired functionality of any future system, delegates struggled to identify how such systems would operate within the current landscape of multiple agency working that lacks both physical and virtual co-ordination. In some ways, this echoes the findings of the Healthcare Commission Report into Innovation and Health 22 and the final report of the NHS Whole System Demonstrator 17 which addressed the integrated use of tele-care in the context of a health community. Silo budgets, culture change and organisational inertia are frequently cited barriers to the uptake of tele-health solutions, even where the technologies are proven to be effective in small-scale trials or through anecdotal evidence. It is also noteworthy that Cruikshank cites the availability or visibility of shared care records 5 as a key enabler of successful tele-health—echoing our findings. These continue to be recurring themes in evaluations of even the more successful tele-health deployments throughout Europe.23,24
The breadth of the care groups supporting patients in this end-of-life context highlighted in the ‘circles of care’ is an important finding. It implies that one or more main carers may have to be given access to information in lieu of the patient, who may not be capable of managing the access. This fundamentally challenges data security models in some current and recently developed health IT systems where patient-centric models of access are the predominant consideration. Again, this is because of the development focus being on reducing the burden of long-term conditions through patient self-management rather than on short-term, highly complex interactions between multiple agencies of care where the individual patient may not be competent. 5
Thus, though the underlying requirement of maintaining open and appropriate communication between parties is a simple one, the information system needs are complex. The challenge is to allow controlled access from outside agencies to detailed care records. Where multiple systems are involved, keeping the content of the patient record aligned is challenging. Current systems encourage institutional ownership with the result that any discussion about system development raises important issues about access, confidentiality and ownership of patient data. These concerns largely reflect the organisations’ needs more so than patients’ needs. 25 The challenge is how to involve agencies and patients in developing systems that can be accessed whenever and wherever needed within the pathway. To enable this vision to be realised, collation of data between different data systems must first be enabled to provide a fuller picture. Secondly, the ability of different agencies to connect with the system should not be limited to NHS services, or hardware location. Thirdly, longer term, collaborative funding models need to be in place to create sustainability. It is likely that in this context the GP record will become the master data sources against which care will be co-ordinated; in this region (Yorkshire and the Humber, UK) the penetration into palliative and community care of TPP SystmOne, which is based on the sharing of a single core record, promises to provide such a platform (SystmOne, The Phoenix Partnership, Leeds, UK). This platform currently carries 20 million detailed patient care records, covers 70% of patients within our oncology catchment and already supports thin client web access under smartcard control. 26 Whether current organisational barriers can be overcome to develop truly patient-centric inter-agency models of service delivery is the subject of our next phase of research. Although our study is UK-based we believe our findings have relevance to all complex care systems. In particular, we have referenced the challenges of using enterprise architectures in delivering care across organisational boundaries, especially where multiple government and voluntary sector agencies and carers are involved.
In summary, we identified barriers to the current use of IT in the community management of cancer pain centred on the number of different agencies and locations involved in delivering care and the perception by healthcare professionals that IT was peripheral to the delivery of this care. We identified important areas for further research and development. These include integrating multiple independent systems to allow sharing of information and developing new approaches to IT, particularly in rethinking the models of security access and of capturing rapidly changing needs in ways that facilitate common interpretation and understanding. This should enable patients, carers and healthcare professionals to engage more effectively with IT (e.g. using messaging and portal technologies) and ensure more responsive, patient-centric co-ordination of care with the ambition of improving outcomes and experiences.
Footnotes
Funding
This article presents independent research commissioned by the National Institute for Health Research (NIHR) under its Programme Grants scheme (RP-DG-1108-10010). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.