
Abstract
Approaches to pain management using electronic systems are being developed for use in palliative care. This article explores palliative care patients’ perspectives on managing and talking about pain, the role of technology in their lives and how technology could support pain management. Face-to-face interviews were used to understand patient needs and concerns to inform how electronic systems are developed. A total of 13 interviews took place with a convenience sample of community-based patients with advanced cancer receiving palliative care through a hospice. Data were analysed using framework analysis. Four meta-themes emerged: Technology could be part of my care; I’m trying to understand what is going on; My pain is ever-changing and difficult to control; and I’m selective about who to tell about pain. Patients described technology as peripheral to existing processes of care. To be relevant, systems may need to take account of the complexity of a patient’s pain experience alongside existing relationships with health professionals.
Background
Pain affects the quality of life of cancer patients, their families and caregivers. 1 For community-based cancer patients, pain remains common, severe and under-treated. 2 Barriers to good pain management include knowledge deficits, misconceptions and inadequate pain assessment. 3 Strategies highlighted for addressing these include empowering patients and their caregivers to self-manage pain, improving communication, and adopting individualised and non-pharmacological approaches. 4 Communication is key to these approaches, and is important for a patient’s quality of life and outcomes in cancer care. Despite this, many patients are left with unmet communication needs. 5 There is a need for new approaches to communicating pain experiences that are acceptable and usable for patients that enable them to share their experience of pain with health professionals.
For patients with chronic conditions such as cardiovascular disease, diabetes, cancer and chronic respiratory diseases, digital communication technology has been shown to enhance communication 6 and access to health care. 7 For palliative care health professionals, electronic systems can enhance workflow through improved symptom identification and assessment and save time during clinic visits.8,9 However, technology can be perceived as peripheral to care delivery if it does not effectively coordinate and communicate information or fails to be positioned within the delivery model of clinical care. 10
A recent literature review of information and communication technology (ICT) use for managing pain in palliative care identified systems for pain and symptom management, and quality of life assessment. 11 For palliative care patients, the benefit of electronic systems has not been well articulated in the literature; proposed benefits include increased communication with health professionals, privacy (through an electronic environment) and added flexibility to assessment. 12 Currently, there is a lack of reported perspectives of palliative care patients regarding how ICT systems could be used as part of their care. It is necessary to pay special attention to patient needs and concerns to ensure they are met in electronic system development. 13
Aim
To describe palliative care patients’ perspectives on managing and talking about pain and the role of technology in their lives. These insights were sought to determine the potential for harnessing technology to support their pain management.
Methods
This work was conducted as part of the development of an electronic system, PainCheck. PainCheck aims to improve the reporting of pain by patients with cancer based at home by enabling them to communicate electronic pain reports to their healthcare professional. Patient perspectives have been gathered alongside those of health professionals, 14 to ensure that PainCheck was tailored to meet the needs of users. Research ethics committee approval was obtained (NRES Committee Yorkshire & The Humber – South Yorkshire; 13/YH/0054).
Design
This qualitative study used face-to-face semi-structured interviews with palliative care patients with advanced cancer.
Sample
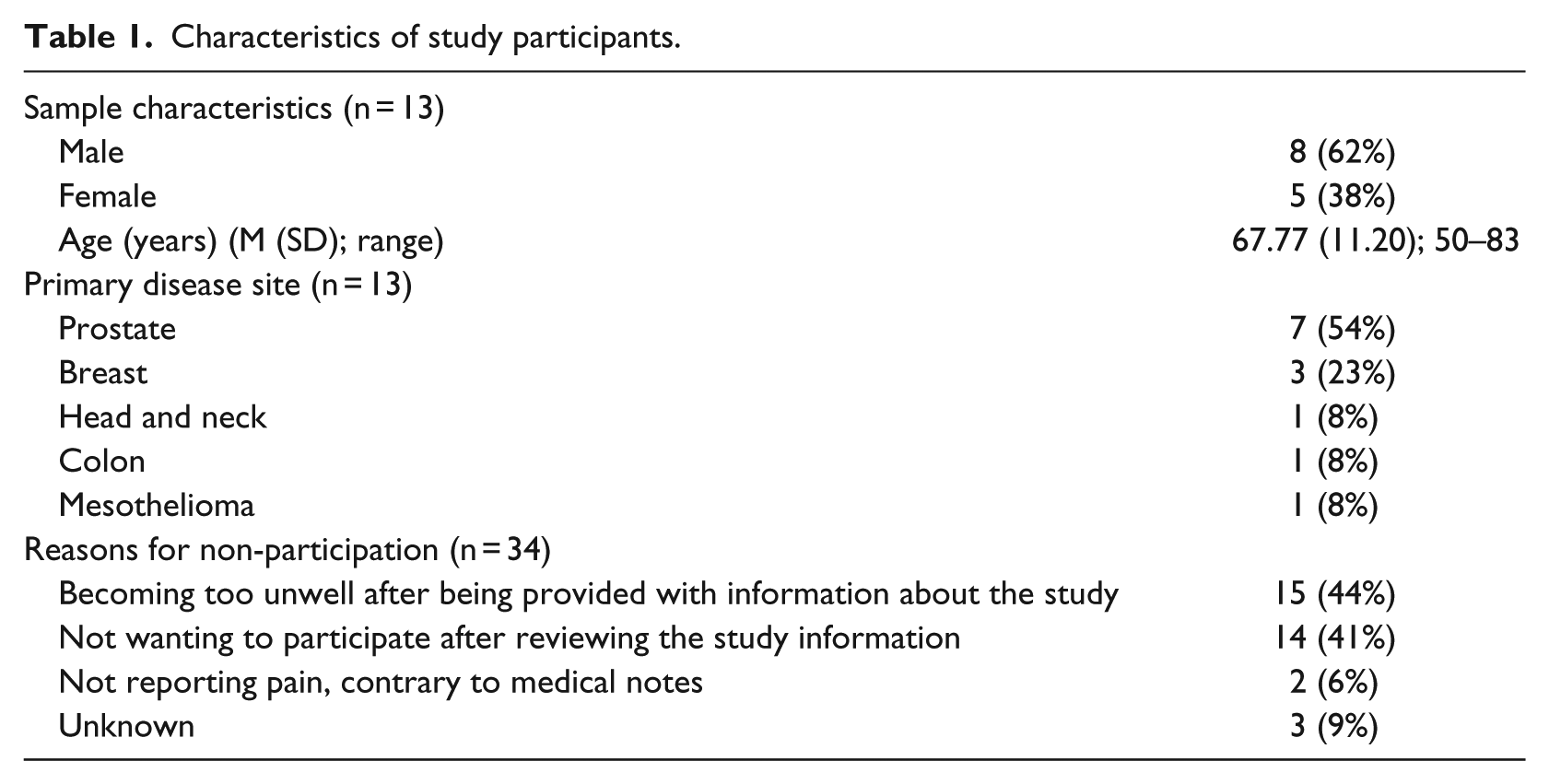
In total, 47 participants were recruited to the study, of which 13 (27.6%) participants took part. Of the 13 participants who completed the study, around two-thirds of the sample were male (n = 8; 62%), the majority were White British, and the average age was 67.8 years old (standard deviation (SD) = 11.2). Over half (n = 7; 54%) of participants had prostate cancer as their primary cancer type. Over half of participants were married or in a common-law relationship (n = 8; 62%) with the remainder either separated, divorced or widowed (n = 5; 38%). Details of patient characteristics and reasons for non-participation are outlined in Table 1.
Characteristics of study participants.
Participants and recruitment
Participants were purposively sampled from two hospice sites by two research nurses, one based at each site. Research nurses initially approached patients at outpatient day centres and inpatient wards that were aged ≥18 years, had advanced cancer (those with metastatic cancer and/or those receiving anti-cancer therapy with palliative intent), had pain (receiving analgesic treatment for cancer symptom-related pain and/or for treatment of cancer therapy-related pain), had a good level of spoken and written English, and were able to provide informed consent. Participants were excluded from the study if, in the opinion of the clinician or research nurse, they were unable to understand and complete the survey and/or unable to provide informed consent, or deemed inappropriate to approach (e.g. those where death is imminent).
Procedure
Interviews were conducted at home or in the hospice by M.J.A. with the participant alone (n = 10) or together with a family caregiver (n = 3). Interviews lasted an average of 69 min (range: 20–110 min). A topic guide was developed which focused on the background and experiences of cancer for participants, how pain is currently discussed and with whom, the role of technology (defined very broadly as any ICT) in the lives of participants and its potential to support pain reporting. The topic guide was modified after the first two interviews, adding a question to further probe who participants preferred to discuss pain with. Interviews were audio-recorded and transcribed verbatim. M.J.A. recorded thoughts and observations following interviews to facilitate reflection. All interviews took place between November 2013 and April 2014.
Data analysis
One coding frame, informed by framework analysis, was developed to classify all utterances by participants. 15 Four transcripts were purposively selected by sex (n = 2 male and n = 2 female) and cancer type (n = 2 prostate, n = 1 bowel and n = 1 breast) to develop the framework. M.J.A. read each subsequent transcript at least twice to familiarise himself with the content, broke the responses into self-contained meaningful units and developed codes for these units. Data were initially coded deductively to areas pre-specified in the topic guide; further codes emerged from the data inductively. Codes were grouped to form overarching themes which were iteratively refined over the course of analysis. M.J.A. and B.M.B. discussed the codes until consensus was reached on meaning and label. Codes were then grouped according to meaning and discussed until consensus was reached on group homogeneity. The groups formed the thematic structure of the coding frame. M.J.A. applied the coding frame to all participant utterances using NVivo 10 to manage the coding process. A total of 141 codes were identified and grouped under 10 themes and one miscellaneous category.
Results
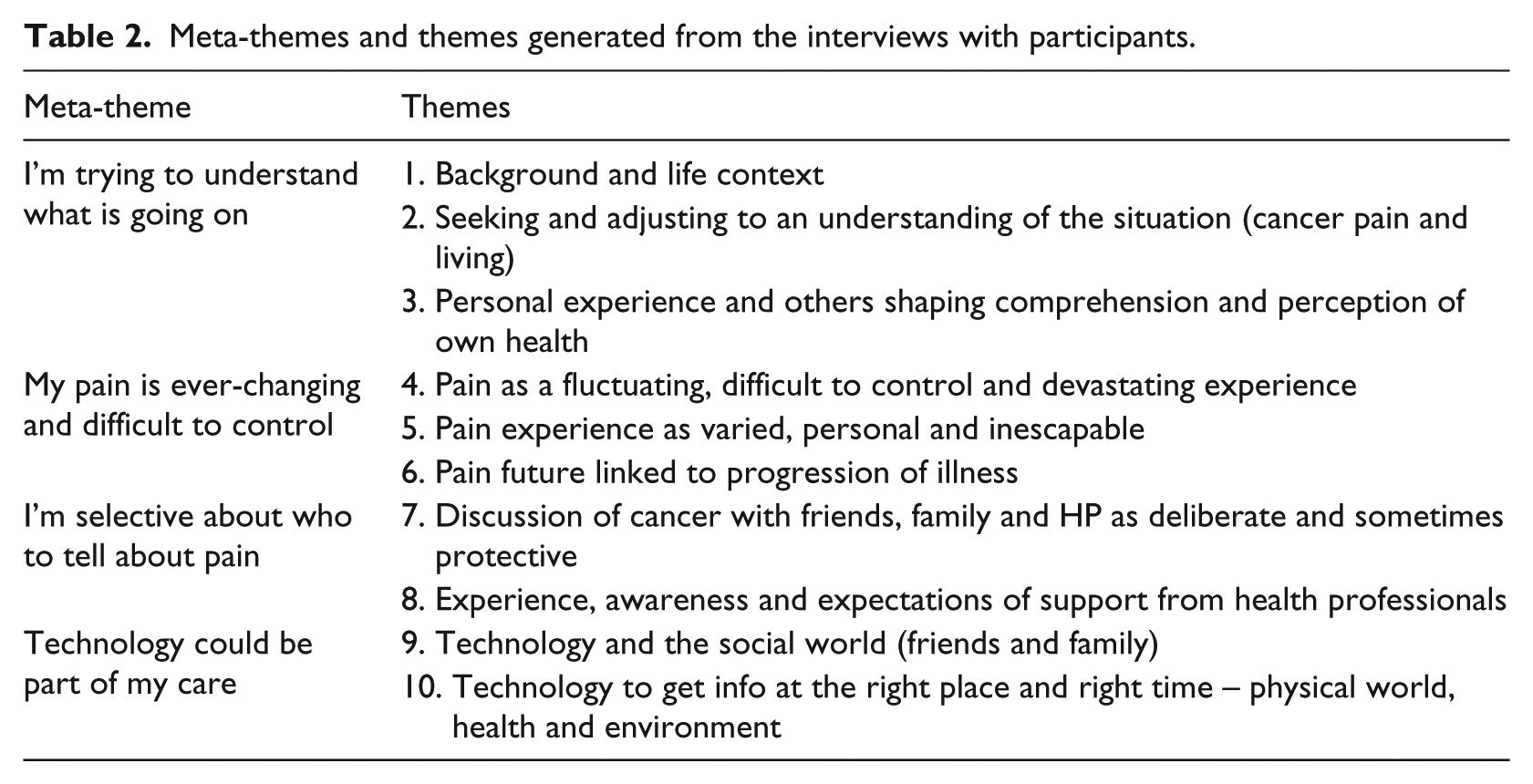
Narrative synthesis organised the findings under four meta-themes: (1) I’m trying to understand what is going on, (2) My pain is ever-changing and difficult to control, (3) I’m selective about who to tell about pain and (4) Technology could be part of my care (Table 2).
Meta-themes and themes generated from the interviews with participants.
I’m trying to understand what is going on
A sense of uncertainty was expressed by participants trying to understand what is going on in their lives while living with advanced cancer. Understanding was sought through reflection on their own identities and using snippets of information from other cancer patients. Their understanding was often incomplete. Symptoms were seen as a marker of changes to and the impact on a patient’s life. The prevalence of problematic symptoms was often interpreted, by the patient, as an indication that the condition is progressing. For patients, pain leads to questioning about the cause of the pain, with concern that pain means a condition is progressing which in turn instigates worry about the consequences of the advancing disease. Mood contributed to the uncertainty about the future for patients with advanced cancer, influencing how they perceive their condition:
I think it’s impossible to feel in control of things when … you know within a space of a very short time you are in a wheelchair, you’re losing, and there’s still, you know, the possibility that you know some, I have a fall or, you know, potentially it’s not just this one spot but potentially it might, my spine is affected by cancer all the way, there’s tumours all the way down, so there’s that kind of knowledge that you know paralysis could be a knock away if you like … (Male, 62, prostate cancer)
How patients self-identify and see themselves is central to how they think about and manage their condition. Most patients compared their own lives to others living with cancer, particularly with regard to symptoms and pain, attributing worse situations (home life, experience of symptoms) to others. For themselves, most patients had a sense of normality that views continuation of daily activities as important. There was an expectation that symptoms would arise and accompany a diagnosis of cancer, and patients would seek an understanding of the interruption of their normality. There was also a stark awareness that normality is becoming harder to achieve and symptoms, such as low mood and fatigue, hindered the living of life:
I just want, that’s what I want, I just want normality, but the normality’s gone, there’s no normality anymore, unless I’m on my own, but even then I can’t do, I look at the house and I think god if I wasn’t ill I’d have this decorated and all sorts done by now, and it’s horrible, because I know as soon as do something I’m going to be in agony. (Female, 56, breast cancer)
As cancer progresses, patients want to continue to complete routine activities with friends and at home that were completed prior to cancer. Adjustment to their condition reveals different levels of adaptation to symptom changes with consequential influences on patient behaviour and decision making:
… but getting things in perspective you can look at the day ahead and think oh god I don’t feel right good and I was going to do so and so but it’ll have to wait a day and I change plans … simply because I’ve moved things around a little, you know. (Male, 67, prostate cancer)
As part of trying to determine what is going on, patients try to gather information to ascertain how long they have left to live. Patients expressed uncertainty about time remaining before death. Their beliefs about their own prognosis were not always consistent with the information they gathered from varying sources. Those receiving a specific prognosis often rejected the accuracy of the time frame for longer time horizons. Such seeking of an understanding of their illness and changing life led patients to describe cancer as creating an uncertainty in their lives. Day-to-day, a patient’s mood can have an influence on their broader outlook of their condition:
You know, mood and mood fluctuations comes in to it, it’s very relevant to it all, if I’m feeling positive and good about things you know I think physically I feel better, if I’m despairing or bit bleak then I think, I feel that physically as well (Male, 62, prostate)
My pain is ever-changing and difficult to control
Patients describe a variability that makes pain difficult to control and manage, and at times uncontrollable. The consequences of experiencing pain at its worst can be debilitating. The variation in pain can be across locations in the body, with some participants experiencing pain in multiple places. Patient beliefs about the likelihood of achieving pain control varied, with differences in how achievable it might be. For patients where pain was constant, there were instances where pain can be perceived as manageable:
I mean some days I could manage the pain quite well and other days I couldn’t manage it at all, I felt I didn’t have much control over it; it was just fluctuating throughout the course of the day, and some days it just stayed steady and other days it just, but as I say I was always I’m always in pain, it’s always there. (Male, 56, head and neck cancer)
Medication was the primary way of controlling pain. The level of control provided by medication varied across time and between patients. The fear of experiencing pain motivated adherence to the medication and a desire to avoid pain led some patients to keep medication in close proximity:
I’ve medicines upstairs and medicine downstairs so that if I get stuck on one level at least I’ve only got to get to the front room cause it’s on the bottom window, so if I’m upstairs I only have to get to the bedroom cause it’s on the dressing table top in there, so I know I’ve not got very far to go to get medicine. (Female, 56, breast cancer)
Pain relief from medication can take time for patients to achieve and is often temporary. Where pain was not controlled, episodes of intense pain were reported, with fatigue and tiredness experienced after an episode of pain. While medication is one way most patients seek to control pain, patients also develop their own non-medical approaches to managing their cancer pain, such as sleeping or taking a warm bath. Actively exploring ways of alleviating their own cancer pain was empowering for some patients:
… but all these things that I do they’re so empowering because I feel that I’m not in just the hands of the doctors because sometimes I find they’ve got tunnel vision. (Female, 62, breast cancer)
I’m selective about who to tell about pain
Patients’ telling about their cancer pain is hindered by difficulty with describing pain. Patients had difficulty in understanding how to quantify or make sense of pain and there was difficulty in expressing the subjective nature of pain. But patients were able to use clear terms to describe the types of pain experienced, its periodicity and an element of knowing when it is likely to occur:
cause I can get these pulse pains as well where they’re really, it feels like something has just grabbed my liver and squeezed it hard, squeezing, and it’s really, really chronically painful, and then it’ll just suddenly stop, and it leaves me feeling bruised, quite warm, quite wet around that area, so it’s like it’s bled out but it’s not bleeding, it just goes off after a while. (Male, 56, head and neck cancer)
The decision of a patient to tell about their cancer pain is often influenced by reluctance to be a burden and the anticipated impact on others. Patients did not think their cancer pain would be of interest to others. When discussing cancer pain with family, most patients expressed reluctance to fully disclose their experience to partners or other members of the family. Choices around disclosure to caregivers were often driven by its anticipated impact on caregivers:
Yes. Em … (Sighs) … I, I think … I tend to keep difficult … things away from wife. Em … because she doesn’t cope with it very well. She always sees the dark side … of things. And em … quite frankly I don’t find that very helpful. (Male, 72, prostate cancer)
There was a contrast between patients with the ability to have intimate discussion with friends, and those whose friends no longer formed part of their life since diagnosis. Withholding of information extended to discussions with health professionals. Causes for withholding included changing personnel in secondary care, anxiety about how they would be perceived, and fear of consequences of disclosure (e.g. an admission):
… I’ve rung the hospital a few times, the trouble when you ring them they want to admit you, you know, when you ring them it’s kind of you know something is wrong with you and then they’ll say I think you need to come down, you know, to the hospital. (Female, 50, mesothelioma)
For patients telling health professionals about their cancer pain, there was an expectation that they should understand the patient. A common area of misunderstanding between patients and health professionals was in discussions about medication. A rapport built with health professionals was often a prerequisite to patients being comfortable to talk openly – this tended to be present in general practitioners (GPs), where some had long and established relationships with patients.
While there was selectivity in discussions about pain with family, friends and some health professionals, the hospice was reported as the focal point of care for most patients. The hospice was seen as an expert in managing pain and cancer. While other health professional groups contributed to care, the hospice was at the core. Patients who were engaged with hospice services describe communication as led and directed through the hospice to other health professionals – with a demonstrated awareness of active communication taking place. Health professionals at the hospice helped to clarify expectations from end-of-life care. The care received from a hospice was used as a benchmark for end of life care received from other providers. Clinical nurse specialists in particular provided direct and regular contact to patients and were often identified as people with whom they have meaningful discussions about their condition:
… when you’re talking with Macmillans it’s just like talking about any other thing and it’s just like it’s just an issue, just, and it’s no different to a bag of fish and chips, really, realistically, it’s just in simple terms isn’t it, this is what we want to talk about, pain, and if you’re in pain you do want to talk about it to somebody don’t you, but they’re far superior to GPs. (Male, 67, prostate cancer)
Technology could be part of my care
Patients reported existing ways that technology is embedded in their lives, particularly when used with their family and friends. There was variation in their use of computers, with frequent users and others that did not use any computer. Most patients had access to and used mobile phones although sometimes this was for a specific reason (such as a mobile phone in the car for emergencies). The use of landline and mobile telephone was the most common and preferred way that participants communicated with other friends and family. Using the phone to talk to people was preferred to sending text messages. Older patients that were not regular users of mobile phones and computers preferred communication that involved talking directly with someone (e.g. a conversation on the telephone) and did not rely on technical knowledge:
The fact that I use the phone, it’s the human voice, it’s being able to talk to a human voice knowing that I’m passing the message on. The electronic way is to me a bit vague, you know, because I’m never sure that it gets to where it should be. (Female, 83, breast cancer)
There was a general willingness to embed technology into interaction with health professionals, with potential benefits to its use as a way of communicating about pain:
I suppose a computer, you know an electronic input, that’s it, kind of thing, and it might, I think people might find it easier to report on themselves in that way rather than ‘I’m alright doctor’, or whoever. (Male, 62, prostate cancer)
Some patients were concerned about the security of their data and reliability of electronic systems, and were worried that it would generate additional work for health professionals. Patients were also fearful of being exposed to unhelpful information about cancer on the Internet, which was perceived to focus on worst-case scenarios:
The only thing I don’t like about the internet, and I hate it, is the fact that it gives out knowledge that is the worst-case scenario for anybody, consequently if something comes up, you know, that somebody says you’ve got X, they look it up on the internet and all sorts of horrible things are told to them and I don’t think that should be. (Female, 83, breast cancer)
Descriptions of patients’ use of technology saw it as peripheral to the way they currently interact with health professionals. Patients had not used technology as a way of communicating with a health professional. This contrasted with approaches taken by patients with friends and family, where technology devices were regularly used and embedded in methods for communicating.
Discussion
Patients were living with uncertainty about their condition, compounded by complex, difficult-to-control pain experiences that can be distressing and provide misleading cues about the advancement of disease. Cancer pain is difficult to control and manage, with patients remaining selective in who they discuss their symptoms with, often withholding information from family and friends. Health professionals, and in particular staff at the hospice, were consulted about pain because they were seen as expert in its management. Patients were willing to explore options for harnessing technology to support pain management, but technology is currently peripheral to existing processes of care. We found that, for those who had access to mobile and communication technologies, technology was linked to maintaining contact with friends and family.
ICT systems are emerging that provide a new approach to pain monitoring and assessment. 11 However, isolated assessment and monitoring of symptoms available with existing systems are unlikely to take account of the complexity of the pain experience described by patients with advanced cancer. Patients expect and value care that treats them as people, rather than a focus on their symptoms. 4 As such, ICT systems need to evolve to support recommendations for in-depth and tailored assessment that situates pain within a wider understanding of a patient and their everyday circumstances. 16 Furthermore, concerns such as exposure to unhelpful information when seeking details relating to a condition may need to be addressed as part of implementation. In these instances, there may be value in approaches in which health professionals support identification of relevant and reliable online health information. 17
While patients report willingness to engage with technology as part of their care, the challenge for those developing systems for cancer pain management is how to align ICT with the needs of individual patients. For example, in this study, patient judgements about how well their pain is controlled were determined by an ability to perform activities or tasks and maintain relationships with family or friends. These personal goals can determine patients as individuals, but are not typically discussed with health professionals. 18 Currently, ICT systems for cancer pain management rely heavily on electronic formats of standardised pain assessment tools (such as the Brief Pain Inventory 19 ). 11 The Brief Pain Inventory allows a patient to rate the severity of their pain and the degree to which their pain interferes with feeling and function. While important to clinical practice, populating ICT systems with only standardised pain assessment tools could miss an opportunity to increase the value of systems for patients. What a patient deems to be a successful outcome from pain management is unlikely to relate solely to numeric pain scores. Future research is needed to understand how more individualised assessment can be developed as part of ICT systems for cancer pain management.
A large proportion of ICT systems for pain management in palliative care support a unidirectional flow of information; data gathered from the patient and sent to the health professional with limited or no feedback. 11 Among health professionals, there is an increasing recognition of the desirability and achievability of self-management of pain by patients with cancer; 20 an approach that could empower patients and increase a sense of control over their lives. In order to facilitate or contribute to such approaches, those developing ICT systems need to determine how data submitted by patients can best be used to deliver personalised feedback, tailored information and relevant guidance.
Patients currently see technology as peripheral to the way that they interact with health professionals. New approaches may be required to encourage and facilitate patient interaction with health services through ICT for their cancer pain management. This is likely to prompt rethinking around models of security access and integration of multiple independent systems used by both patients and health professionals. 10 It is also important to define and understand how and when a cancer patient is likely to interact with and benefit from ICT when it is offered as part of their care. Numerous systems have been developed for use at earlier stages of the cancer trajectory (e.g. symptom management during active treatment).8,21 ICT introduced at this earlier stage may be driven by the likelihood of less advanced disease with fewer complications. For palliative care patients that engage with technology, benefits to its use are only beginning to be understood, such as enabling patients to feel supported and remain in their place of residence. 22 For those with pain, ICT systems are being developed to increase self-management (through incorporating education components and information provision), 23 but their effectiveness for pain management has not yet been determined. ICT can also provide a resource for patients, such as such as supporting pain identification and assessment. 23 Such benefits need to be delivered through systems aligned with patient preferences; easy to access, secure, effective and have minimal or no cost. 24 Intended ICT system benefits need to be aligned with patient preferences; easy to access, secure, effective and having minimal or no cost. 14 Embedding all perspectives (patient, caregiver and health professional) in ICT system design may promote greater engagement with any resultant product. Approaches that encourage such broad stakeholder participation and organisation of parallel integration of ICT systems into existing care processes, such as user-centred design,25,26 are essential for eHealth technology development and may lead to greater uptake and impact. 27 However, additional approaches may be required to guide the marrying of user requirements from both of these groups in ICT system development.
Limitations
This study provides novel insight that can inform the earliest stages of ICT system design. The participants in this study were English-speaking, with a high proportion of males with prostate cancer, who had been referred to a large urban hospice and were receiving symptom management from a specialist palliative care team. The findings may have relevance for other patients with advanced cancer as there was commonality in the experience of pain across disease types. Further research is needed that explores the way in which ICT systems can support pain and symptom management across patients with advanced cancer from a range of age groups and cancer types.
Conclusion
Early engagement with palliative care patients can inform thinking around the requirements for ICT systems at the start of development. The narratives of patients on the management of their pain and the role of technology in their lives pointed to a number of key considerations. Simple approaches that employ well-established technologies may be a preferred starting point. In order for system content to have relevance for a patient, it needs to take account of the complexity of their pain experiences and existing relationships with health professionals. Future research is required to understand how ICT systems can be positioned flexibly within existing delivery models of palliative care.
Footnotes
Acknowledgements
We would like to thank Professor Hilary Bekker for her guidance during the early stages of the analysis.
Declaration of conflicting interests
The author(s) declare no conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This paper summarises independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research programme (RP-PG-0610-10114). The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.