
Abstract
E-health is seen as an important technological tool in achieving self-management; however, there is little evidence of how effective e-health is for self-management. Example tools remain experimental and there is limited knowledge yet about the design, use, and effects of this class of tools. By way of introducing a new view on the development of e-health tools dedicated to self-management we aim to contribute to the discussion for further research in this area. Our assumption is that patient empowerment is an important mechanism of e-health self-management and we suggest incorporating it within the development of self-management tools. Important components of empowerment selected from literature are: communication, education and health literacy, information, self-care, decision aids and contact with fellow patients. All components require skills of both patients and the physicians. In this discussion paper we propose how the required skills can be used to specify effective self-management tools.
Introduction
The number of people with chronic conditions continues to rise, while the number of healthcare professionals caring for those patients is expected to decrease1,2. At the same time, patients are becoming more critical, better informed and more participative 3 . They are increasingly expected to take a more active role in the management of their disease by engaging in self-management activities4,5. The urgent need for self-management is reflected in a range of ongoing initiatives, as for instance, in the Netherlands6,7.
E-health is seen as one of the important support tools for patients and professionals alike6,8–10. Although the number of e-health tools to support self-management is growing11–14, the development of these systems is not always based on the research literature and, consequently, the theoretical basis of these systems is limited, or even lacking 15 . Most tools are still in the experimental phase and there is no body of knowledge yet about the design, use and their effects. As we have argued elsewhere 16 , there is currently little evidence that e-health tools for self-management draw on patient empowerment principles.
This discussion paper aims to add to the theoretical foundations of the design principles of e-health tools dedicated to self-management. It addresses this issue from a new perspective and aims at widening the discussion for further research in this area. As a starting point, we consider that patient empowerment is an important mechanism of self-management. We suggest that the different components of empowerment, alongside the required skills of patients and professionals, are the building blocks for the design of e-health tools.
The paper is organised as follows. A set of six components of empowerment is first identified from the literature. Subsequently, characteristics of self-management with respect to patient’s skills and the physicians’ skills are then derived. We further postulate on how design principles can be derived from the skills into a pathway of four practical steps. Finally, we elaborate on how to test this model and bring it into practice.
New perspective in designing e-health tools for self-management
Components of empowerment
A set of six components of empowerment has been reported in the literature on patient empowerment 8 .
Communication: This consists of facilitating patient communications with health professionals.
Education and health literacy: To ensure that people have the ability and motivation to gain access to, understand and use information in ways that promote and maintain good health. Health education is also a way of raising awareness and stimulating self-criticism.
Information: Access to personal medical information furthers patient control in the management of their health. Good-quality, personalised health information can balance the physician-patient relationship by reducing the knowledge asymmetry that has historically formed within this relationship.
Self-care (support): In many routine activities of daily living (e.g. nutrition, physical activity), patients themselves already engage in health management.
Decision aids: To prepare and help patients for making informed decisions about their care options. This can be achieved through problem definition, option and consequence representation, value elicitation and referral to support services (e.g. patient organization).
Contact with fellow patients: To support self-education and individual responsibility, encourages initiative and gives people an opportunity to help others.
Skills as conditions to patient empowerment
A range of skills been identified as one of the empowerment prerequisites 17 . However, the implications for patients and professionals are not always clearly specified18,19 and the implications for patient empowerment have not been stressed as strongly 20 . In this paper, we use the components of empowerment in order to define the set of required skills. Table 1 shows examples of the skills that patients and professionals should acquire, or be exposed to, for each defined empowerment component.
Overview of the empowerment components, and their associated skills of patients and professionals

Patients should be able to communicate their own needs and know what questions to put to health professionals. Professionals should be able to communicate with patients using various channels. Indeed, both patients and professionals benefit from good communication. For example, Cegala et al. 17 have shown that with highly participative patients, physicians have a more patient-centered communication style.
Competencies for information elicitation, comprehension and use are needed. Patients should have the ability and motivation to gain access to, understand and use information in ways that help them for self-management and maintaining good health. Furthermore, they should be able to know how to acquire relevant knowledge. They need skills on how to interpret their own data and on how to acquire insight into their own condition. Thus, there is a need to help patients to bridge the gap between access to information and understanding information so that they can act upon it. We have shown elsewhere21,22 that one way to address this issue is to provide consumers with tailored information that is contextualized and personalized, e.g. directly relevant and easily comprehensible to the person’s own health situation. At the same time, health care professionals should be able to transfer and explain knowledge and information to their patients in an understandable way. By using screening questions, for example, professionals can identify the health literacy level of their patients and accordingly tune the way information is delivered to the patient 23 .
Self-care activities are intrinsic to self-management. In many routine activities of daily living (e.g. nutrition, physical activity), patients themselves already engage in health-management. A wide range of patient skills are associated with the success of this mechanism, ranging from being motivated, coping, self-efficacy and reporting progress 3 , as well as planning and coping planning 24 . The professionals can take on a coaching role here25,26.
Decision-aids prepare patients for making decisions about their care options. Through problem definition, option and consequence representation, value elicitation and referral to support services (e.g. patient organization), decision-aids tools help patients to consciously make informed decisions about care options. On one hand, patients should be able to make decisions and assume some more responsibility. On the other hand, professionals should have relevant knowledge about treatment options and self-management, and should present it to their patients objectively. As O’Connor et al. 27 point out, different decisions require different strategies to communicate risk and support decisions. Both patients and their professionals need to have the ability to weight ‘effective’ versus ‘preference sensitive’ decisions.
Contact with fellow patients advances self-education and individual responsibility, encourages initiative and gives people an opportunity to help others. Patients should have the skills needed to assert themselves; they should have confidence in themselves, and build trust and share empathy for fellow-patients. They need to know how to contact fellow patients and must be able to be critical about information from these non-professionals. Recent research shows that patients have specific needs when searching and sharing information with fellow patients 28 . From the professionals’ perspective, there is a necessity to become familiar with the positive and negative consequences of the various ways of maintaining contacts with fellow patients.
The skills mentioned above can be both general and specific to a given empowerment component. For example, understanding is a skill is associated with several components. The different competences involved in understanding are closely related to education and health literacy, as well as personal information. Problem-solving skills are another example. They involve a wide range of competences that patients need to have in order to manage their health and to overcome problems associated with their health or chronic condition. This includes, for example, not only knowing when, where and how to seek help, but also managing minor ailments without specialised medical assistance.
A number of skills, such as communications skills are relevant to both patients and professionals, while other skills are patient-specific (e.g. self-efficacy) or professional-specific (e.g. coaching).
Design principles for a four step pathway
In the previous sections, we have reported on the components of empowerment and have described the relevant skills as the derived determinants from these components. When one of the skills falls short, self-management will be less effective. Therefore, it is of the utmost importance to explore which skills are relevant to use e-heath tools and to use this insight in developing them. When one of the skills is insufficient, specific solutions should be provided up by the tools.
In this section, we postulate on how design principles can be derived from the determinants into a pathway of 4 practical steps. We use an example of e-health self-management tool to support the measurement of blood pressure in order to illustrate this pathway (see the use case and Table 2).
Overview of the patient’s skills related to the use case
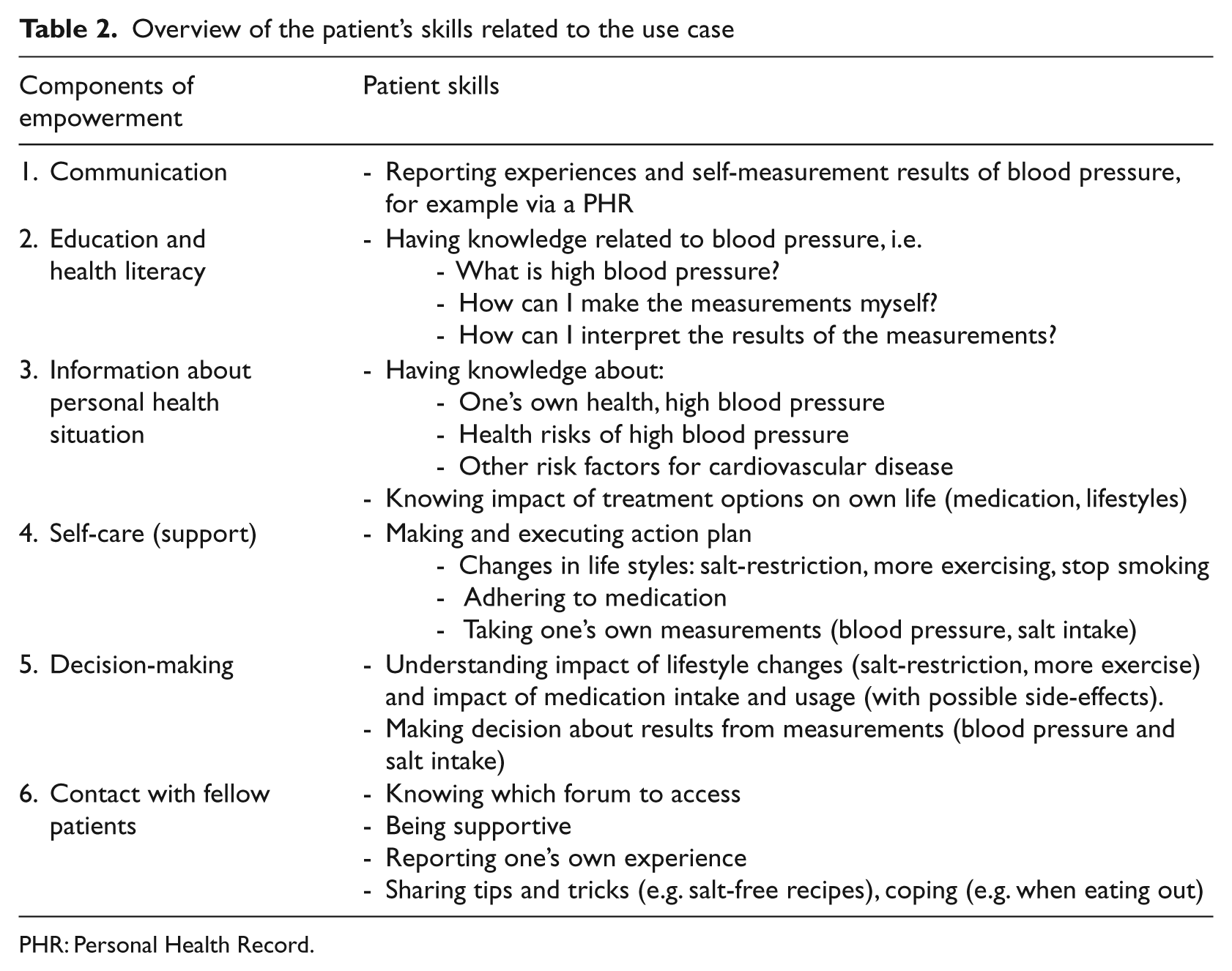
PHR: Personal Health Record.
The use case
Mr Smith has been diagnosed with high blood pressure and this needs to be monitored and controlled. He needs to understand the risk factors involved. More education is needed to enhance the health literacy of the patient so that he can learn what high blood pressure is. The next step involves encouraging the patient to carry out some self-care activities such as taking blood pressure, interpreting the measurements he will make and changes in daily diet. Decisions will be made during this process, alone or in collaboration with the professional. Experiences and stories from fellow sufferers will be of value, for example with regard to the acceptance of the condition, but also in terms of obtaining tips. Communicating with the professional is an intrinsic part of the self-management activities. Mr Smith is asked to report his measurements and his diet changes
Step 1: Specifying the skills needed for the given self-management activity
The first step is to identify the components of empowerment and the skills of patients and professionals that are relevant for the design of an empowerment-based self-management tool. Table 1 can be taken as a starting point. The skills specific to the given self-management activity are elaborated. This can be done, for example in collaboration with patients and professionals, 29 or by using scenarios. In the case of Mr Smith, skills associated with measurements (including the taking and reporting of the measurements, as well as an understanding of the results) are required.
Step 2: Matching the specified skills with the user/ patient profile
This step focuses on determining whether the targeted patients/professionals have enough of the skills specified in step 1. If patients or professionals do not have the required skills, it is then necessary to decide whether and how support can be organized for these skills (see step 3). For example, Mr Smith may have limited skills to formulate his action plan for life style changes.
Step 3: Selecting the alternatives for missing skills
In practice, a tool for self-management will not incorporate all components of empowerment and support all needed skills. Therefore, when support is lacking or insufficient, one must look for alternatives. In some cases, the tool can be extended to include additional support functionalities (for example, graphs or raising the alarm if a measurement is outside the personal guidelines). If this is not possible, alternative means of support, such as educational material and training will have to be found outside the tool. For example, Mr Smith’s understanding of about his health problem may be limited and more education needed so he can learn what high blood pressure is and about the health risks associated with it.
Step 4: Integration in care
This is an important prerequisite for the success and application of the empowerment-based tool for self-management. Adaptations will be required so that the tool can be integrated in the care process. For example, in the case that the measurement of Mr Smith’s blood pressure is high, he should then be able to easily contact his healthcare professional. Preferably, the measurements made by Mr Smith will also have been recorded in the Electronic Patient Record of the healthcare professional so that the appropriate advice can provided to Mr Smith.
Discussion
E-health tools bear the promise of facilitating self-management. We have postulated that these promises can only be captured when the tools are based on patient empowerment components. The components and the coherent skills of patients and professionals have been described. The approach sketched above raises questions with respect to the dynamic fine tuning of a specific set of principles, the proof of concept, automated skills testing to feed the design process, the testing for safety and for efficacy, and the implementation of the e-Health tool.
The first question is: how can one fine-tune a specific set of principles? In other words, how can one specify the design such that it suits a large group of patients and a large group of doctors? How can one personalise these settings? How to proof the principles and the concept? How one can further personalize the specification and realization process by making use of measurement of skills of both the patient and the doctor.
A living lab approach, as commonly used in the field of telecommunications, may be the right vehicle 30 . In a living lab setting, the patients and doctors are confronted with a prototype realization in an early stage of the development process. The gradual upgrading of both the specifications and the realization comes with intensive testing and user feedback. In a living lab setting, the behavioral change of the patient and the doctor can be observed under laboratory conditions. Observation should be fed into the (re-)design process until further improvement does not pay off. Early market introduction with post-market surveillance usually creates a vast amount of user adoption information. The surveillance should involve both patients and doctors.
One may ask if the e-health tool is considered a medical device, as defined by the European Medical Device Directive (MDD) 31 and its recent revision regarding the use of information and communication technology 32 , and its USA equivalents 33 . This question should be put to the legally competent authorities of the countries in which the tools will be used. Regardless of the legal aspects, the European MDD provides a very elaborate framework with respect to safety management.
Efficacy can be tested in a controlled trial with a double trial group of patients and doctors and a double control group, also with patients and doctors. The latest insight in testing behavior change should be included to ensure that the chosen intervention is well described34–38. Finally, the implementation of an e-health tool for self-management should clearly specify the characteristics of the internet-based intervention associated with the tool using, for example, the framework for the development of a science of internet-based interventions proposed by Webb. 39
Conclusion
E-health holds the promise of delivering healthcare at a low cost, while services can be tailored to the specific needs and capabilities of patients and doctors. It is a promise which is not yet fully realised. To quote Sir William Henry Bragg, who won the Nobel Prize for Physics in 1915: “The important thing in science is not so much to obtain new facts as to discover new ways of thinking about them”. This notion triggered our thinking about designing the next generation e-health tools to support patients in self-management. We postulated a pathway to comply with the design principles and build on components of patient empowerment drawn from literature. We call on the scientific community, in collaboration with healthcare partners, to work on this new pathway.
Footnotes
None.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.