
Abstract
Background and Aims:
Ductal carcinoma in situ (DCIS) is a non-invasive form of breast cancer with increasing incidence in recent decades. Early detection and accurate staging of DCIS are crucial for determining the appropriate treatment approach, with breast-conserving surgery (BCS) being the standard when feasible. The role of preoperative magnetic resonance imaging (MRI) in DCIS remains controversial, particularly in relation to its potential to identify incidental findings that may influence surgical decisions. This study aims to evaluate the clinical value of preoperative MRI in patients with pure DCIS, focusing on its impact on surgical management and the potential influence of incidental findings on mastectomy rates.
Material and Methods:
A retrospective review of 91 patients with pure DCIS who underwent preoperative MRI between 2014 and 2019 at Tampere University Hospital, Finland. Patients were divided into two groups: “No incidental MRI findings” and “Incidental MRI findings” with the latter leading to further imaging and biopsies. Surgical approaches and the time delay between diagnosis and surgery were compared. Tumor sizes estimated by MRI, mammography, ultrasound, and histopathology were assessed for correlation.
Results:
Incidental MRI findings were identified in 22% of patients, with a higher mastectomy rate in “Incidental MRI findings” (65.0%) group compared to the “No incidental MRI findings” (41%) group. Despite the higher mastectomy rate in the “Incidental MRI findings” group, most incidental findings were benign. The evaluated mean tumor size was largest on MRI (48 mm) compared to mammography (32 mm) and ultrasound (27 mm). MRI was found to overestimate tumor size, unlike mammography and ultrasound. No significant difference in the delay between MRI and surgery was observed between the two groups.
Conclusions:
In DCIS, incidental findings on MRI were associated with higher mastectomy rate, but overtreatment or unnecessary mastectomies were not detected. MRI may assist surgical decision-making in patients with pure DCIS.
Keywords
Introduction
Ductal carcinoma in situ (DCIS) is a heterogeneous disease characterized by malignant epithelial cells originating in the terminal duct lobular unit, but without crossing the basement membrane. DCIS is considered the earliest form of breast cancer and a precursor to invasive breast cancer (IBC). According to various studies, concomitant DCIS is associated with IBC in 21%–77% of cases. 1
The incidence of pure DCIS (i.e. with no invasive component of cancer) has risen significantly over the past few decades.2,3 In Finland, the incidence increased from 236 cases in 2001 to 595 cases in 2023. In 2023, there were 5214 breast cancer diagnoses in Finland, with pure DCIS accounting for approximately 11% of these cases. 4
In most patients, surgical treatment of DCIS is curative. Both European Society of Medical Oncology (ESMO) and National Comprehensive Cancer Network guidelines (NCCN) recommend breast-conserving surgery (BCS) when the DCIS can be removed completely with a healthy tissue margin and acceptable cosmetic result, and if radiotherapy can be given. In contrast, when the DCIS lesion is extensive or multicentric, mastectomy is generally mandatory. In this decision-making, it is essential to have as accurate imaging modalities to estimate the DCIS extent.5–7
The golden standards in breast cancer diagnostics are mammography and ultrasound combined with core needle biopsy. Sensitivity of mammography varies between 47% - 98%.8,9 Magnetic resonance imaging (MRI) is a second-level diagnostic imaging that supplements mammography and ultrasound. The sensitivity of MRI in breast cancer outperforms both mammography and ultrasound, especially in invasive lobular breast cancer and in patients with dense breast parenchyma.10,11 The diagnostic accuracy of MRI in pure DCIS is less clear. Due to the morphologic features of DCIS, the sensitivity of MRI is more variable compared to invasive cancer and ranges from 20% to 95%.11–14 Furthermore, MRI may also detect incidental lesions that need to be biopsied despite being benign (i.e. false-positive findings, incidental findings).9,15 This can lead to unnecessary examinations and psychological stress for the patient.10,16 Moreover, when additional examinations (second-look ultrasound ± biopsies) are needed after a breast MRI, treatment can be delayed.
There are several studies comparing MRI to mammography and/or ultrasound examination, and histopathological findings, especially in relation to size estimation. These studies show that there is difference in size assessment in different subtypes of breast cancer. If the size of the tumor is overestimated, it can lead to unnecessary initial mastectomies, and if it is underestimated, re-excision rates grow higher.11,15,17–21
The aim of this study was to state the clinical value of preoperative MRI in patients with DCIS without pre- or postoperative evidence of invasive tumor components, with a specific focus on determining the impact of MRI and potential incidental findings on the mastectomy rate.
Methods
At Tampere University Hospital in Finland (catchment area of 530,000 people), approximately 3300 women were diagnosed with breast cancer from 2014 until the end of 2019. All patients with new breast cancer diagnosis are handled at a multidisciplinary breast meeting, that is attended by breast radiologists, pathologists, oncologists, and surgeons. The treatment plan is decided in these meetings and documented in electronic patient records. At the unit a preoperative fast-track process is used, which is an institutional protocol for breast cancer patients with the purpose of minimizing waiting times through effective multidisciplinary workup, streamlined scheduling, early risk assessment via home questionnaires, and pre-admission planning to avoid last-minute issues.
We retrospectively reviewed the electronic patient records of all breast cancer patients, who underwent breast MRI during this period (n = 1878 patients). Inclusion criteria to the present study were: (1) breast MRI performed after mammography and ultrasound and (2) patients with histopathological confirmation of pure DCIS both in the preoperative core needle biopsy and in the postoperative histopathological analysis, without evidence of an invasive breast cancer.
Included patients were further classified in two groups based on breast MRI findings. In the “No Incidental MRI findings” group, surgery was performed with no further imaging, and in the “Incidental MRI findings” group, breast MRI showed incidental findings resulting in second-look imaging (mammography, ultrasound) and new biopsies.
The time delay between diagnosis and operation was analyzed comparing the two groups. In addition, the accuracy of breast tumor size estimation was compared in MRI, mammography, and histopathological measurements.
Each mastectomy case was re-evaluated based on the definitive postoperative histopathological data, and if the decision of original surgical treatment changed from mastectomy to BCS, mastectomy was considered overtreatment.
All statistical analyses were performed using IBM SPSS (Version 28.0.1.1, IBM Corp., Armonk, NY). p values of ⩽ 0.05 were considered statistically significant. Descriptive data is reported as means and standard deviation. The agreement of tumor size measurements between histopathological analysis and different imaging modalities was assessed using Bland–Altman analysis. For each paired observation, the difference between the methods was plotted against their average. The mean difference (bias) was calculated to quantify systematic errors.
This study was approved and the need for informed consent was waived with research permission granted by the Institutional Review Board of Tampere University Hospital (study number R20631) according to the national laws and regulations.
Results
Clinical characteristics
Ninety-one DCIS patients fulfilled the inclusion criteria (4.8% of all breast MRI patients). Out of these 71 patients in the “No incidental MRI findings” group with a mean age 57 (29–80) years. Twenty patients with a mean age 54 (32–74) years were in the “Incidental MRI findings” group and underwent additional examinations. In “No incidental MRI findings” group, the median delay from MRI to initial surgery was 57 days (range, 19–120 days), and in the “Incidental MRI findings” group it was 64 days (range, 21–75 days). There was no significant difference in the delay from MRI to surgery between the two groups.
The location and histopathology of the MRI-detected incidental findings in the 91 study patients are shown in Table 1. Approximately half of the incidental findings were in the ipsilateral breast, with two occurring in the same quadrant and nine in other quadrants. Eight of the incidental findings were found in the contralateral breast. In one case the abnormal MRI finding was a lymphoma in the neck area. In incidental findings of the breast, histopathology was benign in 14 cases, and malignant in 6 cases.
Clinical outcome of 91 study patients between “No incidental MRI findings” (N = 71) and “Incidental MRI findings” (N = 20).
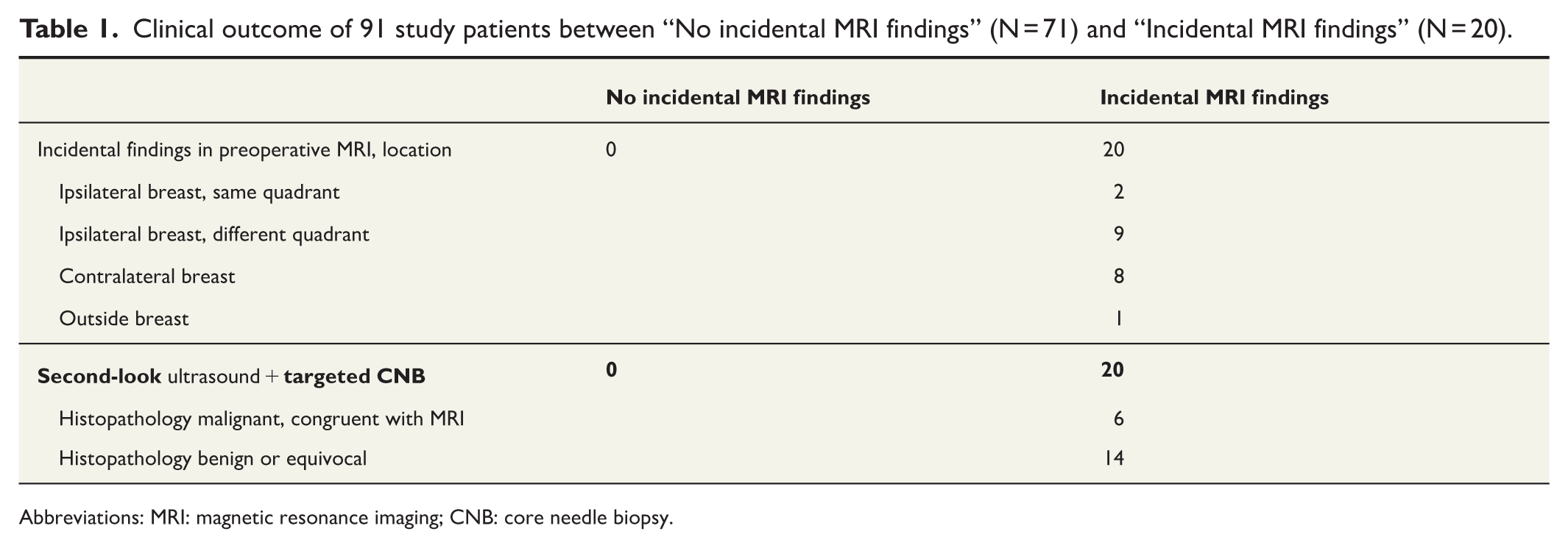
Abbreviations: MRI: magnetic resonance imaging; CNB: core needle biopsy.
Surgery
The differences in surgical approach between these two groups are shown in Table 2. Breast-conserving surgery was performed in 42 (59%) and 7 patients (35%) in the “No incidental MRI findings” and “Incidental MRI findings” groups, respectively.
The differences in surgical approach between study groups.
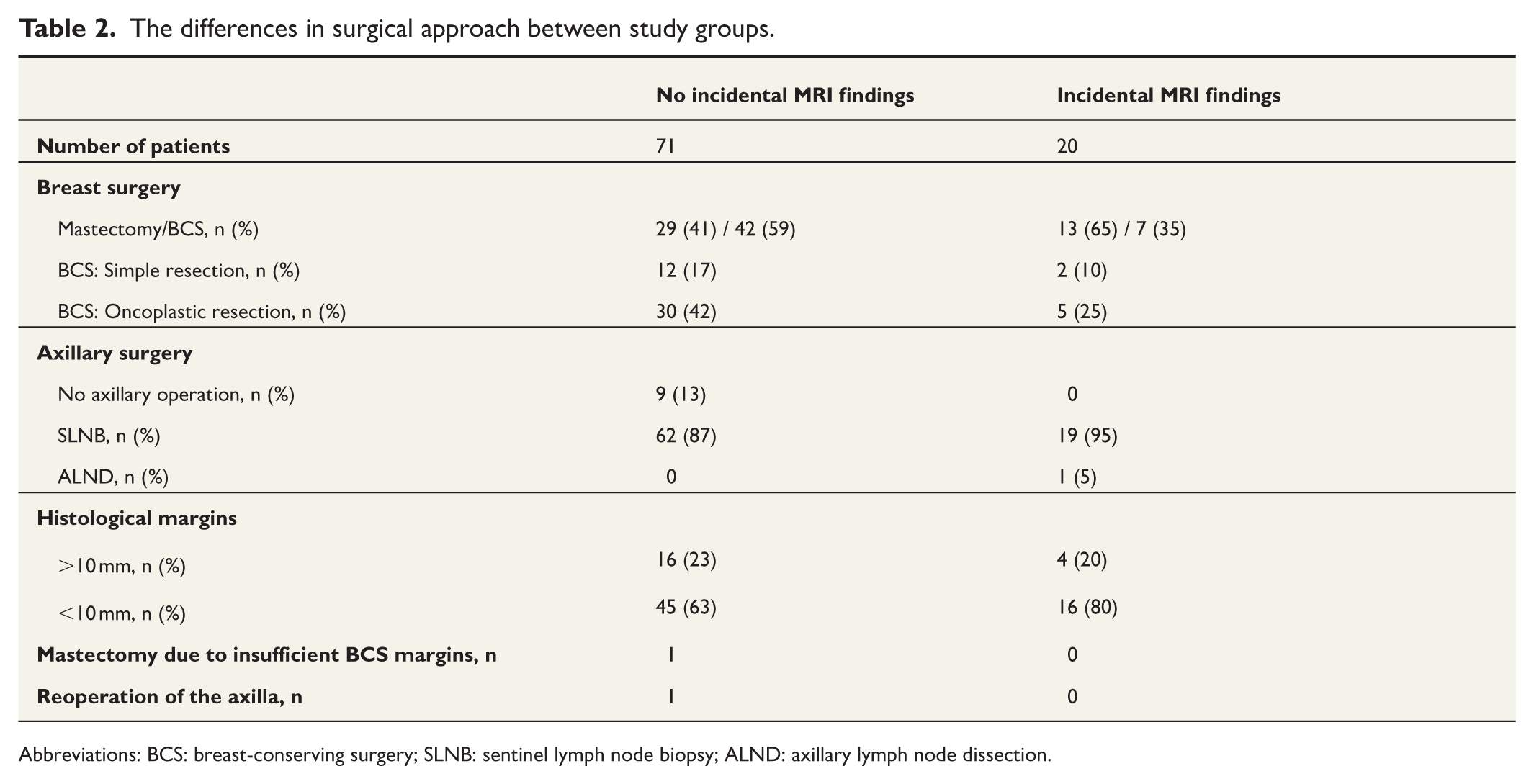
Abbreviations: BCS: breast-conserving surgery; SLNB: sentinel lymph node biopsy; ALND: axillary lymph node dissection.
Patients with incidental findings were more likely to have a mastectomy than patients with no incidental findings, even though most of the incidental findings were benign. The total number of mastectomies was 29 (41%) in “No incidental MRI findings” and 13 (65%) in “Incidental MRI findings.” When each mastectomy case was re-evaluated based on the definitive postoperative histopathological data, each initial surgical treatment was considered correct, and thus no mastectomy was considered overtreatment.
One patient in the “No incidental MRI findings” group needed a re-operation due to insufficient margins after BCS, and one needed an axillary lymph node clearance because of sentinel node metastasis. In the “Incidental MRI findings” group, no re-operations were needed.
Tumor size agreement
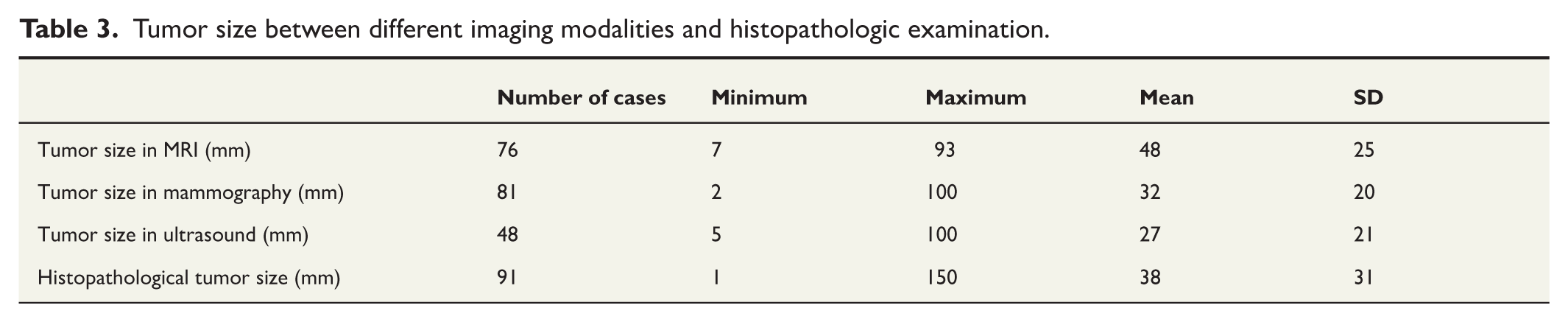
Tumor sizes in different imaging modalities and in histopathologic examinations are shown in Table 3. MRI overestimated the tumor size, unlike mammography and ultrasound, but no imaging modality showed all DCIS findings observed in the histopathological examination. Mammography showed 89% of the lesions (measurement 2–100 mm, mean 32 mm) confirmed by histopathology, meaning that 11% of the lesions were not visible in mammography. In MRI, 84% of the lesions were visible (measurement 7–93 mm, mean 48 mm), and only 52% of the lesions were visible in ultrasound (measurement 5–100 mm, mean 38 mm). In the histopathological examination, tumor sizes varied from 0.6 to 150 mm (mean 38 mm).
Tumor size between different imaging modalities and histopathologic examination.
In the Bland–Altman analysis, the mean difference (bias) was 6 mm between histopathology and MRI, indicating minimal systematic error. The mean difference (bias) was 6 mm between histopathology and mammography, and 16 mm between histopathology and ultrasound. Visual inspection of the Bland–Altman plot suggested a slight proportional bias, as differences tended to decrease with increasing average values (Fig. 1).
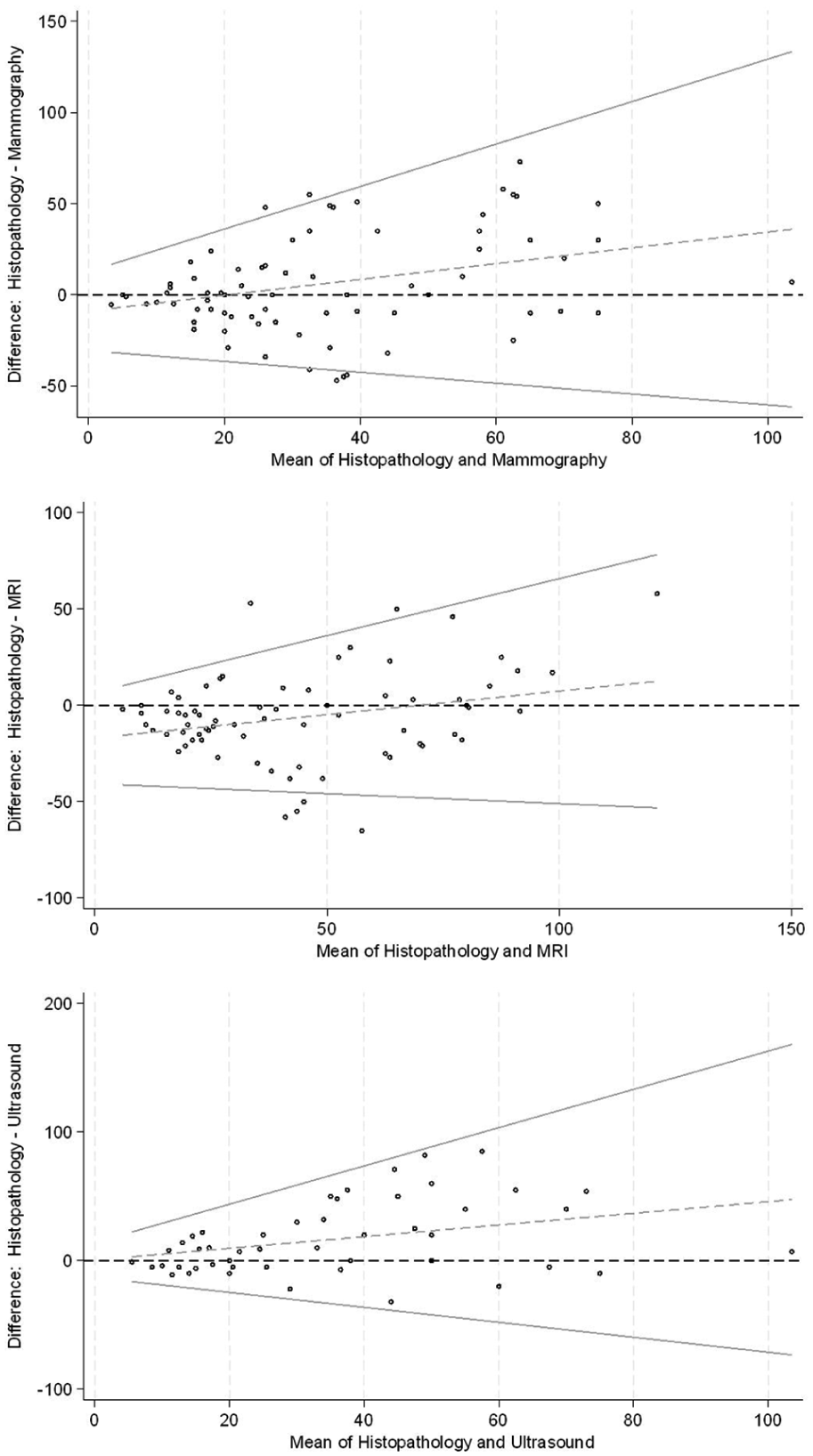
Bland–Altman plots evaluating the agreement of tumor size measurements between histopathological analysis and each imaging modality.
Discussion
In this study, incidental MRI findings were detected in 22% of patients with pure DCIS. The mastectomy rate was higher in these patients (65%) compared to those with congruent findings in MRI and mammography (41%). This result is reasonable and expected, as additional cancer foci increase the tumor-to-breast volume ratio and multifocality, leading to more radical surgery and thus a higher mastectomy rate.
Pure DCIS is an early breast cancer confined to the milk ducts without infiltration beyond the basement membrane. DCIS cannot metastasize and therefore has an excellent long-term prognosis, with a cancer-specific survival rate of around 98% after 10 years follow-up. 22 However, due to its growth pattern, DCIS commonly appears as diffuse non-mass enhancement without clear visible borders. If such a lesion is extensive or multicentric, mastectomy is the treatment of choice when standard BCS or oncoplastic surgery is expected to result in a poor aesthetic outcome. This is most evident in patients with small breasts.
The risk of overtreatment has been a primary concern regarding high-sensitive breast MRI, as MRI alone may alter treatment planning toward a more radical approach.23,24 The conversion of attempted BCS to mastectomy is justified if additional malignant lesions are verified histopathologically and if treatment decisions are discussed by a multidisciplinary team (MDT). MRI-only visible incidental lesions represent a particular multidisciplinary challenge. All 20 of the present patients with incidental MRI finding underwent second-look ultrasound, ultrasound-guided biopsy when possible, and further discussion in the MDT meeting. Notably, only 6 of 20 incidental MRI findings were histologically true positives for additional cancer lesions, whereas 14 findings were benign or equivocal. According to accurate retrospective evaluation, no mastectomy was however judged to be overtreatment, and BCS was not an option in these cases.
All imaging modalities tend to either underestimate or overestimate the extent of DCIS compared with its true size. In this context, “true size” or reference size is defined as the size of the lesion measured microscopically in histopathological examination by an experienced pathologist. Mammography may underestimate the extent of microcalcifications in very dense breasts, resulting in insufficient resection, insufficient margins, and reoperations. 25 Ultrasound is less sensitive than mammography in detecting pure non-mass DCIS. 26
MRI may also underestimate the size, particularly in low-grade DCIS. On the other hand, overestimation in MRI may increase the risk of unnecessary mastectomies and overtreatment in high-grade DCIS. MRI is most likely to over-represent the size of less dense, diffuse DCIS lesions. 13 In this study, the mean size of DCIS was 48 mm on MRI and 38 mm in histopathological examination. The difference can be significantly higher in individual cases. It should be highlighted that MRI is obtained in the prone position, causing an accordion effect by stretching the breast, which may explain the difference between MRI and histopathological size. 27 The specimen also tends to shrink during the fixing process. If the MRI size estimation would alter treatment planning, additional biopsies and MDT management are recommended.
Achieving clear surgical margins of at least 2 mm is crucial to avoid local recurrence. 28 In this study, BCS was used in 54% of all patients with pure DCIS. Only one patient of 49 needed reoperation due to insufficient margins. BCS combined by radiotherapy is preferable in DCIS, as it provides an equal 10-year breast cancer-specific survival compared to mastectomy. 29 Twenty-three of the present 42 mastectomy patients underwent immediate breast reconstruction, and delayed reconstruction will be an option for the rest. If mastectomy is necessary, immediate breast reconstruction should always be offered, as neither adjuvant therapies nor radiotherapy are needed in pure DCIS. Furthermore, only a single operation is needed, and the aesthetic result is usually optimal. Thirty-five of 49 BCS patients in the present study were operated on using oncoplastic techniques. This is a good alternative to mastectomy when the DCIS lesion is extensive and if traditional resection would lead to a suboptimal aesthetic outcome.
It has been stated that MRI causes extra delays to surgery. 30 This delay results from the MRI itself, second-look ultrasound, ultrasound-guided or MRI-guided core needle biopsy and waiting for the histopathological report. Because pure DCIS is associated with an excellent prognosis and no adjuvant therapies are expected, an extra delay of a couple of weeks does not impact the outcome. However, any extra delay is a psychological burden for a cancer patient. In this study, we found no significant difference in delay between patients with incidental MRI findings and those without. Extra delays can be avoided by an effective fast-track process as used at the authors’ institution.
We found in our study that preoperative breast MRI is a useful tool for local staging in DCIS, explaining the very low reoperation rate of 1.1%. A recent study by Cozzi and colleagues conducted a subanalysis of the database of the Multicenter International Prospective Analysis (MIPA) study and compared two matched groups of 309 DCIS patients, one of whom had undergone preoperative MRI, and one of who had not. 31 They found that MRI increased the number of mastectomies as the first-line management, but by allowing better treatment planning, it reduced the reoperation rate (10% vs 22%), and MRI did not significantly increase the definitive total mastectomy rate compared to controls. 31
Despite its benefits, preoperative MRI should not be used indiscriminately in all patients with pure DCIS. Complementary imaging studies cause extra costs and increased workload for the entire breast cancer team. Unselective use of MRI may result in overtreatment of low-risk DCIS with indolent disease. The key question is to identify those DCIS patients who would benefit most from MRI. The present study cannot provide a definitive answer to this question, but in our experience, MRI is indicated in borderline cases where patients have extensive microcalcifications on mammography, but where BCS still may be an option. MRI can assist in decision-making and provide useful information, especially in young patients with dense breast parenchyma and indistinct findings in mammography. The benefit of MRI may be more significant in high-grade DCIS. This is in accordance with three systematic reviews based on observational cohort studies, which generally emphasize the usefulness of preoperative MRI in young patients with extensive and high-grade DCIS.7,32,33 In the multidisciplinary practice, the radiologist’s role in interpreting MRI images is important, as well as the MDT meeting in conveying this information to the surgeon.
This study has several limitations, such as selection bias. In a retrospective setting, MRI has been used based on non-specific indications, and our study patients cannot be generalized to all patients with pure DCIS. This selection bias is an obvious explanation for our high overall mastectomy rate (46%), but it cannot be concluded that breast MRI increases mastectomy rate in general; it can only be concluded that incidental MRI findings are associated with the increase. In addition, we were unable to analyze low-grade and high-grade DCIS changes separately due to missing data. This study also lacks a control group of patients with pure DCIS who have not undergone MRI.
Conclusion
This study demonstrates that preoperative breast MRI can be a valuable tool in the local staging of ductal carcinoma in situ (DCIS), providing essential information that can guide treatment decisions. However, incidental findings on MRI were associated with a higher mastectomy rate, despite many of these findings being benign or equivocal. The increased mastectomy rate in patients with incidental MRI findings highlights the importance of careful decision-making and thorough multidisciplinary discussion, as unnecessary mastectomies can result from over-interpretation of MRI findings. MRI can help identify additional lesions and guide more precise treatment planning. Overall, preoperative MRI aids in minimizing the need for reoperation and optimizing treatment strategies, but it must be applied thoughtfully to avoid overtreatment and unnecessary delays in surgery.
Footnotes
Acknowledgements
We express our gratitude to Otso Arponen, MD, PhD, for his valuable comments regarding the research and to Heini Huhtala, MSc, for the statistical assistance.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
This study project was approved and the need for patients’ consent was waived by the institutional review board of Tampere University Hospital (study identifier: R20631).
Informed consent/Patient consent
N/A.
Clinical trial registration number/date
N/A.