
Abstract
Background:
The surgical management of breast cancer involves either modified radical mastectomy or a conservative approach. Breast-conserving surgery is the preferred surgical treatment for early breast cancer in developed countries, while mastectomy is still more favoured by most centres in developing countries.
Objectives:
To report some quality data on breast cancer surgeries from a sub-urban tertiary hospital in Nigeria.
Design:
Retrospective analysis
Methods:
We retrospectively reviewed all breast cancer surgeries performed between January 2018 and December 2022 at the Irrua Specialist Teaching Hospital.
Results:
A total of 105 female patients underwent breast cancer surgery. Their ages ranged between 27 and 85 years, with a mean of 48.8 years (SD = 12.2). The mean duration of symptoms before presentation was 12.3 ± 17.8 months (1-120 months), with 15.2% presenting with stage I and II disease and 84.7% presenting with stage III and IV disease. Invasive carcinoma NST was the most common histological type in 78 (74.3%) patients. The cancers were predominantly high grade (42.3%) and triple negative (41.5%). Only 9.5% of the patients had breast-conserving surgery, the others had mastectomy. Sixty-three patients (60%) received neoadjuvant chemotherapy while only 25.7% of patients had documented evidence of the completion of adjuvant radiotherapy.
Conclusion:
The rate of breast-conserving surgery in this study was extremely low. This could be attributed to the advanced stage at presentation, predominance of aggressive tumours, limited access to radiation therapy, status of the medical system, and patient preferences.
Introduction
The management of breast cancer has evolved significantly, transitioning from radical mastectomy, introduced by Halsted with its modifications, to various forms of breast-conserving surgery (BCS), which allows for the removal of cancerous tissue while preserving the breast. 1 The change has been attributed not only to a better understanding of the disease at the molecular level but also to major advancements in the fields of adjuvant radiotherapy, chemotherapy, hormonal therapy, and immunotherapy. Breast-conserving surgery with radiation therapy (BCT) has become the preferred approach for early-stage breast cancer in developed countries due to its comparable survival outcomes to modified radical mastectomy (MRM),2,3 making it imperative to educate both professionals and the public about its benefits.
Surgical treatment rates for breast cancer vary widely across Africa, with countries like Nigeria showing rates as low as 35.2% while Cameroon reports 100%. Most countries fall within the range of 48% to 75%.4-8 These differences are influenced by patient factors and available resources. In Nigeria, low surgery rates result from advanced tumour stages, financial barriers, and patient hesitance towards surgery. 8
Modified radical mastectomy remains the most common procedure in sub-Saharan Africa, with some centres reporting rates well above 50%, and many exceeding 90%.5,8 Breast-conserving surgeries are not common in this region due to late-stage diagnoses of invasive cancer.4,7 The delayed diagnosis of breast cancer in Nigeria may be due to the poor awareness about breast cancer screening and the lack of organised screening programmes.9,10 For example, in a study of more than a thousand women in a Nigerian community, only about 20% of the women had received a clinical breast examination, with most not having one in the past year. Only 2.3% reported ever having a mammogram. 11
Additionally, the use of multimodal treatment involving a combination of chemotherapy, surgery, and radiation therapy is low in Nigeria. 12 This is due to the paucity of radiotherapy services and financial constraints that limit access to many adjuvant therapies. Health care spending in Nigeria is primarily paid out-of-pocket, with only about 5% of the population covered by the National Health Insurance Scheme. 13 As a result, there is a decline in the rate of BCS.
The review focused on providing quality data regarding breast cancer surgeries conducted at a suburban tertiary hospital in Nigeria.
Materials and Methods
This was a retrospective review carried out at Irrua Specialist Teaching Hospital, a tertiary health care centre located in Irrua, Esan Central LGA, Edo State, Nigeria. The facility receives referrals from other parts of Edo and neighbouring states. Most of the people accessing the facility live in the rural communities of the central and northern parts of Edo State. The study was approved by the Health Research and Ethics Committee of the Irrua Specialist Teaching Hospital and the requirement for informed consent to participate has been waived by the Ethics Committee.
Inclusion criteria
All female patients who underwent either breast-conserving surgery or modified radical mastectomy between January 1, 2018, and December 31, 2022, were included.
Exclusion criteria
Patients who did not undergo surgery, for example, patients with nonresectable cancers, those who defaulted surgery, and those who died while on neoadjuvant chemotherapy (NACT). We also excluded patients with incomplete data.
Data collection
The data were collected from patient case files obtained from the hospital’s medical records department. We recorded the demographic data and clinical information of the patients, which included age, presenting symptoms and duration, clinical characteristics of the tumour, nodal status, histological diagnosis, receptor status, tumour stage at presentation, type of surgery (BCS or MRM), and whether they received chemotherapy and/or adjuvant radiotherapy. Stage of disease at presentation was reported according to the American Joint Committee on Cancer Manual, 7th Edition. 14 Metastatic work-up consisted of a chest x-ray and abdominal ultrasound in accordance with institutional protocol and international resource-stratified guidelines.15,16 Surgical treatment was provided following established principles. Neoadjuvant chemotherapy was administered based on the National Surgical Adjuvant Breast and Bowel Project (NSABP) protocols B-18 and B-27, 17 while adjuvant chemotherapy followed the ‘St Gallen guidelines’. 18 Although anthracycline-based chemotherapy and taxanes were available options, some patients faced financial constraints that prevented them from accessing taxanes. Hormonal and targeted therapies were offered to patients who could afford them.
Statistical analysis
The data were entered into a predesigned proforma and analysed with Statistical Product and Service Solutions (SPSS) software version 25. Continuous variables were shown as the mean ± standard deviation (SD), and categorical variables were reported as frequencies and percentages. The sociodemographic and clinicopathologic characteristics of patients in the BCS and mastectomy groups were compared using chi-square tests or Student t test. Pearson correlation was used to assess the relationship between marital status, level of education, occupation, and stage of the disease. Statistical significance was set at a P < .05 with a confidence level of 95%.
Results
Data from 168 breast cancer patients were collected during the study. Of these, 105 patients who had undergone either BCS or mastectomy were included, while 63 patients were excluded (Figure 1). The mean age of the participants was 48.8 years (SD = 12.2), with the youngest being 27 years old and the oldest 85 years old.

A flow diagram depicting the patient enrolment process in the study and the different surgical procedures performed.
Modified radical mastectomy accounted for 86.7% of the surgeries performed. Only 9.5% had breast-conserving surgery, while the others (3.8%) had simple or toilet mastectomy. The BCS procedures included wide local excision (60%), segmentectomy (30%), and quadrantectomy (10%). Wide local excision entails the removal of the tumour and a small margin of healthy tissue. Segmentectomy involves the removal of a segment of the breast containing the tumour, while quadrantectomy involves the removal of one-quarter of the breast along with the tumour. In this study, 10.5% of patients had BCS in 2018, 10% in 2019, 5.6% in 2020, 9.5% in 2021, and 11.1% in 2022, with an overall BCS rate of 9.5% over the 5-year period.
Among all participants, 67 (63.8%) were married. The most common occupation among them was trading (41.0%), and 37 (35.2%) had secondary education. However, 15 (14.3%) had no formal education. There were no significant differences in the sociodemographic characteristics of the patients in either group (Table 1).
Sociodemographic characteristics.

Abbreviations: BCS, breast-conserving surgery; T, t test; SD, standard deviation.
Fifty-seven (54.3%) patients had tumours in the right breast, while 48 (45.7%) had tumours in the left breast. The most common tumour location was in the upper outer quadrant (39.0%), followed by the central or subareolar area (31.4%), as shown in Figure 2. The mean duration of breast lumps prior to presentation was 12.3 ± 17.8 months (1-120 months). The tumours were clinically larger than 5 cm in 80% of the patients, and 34 (32.4%) patients had ulcerated masses (Table 2). Mastectomy was linked to larger tumours (>5 cm) compared with BCS, which was associated with smaller tumours (2-5 cm) (P = .004). Mastectomy was more common in cases with ulceration (P = .028). Clinically, axillary node involvement was observed in 78 (74.3%) patients, while 3 (2.8%) patients had palpable supraclavicular lymph nodes.

A pie chart showing the location of tumours in the different areas of the breast.
Clinicopathological characteristics.

Abbreviations: BCS, breast-conserving surgery; HER 2, human epidermal growth factor receptor 2; HR, hormone receptor.
Only 1.9% and 13.3% of patients had stage I and II disease, respectively. Fifty-nine percent (62/105) of patients had stage III disease, with the majority (75.8%) having stage IIIB disease, while 25.7% (27/105) had stage IV disease. Mastectomy was more common in patients with advanced stage disease compared with those with early-stage disease (P = .030). Out of the 57 patients with Nottingham histological grading, 17.5% had low-grade disease (grade I), 40.3% had intermediate-grade disease (grade II), and 42.1% had high-grade disease (grade III). Mastectomy rates were higher for tumour grade II and III while BCS rates were higher for tumour grade I (P < .001).
In this study, patients who received NACT (63 patients) were more likely to undergo mastectomy (61 patients, 64.2%) than BCS (2 patients, 20%), P = .013.
Immunohistochemistry (IHC) results were available for 41 (39.0%) patients. Of these, 34.1% were oestrogen receptor (ER) positive, 26.8% were progesterone receptor (PR) positive, and 24.4% were human epidermal growth factor receptor (HER-2) positive. In combination, 12 (29.3%) were HR+/HER2−, 3 (7.3%) were HR+/HER2+, 9 (21.9%) were HR−/HER2+ (HER2-positive) and 17 (41.5%) were HR−/HER2− (triple-negative or basal-like), of which 10 (58.8%) were younger than 50 years. The molecular subtypes did not influence the choice of procedure.
The marital status, level of education, and occupation of patients showed weak correlation with the stage at presentation (Table 3).
Correlation of stage of disease with marital status, level of education, and occupation.

The main sites of metastasis were the lungs (10, 36%), brain (6, 21%), liver (3, 11%), spine (3, 11%), and other bones (3, 11%), as shown in Figure 3. The histological profile of the patients is shown in Figure 4. Invasive carcinoma no special type (NST) was the most common histological type in 78 (74.3%) patients.
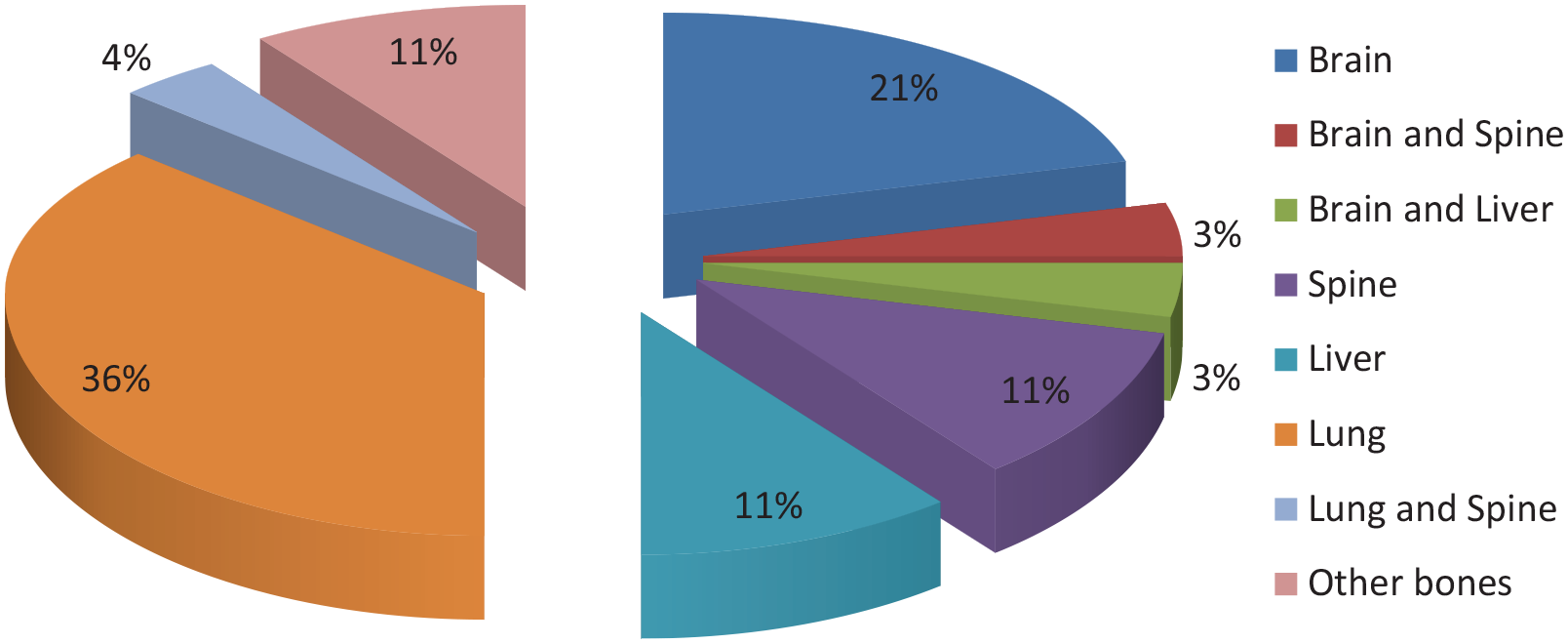
A pie chart showing the different sites of metastasis from breast cancer and their corresponding percentages.

A bar graph illustrating the 2 surgical treatment options for breast cancer in the study and the different histologic types based on the WHO classification of tumours of the breast Fourth Edition, 2012.
The patients were referred to radiation oncologists at other centres/states for adjuvant radiotherapy, and only 27 out of the 105 patients (25.7%) reported evidence of completion of radiotherapy. Others were lost to follow-up in our facility.
Discussion
This study reviewed 105 patients with breast cancer who underwent surgical treatment. Most breast cancer surgeries were mastectomies, with an extremely low rate of breast-conserving surgeries. The overall BCS rate of 9.5% in this study is consistent with rates reported in other studies in Nigeria.8,19,20 In Europe, the rates of mastectomy and breast conservation are reported as 30% and 70% respectively, while in Africa, the mastectomy rate is much higher at 85%. 21 The low BCS rates in low- and middle-income countries (LMICs) stem from late-stage at presentation and inadequate diagnostic resources. 22
Breast cancer in many developing countries is often diagnosed at an advanced stage, with patients presenting with large tumours, and multiple lymph nodes as observed in this study. 8 A significant number of patients in this study (62.9%) sought medical attention only after experiencing symptoms for over 6 months, with an average illness duration of 12.3 months. Similar delays have been reported in other local studies.8,20,23 Reasons for delayed presentation include fear of mastectomy, ignorance, reliance on spiritual beliefs, and the use of herbal remedies. 23 These factors may explain why a high percentage of our patients (59%) presented with stage III disease and 25.7% with stage IV disease leading to a higher incidence of mastectomy. These findings align with similar studies conducted locally.9,20,23
The late presentation of the disease in LMICs is worsened by a lack of awareness of breast cancer. Population-based mammographic screening is not commonly used in LMICs, leading to women often detecting their disease only after palpable lump or other advanced symptoms have appeared. 24 Even after the lump is detected, there is a significant time gap before a medical consultation is sought. Over 50% to 70% of women present with advanced-stage disease, requiring mastectomy as the primary surgical option. 25
In this study, 2 patients with stage IIIB tumours received NACT to downstage the tumours before being offered BCS. Studies have shown that BCS can still be a feasible option for patients with stage III tumours following successful downstaging with NACT.26,27 However, our study found a high rate of mastectomy after NACT, possibly due to factors such as advanced disease stage, large tumour size, poor response to chemotherapy, patient noncompliance, logistical challenges with radiotherapy, and individual preferences of surgeons and patients.
Nottingham grade data was not available for 45.7% of patients. Among the available data, 42.1% were categorised as high grade, which aligns with results from a previous study in Nigeria. 20 Tumour grades II and III were associated with a higher rate of mastectomy in this study, consistent with the findings of Garcia-Etienne et al. 28 Young African women often have more severe forms of the disease due to higher grade and late diagnosis. Triple-negative breast cancers, associated with poor prognosis, were found in 41.5% of patients in our study, aligning with a study from East Africa where 34% had triple-negative tumours. 29 This is higher than the 12% reported in a European study. 30 HER 2-positive breast cancers were present in 21.9% of cases, often associated with aggressive disease and higher mastectomy rates. The local recurrence risk is higher for HER 2-positive and triple-negative cancers than for ER+/PR+ cancers. 31 The lack of a significant association between the molecular subtypes and the type of surgery in our study may be attributed to the small percentage of patients who underwent immunohistochemistry.
The limited access to radiotherapy in developing countries is a significant factor contributing to the low percentage of BCS. 19 In our study, < 30% of patients received adjuvant radiotherapy, which is even greater than the <10% reported by Olasehinde et al 9 in Ile Ife, Nigeria. This is a common problem in Nigeria, where there are few radiotherapy centres serving a large population, and as such, the machines are overstretched, frequently breaking down and resulting in long waiting lists. Consequently, several patients are unable to access radiotherapy services for financial and logistic reasons, while many others are lost to follow-up after referral, as may have happened in our case. This may result in reluctance among surgeons to perform BCS. Some patients who are eligible for BCS from a surgical perspective may opt equally for a mastectomy to avoid undergoing radiotherapy.
Patient choice is a critical factor when deciding between MRM and BCS. Patients are encouraged to actively participate in the decision-making process when choosing their surgical treatment. While European data shows that over 70% of patients prefer BCS, 28 local experiences indicate a high acceptance rate for mastectomy due to misinformation, misconceptions, and exaggerated fears. 32 Factors such as access to healthcare facilities, financial constraints, and societal influences also play a role in patient’s decision-making process. In Nigeria, where most healthcare expenses are paid out-of-pocket and health insurance coverage is limited, 13 patients with low socioeconomic status may face challenges in accessing timely treatment and adhering to recommended care. This pattern is also reflected in the outcomes of breast cancer cases in Nigeria. Research showed a 5 year overall survival rate of 25.6%, with rates of 45% for stage II, 15% for stage III, and 5% for stage IV. The median survival time was 30 months. 33 Improved survival rates are linked to multimodal treatment or early detection. 12
Limitations of the Study
The study is retrospective and single hospital-based, so the results need to be generalised with caution. The unavailability of facilities for immunohistochemical studies in our centre is also a challenge to us, as seen with the limited number of patients with IHC data in the study.
Conclusion
Worldwide, the trend to conserve the breast has increased over the years, but the rate was extremely low in this series, making it difficult to reach reasonable conclusions. Late presentations may have resulted in the higher disease stage observed, considering that the stage of breast cancer may be a strong determinant of the type of surgery. Other factors that may have contributed to the low numbers of breast-conserving surgeries in this study include limited access to radiation therapy, predominance of biologically aggressive forms of breast cancer, patient preference for mastectomy, and prevailing socioeconomic factors.
Our extremely low number of breast-conserving surgeries reflects the challenges of offering the procedure in a resource-limited environment, although we believe it is worth the effort. Improved awareness of the disease and increased investment in radiotherapy facilities to increase access and affordability should be targets for future interventions to increase the incidence of BCS.