
Abstract
Background and Aims:
To evaluate wire-guided localization for nonpalpable breast cancer regarding procedure and surgery-related outcome in a nonteaching community hospital in the Netherlands.
Material and Methods:
A consecutive series of 117 patients who were treated with breast-conserving surgery after wire-guided localization for nonpalpable breast cancer between January 2006 and December 2010 was retrospectively analyzed. The patients’ digital records were reviewed for patient, radiological, histological, and surgical characteristics. In order to quantify the excess resected tissue, a calculated resection ratio was determined by dividing the total resection volume by the optimal resection volume. The optimal resection volume was defined as a spherical tumor volume with an added 1.0 cm margin. The total resection volume was defined as the corresponding ellipsoid.
Results:
There were no procedure-related complications. There were two postoperative hemorrhages. Margins were clear in 92.3% of the cases after the first surgical procedure. Eight (6.8%) patients required two operations and one (0.9%) patient required three operations in order to obtain negative margins. Breast conservation was possible in 113 (96.6%) patients. The median calculated resection ratio was 1.87 (range 0.47–14.92).
Conclusions:
This study proves that it is possible to obtain excellent results performing breast-conserving surgery for nonpalpable breast cancer regarding margin status, total amount of operations, and the ratio between tumor and resected tissue volume using wire-guided localization as a localization tool.
Keywords
Introduction
With the introduction of stereotactic-guided and ultrasound (US)-guided large core needle biopsy, the role of wire-guided breast biopsy has shifted from a diagnostic to a therapeutic one for nonpalpable breast cancer (1). Alternative localization methods for nonpalpable breast cancer, such as US-guided and radioguided localization, have been advocated in the past and have come to attention again recently (2, 3). In these studies, wire-guided localization (WGL) is reported to be a technically demanding radiological and surgical procedure. Complications such as wire dislocation and migration and even pneumothorax have been described (3). It is also argued that breast-conserving surgery (BCS) after WGL results in less radical resections than US-guided BCS or BCS with radioguided occult lesion localization (ROLL) (3), hence the need for these alternative localization procedures.
The authors believed that they had seldom encountered any of the above-mentioned disadvantages of WGL, and they had the idea that both radiologists and surgeons in their clinic were very satisfied with the procedure. Therefore, a retrospective analysis was performed of all WGL procedures of nonpalpable breast cancer cases in our institution from January 2006 to December 2010. In order to quantify the amount of tissue resected in relation to breast volume, the calculations of Krekel et al. (2) were utilized. The purpose of the study was to describe the results of WGL for nonpalpable breast cancer in our institution, specifically with regard to the above-mentioned disadvantages of the procedure.
Material and Methods
Hospital
The Ziekenhuis Rivierenland is a nonteaching community hospital in the middle of the Netherlands. It serves an area of approximately 120,000 inhabitants. Yearly, 600 new patients visit our outpatient breast clinic. A total of 140 new cases of breast cancer are treated in the hospital on a yearly basis. In all, 70% of these patients are treated with a BCS.
Patients
A retrospective analysis was performed on a consecutive series of patients who had been treated with BCS after WGL for nonpalpable breast cancer from January 2006 to December 2010. Patients who underwent WGL on both breasts and patients for whom the preoperative diagnosis was not available had been excluded from the analysis. Patient, radiological, surgical, pathological, and clinical characteristics had been identified from the hospitals’ digital patient information system. The characteristics that were collected were age, radiological size, radiological appearance, localization method, histological diagnosis, histopathological grade, pathological size, radiologists, margin width, margin status, total amount of operations, and surgeons. Margin status was recorded as positive or negative for ductal carcinoma in situ (DCIS) and invasive carcinoma as defined by the World Health Organization (WHO) and Dutch guideline for breast cancer. A focally positive margin was considered as positive.
Localization Procedure
The localization procedure was performed in the morning after the patient was admitted to the hospital. A Breast Lesion Localization Wire from Bard® Dualok®, 20 gauge, 10.7 cm (Bard Biopsy Systems, Tempe, AZ, USA), was used in all cases. In the case of an US-guided localization, patients were placed in the supine position. Stereotactic localization procedures were performed in the prone position on a LORAD® MultiCare Platinum table (Hologic, Inc., Bedford, MA, USA). All procedures were performed under local infiltration anesthesia of the skin. All localizations wires were taped rigorously to the affected breast in order to prevent dislocation.
Surgical Procedure
All patients were operated on the same day they were admitted and the localization procedure was performed. Before surgery, the incision site was determined by letting the patient sit up and lie down. The incision site was often a few centimeters away from the wire entrance. Patients were operated under general anesthesia. First, the sentinel node biopsy was performed. After incision, the cutis and subcutis were mobilized from the mammary gland in all directions, and the wire was luxated into the surgical area. Then a lumpectomy or segmentectomy was performed and the specimen was marked with sutures. Thereafter, the specimen was sent for radiology. The mammary gland was mobilized from the pectoralis fascia, and the surgical cavity was marked with metal clips in all directions. The mammary gland was closed in two layers and the skin was closed with an absorbable monofilament intracutaneously placed suture. No drains were used. After a confirmation call from the radiologist that the specimen contained the entire malignancy, the patients’ general anesthesia was discontinued.
Calculation of the Volumes
The calculations of the optimal resection volume (ORV), total resection volume (TRV), and calculated resection ratio (CRR) have been described by Krekel et al. (2). Briefly, the ORV for each malignancy was calculated as the spherical tumor volume plus an extra 1.0 cm margin of healthy breast tissue, calculated by the formula 4/3 π (r + 1.0 cm)3. The TRV was assumed to be ellipsoid and was calculated by the formula 4/3 π (a × b × c). CRR was defined to determine the amount of excess breast tissue resected and was calculated by dividing TRV by ORV (CRR = TRV/ORV). In a perfect excision, the CRR = 1.0. If twice the needed amount of tissue is excised, the CRR = 2.0.
Statistical Analysis
Data were entered in a database of the Statistical Package for the Social Sciences (SPSS statistical software, version 17.0; SPSS, Inc., Chicago, IL, USA). Continuous data were depicted as a median value with their range.
Results
A total of 117 patients were included in the study. Patient and tumor characteristics are mentioned in Table 1.
Patient and tumor characteristics.
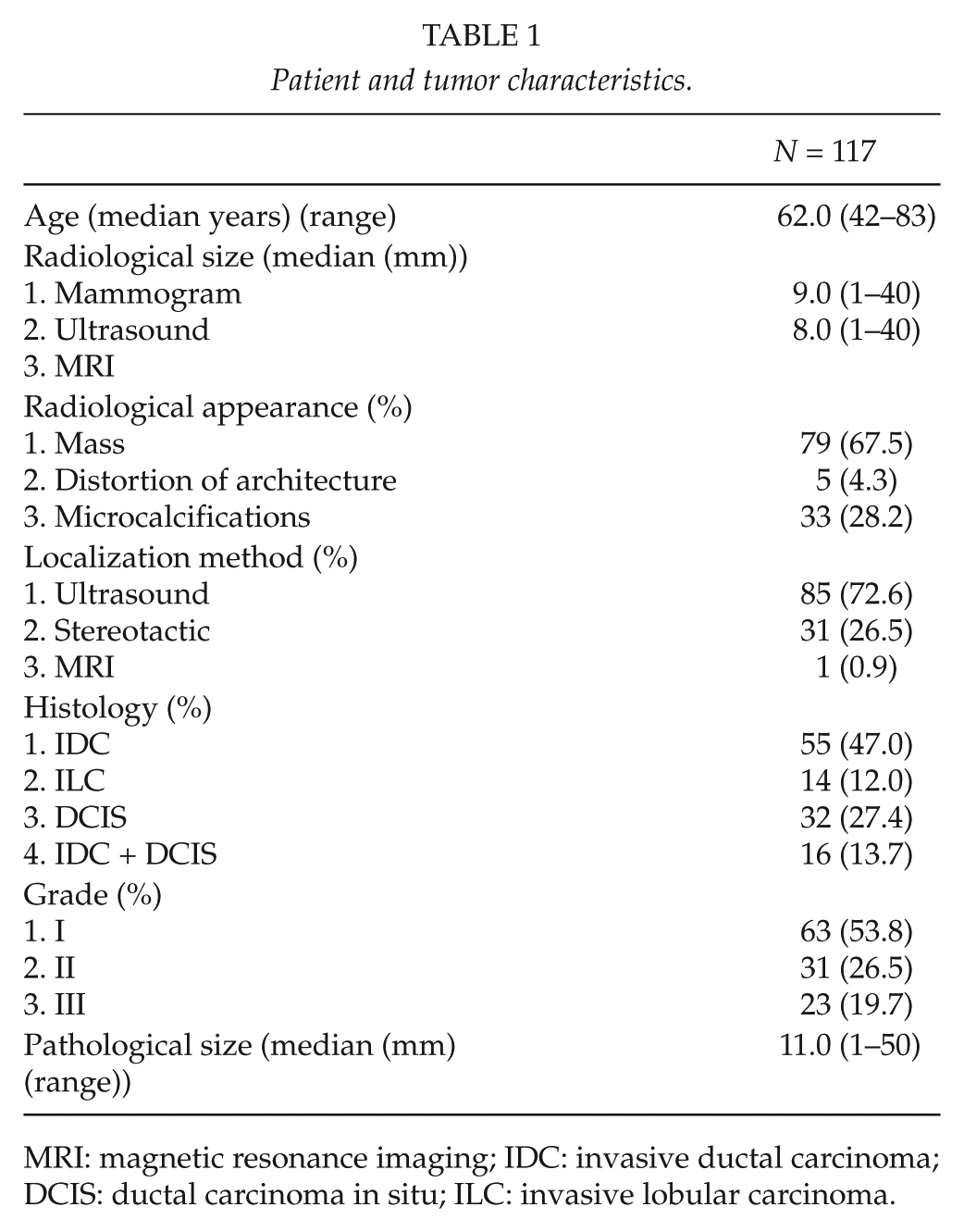
MRI: magnetic resonance imaging; IDC: invasive ductal carcinoma; DCIS: ductal carcinoma in situ; ILC: invasive lobular carcinoma.
Procedure and surgery-related results are shown in Table 2. There were no complications related to wire placement by the radiologist. Five radiologists performed the procedure. After the first excision of the tumor, 92.3% (108) of the cases had negative margins. Eight (6.8%) patients had to be treated with a second and one (0.9%) patient with a third operation in order to obtain negative margins. In all, 113 (96.6%) patients had finally been treated with BCS and four (3.4%) with a mastectomy by three surgeons. There were two postoperative hemorrhages in 127 operations. Median value for CRR was 1.87 (Table 3).
Procedure and surgery-related results.
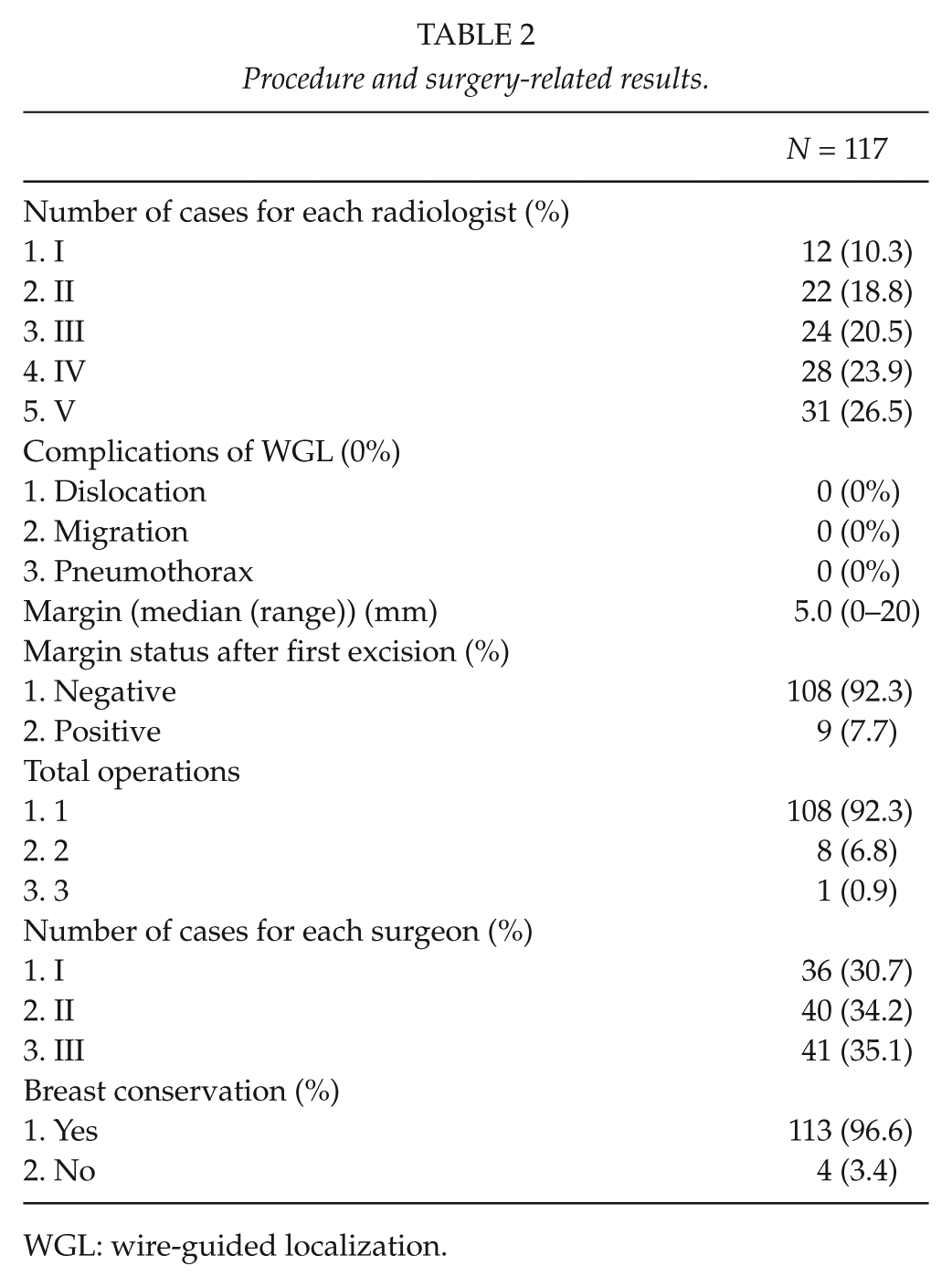
WGL: wire-guided localization.
The optimal resection volumes, the total resection volumes, and the calculated resection ratios.
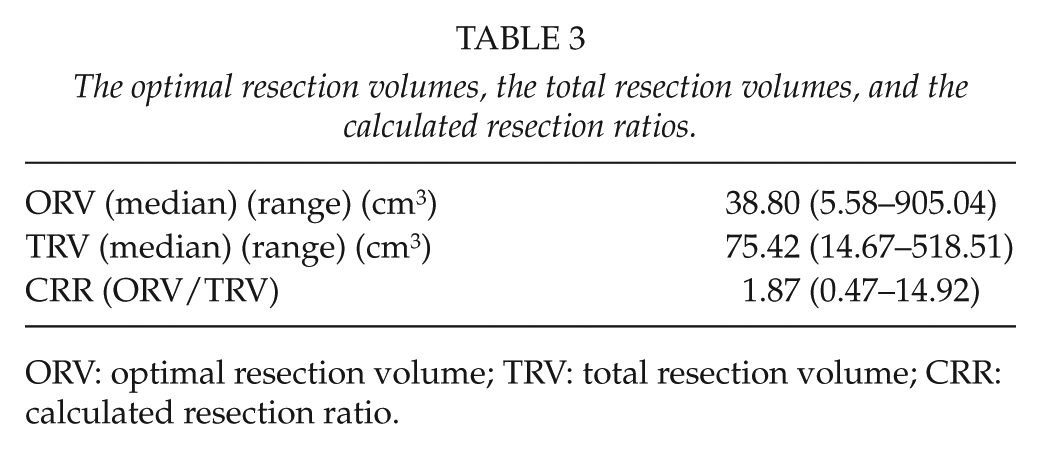
ORV: optimal resection volume; TRV: total resection volume; CRR: calculated resection ratio.
Discussion
Recent articles on ROLL and US-guided excision for nonpalpable breast cancer give the impression that WGL is inferior to these newer techniques. Arguments for these alternative localization procedures are more radical excisions, less complications, less excess breast tissue excision, and less patient discomfort (2–4). The authors of this study would like to demonstrate that in the hands of a dedicated team, excellent results can be achieved by using WGL that, at least, equals the results of these other techniques. In their opinion, WGL should not be abandoned but should rather remain one of the options for radiologists and surgeons in order to treat patients with nonpalpable breast cancer.
In this study, there were no localization procedure-related complications. Complications after WGL are rare, however, and cannot be ruled out on the basis of 117 patients. In a systematic review by Lovrics et al. (3), there were two studies in which the rate of localization problems varied from 0 (out of the 79 procedures) to 2 (out of the 16 procedures). These wide variations can probably be explained by defining complications and by the nature of the study (prospective versus retrospective). Because this study is a retrospective study, the recording of complications can be suboptimal due to lack of documentation. As a consequence of the retrospective character of the study, there was no group of patients who were treated with other localization methods available as a control group. Therefore these conclusions must be interpreted with caution.
In most cases with involved margins after BCS for nonpalpable breast malignancies, the size and/or the number of the lesion(s) is underestimated by radiological imaging. This is particularly the case in the presence of an extensive intraductal component, multifocality, or invasive lobular carcinoma (ILC). Therefore, the case mix of the study greatly influences the results of surgical margins and reoperations. In our study, the patients with ILC, DCIS, and invasive ductal carcinoma (IDC) + DCIS (Table 1) were not underrepresented, and therefore the results of the study are not due to a favorable case mix. Margin clearance rate after the first excision was 92.3% for the whole study population. In all, 27% of the patients had pure DCIS. In other studies, positive margins after excision of DCIS are described up to 33% (5). For invasive carcinoma, a positive margin rate of 6.4% was found in a retrospective analysis of patients treated at the Comprehensive Cancer Center of the Ohio State University (6). In reports describing positive margins in nonpalpable breast carcinoma, the rate varies from 0% to 57.7% (7, 8). Sample sizes in both studies are very small, however (26 patients). In the light of these figures, the results regarding margin status in our study can be interpreted as fairly good. On the contrary, guidelines for histopathological assessment regarding surgical margins and guidelines for reoperations vary among different institutions and countries. Therefore, comparison of these figures between different studies is unreliable.
In order to quantify the amount of resected excess breast tissue, the calculation method of Krekel et al. (2) was also used in our study. In the study of Krekel et al., the median CRR ranged from 2.8 for WGL to 3.2 for US-guided resection and 3.8 for ROLL. If a CRR of 1.0 is ideal, indicating a perfect balance between the ORV and TRV, the excess tissue resected in that study was 2.8–3.8 times in excess. In our study, the median CRR was 1.9. Also, the range (0.47–14.92) in our study was much smaller than the results presented in the Krekel et al. (2) study (0.3–29.0). The authors of this study think that this calculation is a more accurate method in order to quantify the excess breast tissue than specimen weight or volume. This calculation method is also a better tool to compare results of other studies because it is more objective than weight and volume.
The most recent article that disparages WGL is the systematic review by Lovrics et al. (2). In this review, the supremacy of radioguided surgery (RGS) is proven by five randomized clinical trials (RCTs) and seven cohort studies. Nine studies compared ROLL with WGL and three studies compared WGL with radioguided seed localization (RSL). All RCTs were of poor quality due to lack of concealed random allocation and small numbers. The cohort studies also contained small sample sizes. The forest plots for surgical margins and number of operations were in favor of RGS. However, it is noteworthy that in most studies, the reported percentages of involved margins were high, up to 29% for RGS and 58% for WGL. As discussed by Lovrics et al., there was heterogeneity of study designs and endpoints and potential biases inherent in cohort studies. Because it is a novel technique, there may be publication bias as well. After considering all these disadvantages, it is our opinion that drawing conclusions from this review should be done with caution.
Finally, the authors think it is important to maintain the experience with WGL because in some circumstances, it will be difficult to perform US-guided excision (e.g. in the case of microcalcifications) or ROLL or other RGS (e.g. relative contraindication for radioactive radiation in patients).
Conclusions
In our hands, BCS after WGL for nonpalpable breast cancer is a reliable method with few complications and excellent results regarding margin status, total of operations, and excess breast tissue excision. Therefore, it is the authors’ opinion that this method should not be abandoned.
Footnotes
Declaration of Conflicting Interests
All authors have no conflict of interest to disclose.
Ethical Approval
No approval of the ethical committee was required.