
Abstract
Background and Aims:
In Iceland, oncoplastic breast-conservation surgery has been performed since 2008. The aim of this population-based study was to assess and compare the efficacy and patient satisfaction of standard breast-conservation surgery with oncoplastic breast-conservation surgery.
Materials and methods:
This is a population-based, retrospective, observational cohort study on all women undergoing breast-conservation surgery in Iceland from the 1 January 2008 to 31 December 2014. A multivariate logistic regression and linear regression were performed to assess differences in outcomes and a patient satisfaction questionnaire was used to assess certain patient-related outcome measures.
Results and conclusion:
A total of 750 women underwent breast-conserving surgery, 665 had standard breast-conservation surgery and 85 oncoplastic breast-conservation surgery. Oncoplastic breast-conservation surgery was associated with a significantly larger mean size (2.4 cm vs 1.7 cm, p < 0.001) and weight (181.8 g vs 63.4 g, p < 0.001) of breast specimen excised when compared to standard breast-conservation surgery. After correcting for confounding factors, there was no significant difference in surgical margin involvement (odds ratio = 0.97, confidence interval = 0.44–1.97), frequency of complications (odds ratio = 1.06, confidence interval = 0.46–2.18), frequency of reoperations (odds ratio = 0.98; confidence interval = 0.50–1.81), or time to first adjuvant therapy (–0.23 days for oncoplastic breast-conservation surgery, p = 0.95). Patient satisfaction was high in both groups, although not statistically different (96% in oncoplastic breast-conservation surgery group vs 89% in the standard breast-conservation surgery group, p = 0.84). Our results show that oncoplastic breast-conservation surgery is at least as safe as standard breast-conservation surgery in selected cases and may be preferable in ductal carcinoma in situ.
Background
For women choosing breast conservation, oncoplastic breast-conservation surgery (OBCS) has emerged as a surgical option for many. The goal of this type of surgery is to optimize both the oncological and cosmetic outcomes of breast conservation. In the face of studies suggesting cosmetic failure rates of up to 50% following standard breast-conservation surgery (SBCS), it seems rational that techniques that may potentially improve cosmetic outcomes should be offered, especially if they do not compromise on the oncology (1–4).
Previous studies have suggested that cosmetic outcomes of OBCS may be superior to SBCS (2, 5).
Another potential advantage of OBCS is that it may increase the rates of breast-conservation surgery compared to mastectomy, as these techniques allow excisions of larger cancers, which previously would have been treated with mastectomy (5, 6).
OBCS can be divided into two different types of procedures: volume replacement and volume displacement. With volume replacement, the tumor is removed and the defect is replaced with a local flap outside of the breast, such as chest wall perforator flaps (lateral intercostal artery perforator (LICAP); intercostal perforator (ICAP) or pedicled flaps (thoracodorsal artery perforator (T-DAP) or latissimus dorsi ( LD-miniflap). This approach is particularly useful in women with smaller, non-ptotic breasts (6–8). Volume displacement involves either glandular rotational flaps or the use of secondary or extended dermoglandular flaps within the breast and may often involve the use of breast reduction techniques. Hence the term therapeutic mammoplasty is often used for these types of procedures. These techniques are better suited for women with some level of ptosis or larger breasts. Contralateral reduction mammoplasty is often performed at the same time for breast symmetry. Figs 1 and 2 show examples of volume replacement and volume displacement.
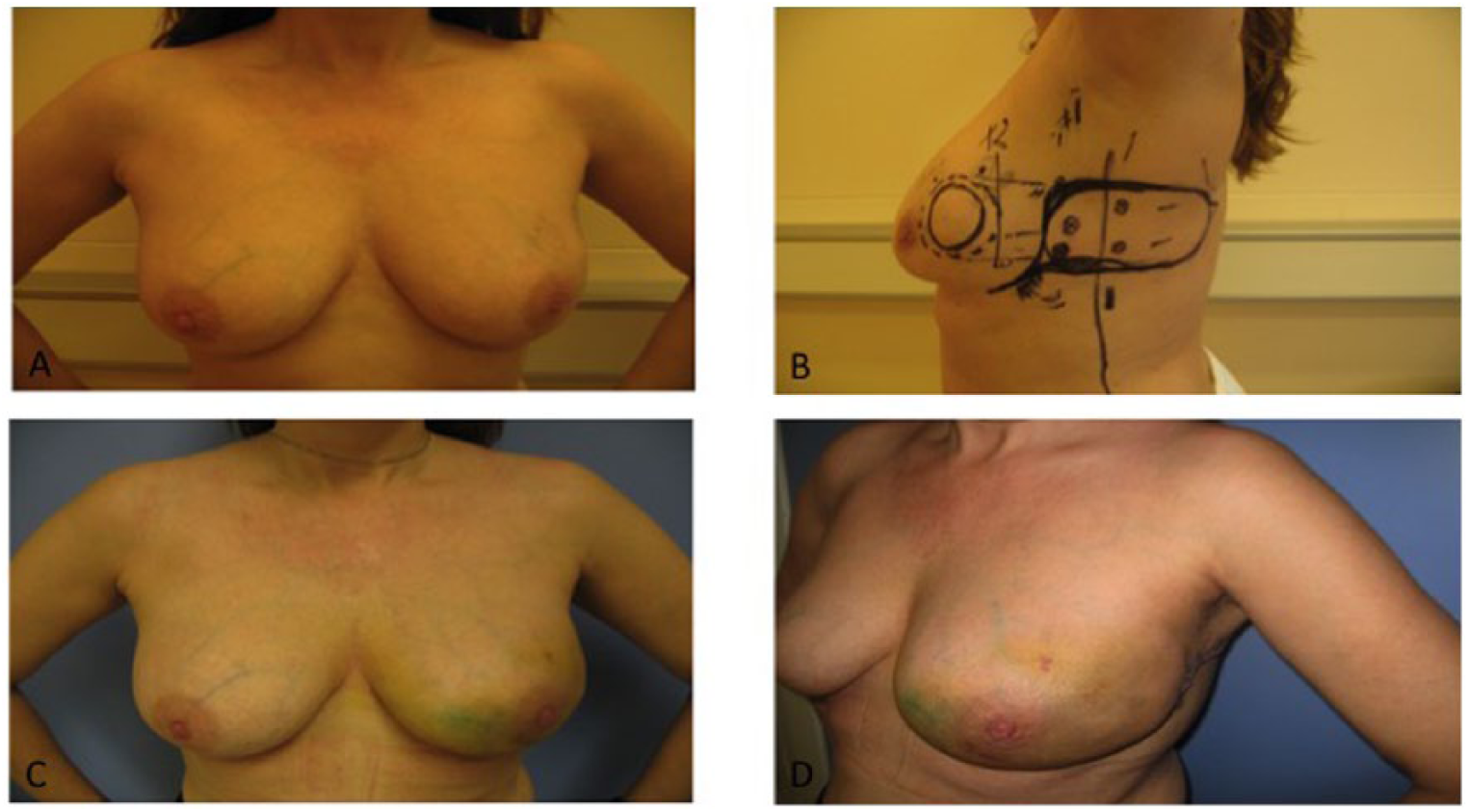
Volume replacement procedure with a LICAP flap.

Bilateral volume displacement. On right side, central skin paddle from advanced inferior pedicle.
OBCS has been performed in Iceland since 2008, but the extent and efficacy has not been investigated. OBCS was offered to women who were at risk of cosmetic failure with SBCS due to size or location of tumor. Also OBCS was rather offered to non-smokers and women with larger breasts. The aim of this population-based study was to assess the extent of breast-conserving surgery and to compare the efficacy and patient satisfaction of SBCS with OBCS from 2008 to 2014.
Methods
Study Design
This is a retrospective, observational cohort study on all women who underwent breast-conserving surgery in Iceland at Landspítali University Hospital from 1 January 2008 to 31 December 2014. The exclusion criteria were: mastectomy, no tumor seen in the removed breast tissue, bilateral SBCS, and males.
The women included in the study were stratified in two groups based on whether they underwent SBCS or OBCS. The OBCS group contained both volume displacement (therapeutic mammoplasty) and volume replacement procedures. A single surgeon (K.S.A.) performed all of the OBCS. Level 1 and level 2 oncoplastic procedures (minimal gland mobilization techniques) were not included in the study group.
Data of the patients were collected from medical records and included all communication with patient from time of diagnosis to end of study period, that is, 31 December 2014. The data collected were as follows: age, smoking status, use of hormone therapy prior to diagnosis, positive family history for breast cancer, admission time, tumor size, weight of breast tissue removed, histological typing, TNM stage, nodal involvement, tumor margin status, patients requiring re-excision, type of adjuvant therapy, time to first adjuvant therapy, and complications (hematomas, seromas, surgical infection, and neurologic pain). The data were collected on Excel document.
Statistical Analysis
The statistical software R was used for statistical analysis. T-test and binomial test were used for comparing variables in the two stratified groups (i.e. OBCS and SBCS).
A number of outcomes were of special interest when comparing the efficacy of the two surgical approaches, that is, OBCS and SBCS. Those investigated here were rates of tumor involvement in surgical margins, frequency of complications, time to first adjuvant therapy and reoperation rate.
As many of the variables that were sampled are dependent on each other, a stepwise backward selection was applied to see which variables affected the outcomes. A multivariate logistic regression and linear regression were performed to correct for the effects of those variables to reveal how the different surgical approaches affected the outcomes stated above.
A p-value of <0.05 was deemed statistically significant.
Question Lists
To evaluate patient satisfaction with aesthetic outcome and information provision prior to surgery, question lists with six questions were sent out to women in both stratification groups.
Results
A total of 750 women underwent breast-conserving surgery from 2008 to 2014. Of which, 665 women had SBCS as opposed to 85 OBCS. Therefore, 11.3% of all patients having breast-conservation surgery in our unit had OBCS. Of these 85 patients, 76 (89.4%) had volume displacement and 9 (10.6) had volume replacement.
Table 1 summarizes the data collected for the two stratified groups.
Demographic characteristics.
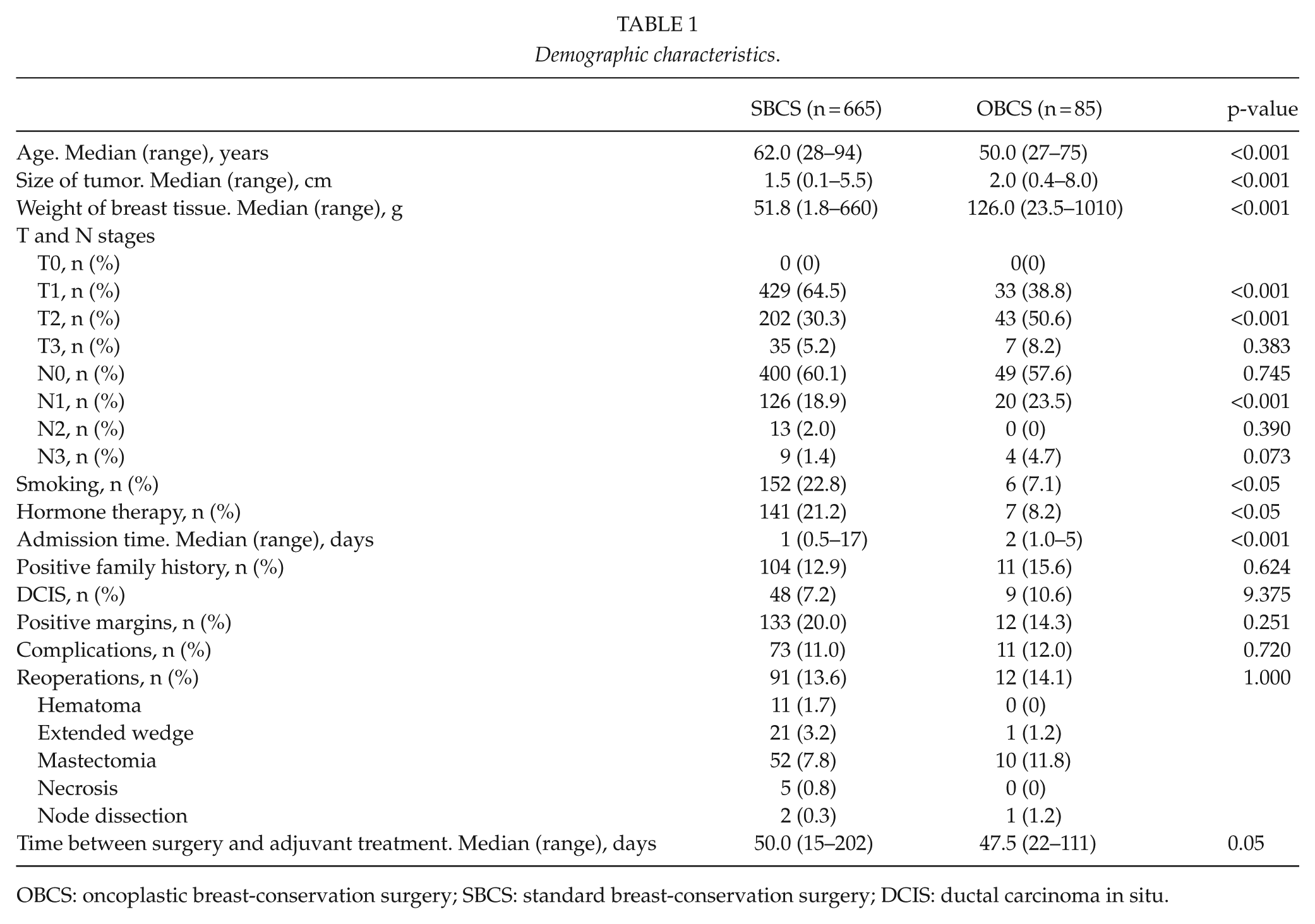
OBCS: oncoplastic breast-conservation surgery; SBCS: standard breast-conservation surgery; DCIS: ductal carcinoma in situ.
In Table 1, some significant differences are seen between the two stratified groups. Patients in the OBCS group were significantly younger and significantly fewer were smokers. Also, the mean size tumor was significantly larger, nodal involvement was more frequent, and more breast tissue was removed in the OBCS group. Furthermore, the median admission time was significantly longer for the OBCS group, although the admission time for OBCS was considerably shorter in the last year of the study period, 2014, with a mean of 1.7 days as compared to 3.1 days in the first year of the study period, 2008.
Table 2 shows the results of the multivariate logistic regression. Linear regression for time to first adjuvant therapy showed no statistical difference between the OBCS and SBCS (–0.23 days for OBCS with p-value of 0.95). It is evident that when corrected for the following variables: age, smoking status, weight of breast tissue removed, use of hormonal therapy prior to surgery, and TNM stage, there is no significant difference in surgical margin involvement, frequency of complications (hematomas, seromas, surgical infection, and/or neurologic pain), frequency of reoperations, or time to first adjuvant therapy.
Multivariate logistic regression.
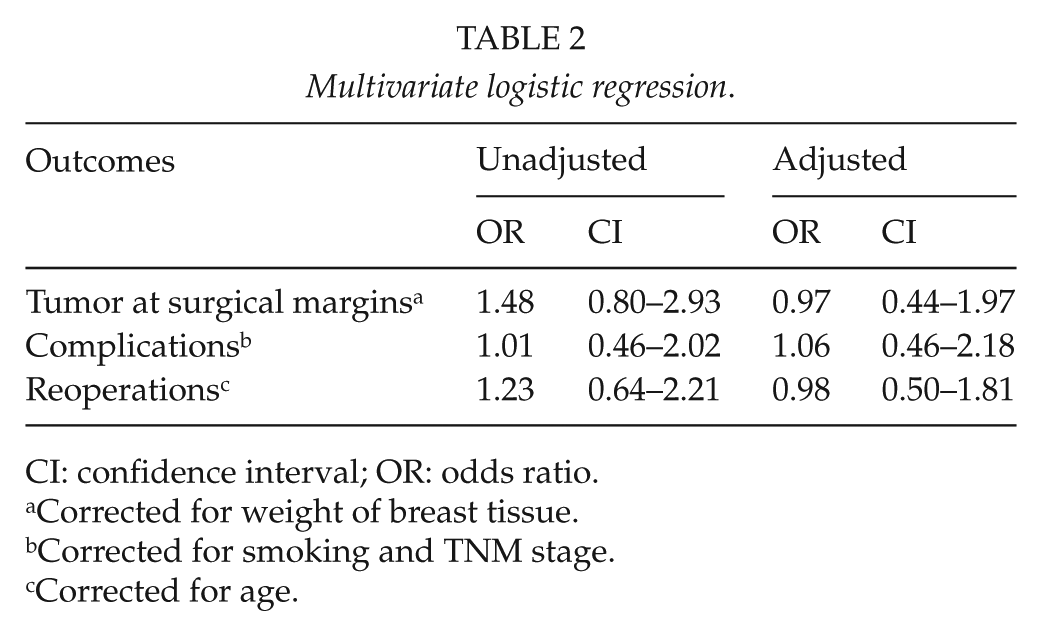
CI: confidence interval; OR: odds ratio.
Corrected for weight of breast tissue.
Corrected for smoking and TNM stage.
Corrected for age.
DCIS was seen in 57 (7.6%) women who underwent breast-conserving surgery (Table 3). Similar percentages of patients had surgery for DCIS in the two groups. Although not statistically significant, the rates of margin involvement were lower in the OBCS than in the SBCS group (42% vs 22%).
Histological characteristics.
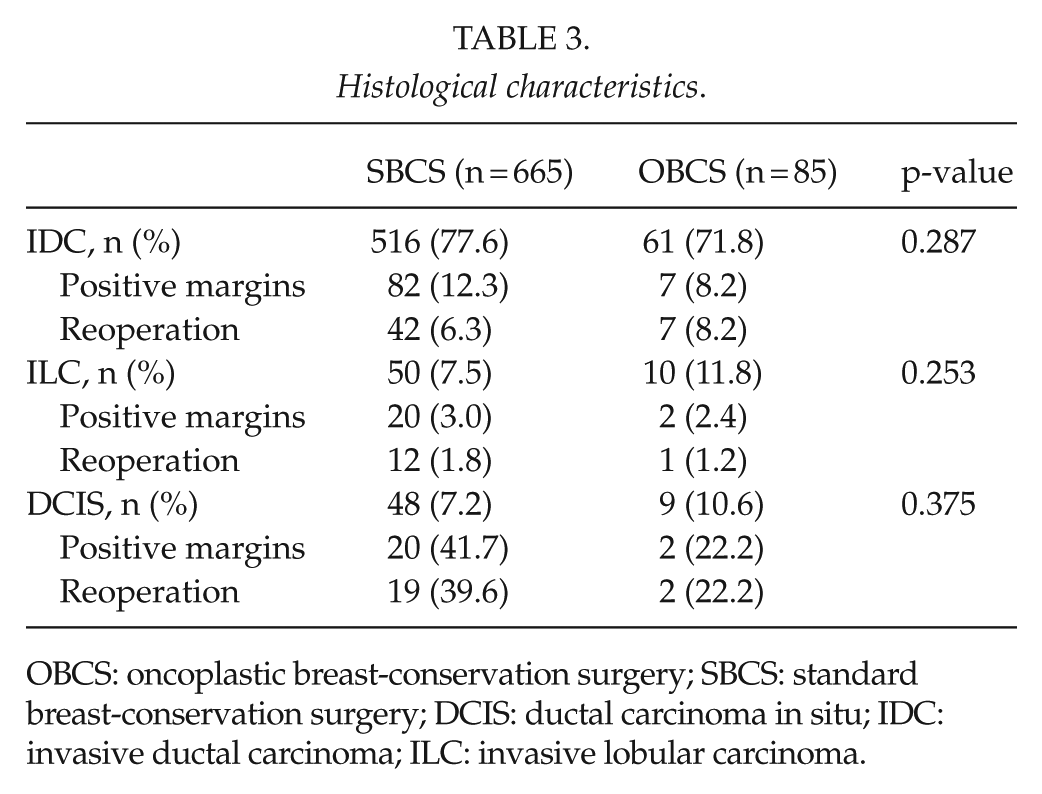
OBCS: oncoplastic breast-conservation surgery; SBCS: standard breast-conservation surgery; DCIS: ductal carcinoma in situ; IDC: invasive ductal carcinoma; ILC: invasive lobular carcinoma.
Question lists were sent to 448 women in total. Of those, 75 were in the OBCS group and 373 in the SBCS group. Response rate was 68% in the OBCS group but 43% in the SBCS group.
Although a detailed patient-related outcome questionnaire was sent to the patients (Supplementary Appendix 1), Fig. 1 shows the patients reply to the question whether they were happy with the aesthetic outcome of the breast following their surgery.
Fig. 3 shows that overall in both groups there was a high satisfaction rate with the cosmetic outcomes of the surgery, although a slightly higher rate of women in the OBCS group replied with “I agree very much” or “I agree for most parts” though the difference is not statistically significant.
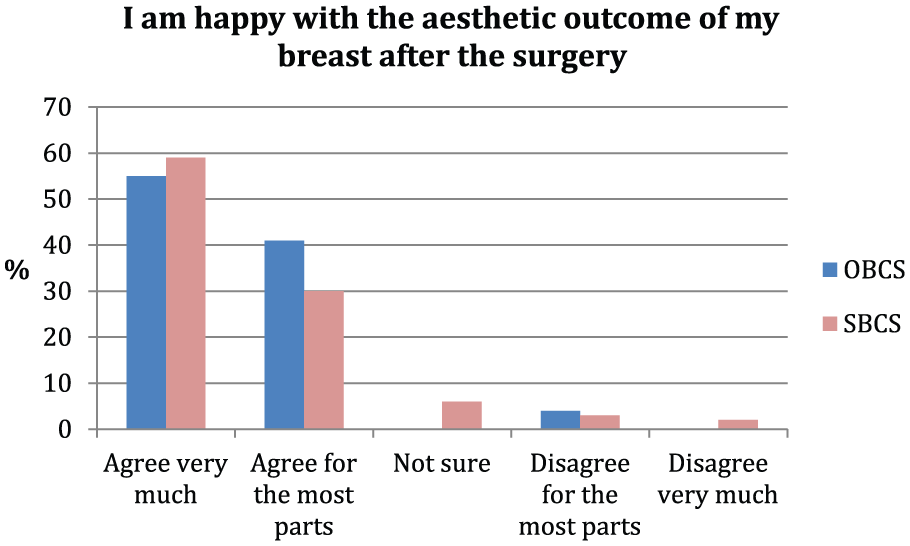
Patient questionnaire – satisfaction with aesthetic outcome.
Discussion
In this study, we show that patients offered OBCS in our institution, have derived good short-term outcomes from their surgery, when compared to patients having SBCS in the same time period and satisfaction with the aesthetic outcome is high. We believe that in order to achieve good outcomes for patients having OBCS, a stringent selection criteria needs to be applied, especially for breast units beginning to offer these types of procedures. In general, they should be offered when the expected excision of breast tissue is proportionately high and SBCS is likely to result in a poor cosmetic outcome (5, 6, 9–11). Also, they should be offered when there is a high risk of margin involvement, that is, in multifocal disease or DCIS (12). In the UK Sloane project, reoperation rates were nearly twice as likely when breast conservation was performed in patients with DCIS, irrespective of grade, as compared to isolated invasive disease (29.5% vs 18%) (13). Studies do in fact suggest that OBCS may reduce reoperation rates in patients with DCIS or multifocal disease (1, 2, 10, 14–16).
In our study, only 11.3% of all women treated with breast-conservation surgery had OBCS, which were significantly younger, and the large majority (93%), were non-smokers when compared to the SBCS group. Our results also show that we have selected OBCS for women with larger tumors and in situations where we have deemed larger resection specimens to be preferable, that is, in DCIS (2). Women with DCIS and treated with SBCS in this study, had over a 40% rate of margin involvement, whereas this was much lower, 22%, in women treated with OBCS. Overall, however, in patients with DCIS and invasive breast cancer, there did not seem to be a difference in margin involvement between the two surgical groups.
Therefore, we believe that, at least in the short term, OBCS surgery is at least as safe as SBCS, even in larger cancers and may be preferable in patients with DCIS. This is in agreement with results from previous studies as mentioned above. To further evaluate the oncological safety of OBCS, such as local recurrence rates, a more long-term follow-up is necessary. Recent studies with long-term follow-up do however suggest that these procedures are oncologically safe. (17)
Because of the higher complexity of OBCS compared to SBCS, concerns have been raised that OBCS may be associated with a higher risk of complications, which may delay subsequent adjuvant therapy. Studies have, however, not supported this view (2, 18, 19). The results of this study show that complication rates following OBCS are not higher when compared to SBCS nor is the time to adjuvant therapy prolonged.
When new surgical techniques are being implemented in individual institutions, procedural costs are of course of importance. Both the length of operating time and hospital stay have bearing when calculating these costs. Although in our study, the hospital stay for patients having OBCS was on average significantly longer than in the SBCS group, the admission time shortened considerably from the first year of the study period to the last (3.1 days in 2008 vs 1.7 days in 2014).
This highlights the fact that with increasing experience, the hospital stay may be expected to be equivalent in the two groups. Many experienced breast units now offer OBCS as day surgery (2, 20)
Our study is one of the few whole population studies to publish outcomes on OBCS. A published national survey conducted in France showed that OBCS was offered to 13.9% of all patients having breast-conserving surgeries (21). Although the type of OBCS differs in this survey in comparison to our study, our study shows that proportion of patients being offered OBCS was comparable (13.9% vs 11.3%). Overall, it seems that the rates of OBCS is relatively low, and one explanation for this is that in the study period, there was only one surgeon performing OBCS in our unit. It is likely that these rates may increase, if the unit employs more oncoplastic breast surgeons in the future.
Regarding the aesthetic outcome, the results of our study are in keeping with a recently published study that showed good or excellent aesthetic outcome even though patients who had OBCS had significantly larger tumors and nodal involvement was more frequent (22). The response rate to the question list was higher in the OBCS group. It is probably due to closer follow-up after the operation when compared to the SBCS.
Our study has some limitations. It is retrospective and not randomized and thus prone to selection bias. For example, there is a certain criteria for choosing patient who can have OBCS and thus it was known that the two groups would not be identical. We tried to correct for those differences with the logistic regression. The study focuses on short-term outcomes of OBCS and thus cannot be used to comment on the safety of the OBCS when looking at recurrence rate.
Conclusion
Our results show that in our unit, OBCS is at least as safe as SBCS in selected cases in the short-term. Also, patient’s satisfaction with the aesthetic outcomes of OBCS is high.
Supplemental Material
Questionnaire – Supplemental material for Oncoplastic breast-conserving surgery in iceland: A population-based study
Supplemental material, Questionnaire for Oncoplastic breast-conserving surgery in iceland: A population-based study by E. P. Palsdottir, S. H. L. Lund, K. S. A. Asgeirsson in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors thank Pétur Sólmar Guðjónsson for his contribution to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The ethics committee of Landspítali University Hospital, Siðanefnd, gave their written consent for our study on 24 March 2017. The ethics committee reference number for our study is 16/2014.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Vísindasjóður Landspítalans (Landspítali University Hospital research fund).
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.