
Abstract
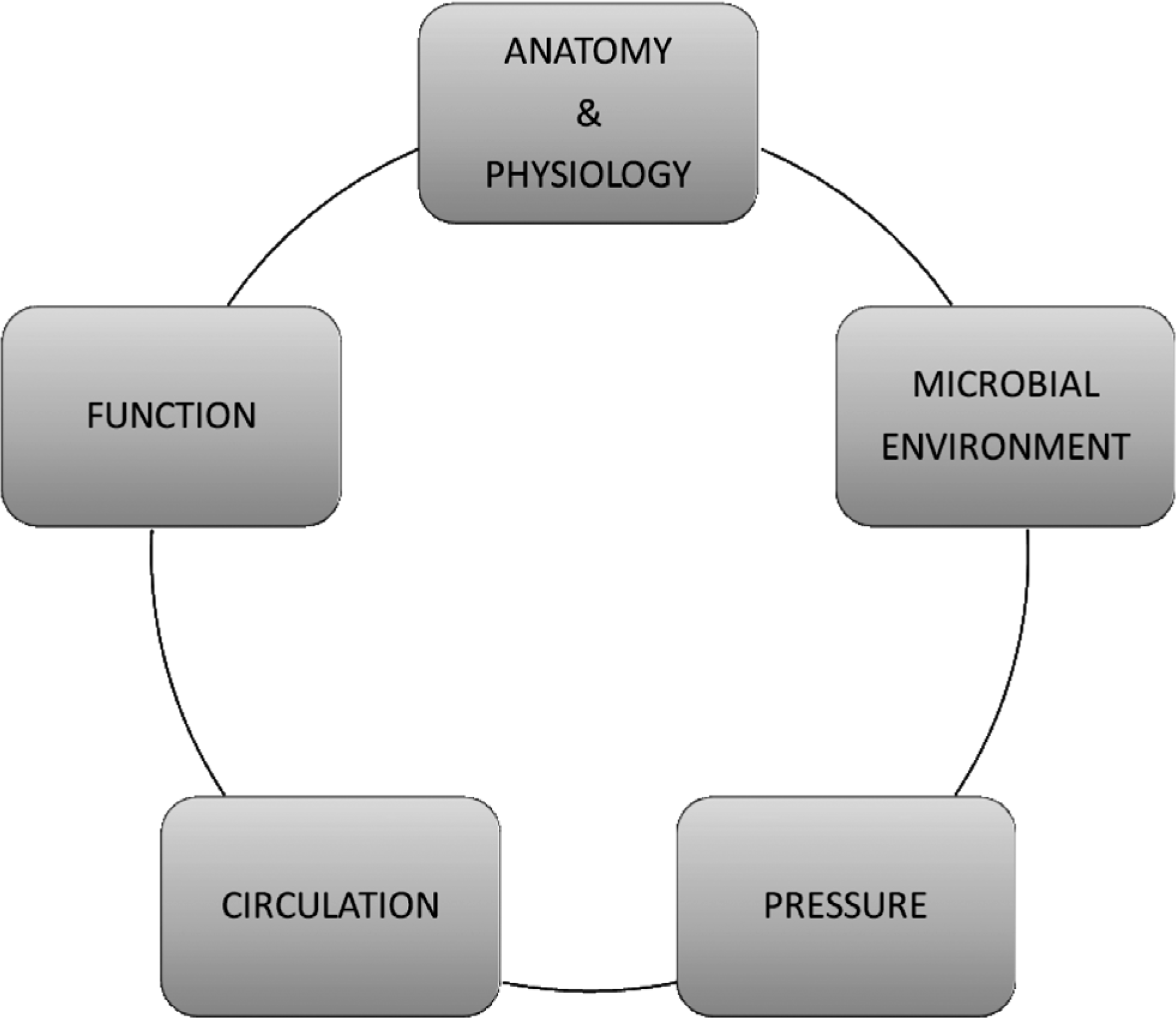
Perineogenital and pelvic surgery is challenging due to the complex anatomy and physiology, multi-organ involvement and microbial environment of this region. In reconstructive surgery local and pedicled flaps are usually applicable. Microvascular flaps are rarely needed. Positioning of the scars, tension in the wound edges and pressure conditions must be taken into account, because failed correction may create more functional and aesthetic problems as the defect itself. This brief review focuses on the reconstructive methods of perineum, genitals and pelvic floor, site by site, with special emphasis on functional details.
Keywords
INTRODUCTION
The perineogenital region is vital for many functions of the body, such as urination, bowel evacuation, sexuality and reproduction. This region must endure external pressure projected to the body on a sitting position, tension due to movement of the hips and friction from direct contact to clothes, hygiene products or during the intercourse.
The complex role of this region must be taken into account, when operative treatment is planned. In addition, its normal appearance is extremely important to self esteem and sexuality. Even minor functional details should be considered. Embarrasment and shame associated with perineal troubles are also common and a discrete, yet open, attitude by the surgeon is necessary in order to get a thorough anamnesis and proper follow-up information later. Disease or its incompetent treatment may have devastating effects not only locally, but also affect the daily routines, social contacts, intimate life and mental health of the patient.
GENERAL PRINCIPLES
Reconstruction of the perineopelvic region or genitals is indicated in defects with large surface or in functionally crucial areas. Indication varies from congenital defects to infection, tumors, trauma, lymphedema or uncommon problems, e.g. gender dysphoria. Reconstructive principles and challenges are mainly similar regardless of the etiology and depend more on the specific site of the defect (Fig. 1A).
Timing of the reconstruction is challenging. Deep structures, like the pelvic floor and vagina, require immediate reconstruction, as scarring may exclude later attempts of reconstruction. On the other hand, delayed reconstruction may be beneficial in infected defects, as wound contraction may reduce the reconstructional needs.
Intraoperative conditions are demanding due to difficult anatomy and physiology, multiple functioning organ systems, skin colonised permanently with bowel flora, external and intra-abdominal pressure and the rich vascularity with increased risk to haematoma. The patients are often multi-morbid, presenting with cardiovascular diseases, diabetes, smoking, immunosuppression and poor nutrition. These and local factors like previous radiation therapy or infection, have impact on recovery. Normal wound healing in this region is slow and often with secondary intention (1, 2).
Challenges in perineopelvic surgery
The risk for psychological problems is significant in the genital surgery. If there is a discrepancy with the symptoms of the patient and the clinical findings, Thersite's complex should be taken into account. In this mental disorder patient is observing and ashamed of a fictional defect in his/her body, usually in the face or genitals (3, 4, 5). It has influence both on the decision making with the treatment and on the patient satisfaction after potential operation.
As numerous large-scale studies have shown, normal genitals vary largely in appearance and dimensions (6, 7, 8, 9, 10, 11, 12, 13, 14). This aspect should be taken up by a surgeon, as the perineal anatomy stays loaded with myths and beliefs even in our times.
Perineogenital region has a high risk for chronic pain: iatrogenic nerve and muscle damage, preoperative chronic pain, infection, psychosocial factors, etc. Meticulous operation technique, wound care and proper perioperative pain relief are important (15, 16).
Aims in reconstruction are unobstructed urination and defecation with normal continence, avoidance of urinary infections and permanent ostomies. Preservation of normal sexuality and reproduction is desirable, aiming at a satisfactory aesthetic outcome with protective and erogenous sensitivity.
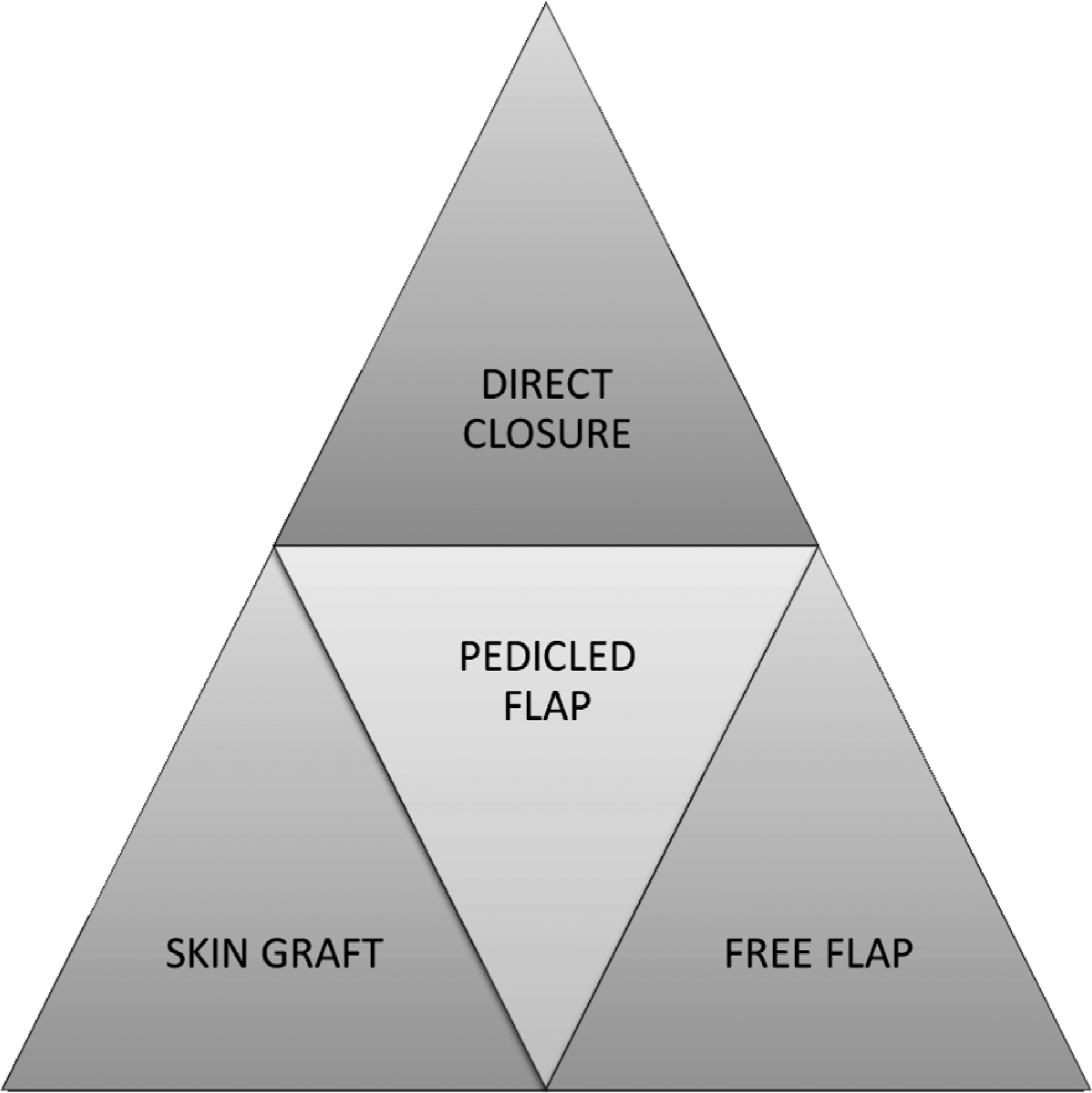
Reconstruction is planned individually, replacing deficient tissue with similar “like with like”, restoring function and aesthetics and preserving nerves. Reconstruction method of choice in the perineopelvic region is primarily direct closure assisted with wound edge mobilisation and an additional relaxing incision or a local plasty (rotation, transposition etc.), if necessary. Skin grafting in this region is not the first option, as the graft take is often suboptimal due to shearing forces and bacterial colonisation. The grafted site cannot resist external pressure and may result in an unstable scar. Many local flaps can reach the defect, allowing quicker and simpler solution compared to free flaps. Time consuming and elaborate microsurgery is usually the last choice, if local or pedicled flap options are not available. Donor site defects should be encountered and reconstructions should be planned as simple as possible (Fig. 1B).
Reconstructive methods
FUNCTIONAL CONSIDERATIONS
The complex functions of the digestive and the urinary system are well understood and their preservation is obvious for most surgeons. Still, the significance of the genital skin remains often ignored. Loose skin in that region is functional, and not some extra tissue to be wasted in reconstructions.
Genital wounds may often be primarily closed. False orientation or tension of the scar, even a minimal scar in a critical area, an extra bulk or a lack of proper buffer may have profound effects in daily life. It is therefore necessary to be aware of the details and purpose of the anatomical structures while planning a reconstruction.
Perineum is an important barrier between the anus and the vagina. Large resection without reconstruction will result in a cloaca-like structure, which is prone to urinary infections or vaginitis. Most of the external pressure on a sitting position is projected to the perineum and the ischial tubercles. A shortened perineum in both male and female patients shifts the highest pressure towards the anus, which may lead to hygiene problems, ulceration or soiling.
Scrotum protects the testicles allowing spermatogenesis in suitable temperature. Labias shelter urethral orifice, introitus and clitoris thus hindering friction and contamination. Both scrotum and labias have important buffering effect against external impact due to the softness and the gliding movement of the tissue.
Panniculus carnosus is a thin muscle layer below fascia superficialis. In humans this kind of structure exists in a few spots of mobile skin, e.g. platysma and fascia dartos in the genital region. Penile skin is extremely thin and elastic. This special skin is difficult to replace especially on the dorsal aspect of the penis. Large resection may shorten and scar the penile skin to an extent, that it is too short and stiff to allow normal erection. Reconstruction should thus be performed with scrotal flap, which is the only similar tissue securing its function (Fig. 2A–C).
Preputial skin shelters the thin and sensitive surface of glans. Circumcision especially in adulthood may cause problems, as the skin of the glans dries causing hyperaesthesia and even chronic pain. Besides scars in sulcus coronarius are often instabile and thus prone to ulcerations.
PREPARATIONS FOR RECONSTRUCTION
Before the reconstruction, the need for urine diversion (bladder catheter or cystostomy), bowel preparations (emptying or enterostomy) and postoperative pain relief (epidural analgesia) are considered. Perioperative pressure ulcer prevention is important. Position on the operation table and during potential postoperative immobilisation is planned carefully. Special mattresses, cushions and textiles, as well as nutrition and wound products preventing maceration of the skin are important.
Thrombose prophylaxis is planned according to individual risk factors. Dietary supplements can be used to correct the nutritional state of the patient. Also other factors compromising wound healing (e.g. smoking, cortisone or diformin medication) should be eliminated, if possible.
Aerobic and anaerobic antibiotics (e.g. kefalosporin and metronidazole) are administered prophylactically in reconstruction cases. Infected operation site is advisable to treat with debridement, open wound care and targeted antibiotics well in advance.
Despite infection, immediate reconstruction is sometimes necessary, especially in deep resections where many organ systems and the pelvic floor are involved. In these cases the risk for wound healing problems is increased, which must be taken into account in the operation plan: synthetic materials are avoided, a transient loop-enterostomy is considered, special attention is given to wound closure and postoperative wound care.
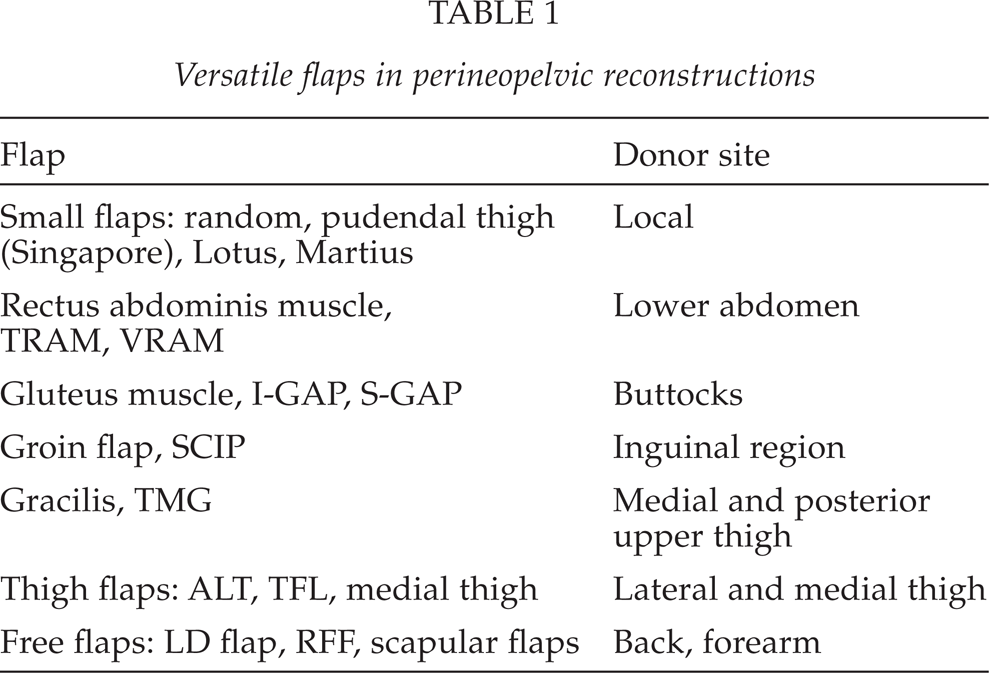
FLAPS
(Table 1)
Conventional random skin or mucosal flaps produced by rotation or transposition from adjacent structures are useful and usually a better solution compared to skin grafting, the result of which is easily spoiled by bacterial contamination or pressure. Skin flaps harvested from the groins and based on superficial perineal vessels from internal pudendal vessels and often reinforced with a posterior skin bridge are long, pliable and useful especially in vaginal reconstructions (Pudendal-thigh or Singapore flaps) (17). Lotus flaps originating from pudendal perforators of internal pudendal vessels are equally useful in the perineum (18). Gluteal fold flap has been popular in the same region (19).

Deep circular burn wound

Scroral flap after revision
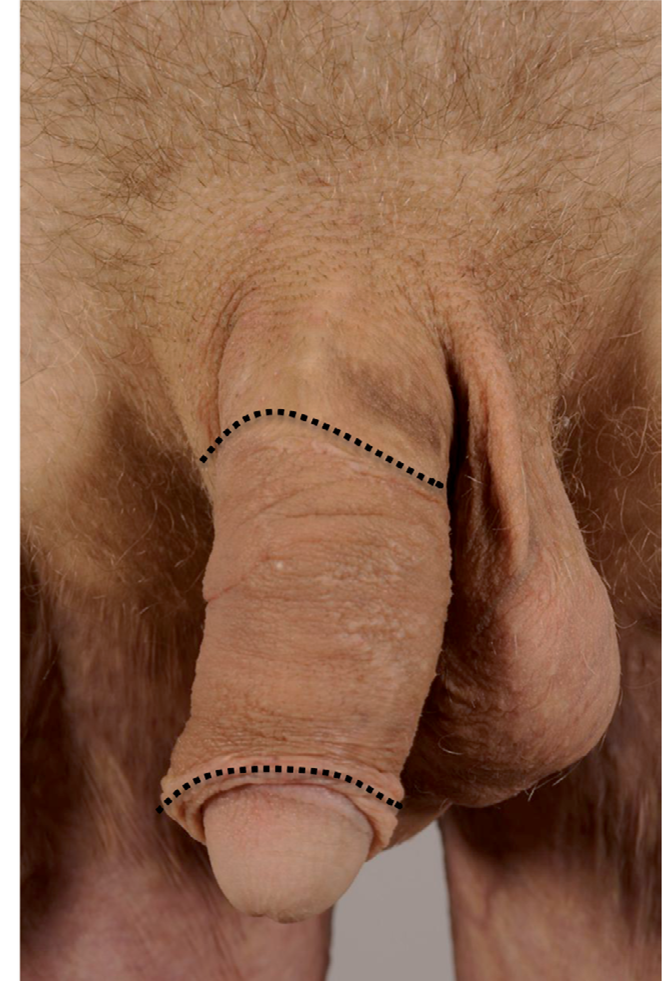
Final result: scrotal flap between the lines

Metastatic anal cancer
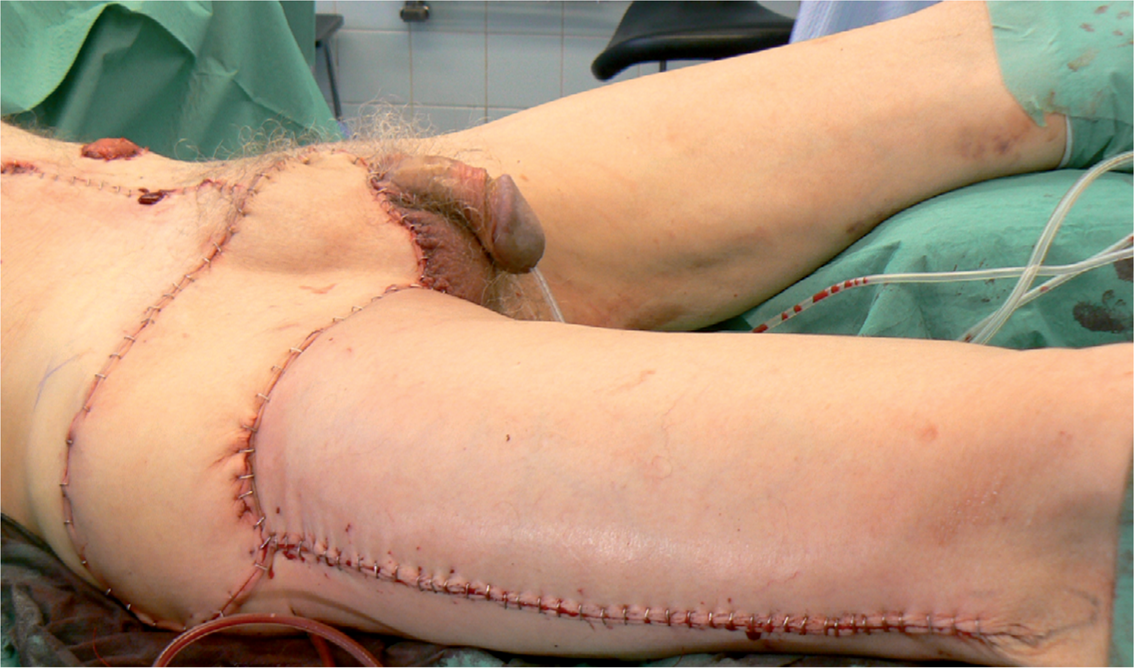
Resection and reconstruction with ALT+ TFL flap
Tensor fascie latae flap (TFL) has very constant anatomy and can be utilised to cover lateral defects, e.g. in inguinal regions (20, 21, 22). It can also be raised together with anterolateral thigh flap (ALT)(23), which allows a longer flap design to reach the pubic region, e.g. in locally advanced epidermal cancer (Fig. 3A–B). ALT flap mobilised on its pedicle reaches the genital region easily, enabling its use in phalloplasties or vaginal reconstructions, but donor site phantom pain may occur. Gracilis muscle or musculocutaneous flap is the method of choice in the perineogenital reconstructions and in the pelvic floor (24). Traditional flap design with a vertical skin island is insecure, but according to current knowledge the angiosome for skin circulation is transverse (TMG, transverse myocutaneous gracilis flap) (25, 26, 27). The transverse skin island allows easier accessibility to the pelvic floor, invisible donor site scars and more reliable skin island. Also the medial thigh flap is useful in vulvovaginal reconstructions (28).
Gluteal flaps (29) with or without skin island have been popular especially in pressure ulcers. In the pelvic floor reconstruction, they have been used together with synthetic allograft materials (30). Donor site may be problematic due to reduced flexion strength of the hip or pain while sitting, though (31). Gluteal muscle may thus not be the primary reconstruction material for mobile patients, if other options are available. Gluteal perforator flaps (S-GAP and I-GAP) do not affect the motor function and may be used to cover posterior defects (32, 33). Also hamstring muscle flaps (semitendinosus, semimembranosus and biceps femoris muscles) have tradionally been used for the same indication (34, 35).
The groin flap (36) is based on superficial circumflex iliac vessels and can be harvested with a hairless skin island up to 12 × 30cm large. Both the traditional groin flap and its perforator version SCIP (superficial circumflex iliac artery perforator) flap (37) are versatile especially in urethral reconstructions.
Abdominal rectus muscle flaps with (TRAM, VRAM, oblique RAM) or without skin island have been popular in pelvic floor and vaginal reconstructions (38, 39, 40). They have some drawbacks, though. In these operations, a simultaneous laparotomy is usually needed, and at least one ostomy, either enterocutaneostomy or urine diversion, which limits the amount of available tissue. The total operation time is elongated, as the flap harvest and laparotomy cannot be performed simultaneously. Besides, rectus abdominis muscle has very important function in maintaining the stature of the body together with back muscles. It should thus not be used as a primary flap in pelvic reconstructions where enterostomies are planned, as donor site defect is significant and the total operation time is longer. Abdominal skin flaps (DIEP, SIEA) (41, 42) offer valuable pedicled tissue in the reconstructions of groin, pubic and perineal defects, as well as reconstructions of vagina or pelvic floor, if laparotomy is performed. Their use might be limited due to previous abdominal operations and their scars.
Out of numerous microvascular flaps the most useful is the myocutaneous latissimus dorsi flap. This big flap covers large surfaces and fills big cavities. Smaller free flaps are usually not needed, as local flap options offer the same amount and quality of tissue. Radial forearm flap has, though, one important indication; it is used in phalloplasties (43).
Versatile flaps in perineopelvic reconstructions
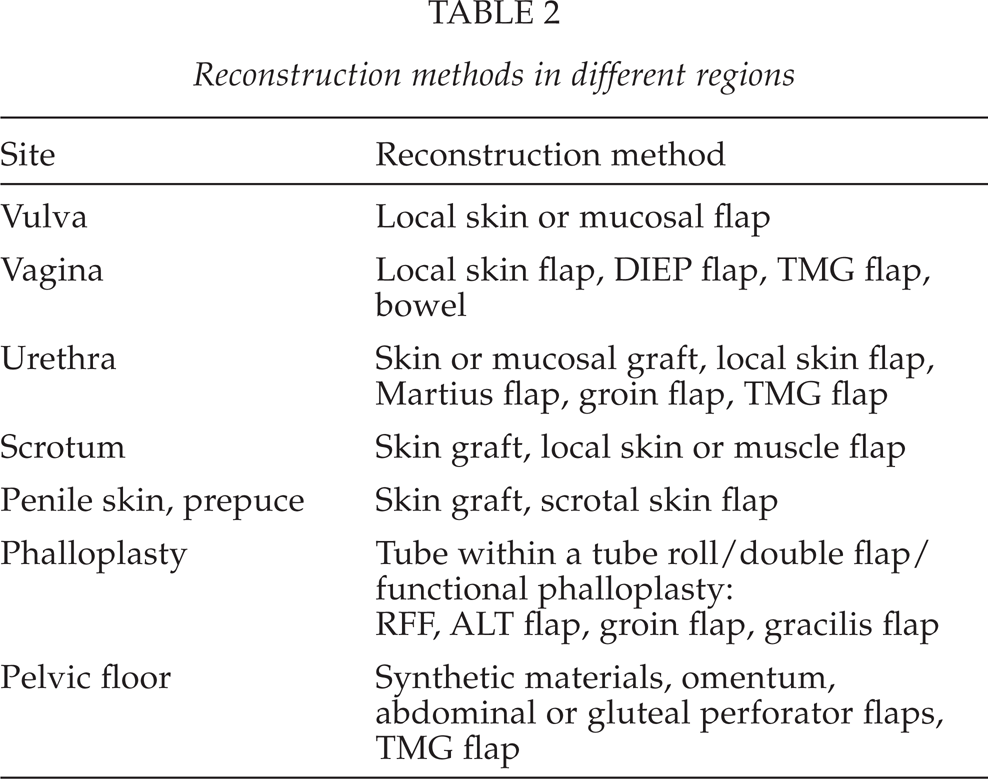
METHODS SITE BY SITE
(Table 2)
VULVA
Defects are usually treated with mobilisation of surrounding tissues or local flaps, e.g. Singapore, Lotus, gluteal fold or groin flap. Resection of labia majora is comparable to eye lids or lips; fairly big resections allow direct closure and (posterior) fixation is needed. Tension line should be in an anteroposterior direction in order to prevent opening of the labias, as this could result in the friction of the clitoris and the urethral meatus and drying of the introitus. Aim is as normal appearance and function as possible. Voiding should be unobstructed and the urine stream in midline, because hygienic problems are common otherwise. Careful planning of the flaps is essential, as patient's sex life may be ruined due to falsely directed, painful scars. Open introitus is important, not only for sexual function, but enabling outflow of vaginal secretion and even disease control by vaginoscopy.
VAGINA
Usually there is ample tissue for a local mucosal flap in partial defects of vagina. In smaller defects different skin flaps (e.g. Singapore, Lotus, gluteal fold and medial thigh flaps) are also versatile. If there are wound healing compromising factors, like previous radiation therapy or a fistula to adjacent structures (bladder, rectum), filling of the defect with well vascularised muscle tissue (usually gracilis) is beneficial. In bigger defects (over half of the vagina) abdominal flaps have traditionally have been proposed for reconstruction. Pedicled bowel segments (colon and ileum) have been used (44, 45). They give a soft, pliable and moist end result, but complaints of rich mucus secretion and odor problems are infrequent. Pedicled TMG flap, either uni- or bilateral, including both muscle and skin component, suits well for vaginal reconstructions. DIEP flap reaches the region on its pedicle and is a good option, if suprapubic approach is used. In gender reassignment surgery vaginoplasty is performed with penile and posterior scrotal skin and a skin graft, if necessary. Vaginal lining from skin needs lubrication and careful cleaning at the beginning but it seems that the secretory function of the skin glands changes and to our clinical experience one year postoperatively skin in the vagina resembles mucosal lining macroscopically.
URETHRA
Congenital malformation, like severe hypospadia or bladder extrophy, stricture after infection or trauma, fistula between urethra and adjacent structures due to radiation therapy, infection, pressure or iatrogenic reasons, as well as tumor resection or trauma, may necessitate urethral reconstruction.
Goal is to achieve unobstructed urine flow with normal continence and no fistulas. If resection of the defect and direct closure is not possible, transposing the defect to the anterior wall of urethra allows the use of skin or mucosal graft, as there are supporting structures, e.g. symphysis, for the graft. Cultured autologous urothelium has been in experimental and limited clinical use, but its production is laborious, needs special settings and is expensive (46). In smaller fistulas, an interposition of a bulbocavernosus muscle, i.e. Martius procedure (47), may be used but especially fistulas between rectum and urethra need bigger muscle, usually gracilis. Local islanded skin flap may replace the missing urethral wall in the pressure ulcer reconstructions. A total reconstruction of urethra distal to sphincters can be corrected with an axial, extended groin flap, like in phalloplasties. In all longer reconstructions postvoidal dripping of urine is a problem, as the spongious tissue around urethra is missing.
Reconstruction methods in different regions
SCROTUM
In scrotal defects testicles can temporarily be buried under inguinal or medial thigh subcutis. After acute phase, the scrotum is reconstructed to restore normal appearance, a pocket for testicles allowing more optimal temperature for spermatogenesis, hindering their atrophy and sheltering the pain sensitive organs from external impact. Skin graft alone lacks the buffering effect of a subcutaneous tissue. Direct closure is often possible, if even a small remnant of scrotal tissue is left, as its skin is very elastic. Perineal soft tissue or medial thigh skin flaps are useful in total loss. Neoscrotum can also be shaped of gracilis muscle, which is opened as a fan by releasing its fascial structures, sutured as a pouch and grafted with a thick skin graft.
PENILE SKIN
Phimosis, infection, e.g. balanitis xerotica obliterans or Fournier's gangrene, dermatological problems like lichen, tumors, burns or trauma are etiological factors for penile skin defects. Repeated circumcision in persistent balanitis may create a troublesome shortening of penile skin, an iatrogenic hidden penis, which indicates reconstruction.
Due to very special properties of its skin, penile skin reconstructions are delicate. Reconstruction should produce ample, gliding skin allowing erection, in avoidance of painful and instabile scars, especially in sulcus coronarius or frenulum. Missing penile skin can be replaced with skin graft. The thicker the graft, the less scar formation, but full thickness skin graft take is suboptimal. Usually a thick partial thickness skin sheet covering the whole defect, rotated helically around the shaft, produces an acceptable end result. Scrotal skin has the same properties as penile skin; it is elastic, loose and expandable. Scrotal skin flap should be selected, if there is risk of poor graft take, shortening or scarring.
PHALLOPLASTY
Indication for phalloplasty is often gender dysphoria, but it is also indicated after penile amputation due to cancer or trauma or severe congenital malformations. Numerous phalloplasty methods with pedicled or free flaps have been described proving that none of them is ideal (48). Neophallos is not a penis; sexual function is different, protective and erogenous sensitivity are lacking or diminished and the appearance and urinary function are never perfect. Voiding may be possible on a vertical position, but lack of supporting tissue around neourethra causes pooling and dripping of urine afterwards. Skin lining in neourethra produces debris resulting in permanent bacteriuria with typical odor.
Microvascular radial forearm flap constructs a neopenis in “a tube within a tube roll” fashion and has been a gold standard among different phalloplasty methods (49). In 2005, we started to use our own method, a double flap phalloplasty (50) where the neourethra is formed of a pedicled extended groin flap and wrapped inside of another flap, either pedicled extended groin flap or pedicled ALT from contralateral side. The double flap phalloplasty is simpler and the donor sites are less visible than in the RFF phalloplasty.
In 2007, a technique of functional phalloplasty with a neurotised latissimus dorsi muscle allowing motor function was presented (51). Since 2010, we have used our own functional phalloplasty method with bilateral gracilis muscle flap for the penile shaft and a groin flap for the neourethra (52). Wound healing is quicker, the donor site problems minimal, color match good and fistula formation rarer than in phalloplasties where skin-subcutaneous flaps are used.
PELVIC FLOOR
Reconstruction of the pelvic floor is necessary after pelvic exenteration or after resection of an extensive tumor of colorectal or urogenital origin. In colorectal malignancies, total mesorectal excision (TME) has become a commonly used resection technique (53, 30), which creates a bigger levator muscle defect than with conventional abdominoperineal excision thus increasing the risk for perineal hernia. At present, patients receive preoperative radiochemotherapy more frequentely, which might even double the frequency of wound healing problems (54).
Several autologous flaps and synthetic materials have been introduced to the reconstruction of the pelvic floor (55, 56, 57). Especially omentum and rectus abdominis flap with skin island have been widely accepted. In colorectal surgery gluteus muscle flaps with overlying skin combined with synthetic materials, like allogen dermal matrix (ADM), have gained popularity lately. Current synthetic materials are strong and versatile, but also expensive and not ideal in infected wounds. Especially if an autologous flap is needed to fill the pelvic cavity and give support, TMG flap offers, except muscle, the patient's own vascularised dermis to patch the defect in the pelvic floor and is thus ideal flap in bigger pelvic floor defects.
FUTURE PERSPECTIVES
The pelvic region is everyone's and no one's land, which makes the development of treatment protocols demanding. Flexible cooperation between several specialities is extremely important, and each patient should get individually planned treatment.
Synthetic matrix products are good innovations aiding in tissue repair and hernia prevention, but they are expensive to produce and use. In future they should be compared with the old methods using autologous tissues, such as fascia lata, dermis or muscle (58).
Palliative surgery in perineopelvic region has been neglected in many cases, possibly due to reconstructional challenges. Still, it seems that pelvic palliative surgery alleviates effectively the suffering of the patient and gives better quality of life and should thus be promoted.