
Abstract
Backround and Aims: Soft-tissue reconstruction of the vulva following resection of malignancies is challenging. The function of perineal organs should be preserved and the reconstructed area should maintain an acceptable cosmetic appearance. Reconstruction with local flaps is usually sufficient in the primary phase after a radical vulvectomy. Numerous flaps have been designed for vulvar reconstruction usually based on circulation from the internal pudendal artery branches.
In this paper we introduce our modification of the gluteal fold V–Y advancement flap as a primary reconstruction after a radical vulvectomy.
Patients and Methods: Twenty-two patients were operated with a radical vulvectomy because of vulvar malignancies. The operation was primary in eight and secondary in 14 patients. The reconstruction of the vulva was performed in the same operation for each patient
Results: All flaps survived completely. Wound complications were registered in three patients. Late problems with urinary stream were corrected in two patients. A local recurrence of the malignancy was observed in six patients during the follow-up period.
Conclusions: Gluteal fold flap is easy to perform, has a low rate of complications and gives good functional results.
Even a large defect can be reconstructed reliably with this method. A gluteal fold V–Y advancement flap is sensate and our modification allows the flap to be transposed with lesser dissection as presented before.
Keywords
INTRODUCTION
High morbidity and recurrence risks after vulvectomy are well documented in the literature (1). An immediate reconstruction of the defect allows a more radical resection of the affected vulva improving clear resection margins (1). Recently, there has been an increase in the incidence of vulvar cancer (2). This is probably due to the higher incidence in young women and is closely related to the induction of human papillomavirus to vulvar intraepithelial neoplasia (3). However, the patients are still most often in old age and frequently in a poor general condition. The most preferred method for vulvar reconstruction should produce a functional result to the area with an acceptable cosmetic result. The flaps should not be too bulky and the ideal reconstruction should result in a low rate of complications.
Several methods have been introduced for vulvar reconstruction. Primary reconstruction with local tissue whenever possible is the standard treatment (4). The gluteal fold area consists of a rich network of cutaneous perforators arising from the internal pudendal artery. This is why the area serves as good basis for flaps raised to cover central defects in the perineum. A traditional gluteal fold flap is used as a transposition flap based on these perforators (4).
Paik-Kwon et al. introduced this flap to be transferred to the defect in a V–Y manner with good results (2). Since then this method has gained popularity and is used as a standard treatment in several clinics (5). The advantage of the V–Y technique is that the base of the flap can be wider and it requires less dissection compared to a transposition flap in order to reach the midline. One more major advantage is that in a V–Y manner the branches of the pudendal nerve are not cut and thus the flaps remain sensate (2).
In this paper we present our results of vulvar reconstruction with V–Y gluteal fold flaps. We have modified this method further to a less invasive direction not presented before in the literature.
PATIENTS AND METHODS
Twenty-two patients were operated between November 2005 and October 2010 in the Department of Gynaecology in Tampere University Hospital. The mean age of the patients was 78 years (range 39–89 years). The operated malignancies were epidermoid carcinomas in 19, Paget's disease in two and a malignant melanoma in one patient. The operation was primary in eight patients and secondary in 14 patients after a recurrence of a former smaller resection and direct closure of the wounds. The operations lasted in average 3 hours 20 minutes (range 1h 45 min–5h). A radical vulvectomy was done after the lymphatic procedure. The reconstruction of the vulva was performed in the same operation for each patient.
OPERATIVE TECHNIQUE
The patients are in a gynaecologic position during the whole procedure (Fig. 1). At first a sentinel node biopsy and/or inguinofemoral and parailiacal lymphadenectomies according to the nodal status are performed. This is followed by a radical vulvectomy. In the reconstruction the flaps are designed drawing the gluteal fold line as the centre of the flap (Fig. 2). The flap is dissected with medial traction straight down through the fascia. The flap is only slightly undermined in the posteromedial edge where the movement of the flap is biggest. The upper medial sharp corner is left intact so that the flaps move in a swinging manner keeping the upper corner as a pivot point (Fig. 3). The donor site is closed directly in two layers. The medial edges of the skin are sutured to the vaginal and urethral openings. No drains are used. A urinary catheter is left in place for five days and the skin sutures are removed on day 10. The patients lay in bed for three days legs slightly separated. After that they are mobilised freely but avoid sitting in an ordinary chair for one week.
RESULTS
Primary wound complications were registered in three patients. One dehiscence of the donor wound and two wound infections were noticed. All of these healed with conservative methods. All flaps survived completely.
The mean size of the tumour measured from the specimen was 4 cm (range 1,5–12 cm). The lateral surgical margins were relevant in all patients. However, centrally at the vaginal resection line the margins were assessed only marginal (less than 7 mm) in 12 patients.
Postoperatively, eight patients received local radiation therapy to the vulvar and inguinal areas. The radiation therapy was given approximately two months postoperatively. The mean radiation dose given was 50 Gy (range 38–56 Gy). In two patients the planned radiation therapy had to be postponed because of delayed wound healing.
The mean follow up time was 29 months (range 2–79 months). A late disturbance in the urinary stream was noticed in two patients as a result of a skin hood over the urethra. A local skin plasty solved the problem in both cases.
A recurrence of the malignancy in the vulva was noticed in six patients in average of 12.5 months after the reconstruction. The recurrent disease was treated operatively in two patients and conservatively in four patients.
DISCUSSION
Despite advances in neoadjuvant therapy for vulvar malignancies, surgical resection of the tumour remains the treatment of choice (4). Immediate reconstruction of the surgical defect enables large tumour resection improving clear pathological margin rates and facilitates wound healing after vulvectomy (1). Several musculocutaneous flaps have been introduced for vulvar reconstruction. These flaps are usually too bulky and do not give the best result after a standard vulvectomy (1, 6, 7).
The use of local flaps for vulvar reconstruction has gained popularity recently (4, 9, 10). The tendency of recurrence of vulvar cancer has to be kept in mind when planning the primary reconstruction. Using local flaps in the primary reconstruction allows the possibility to use a larger and more bulky flap in case of further operations needed. Local flaps are thin and pliable and the vascularity based on terminal branches of the internal pudendal artery is reliable (8). The traditional gluteal fold flap is based on these vessels and is used as a transposition flap (1). Paik-Kwon et al. presented a V–Y modification of the gluteal fold flap in 2006 (2). They presented excellent results and showed that even large defects can be closed in this manner. Similar good results were confirmed also by an Italian group (5). A specific advantage is that in a V–Y fashion the pudendal nerves are not cut and thus the flaps are sensate postoperatively (Fig. 5).
We started using the gluteal fold flap in a V–Y fashion in 2005. Quite soon we realised that the flaps did not have to be dissected completely free as island flaps. We left the anterior sharp corner intact and transposed the flaps in a swinging manner keeping the anterior part as a hinge for the movement. When doing this we realised that even larger defects could be reconstructed without tension. In our opinion this saves time, keeps the sharp most critical corner of the flaps intact without loosing the ability of the flaps to be transferred to cover the defect.

A 39-year-old woman with a stage III vulvar cancer. The patient had refused surgical treatment two years previously.
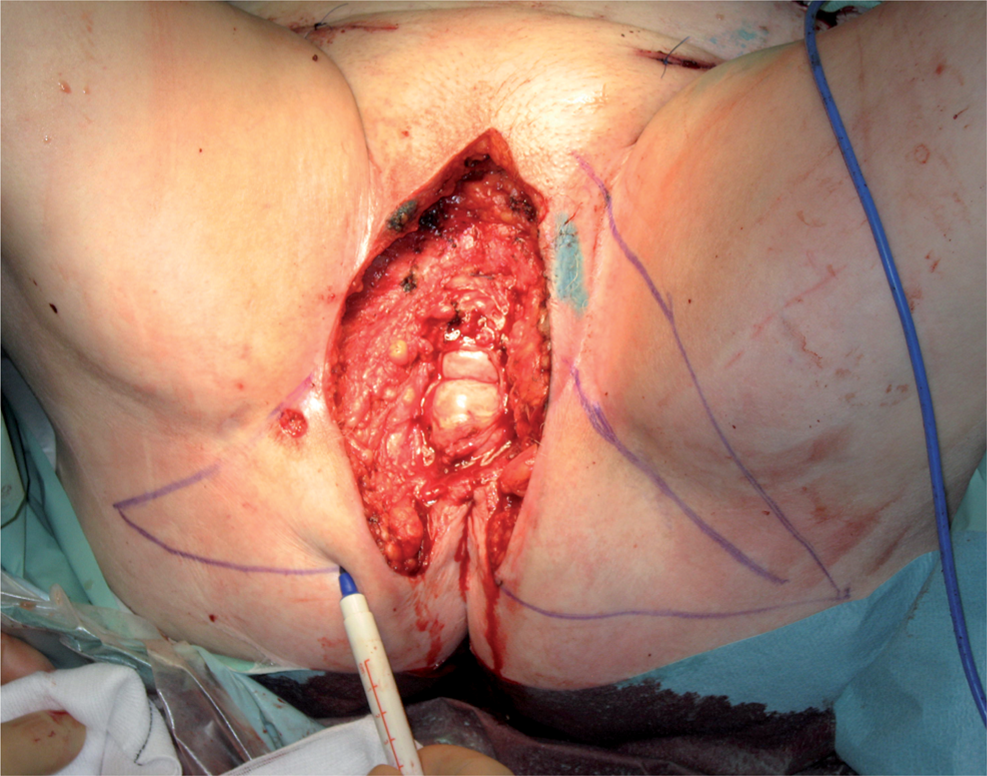
A radical vulvectomy was performed with sentinel node biopsies and inguinofemoral and parailiacal lymphadenectomies. The flaps are planned keeping the gluteal fold crease as a centre line for the flaps. The upper sharp corner is left intact.

The flaps are transposed to cover the defect keeping the anterior corner as a hinge for a swinging movement of the flaps. The flaps are only slightly undermined in the medial part. The medial skin edges are sutured to the urethral and vaginal stumps.

One week after the operation the wounds were healing otherwise normally but showing a slight dehiscence of the upper vertical wound. This was infected but treated conservatively and healed well. The patient got chemo-radiation therapy postoperatively. Four years after the operation she was disease-free and had a normal urinary function and could perform a normal sexual intercourse.
We had an equal number of recurrent tumours in the follow-up period as reported in the literature (11). Recurrence is a typical phenomenon in vulvar cancer. Primary gluteal fold flaps enable still the use gracilis, rectus abdominis or whatever more distant flaps in secondary cases without problems.
Our modification of the gluteal fold flap is easy to perform and seems to fit for all standard cases of vulvectomy. The procedure is effective in reconstructing even a large defect and has a minimal rate of complications. The functional results are acceptable allowing urination and sexual intercourse. The flaps or scars seem not to affect walking or sitting of the patients. The scars are quite well hidden and the flaps are sensate. That is why this method is our primary choice for vulvar reconstruction.
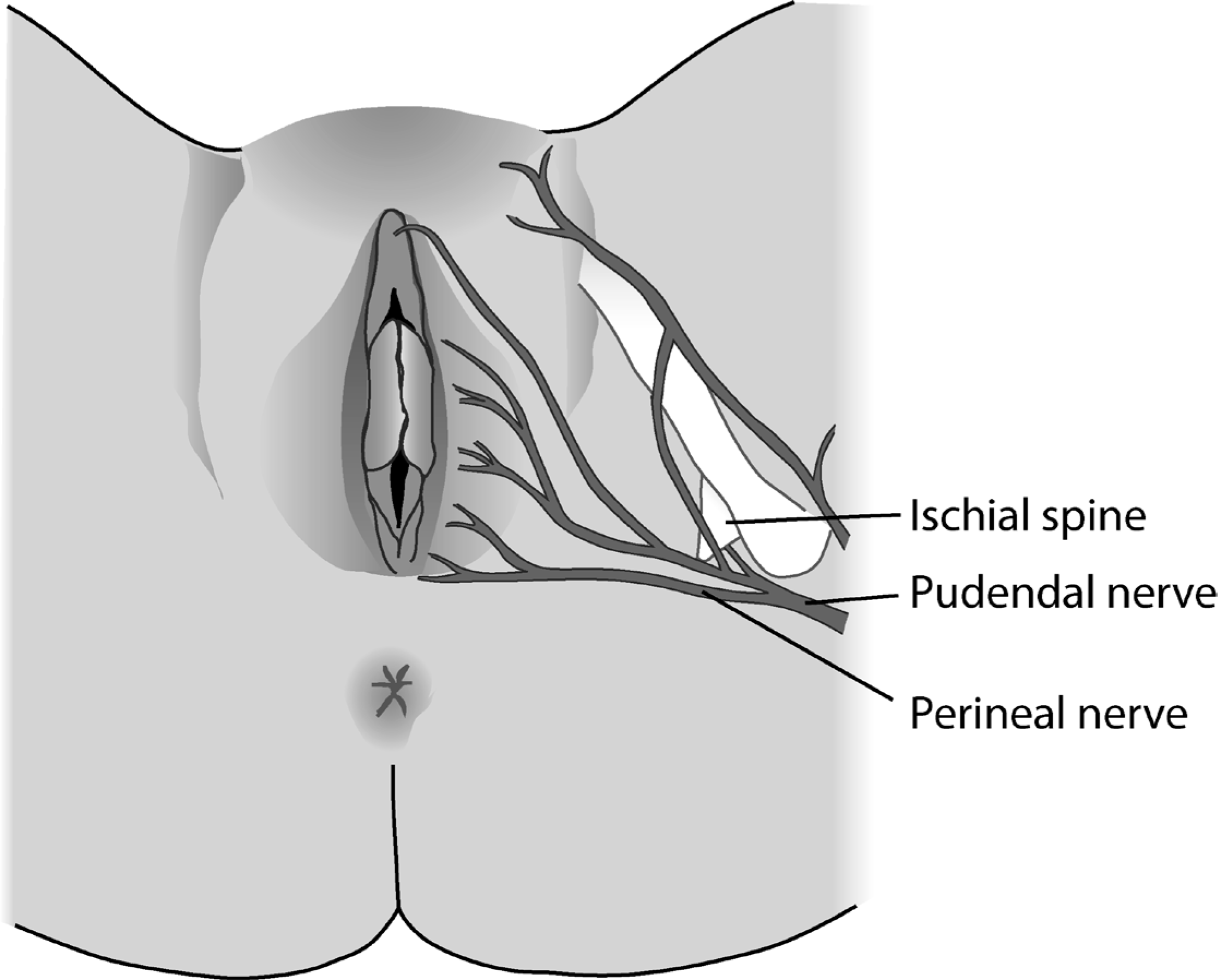
A schematic drawing of the course of pudendal nerve giving sensation to the vulva. In a V–Y gluteal fold operation the nerve branches are left intact giving sensation to the flaps.